
Abstract
Background/objective
Physical, cognitive and psychological factors such as self-efficacy and motivation affect participation in populations with acquired disabilities. Volition is defined as a person's motivation for participating in occupation. The concept of ‘volition’ expands similar concepts and theories, which focus mostly on cognitive processes that influence motivation. Although volition seems to affect participation, the association between these two concepts has not been examined in populations with acquired disabilities. This scoping review explored this association.
Methods
The literature review used a structured five-stage framework, according to predefined inclusion and exclusion criteria. Seven electronic databases (CINAHL, PsycINFO, PubMed, Web of Science, SCOPUS, The Cochrane Library-Wiley, OTseeker) and Google Scholar were searched for relevant articles, published in English from January 2001 to May 2018.
Results
A total of 18 articles, relating to populations with various diagnoses were included. Two directly examined volition and participation and showed a positive association between them. Other articles discussed the effect of participants’ chronic condition on their volition and participation, the effect of volition on participation, or the effect on participation of an intervention addressing volition.
Conclusions
An acquired disability affects both volition and participation, and volition seems to affect participation among people with acquired disabilities. Few articles showed positive effects of interventions that addressed clients' volition, on participation. Further research should include additional health conditions and types of literature, to better understand the association between these concepts. This understanding will contribute to the development of occupational therapy interventions that emphasise volition, in order to improve participation outcomes.
Introduction
Participation is defined as ‘the act of participating’ or ‘taking part in something’ (https://www.merriam-webster.com). The concept of participation has developed over time and has expanded to various areas, including healthcare. A similar concept is ‘patient participation’. According to Nilsson, From, and Lindwall (2019), patient participation includes a process of learning (the tasks, routines and roles that are relevant and available for the patient) and reciprocity (mutual engagement in activities), that occur in a caring relationship between the patient and the healthcare provider. Kvæl, Debesay, Langaas, Bye, and Bergland (2018) described two important components of patient participation: ‘engagement’, which is the process of transitioning from a passive approach to one’s medical condition or disability to a more active committed one; and ‘activation’, which is similar to the commitment component of patient engagement. They argue that patient participation is an important part of empowerment, which is the process of taking responsibility on one's own health. According to Kvæl et al. (2018), the process of patient participation needs to be conceptualised as an interaction between health condition, environmental factors and the patient's personal factors. In 2001, participation was given new meaning, as part of the International Classification of Function, Disability and Health (ICF) (World Health Organization, 2001).This classification is also based on the interaction between personal factors, the health condition and the environment, that together influence an individual's functioning and disability. According to the ICF, participation is defined as ‘involvement in a life situation’ and includes communication, mobility, and domestic and community functioning. The ICF definition of participation seems to include the components of engagement and learning that were mentioned earlier. In addition, the definition of participation has been expanded more recently to include subjective issues such as choice, importance and enjoyment (Desrosiers et al., 2008; Heinemann et al., 2013; Vargus‐Adams, 2012).
Since the publication of the ICF (2001), participation has become a major outcome of rehabilitation (Mallinson & Hammel, 2010; Engel-Yeger, Tse, Josman, Baum, & Carey, 2018), and an important outcome of interventions in occupational therapy (Lewthwaite et al., 2018; Noyes, Sokolow, & Arbesman, 2018; Piškur, 2013). Use of the concept of participation has expanded due to its association with satisfaction, wellbeing and quality of life (Amoah, 2018; Bergström, Guidetti, Tham, & Eriksson, 2016; Wong et al., 2017), and it is becoming a preferred outcome of rehabilitation specialists, especially for patients with acquired disabilities (Engel-Yeger et al., 2018).
The ICF defines disability as an ‘umbrella term for impairments, activity limitations or participation restrictions’ (WHO, 2001) that result from interactions between a person (with a certain health condition) and that person’s contextual (environmental and personal) factors. An acquired disability evolves following an accident, illness, or development of a health condition (Levack et al., 2015). A review of the literature shows that people with acquired disabilities due to diverse health conditions such as stroke, multiple sclerosis (MS), chronic pulmonary and kidney diseases, and mental disorders, usually experience a decrease in participation (Cahill, Connolly, & Stapleton, 2010; Chugg & Craik, 2002; Dumont, Gervais, Fougeyrollas, & Bertrand, 2004; Hoyle, Gustafsson, Meredith, & Ownsworth, 2012; Seidel et al., 2014; Taylor et al., 2010).Various factors were found to affect participation among these populations, including age, motor and cognitive impairments, psychological factors, environmental accessibility and family support (Cahill et al., 2010; Desrosiers et al., 2008; Gadidi, Katz-Leurer, Carmeli, & Bornstein, 2011; Hammel, Jones, Gossett, & Morgan, 2006; Seidel et al., 2014). Another important factor that affects participation is self-efficacy, which was defined by Bandura (1997) as ‘the person's belief about his/her ability to organize and execute the actions needed to accomplish a goal’.
Kielhofner's Model of Human Occupation (MOHO) (Taylor, 2017) is a well-known theoretical and clinical model in occupational therapy. It aims to explain the factors that influence human occupation, a new term for participation. This model includes four major components that influence human occupation: volition, habituation, performance capacity and the environment. Volition, explains how individuals choose and are motivated to perform activities and occupations that fill their lives. It includes a process of anticipation (of fields of interest and activities), choice (of activities and occupations), experience (of actions and enjoyment/satisfaction) and interpretation (of these actions). The process is influenced by three elements: personal causation, values and interests. Personal causation is the awareness of the effects of one's acting and doing, and includes a sense of personal capacity, which is an individual's evaluation of his/her physical, intellectual and social abilities, and self-efficacy. Values derive from the surrounding culture, as the described process of anticipation, choice, experience and interpretation takes place within a cultural context. Interests are related to the enjoyment and satisfaction of doing things or participating in activities. Each person creates his/her own unique pattern of interests (Kielhofner, 2008; Taylor, 2017).
The concept of volition in the MOHO expands similar concepts and theories, such as such as Bandura's Self-Efficacy theory (1994, 1997), and the Theory of Planned Behavior (Ajzen, 1991), that deal with the factors that motivate people to action. According to the Self-Efficacy theory (1994), human motivation is influenced by perceived self-efficacy, the beliefs that determine people's goals, the effort they expend in their accomplishments, and their persistence in dealing with difficulties and failures. Ajzen's Theory of Planned Behavior (1991) focuses on intention and motivation as the main causes for actions and behaviours. According to this theory, a person's engagement in a behaviour or action is affected by the degree of intention for this action. This intention is influenced by personal attitudes or values, subjective norms, and the ‘perceived behavioural control’, that is congruent with Bandura's definition of perceived self-efficacy (Redding, Rossi, Rossi, Velicer, & Prochaska, 2000). These concepts and theories show that human motivation is influenced mostly by cognitive processes, that include thoughts and beliefs regarding capabilities, and the ability to direct and sustain behaviour towards a specific goal. Less attention is given to social and cultural factors, emotions and feelings – all of which could have a strong influence on motivation and participation (Pritchard, Brown, Barker, & Haines, 2014). The concept of volition in the MOHO expands upon these ideas, because it also includes socio-cultural and affective factors, which, according this model, influence occupational choices and participation (Taylor, 2017).
Since a person's volition is also influenced by factors such as interests and values, which develop throughout one’s life, the question raised is whether a person's volition might be associated with participation or improvement in participation after an injury, onset of a disease or chronic disability.
The literature shows evidence of an association between motivation and participation, especially in exercise or sport activities. Broonen, Marty, Legout, Cedraschi, and Henrotin (2011) describe the concept of ‘implementation intentions’, which is the plan to carry out a physical activity that connects the motivation to exercise with exercise participation. This was found in studies of individuals with acquired disabilities due to low back pain (Broonen et al., 2011), heart disease (Luszczynska, 2006) and spinal cord injury (Latimer, Ginis, & Arbour, 2006).
The ‘Self-Determination Theory’ (Ryan & Deci, 2007), postulates that intrinsic motivation is essential to exercise adherence. This theory was examined in several studies that showed an association between motivation and exercise participation in individuals with acquired disabilities due to MS (Fasczewski, Gill, & Rothberger, 2018), Parkinson's Disease (Chang, 2012) and other diseases. However, none of these studies related to the broader concept of volition as defined in the MOHO (Taylor, 2017), which includes emotional and cultural factors. Moreover, this body of research focuses on the association between motivation and participation mostly in exercise and sports and does not examine it in relation to participation in daily domestic and community activities. To the best of our knowledge, a review that examines the association between volition as defined by MOHO, and participation has not been conducted.
Examining the association between these two concepts is important, especially for occupational therapists, who focus on improving clients' participation in all facets of life. Increased understanding of this association is required to understand the implications of volition on participation outcomes, and to consider if and how it should be addressed in therapy. As many of the clients treated by occupational therapists have acquired disabilities, it is important to examine the association between volition and participation in daily activities, particularly among these populations.
Arksey and O'Malley (2005) described four reasons for conducting a scoping review, one of which is ‘to identify existing gaps in the literature’, which is the main purpose of the current review. This scoping review aimed to summarise the evidence related to the association between volition and participation among adults with acquired disabilities.
Methods
The methodology used in this study was based on the five-stage framework for scoping reviews proposed by Arksey and O'Malley (2005).
Identifying the research question
The main question addressed in this review was: ‘What is known from the literature about the association between volition and participation among people with acquired disabilities?’
Identifying and selecting relevant studies
The following databases were searched by the authors for relevant articles published in English from May 2001 to May 2018: CINAHL, PsycINFO, PubMed, Web of Science, SCOPUS, The Cochrane Library-Wiley, and OTseeker. Google Scholar was also searched. The search was limited to journal articles published since May 2001, which is the date the ICF was first published (WHO, 2001), where the new meaning of the concept of participation was first mentioned. The review did not include evidence from published books or manuals. Search terms initially included volition combined with participation, without focusing on a specific population, to identify as many relevant articles as possible. A search in Google Scholar with these terms yielded 29,900 results. To narrow the search and reach more relevant articles, the term ‘Kielhofner’ was added.
The search included peer-reviewed articles that described exploratory, observational or interventional studies, using quantitative and/or qualitative methods. To reach all relevant literature, the search included grey literature that was found through Google Scholar. Articles and other forms of literature were selected if their content met all of the following criteria: 1. The term volition, based on Kielhofner's definition, appeared in the abstract and/or full text. 2. The term participation, in the context of the ICF definition or similar models mentioned above appeared in the abstract and/or full text. 3. Literature related to populations with a disability due to an acquired disease or condition, regardless of age or type of disease. 4. Studies that included: a. an assessment or description of the participants' volition, individually or as part of the four components of the MOHO (Kielhofner, 2008), as well as a description or assessment of the participants' participation; or b. an intervention program that addressed volition and was related to improving aspects of participation. Articles were excluded if their content included studies regarding populations with congenital or developmental diseases; studies related to psychometric properties of assessment tools for measuring volition and/or participation; and studies in which the participants did not have a medical condition that caused a disability.
Charting the data
Once the articles were chosen, the author(s), year of publication, study location, diagnosis, sample characteristics, study aim, methodology (quantitative/qualitative/mixed), outcome measures and results relevant to the research question were recorded.
Collating, summarising and reporting the results
After reading all included articles, the authors searched for common themes, and eventually defined three main categories into which all articles were organised (Table 1): (1) The influence of a disease or a chronic condition on volition and participation; (2) The influence of volition on participation; and (3) The effect of an intervention that addressed volition on participation outcomes.
Description of included studies (alphabetised according to first author).
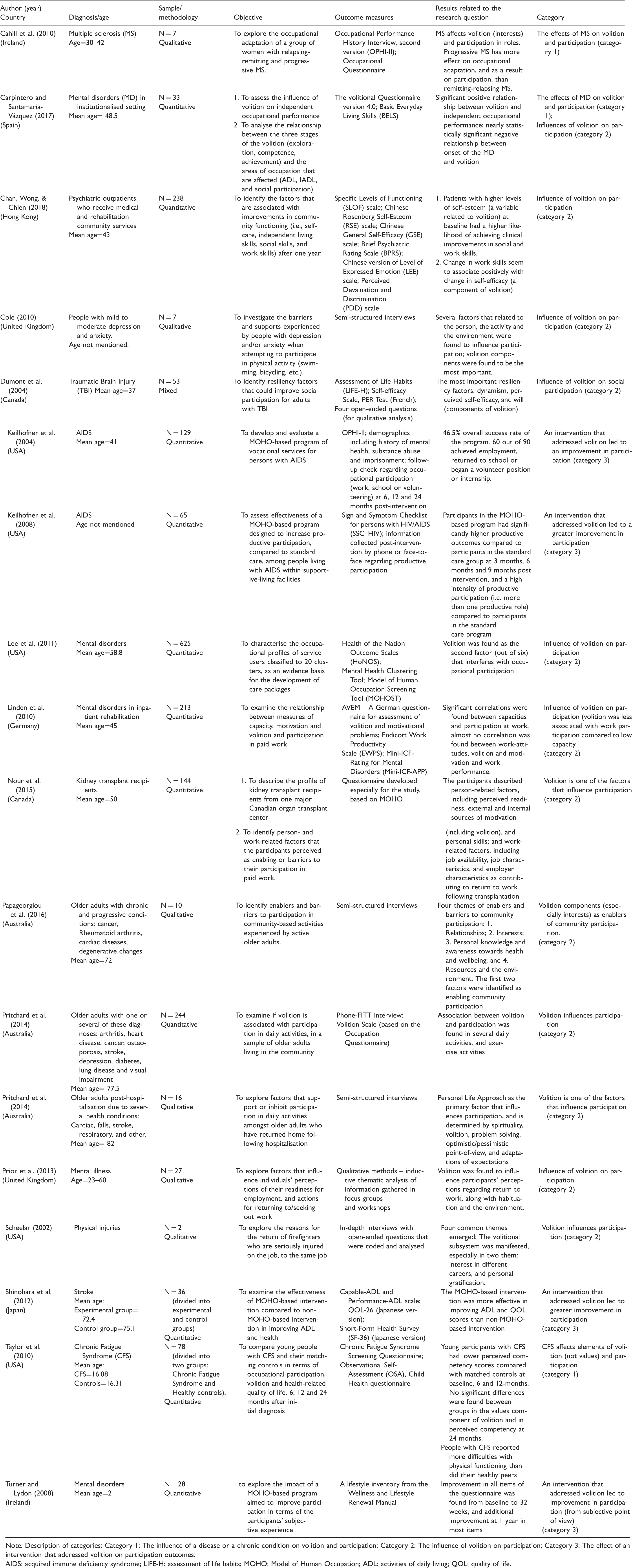
Note: Description of categories: Category 1: The influence of a disease or a chronic condition on volition and participation; Category 2: The influence of volition on participation; Category 3: The effect of an intervention that addressed volition on participation outcomes.
AIDS: acquired immune deficiency syndrome; LIFE-H: assessment of life habits; MOHO: Model of Human Occupation; ADL: activities of daily living; QOL: quality of life.
Each author categorised the articles independently. This was followed by discussion between them when differences occurred until consensus was reached.
Results
Initially, 1806 articles were found. After excluding duplicates, selecting literature by title and abstract, and reviewing the full text of relevant literature, 18 articles were selected and included in this scoping review. The search process is represented in Figure 1. The studies were published from 2002 to 2018; eleven were quantitative, six were qualitative, and one used mixed-methods. Six took place in the United States and Canada, while the remainder were conducted in Australia, Europe, Hong Kong and Japan. Seven articles included people with mental disorders. The rest included individuals with traumatic brain injuries or stroke, progressive diseases (MS), injuries, and a variety of chronic conditions. Four studies related only to the aspect of participation in paid employment, while the others reported varied aspects of participation. Most of the articles were classified to category 2: the influence of volition on participation. Table 1 summarises the data from each article, including its category.
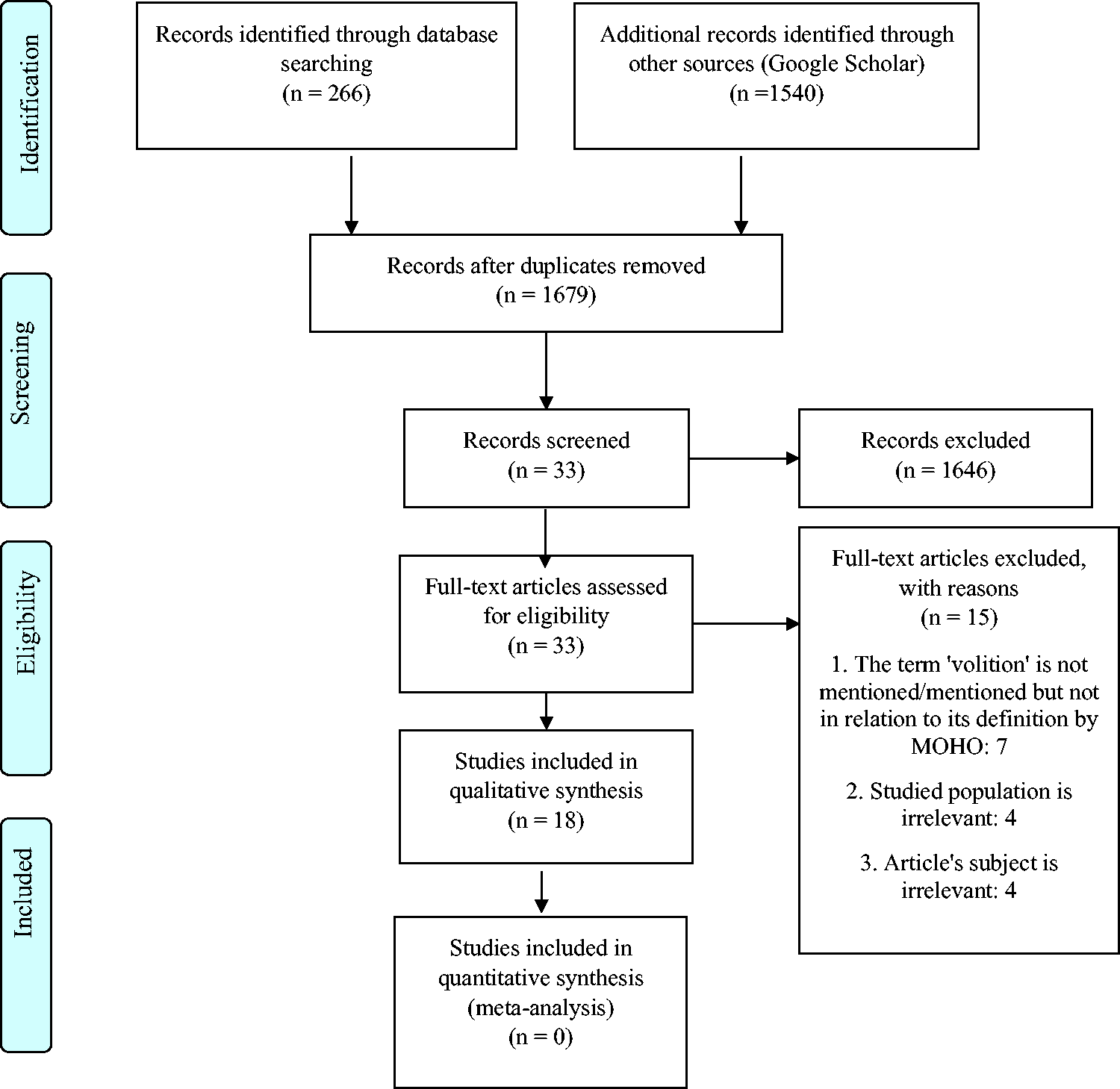
Flowchart of search strategy based on PRISMA flow diagram.
Two articles related to the research question specifically: Pritchard et al. (2014) and Carpintero and Santamaría-Vázquez (2017). Pritchard et al. (2014) examined the association between volition and participation among older adults living in the community with a variety of chronic conditions, including heart disease, cancer and stroke. Data regarding the levels of volition and participation were collected from the participants through self-report measures. The results showed a positive association between volition and participation in several daily activities, including light house-work, meal preparation, shopping and gardening, and in walking and strengthening exercises, suggesting that higher levels of participation were associated with higher levels of volition for these specific activities. Carpintero and Santamaría-Vázquez (2017) examined the influence of volition on independent occupational performance (a term similar to participation). In addition, they explored the relationships between the three stages of volition (exploration, competence and achievement), as defined by De Las Heras, Geist, Kielhofner, and Li (2007), and participation in BADL, IADL and social participation in people with mental disorders living in an institutionalised setting. The results found positive association between volition (and each of its stages) and independent participation in self-care, domestic and community skills, as well as social activities and relationships.
Three articles discussed the influence of a disease or chronic condition on volition and participation (category 1) (Cahill et al., 2010; Carpintero & Santamaría-Vázquez, 2017; Taylor et al., 2010). Their results presented a negative effect of a chronic disease on a person's volition and participation among populations with MS, CFS and mental disorders.
Twelve articles discussed the influence of volition (or one of its components) on participation (category 2) (Carpintero & Santamaría-Vázquez, 2017; Chan et al., 2018; Cole, 2010; Dumont et al., 2004; Lee et al., 2011; Linden, Baron, & Muschalla, 2010; Nour, Heck, & Ross, 2015; Papageorgiou, Marquis, & Dare, 2016; Prior et al., 2013; Pritchard et al., 2014; Pritchard, Warren, Barker, Brown, & Haines, 2016; Scheelar, 2002). The results of most of these studies, including Pritchard et al. (2014) and Carpintero and Santamaría-Vázquez (2017), showed that volition (or its components) affects different domains of participation, such as community and social participation, and return to work, among populations with various chronic diseases and conditions. Linden et al. (2010) was the only study that reported less effect of volition on participation. They found that work performance was affected more by the ability to work after the onset of the mental disorder, than it was with volition.
Four articles discussed the effect of an intervention that addressed MOHO components, including volition, on participation outcomes (category 3). The populations in these studies included post-stroke (Shinohara, Yamada, Kobayashi, & Forsyth, 2012), Acquired Immune Deficiency Syndrome (AIDS) (Kielhofner et al., 2004; Kielhofner, Braveman, Fogg, & Levin, 2008), and people with mental disorders (Turner & Lydon, 2008). All four studies showed effectiveness of the interventions that addressed volition in improving objective or subjective participation outcomes. Moreover, Kielhofner et al. (2008) and Shinohara et al. (2012) also showed they were more effective than regular/standard care interventions were.
Discussion
This scoping review summarises findings from 18 peer-reviewed articles regarding the association between volition and participation, among adults with acquired disabilities, that related to different elements of volition and participation. Only two studies (Carpintero & Santamaría-Vázquez, 2017; Pritchard et al., 2014) examined the research question specifically, and found a positive association between the two concepts. Their results indicate that volition, which includes the understanding of and confidence in one’s self-ability, the meaning of the activity, and the level of interest one has in the activity, is an important factor that can lead to more participation and engagement in daily domestic, community and social activities, and not only in exercise and sports activities, as was found previously in related literature; and vice versa: increased participation can lead to improvement in volition, all of which can result in improved health and wellbeing.
The remaining studies in the review showed a general influence of volition or its components on participation, and the influence of the disease or the chronic condition on volition and participation. Since the primary purpose of this scoping review was ‘to identify existing gaps in the literature’, the findings indicate that research in this field is still preliminary, despite its importance for the development of rehabilitation programs for people with acquired disabilities.
It is possible that only two studies that examined the association between volition and participation specifically were found, because the MOHO was used less as a clinical and theoretical model in therapy or rehabilitation settings of the populations mentioned in the review. Most adults with acquired disabilities such as TBI, stroke, MS, arthritis and the majority of chronic diseases, usually receive occupational therapy in medical or rehabilitation facilities. In these settings, the main treatment approaches focus on improving client factors, function and participation, by relating mostly to common basic and instrumental activities of daily living. In addition, limited time is given for therapeutic processes with each client within those settings, and sometimes there is an ‘unspoken’ expectation to perform a brief assessment and provide quantitative outcomes regarding the client's progress after one or two therapeutic sessions. This might explain the limited use of the MOHO and its specific instruments to assess clients' volition in the described settings, as compared to other settings and populations, such as people with mental disorders, developmental disabilities and dementia. The limited use of MOHO in these settings can also be concluded from other literature that relate to the relationship between volition and participation and were not included in the review, such as Des Las Heras, Lierena, and Kielhofner (2003) and Taylor (2017), which show the influence of focusing on clients' volition in therapy, on gradual improvement in their participation. Both the manual (Des Las Heras et al., 2003) and book (Taylor, 2017) exhibit the relationship between these concepts mostly in clients with mental disorders, dementia and developmental disorders and less in physical and neurological conditions, and/or physical rehabilitation settings. This can also explain the finding that almost half of the articles found in the current review focused on people with mental disorders. Another possible explanation is that the concept of volition does not need to be assessed and addressed in some therapeutic settings; however, the results of this review seem to refute this explanation. The lack of using MOHO as a clinical and theoretical model with the described populations, along with possible lack of awareness of therapists regarding the importance of addressing volition in these settings, seems to be more reasonable.
The articles included in the review related to one or several aspects of participation (i.e. community/social participation, work etc.), as can be seen from the results. In addition, the concept of volition has appeared in various ways in the included articles: in most studies it was mentioned as one of the four major components of MOHO, in the rest only some components of volition were found to be associated with participation (especially personal causation and interests). These findings indicate the diversity in the relationship between these two concepts.
The results of this review shed more light on the dynamics between the volition and the participation of people with acquired disabilities. They imply that in most cases, their own perception of their abilities to participate in activities, independently or with support, their values – such as the importance of work, the value of being active, etc., and their fields of interest and enjoyment, will have positive (improvement) or negative (no change or deterioration) influences on their participation. In addition, the disease or condition itself can have a negative effect on volition and participation. Nevertheless, a decrease in participation due to the disease or disorder, does not have to be caused by a decrease in volition (Linden et al. 2010).
Study limitations
This scoping review had several limitations. First, it did not include books or other forms of literature such as manuals. This might have limited the evidence found regarding the research question. In addition, very few of the selected articles specifically examined the association between volition and participation. Second, the populations studied did not include some health conditions that have major implications on functioning and participation, such as Parkinson's disease, spinal cord injury or motor neuron diseases. Furthermore, the interventional studies included in the review examined only people with AIDS and post-stroke. The exclusion of literature that was not published in English, might have omitted additional relevant articles. Moreover, the very specific inclusion criteria, might have omitted related literature that used different wording or terminology. A more general search yielded a few relevant articles that exhibited the relationship between volition and participation but they did not use the concepts of ‘participation’ (Jones, 2008) and ‘volition’ (Fan, Morley, Garnham, Heaseman, & Taylor, 2016). The quality of the articles included in the review was not assessed; however, this is usually not part of a scoping review. A further limitation is that the outcome measures used in the included studies were mostly self-report instruments. No observational tools were used to assess volition and participation, but this is probably due to a lack of instruments that were appropriate for the studies' aims and settings. It is recommended future reviews include evidence of the implementation of MOHO and its components including volition, in populations with acquired disabilities, as described in books and other forms of literature regarding MOHO (De Las Heras et al., 2003; Taylor, 2017).
Conclusions
This review suggests that the volition of a person with an acquired disability is an important factor which affects participation in domestic, social and community activities, as well as employment. Furthermore, a disease or a major change in health status can affect both volition and participation, and an intervention that addresses volitional components can contribute to improving participation. We believe these findings highlight the importance of examining the association between the two concepts, in order to improve rehabilitation outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.