
Abstract
Objective
The purpose of this study is to introduce a standardised assessment tool by verifying the reliability of the translated Korean version of the Feeding Abilities Assessment (K-FAA), which was developed to suit Korean culture.
Methods
The research subjects were 65 patients with dementia living in nursing homes. The K-FAA was completed by verifying the suitability of translation and reverse translation. The validity of the K-FAA was established through content validity, while its reliability was analysed based on internal consistency reliability for the items, test–retest reliability and inter-rater reliability.
Results
The content validity index determined, based on the assessment of professors, occupational therapists, and nurses, was more than .70. Cronbach’s α was more than .929, showing good internal consistency. A test–retest reliability of .884 was derived using Pearson’s correlation coefficient (p < .01), and an inter-rater reliability of .800 was derived using the kappa coefficients; intraclass correlation coefficient was .897, which also indicated good reliability.
Conclusion
The K-FAA was modified to fit the Korean domestic situation, and this assessment had high reliability. Therefore, K-FAA can evaluate the feeding ability of patients with dementia. Future studies should focus on providing evidence-based data to maintain or supplement the feeding ability of patients with dementia in Korea.
Introduction
Dementia is an acquired disease involving loss of intellectual capacity owing to brain dysfunction (Lee, 2013). People with dementia experience difficulties in performing daily activities because of their damaged cognitive function (Roger & Gerry, 2003). For example, people with dementia lose the functional ability to take a bath, followed by dressing themselves, using the bathroom, walking and eating (Cohen-Mansfield, Werner, & Reisberg, 1995; Kim & Jung, 2013).
Eating has a critical influence on not only the physical maintenance of a human being but also on the psychological and social aspects of human life (Hung & Chaudhury, 2011). In nursing homes, meal times are fixed, and workers simultaneously provide food to multiple elderly people within the designated time period. Hence, the focus is on the easy and prompt provision of food (Chang & Roberts, 2008; Kayser-Jones & Schell, 1997; Lee, 2002). This method hinders the joy of eating in patients with dementia and restricts their independent daily life. As a result, it can reduce the dignity of patients with dementia and increase their caregiver’s burden. To increase the quality of life of patients with dementia and their caregivers, maintaining physical functioning for as long as possible should be the goal of therapy related to daily living performance (Yang et al., 2012). Performance of activities of daily living (ADL) is one of the most important domains in occupational therapy. The capacity and limitations of patients can be understood by evaluating their ADL (Park, Lee, Jung, & Yoo, 2003). However, there are very few tools that evaluate the feeding of patients with dementia in Korea.
The Edinburgh Feeding Evaluation in Dementia Questionnaire (EdFED-Q) and the Eating Behavior Scale (EBS) are some of the international evaluation tools related to the feeding of patients with dementia (Tully, Matrakas, Muir, & Musallam, 1997; Watson, 1994). In Korea, the Eating Behavior Management Needs was developed by Lee (2015). These existing evaluation tools are widely used owing to their convenience and simple contents. However, the tools have limited use for direct evaluation and cannot provide an insightful understanding of the feeding ability of patients with dementia because the number of questions is small, and the items only involve contents related to the level of help required for the patient. The Eating Behavior Management Needs scale that was developed in Korea is appropriate for Korean culture. However, it is difficult to understand the actual functional level of patients.
In Canada, LeClerc and Wells (1998) developed the Feeding Abilities Assessment (FAA) to overcome the limitations of the existing international tools; they also tested the reliability and validity of the FAA using a sample of 156 patients with dementia (LeClerc, Wells, Sidani, Dawson, & Fay, 2004). This tool includes the evaluation of feeding performance ability and skill using utensils because it was originally developed to evaluate the feeding-related abilities of patients with dementia who are affected by ideational apraxia. The advantage of the FAA is that the assessment outcome can be used to design an intervention method that supplements the lost skills because the tool comprises assessment items based on the level of help needed, such as verbal direction or physical help (LeClerc et al., 2004).
This study develops a Korean version of the Feeding Abilities Assessment (K-FAA) by adapting and modifying the original, thereby capturing the feeding ability of patients with dementia, taking into consideration Korean culture. By testing the content validity and reliability of the developed K-FAA, we aim to introduce a standardised tool that is applicable to the Korean population.
Methods
Subjects
A total of 65 patients with dementia were selected as the subjects of this study by referring to Javali, Gudaganavar, and Raj (2011), who reported that high reliability of internal consistency can be secured when the number of subjects exceeds 50. All subjects who participated in this study (1) stayed in a nursing home for longer than one week; (2) were capable of eating meals by themselves with no physical defects (amputation, paralysis or fracture); (3) had no dysphagia or cerebrovascular accident and (4) were capable of communicating. Before beginning this research, the study protocol was approved by the Institutional Review Board (IRB) at Yonsei University. Following this, the subjects received sufficient explanation about the purpose and method of the study, and only those who voluntarily agreed to participate in the study were selected. This study was conducted over approximately two months from August to September 2017.
Assessment tools
FAA
This tool evaluates the feeding ability of patients with dementia in two steps (Table 1). First, it measures the subjects’ ability to initiate, sequence and follow through with complex or simple actions (feeding performance ability). Second, it assesses whether a subject can use tools appropriately.
Korean version of the Feeding Abilities Assessment.
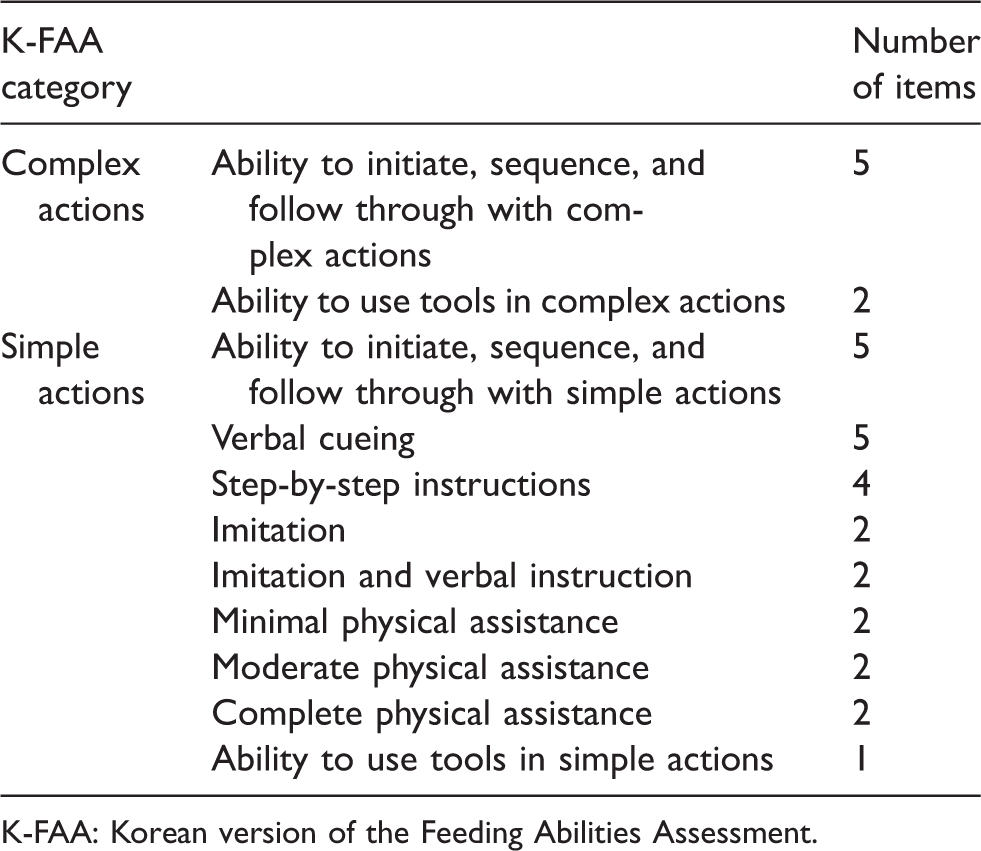
K-FAA: Korean version of the Feeding Abilities Assessment.
We conducted an observation-based evaluation during the subjects’ usual mealtime in their usual mealtime environment. Before this, we verified that subjects’ glasses and dentures were ready for use. The evaluation was conducted by dividing eating tasks into the two domains of complex and simple actions. During the observation of the subjects’ eating behaviour, the tester scored the item as ‘yes (0)’ when the subject was capable of performing the relevant action and as ‘no (1)’ when the subject was incapable of doing so. The evaluation ended when the answer to all items in the first domain was ‘yes’. If the answer was ‘no’ to more than one question in the first domain, the evaluation continued to the second domain of simple action. The lowest and highest scores of the evaluation were 0 and 32, respectively. A lower score represents the subjects’ capability for independent feeding.
Procedure
In this study, the following two steps were performed to develop the K-FAA and test its reliability (Figure 1).
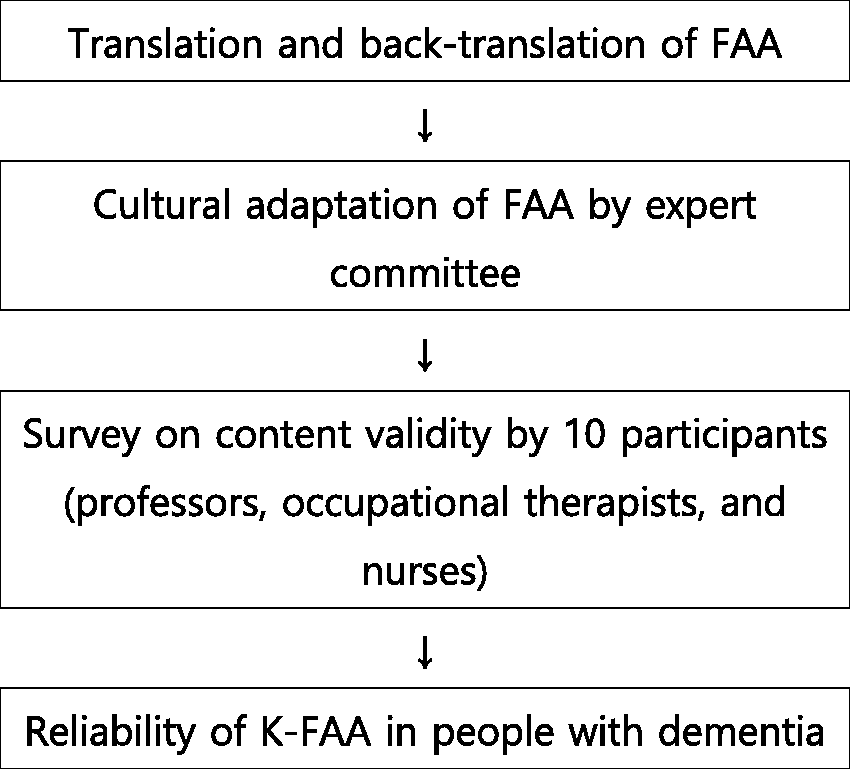
Research process.
Stage 1: Development of the K-FAA
We first worked on adapting the FAA to a Korean context to produce a Korean version. The adaptation process consisted of translation and a validity test, an evaluation of the understandability of the translated outcome and reverse translation and another validity test. The K-FAA was completed after a review process by an expert committee (Table 2). The validity of the K-FAA was computed by measuring the content validity of the tool using 10 participants comprising professors in the department of occupational therapy from the university, occupational therapists and nurses working with patients with dementia or in elderly facilities.
FAA change process for cultural adaptation.
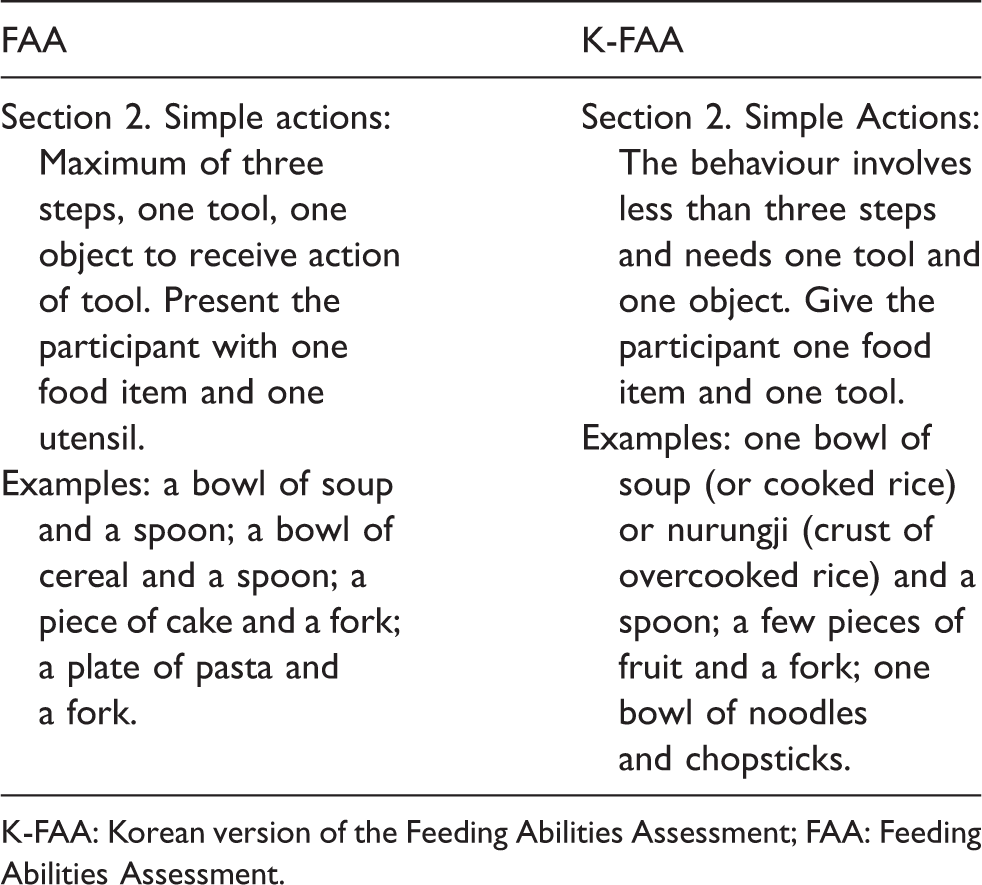
K-FAA: Korean version of the Feeding Abilities Assessment; FAA: Feeding Abilities Assessment.
Stage 2: Reliability analysis
Reliability was verified by testing the internal consistency, test–retest reliability and inter-rater reliability. The internal consistency was computed by analysing the K-FAA scores of 65 patients with dementia. Observation assessments on 20 patients with dementia were conducted twice with a one-week interval to determine test–retest reliability.
The entire study was carried out by one of the authors, and one occupational therapist partially participated in the analysis of inter-rater reliability. The tester had full knowledge about and received sufficient training on the evaluation tool. Inter-rater reliability was evaluated using a sample comprising 12 patients with dementia.
Results
The partcipants in this study included 65 patients, comprising 9 men (13.8%) and 56 women (86.2%). The average age of the subjects was 83.2 years. Most of the subjects had lived in an elderly facility less than two years. The general characteristics of the participants are presented in Table 3.
Subject characteristics (N=65).
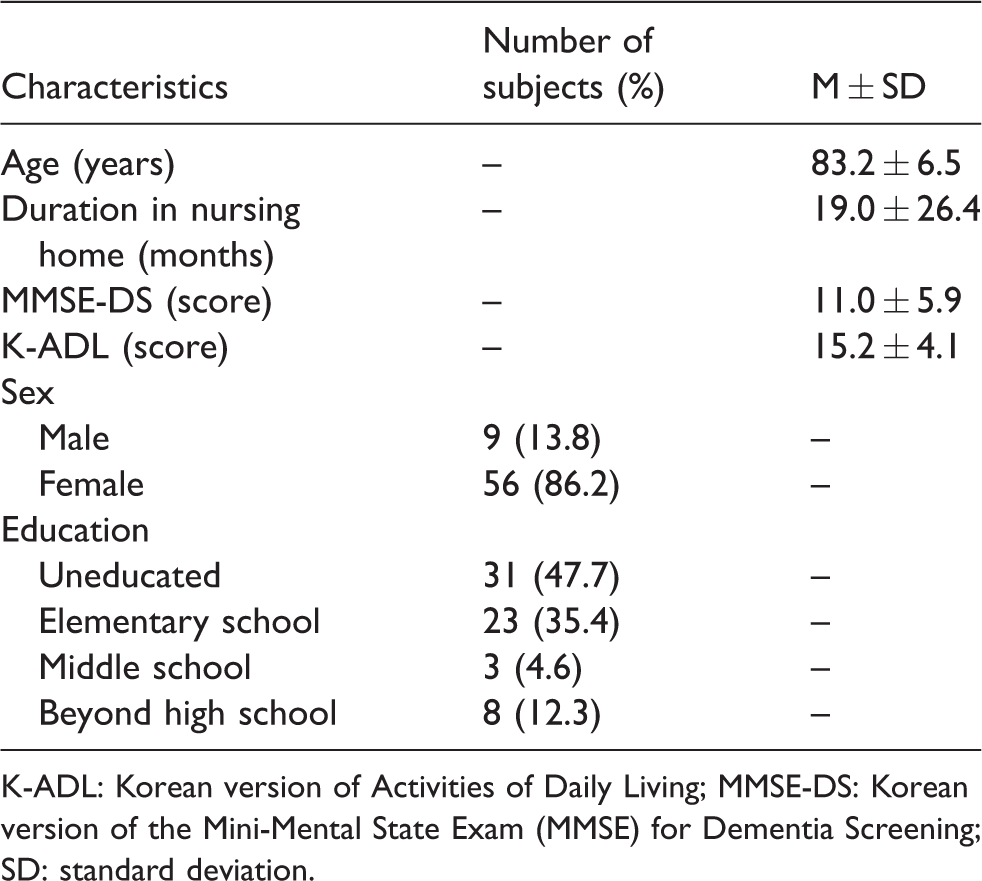
K-ADL: Korean version of Activities of Daily Living; MMSE-DS: Korean version of the Mini-Mental State Exam (MMSE) for Dementia Screening; SD: standard deviation.
Development of the K-FAA
We computed the content validity index (CVI) of the measurement items to assess content validity, which was confirmed with a CVI of over .70 on 32 items. The CVI of each item ranged between .70 and .85, and the total CVI of the K-FAA was .78.
Reliability analysis
Internal consistency
Cronbach’s α value of each item in the K-FAA ranged between .929 and .965, indicating high reliability (Table 4).
Cronbach’s α of the item was deleted from the K-FAA.
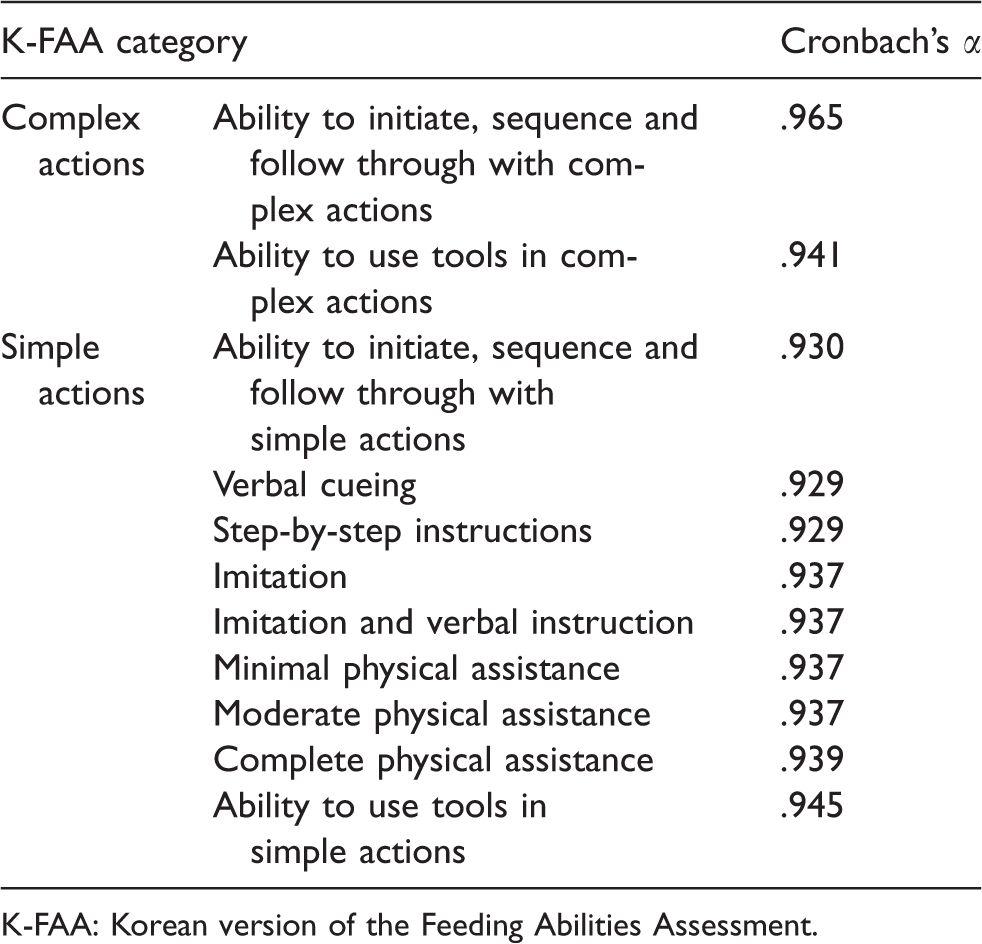
K-FAA: Korean version of the Feeding Abilities Assessment.
Test–retest reliability
To measure the test–retest reliability, we computed the correlation coefficient of the total K-FAA scores using the initial test score and the retest score and also, conducted a paired t-test (Table 5).
Test–retest reliability of K-FAA.
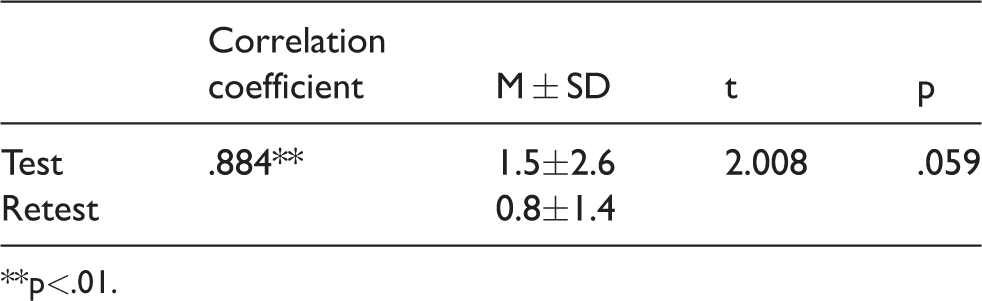
**p<.01.
The correlation coefficient between the initial test and the retest was .884, indicating good correlation that was statistically significant at a significance level of p < .01. The average K-FAA score was 1.5 ± 2.6 in the initial test and 0.8 ± 1.4 in the retest. The t-value was 2.008.
Inter-rater reliability
To test the inter-rater reliability, we computed the Kappa index and intraclass coefficient (ICC) of the total K-FAA scores of 12 patients with dementia who were evaluated by two occupational therapists.
The inter-rater coefficient was .800, implying good correlation that was statistically significant at a significance level of p < .005. The ICC value was .897, which also implies good correlation (Table 6).
Inter-rater reliability of K-FAA.
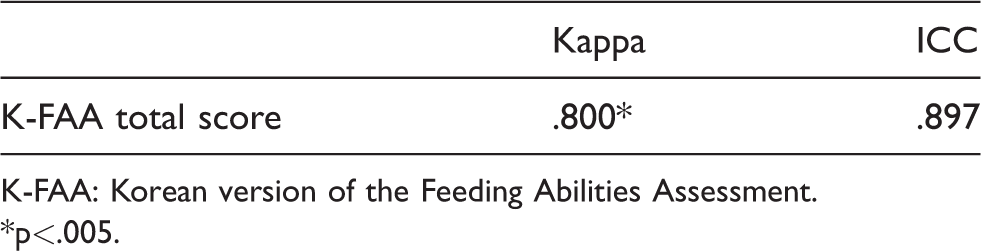
K-FAA: Korean version of the Feeding Abilities Assessment.
*p<.005.
Discussion
This study developed a K-FAA, which was devised to evaluate the feeding ability of patients with dementia, by adapting the items from the original FAA according to Korean culture and testing its reliability.
During the development of the K-FAA, the contents of the original tool were altered and supplemented considering local circumstances in Korea. Because the examples suggested by the original FAA refer to western meals, we needed to change the contents to foods that suit the Korean culture. Through discussion, the examples were changed to ‘one bowl of soup (or cooked rice) or nurungji (crust of overcooked rice) and a spoon’, ‘a few pieces of fruit and a fork’ and ‘one bowl of noodles and chopsticks’. The words ‘one bowl of soup and a spoon’ were uniformly used in the evaluation questions. Considering that cooked rice (porridge), soup and a side dish are universal in Korean-style meals, we believe that uniformly using soup in the all the items was appropriate.
The validity of the completed K-FAA was confirmed with the CVI value ranging between .70 and .85. This is consistent with previous studies where the CVI of each item ranged between 67% and 100% (LeClerc et al., 2004). In our study, content validity was tested by utilising diverse subjects comprising professors at the department of occupational therapy, occupational therapists and nurses. It is meaningful that the content validity of the FAA was confirmed among diverse occupations in the field of health and medicine.
The high internal consistency of the K-FAA that ranged between .929 and .965 implies that all items have strong consistency. The internal consistency of the K-FAA was similar to or higher than that of the original FAA (>.80). The original author suggested that if subjects could perform all items, they would obtain a score of zero, and that a consistent score could lead to a high internal consistency (LeClerc et al., 2004). Nevertheless, high internal consistency of the K-FAA in our study indicates the stability of the tool, considering that the internal consistency of another feeding-related evaluation tool developed in Korea was .888.
In the test–retest reliability check that used a sample comprising 20 patients with dementia, the coefficient was .884, which was similar to the results of the original FAA whose test–retest reliability was measured using a sample of 28 subjects (.75–1.00). In our study, the test interval was set at one week, and we implemented the test in identical environments during the same mealtime to minimize variables. The test results indicated high reliability.
The inter-rater reliability was also high, with a Kappa index of .800 and an ICC index of .897, which is supported by the Kappa index of the original author that was higher than .80. The high inter-rater reliability in our study can be attributed to the clinical inferential skill of one of the authors and the tester, as both were specialized in treating elderly patients with dementia and had five years of work experience in the field of occupational therapy.
This study has several limitations. First, because the sample comprised only those who lived in the metropolitan area, the study results cannot be generalized. Future studies will need to evaluate and present the assessment outcomes of the functional state of patients with dementia who live in diverse regions. Second, all the subjects who participated in this study were living in a nursing home. We could not evaluate the feeding ability of patients with dementia who live at home or in a hospital. Further studies should be conducted to present assessment outcomes according to the living environment of patients with dementia. Also, to compare the feeding abilities according to stage of dementia, future research should include subjects in various stages of dementia. Finally, patients with dementia experience functional loss as the disease progresses, including coordination problems during eating. Because the evaluation of patients’ skills in using eating tools is broad-based with the K-FAA, evaluating the feeding ability of all types of patients with dementia is difficult. Items that can evaluate the feeding ability of patients in the early, middle and end stages of dementia should be included in future evaluation tools.
Patients with dementia experience difficulties in continuous movement when using tools due to ideational apraxia (Jeong, 2009). The FAA was developed to evaluate the feeding performance ability of patients with dementia, rather than to evaluate the behavioural problems that occur during mealtimes. The FAA can evaluate patients’ skill in using tools or a series of continuous movements that occur during eating.
Considering the current situation in Korea, where tools for feeding-related evaluation are scarce, our study is significant in that we developed the K-FAA to evaluate the feeding ability of patients with dementia. In addition, the study was conducted among 65 patients with dementia to confirm the reliability of the K-FAA. We expect that the K-FAA can be useful in providing well-grounded data that can help maintain or compensate the feeding ability of patients with dementia.
Conclusion
This study developed and tested the reliability of a K-FAA to evaluate the feeding abilities of patients with dementia. The K-FAA was completed by first translating the original FAA, after which an expert committee performed content screening and cultural adaptation. The completed K-FAA was verified by a health and medical expert, and a CVI value between .70 and .85 was obtained. The reliability of the K-FAA was assessed by testing the internal consistency, test–retest reliability and inter-rater reliability. The test results indicated high reliability of the K-FAA: The internal consistency was over .929, the coefficient of the test-retest reliability was .884 and the inter-rater reliability of the Kappa index and the ICC was .800 and .897, respectively. We expect that the K-FAA can be used to evaluate the meal performance abilities of patients with dementia in clinical fields in Korea.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.