
Abstract
Background
Psychological factors have been reported to affect chronic pain and may lead to inactivity after total knee arthroplasty. This study aimed to determine whether the use of an activity diary for goal setting during occupational therapy would reduce pain, and improve psychological and physical performance in patients after total knee arthroplasty.
Methods
A total of 41 total knee arthroplasty participants from two cohorts were recruited in the study and allocated by convenience to either the experimental group using an activity diary (n = 20) or the control group (n = 21). Occupational therapy intervention (1–2 weeks postoperatively) to promote goal achievement was performed in both groups, and self-monitoring was performed in the diary group by using the activity diary. The outcome indices were Canadian Occupational Performance Measure, pain (resting pain, walking pain), pain catastrophizing (rumination, helplessness, and magnification), anxiety, depression, pain self-efficacy, and physical activity level. Data were evaluated by using analysis of variance analyses with post hoc tests.
Results
A time-by-group interaction emerged for Canadian Occupational Performance Measure, walking pain, pain catastrophizing, anxiety, depression, and physical activity level (p < 0.05), both favouring the diary group. The diary group also showed greater improvement in Canadian Occupational Performance Measure, walking pain, anxiety, and physical activity levels at four weeks postoperatively, compared to the control group (p < 0.05).
Conclusion
The use of the activity diary in this study increased occupational therapy effectiveness, reduced patients’ pain, and prevented a decline in physical performance. We believe that the use of an activity diary is an effective and feasible addition for total knee arthroplasty patients.
Keywords
Introduction
Based on an epidemiological survey regarding musculoskeletal chronic pain in Japan, the rate of complaints was 11.1%, and approximately 30% of patients with chronic pain have a history of morbidity ≥5 years; additional patients continue to receive treatment (Nakamura, Nishiwaki, Ushida, & Toyama, 2014). Because of significant increases in medical costs due to musculoskeletal chronic pain, as well as social losses, there is an increasing need to prevent musculoskeletal chronic pain.
Many musculoskeletal diseases that cause chronic pain are reported as lumbar diseases, with the exception of osteoarthritis of the knee. Total knee arthroplasty (TKA) may be the result of chronic pain in approximately 15% of cases (Ackerman, Graves, Wicks, Bennell, & Osborne, 2005). Despite surgical operation, urgent countermeasures are needed to prevent chronic pain and reduced physical activity. Negative psychological factors, such as anxiety, depression, and pain catastrophizing, etc., have been reported to affect chronic pain after TKA (Sullivan et al., 2011). However, self-efficacy is regarded as a positive psychological factor for mitigation of pain catastrophizing (Wylde, Dixon, & Blom, 2012). van den Akker-Scheek, Stevens, Groothoff, Bulstra, and Zijlstra (2007) reported that self-efficacy affected walking and pain after TKA. These prior studies indicated that pain catastrophizing, anxiety, and depression are related to chronic pain after TKA; and pain and self-efficacy are related to the restriction of activity levels.
We previously reported a relationship between Canadian Occupational Performance Measure (COPM) and pain catastrophizing after TKA (Hiraga, Hirakawa, Hisano, & Shiota, 2015). Notably, improvement in helplessness (i.e. helplessness in a painful situation) was recognised by occupational therapy (OT) practitioners after establishing the COPM goal in a quasi-randomised controlled trial (Hiraga, Hisano, Hirakawa, & Nomiyama, 2016). However, improvements were not observed in pain, rumination (i.e. attention to pain), or magnification (i.e. overestimation of pain threats) (Hiraga, Hisano, Hirakawa, & Nomiyama, 2017). Furthermore, it was not possible to examine effects on anxiety, depression, or physical activity in the prior studies. Therefore, it was necessary to develop OT treatment and practice protocols that addressed psychological factors for chronic pain after TKA.
There have been recent studies of interventions in which chronic pain patients wear pedometers to self-manage activity, thereby avoiding increases in pain and enabling them to record daily activities (Hirase et al., 2018; McDonough et al., 2013). We previously reported a case in which use of an activity diary together with OT resulted in improvement of pain, psychological factors, and activity levels; the protocol encouraged self-management of walking and pain (Hiraga et al., 2017). Importantly, it is necessary to clarify the effects of self-management with a daily activity record regarding pain, psychological factors, and activity levels.
Therefore, we investigated whether the use of an activity diary for goal setting during OT would reduce pain, and improve psychological and physical performance in patients after TKA.
Methods
Study design
This study comprised a non-randomised controlled trial. Patients were divided into: the diary group (OT plus activity diary) or control group (OT alone).
Ethical considerations
All participants provided informed consent, and the study design was approved by the appropriate ethics review board at Fukuoka Rehabilitation Hospital (FRH 2014-R-010).
Participants
Power analysis
We used G*Power 3 (Faul, Erdfelder, Lang, & Buchner, 2007) to perform preliminary test force analysis and estimate the required sample size. The power was set at 0.8, and the significance level (α) was set at 0.05 (Cohen et al., 1992). Effect size was set at 0.25, which constitutes a moderate standard for two-way analysis of variance. The power analysis indicated that 24 patients (12 per group) were required for pre- and post-evaluations.
Target participants
Inclusion criteria were TKA performed between May 2014 and September 2016 in Fukuoka Rehabilitation Hospital (Fukuoka, Japan); 45 patients were evaluated. Patients hospitalised May 2014–June 2015 were assigned to the control group; those hospitalised July 2015–September 2016 were assigned to the diary group. Exclusion criteria included diagnosis of dementia and obvious mental illness (e.g. depression) that would interfere with completion of the questionnaire, as well as refusal to participate in OT. Additional exclusion criteria comprised postoperative complications (e.g. nerve injury and deep vein thrombosis), other significant medical diseases interfering with postoperative rehabilitation, previous TKA (TKA of the opposite limb and revision), and TKA performed for causes other than degenerative diseases (e.g. rheumatoid arthritis and bone necrosis). Two of the 45 patients were excluded, resulting in a total of 43 TKA patients from two cohorts; these patients were allocated by convenience to either the experimental group using an activity diary (n = 21, four males, 17 females; age: 76.1 ± 7.1 years) or the control group (n = 22, two males, 20 females; age: 76.4 ± 5.4 years).
All patients received general anaesthesia; non-steroidal anti-inflammatory drugs were administered at a dose of 60 mg (three tablets per day) for two weeks postoperatively. All patients followed the same physical therapy and OT protocols after operation. All patients began physical therapy, including knee joint range of motion exercises (flexion–extension) and stretching, on the first day postoperatively. OT began at 1–2 weeks postoperatively for the purpose of improving everyday life. Patients were discharged upon the physician’s approval and on patient request at four weeks postoperatively.
OT for each group: Goal setting and practice
We used a previously reported method (Hiraga et al., 2016) for goal setting and practice in the diary and control groups at 1–2 weeks after surgery. The implementation procedure used COPM (Law et al., 1990) to list five target goals and determine the priority of the goals. After determining the priority order, we evaluated the performance of each goal with a 10-point scale (1: not possible; 10: very good). Satisfaction was also evaluated on a 10-point scale (1: not satisfied; 10: very satisfied). Performance and satisfaction scores were determined for each factor.
In practice, the patient may write, ‘I want to be able to do the clean-up’. The patient starts with a low load, such as standing position, progresses to movement, and then practices using what is necessary for cleaning. Ultimately, this practice encourages the patient to achieve the goal in cleaning. All OT interventions required 40 min per day.
OT using the activity diary
We used an activity diary developed by Fukuoka Rehabilitation Hospital for intervention in the diary group (Hiraga et al., 2017) but not in the control group. The activity diary was designed to record date, steps, and pain (11 items) daily; this facilitates achievement of activity goals while encouraging active self-management. A pedometer (Pleasure Walker PZ-150; Yamasa Co., Ltd, Tokyo, Japan) was used to record the number of steps per day; the pedometer was attached to the foot of the non-operative side. Previous studies have reported that a pedometer attached to the foot is superior to a pedometer worn on the wrist for detecting the amount of activity (Rhudy & Mahoney, 2018). In addition, we focused on improving activity, rather than solely evaluating pain. Pain levels and comments were recorded in the activity diary, and we implemented a feedback protocol to enable patients to experience achievement. For example, if a patient commented, ‘I am in pain every day’, we asked ‘why do you have knee pain?’ ‘How can this be done easier?’. This feedback protocol was implemented to shift from negative to positive comments. Such intervention was incorporated into the OT programme of 40 min/day. Use of the activity diary began on Day 1 at the start of OT (Figure 1).
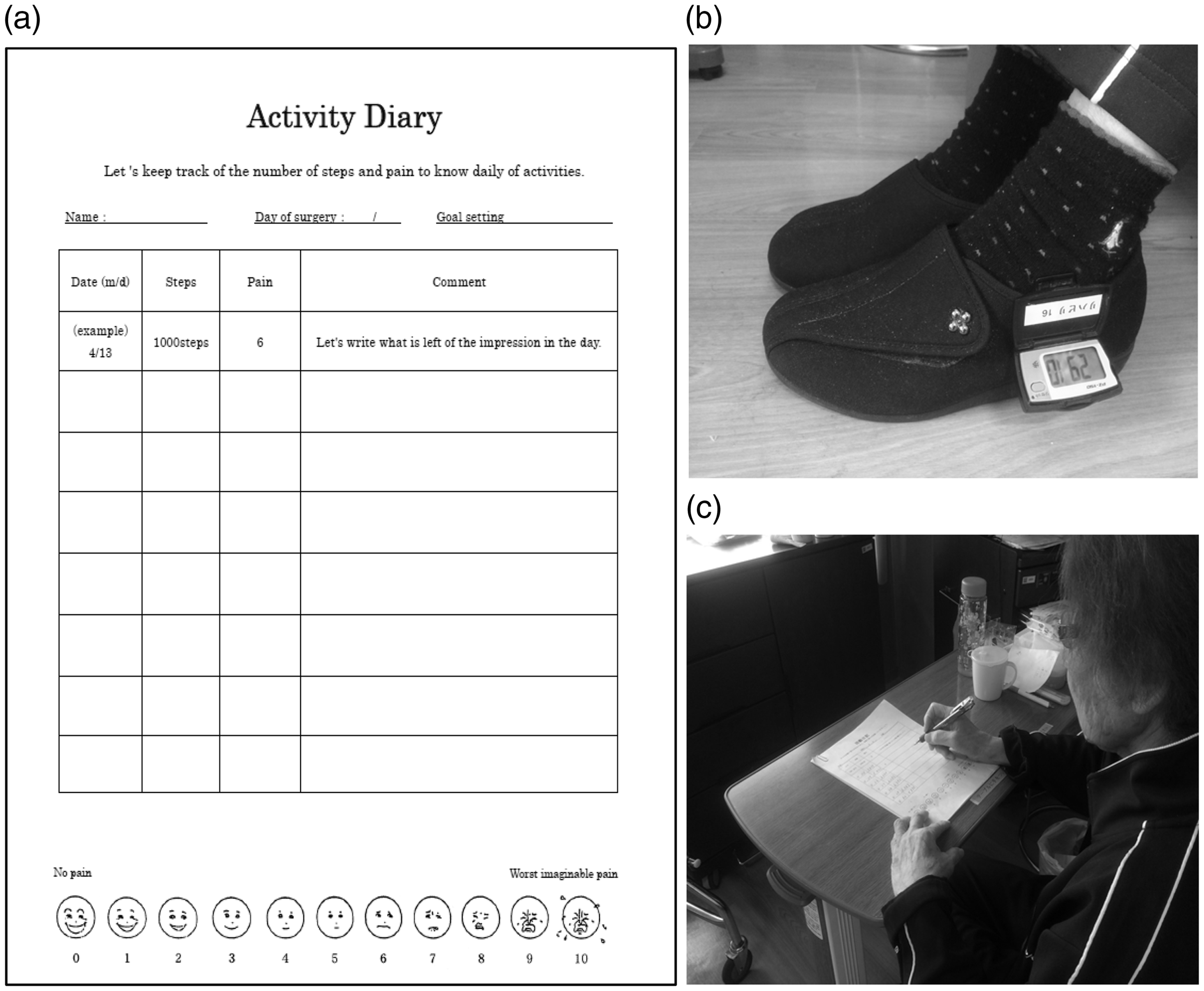
Activity diary. (a) Self-management was accomplished by recording the number of steps, evaluation of pain, and comments; (b) pedometer attached to the foot on the non-operative side; and (c) recording in the activity diary.
Assessment
The assessment was performed pre-OT (1–2 weeks postoperatively) and post-OT (4 weeks postoperatively).
Pain
The numerical rating scale (NRS) (Jensen, Turner, & Romano, 1994) was used to evaluate pain on an 11-point scale (0: no pain; 10: worst imaginable pain). Resting and walking pain were both assessed on the NRS.
Pain catastrophizing
The Pain Catastrophizing Scale (PCS) (Sullivan, Bishop, & Pivik, 1995) was used to evaluate pain catastrophizing. The PCS comprises 13 items and uses self-evaluation on three subscales: rumination, helplessness, and magnification. The patient evaluates the time spent on the condition on a five-point scale (0: not at all; 4: all the time). A high score indicates strong pain catastrophizing.
Anxiety and depression
The Hospital Anxiety and Depression Scale (HADS) (Zigmond & Snaith, 1983) was used to evaluate anxiety and depression; HADS comprises 14 questions. The patient evaluates anxiety and depression, and how much time is spent in that state, on a four-point scale (0: not at all; 3: most of the time). HADS subscale scores were also evaluated in this study.
Pain self-efficacy
The Pain Self-Efficacy Questionnaire (PSEQ) (Adachi et al., 2014) was used to evaluate self-efficacy for pain. PSEQ uses self-entry of scores for 10 items on a seven-point scale (0: not at all confident; 6: completely confident).
Physical activity levels
An activity meter (Active Style Pro; OMRON Corp., Kyoto, Japan) was used to evaluate physical activity. The activity meter was worn on a patient’s foot for 24 hours. Steps and physical activity were measured, and times for metabolic equivalents were calculated in minutes for physical activity. Previously, Ohkawara et al. (2011) found high reliability in the calculation of steps and physical activity levels using the Active Style Pro.
Statistical analysis
We used t-tests to evaluate significant differences in age, body mass index (BMI), and hospital inpatient days. We used Chi-squared tests for group comparisons in demographics such as gender, employment, smoking, and drinking. We analysed the effects of the intervention protocol on outcome measures using a 2 × 2 (time (baseline and pre- to post-OT) × group (diary and control groups)) analysis of variance. Post hoc Bonferroni tests were used for specific comparisons, and two-sided significance was determined. Statistical analyses were performed with IBM SPSS Statistics Version 22 (IBM Corp., Armonk, NY, USA).
Results
Figure 2 presents a flow chart outlining participation in this study. In total, 45 participants were screened for enrolment, and two failed to meet the inclusion criteria (n = 2). We enrolled the remaining 43 participants in the study and non-randomly allocated each patient to either the activity diary group (n = 21) or the control group (n = 22). One patient from each group withdrew from the trial and could not be evaluated. A total of 20 patients in the diary group and 21 patients in the control group completed the study. All patients in the diary group completed the pain, number of steps, and comment categories of the diary.
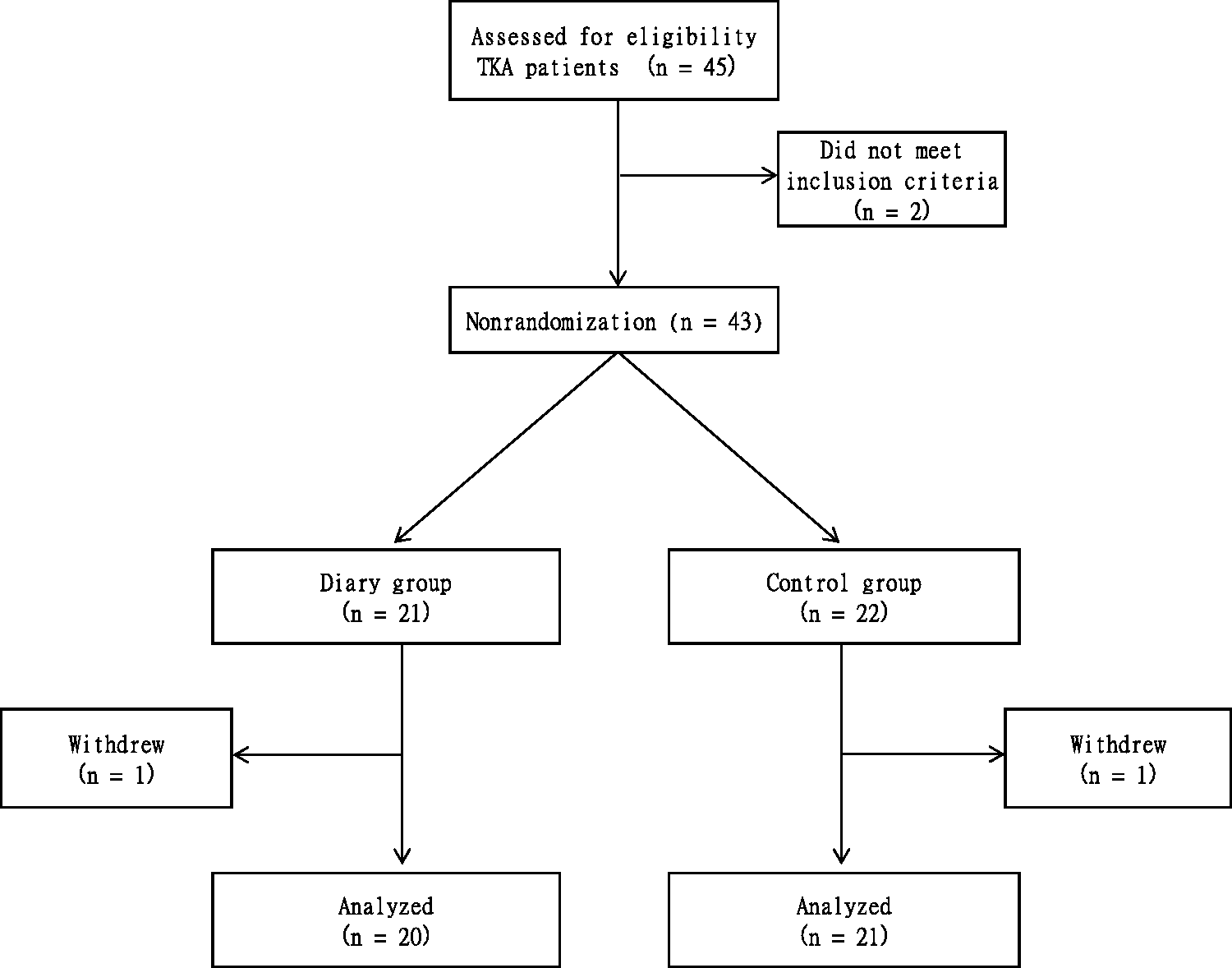
Patient recruitment and flow through study. TKA: total knee arthroplasty.
Baseline characteristics
Table 1 summarises the baseline characteristics of patients. There were no significant differences in age, sex, BMI, employment, smoking, drinking, goal setting, pain intensity, psychological status, or physical activity between the two groups.
Baseline characteristics of patients, by group.
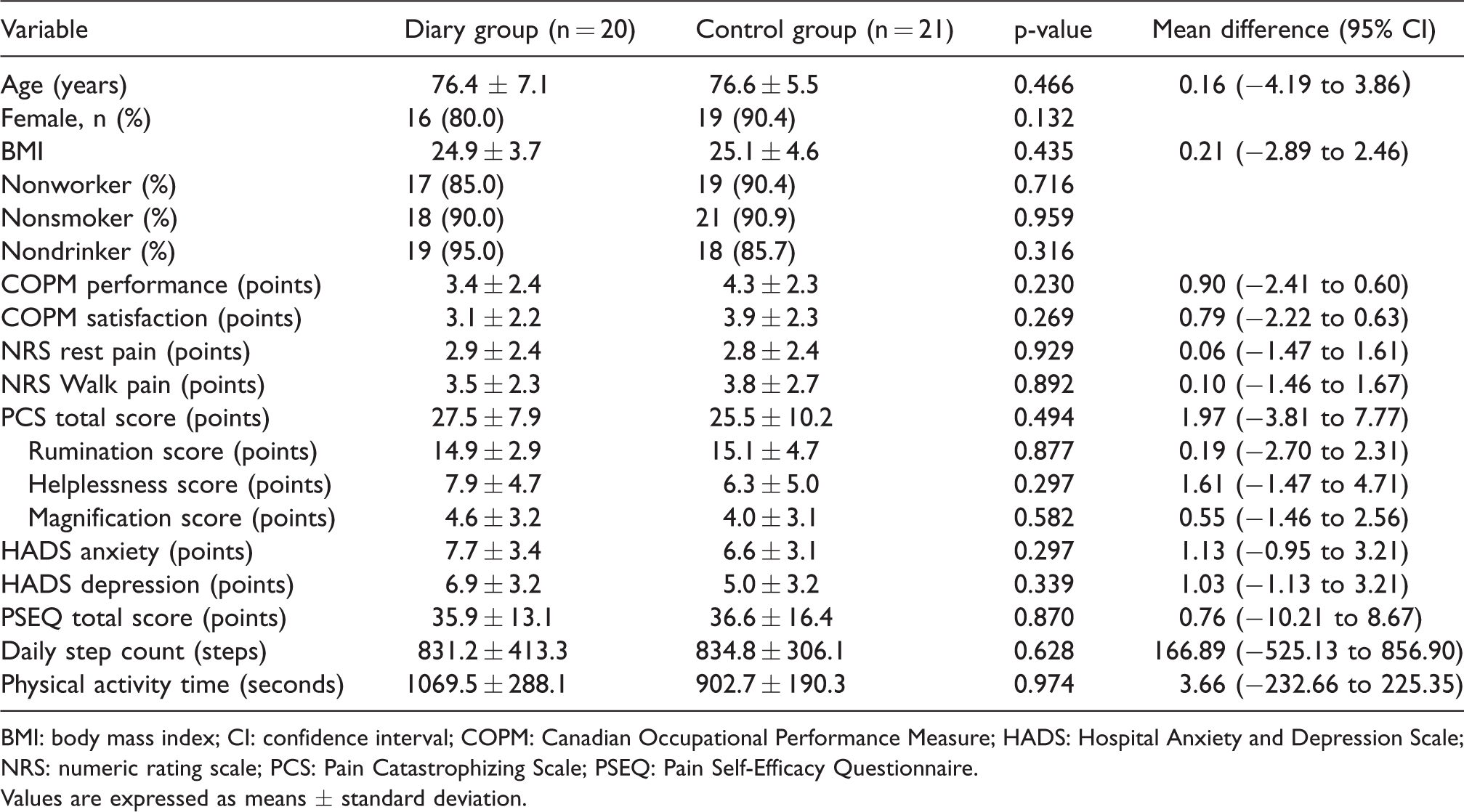
BMI: body mass index; CI: confidence interval; COPM: Canadian Occupational Performance Measure; HADS: Hospital Anxiety and Depression Scale; NRS: numeric rating scale; PCS: Pain Catastrophizing Scale; PSEQ: Pain Self-Efficacy Questionnaire.
Values are expressed as means ± standard deviation.
Length of hospital stay
The length of hospital inpatient stay was significantly better for the diary group than for the control group (31.4 ± 4.6 days versus 40.8 ± 13.0 days; p = 0.002).
Diary group and control group effects
Figure 3 presents the progress of activity diary use on daily step count and pain (11 items). Table 2 presents the interaction between the groups (time (baseline and pre- to post-OT) × group (diary and control groups)). There were no significant differences between group measurements for the diary and control groups in NRS rest pain score, PCS rumination score, PCS helplessness score, or PSEQ total score.
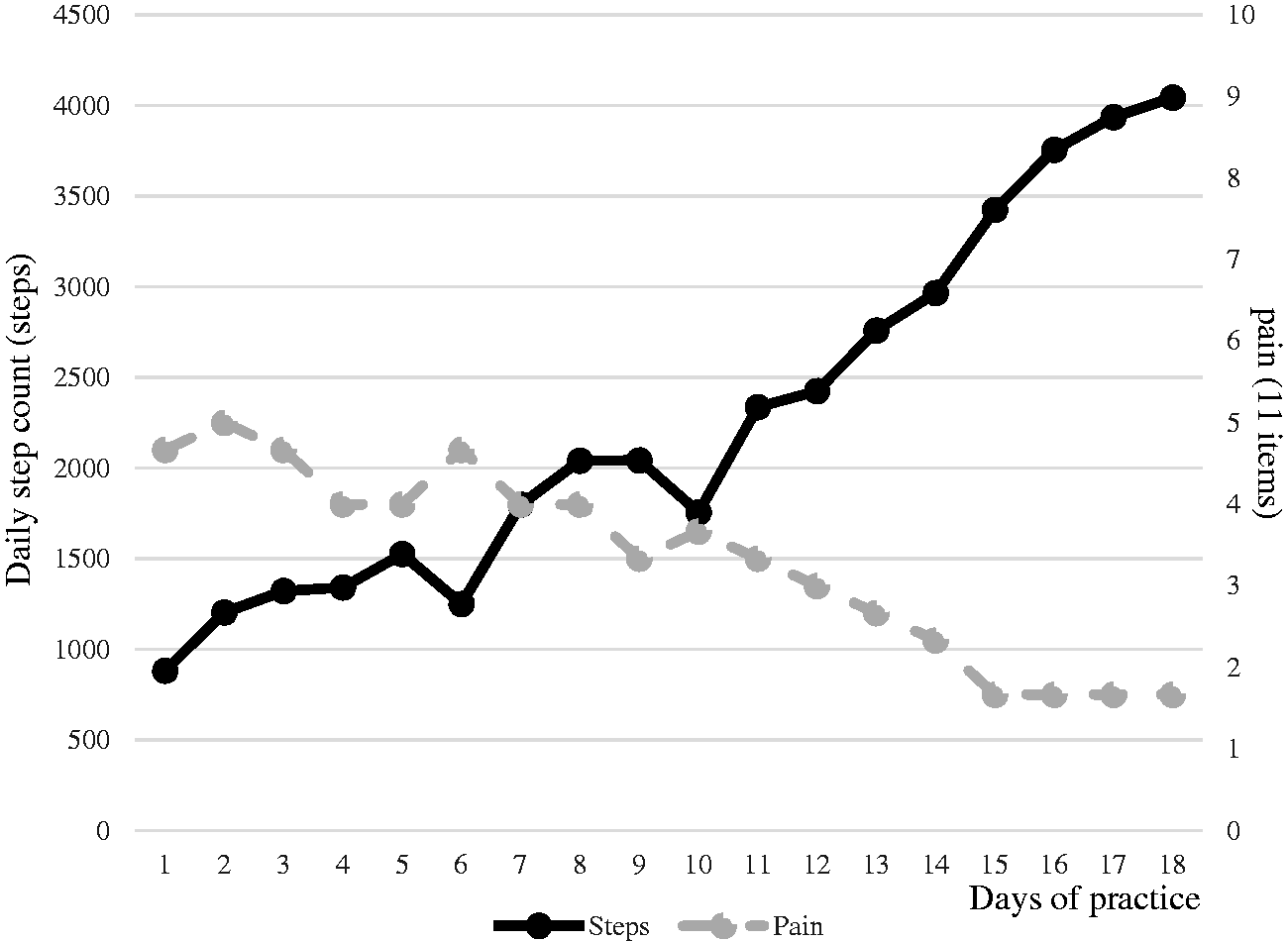
Record of OT using an activity diary. The combination graph shows the trends of mean step count and mean pain over 11 steps in the diary group.
Pre- and post-OT outcomes, by group.
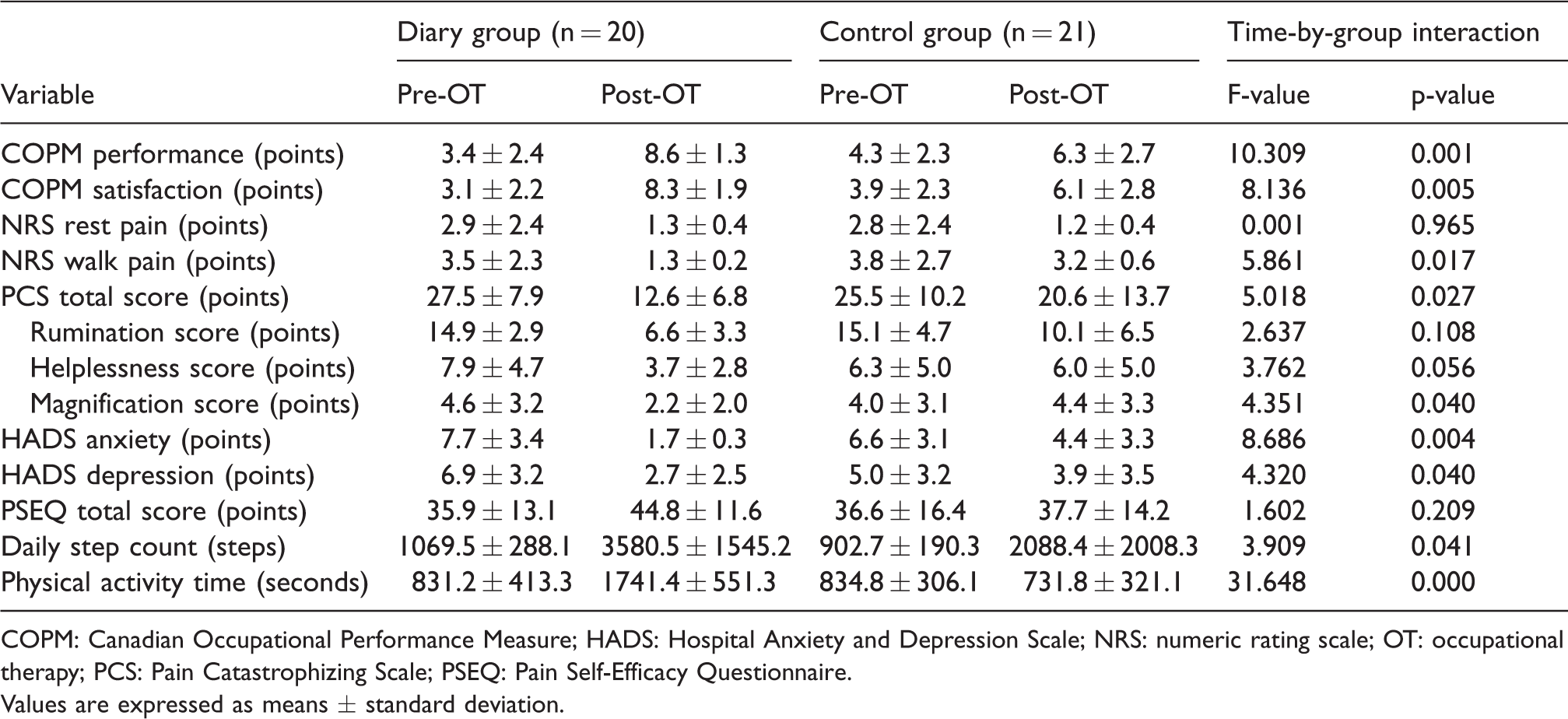
COPM: Canadian Occupational Performance Measure; HADS: Hospital Anxiety and Depression Scale; NRS: numeric rating scale; OT: occupational therapy; PCS: Pain Catastrophizing Scale; PSEQ: Pain Self-Efficacy Questionnaire.
Values are expressed as means ± standard deviation.
Diary group effects
Table 3 presents the results of outcome measurements in the diary and control groups. The mean COPM performance and satisfaction scores post-OT were significantly better for the diary group than for the control group (COPM performance: 8.6 ± 1.3 for the diary group versus 6.3 ± 2.7 for the control group, p = 0.001; COPM satisfaction: 8.3 ± 1.9 for the diary group versus 6.1 ± 2.8 for the control group, p = 0.007). Within the diary group, the mean COPM performance and satisfaction post-OT scores improved significantly over those of the pre-OT values (p = 0.000 and p < 0.000, respectively). The mean NRS walking pain score post-OT was significantly better for the diary group than for the control group (1.3 ± 0.2 versus 3.2 ± 0.6; p = 0.010). Within the diary group, the mean post-OT score improved over the pre-OT score (p = 0.001). The mean HADS anxiety score post-OT was significantly better than for the diary group than for the control group (1.7 ± 0.3 versus 4.4 ± 3.3; p = 0.031). Within the diary group, the mean post-OT score improved over the pre-OT value (p = 0.005). The mean daily step counts and physical activity time post-OT were significantly better for the diary group than for the control group (daily step count: 3580.5 ± 1545.2 versus 2088.4 ± 2008.3, p = 0.013; physical activity time: 1741.4 ± 551.3 versus 731.8 ± 321.1; p = 0.000). Within the diary group, the mean post-OT values improved over the pre-OT values (p = 0.000).
Multiple comparisons of diary and control groups.
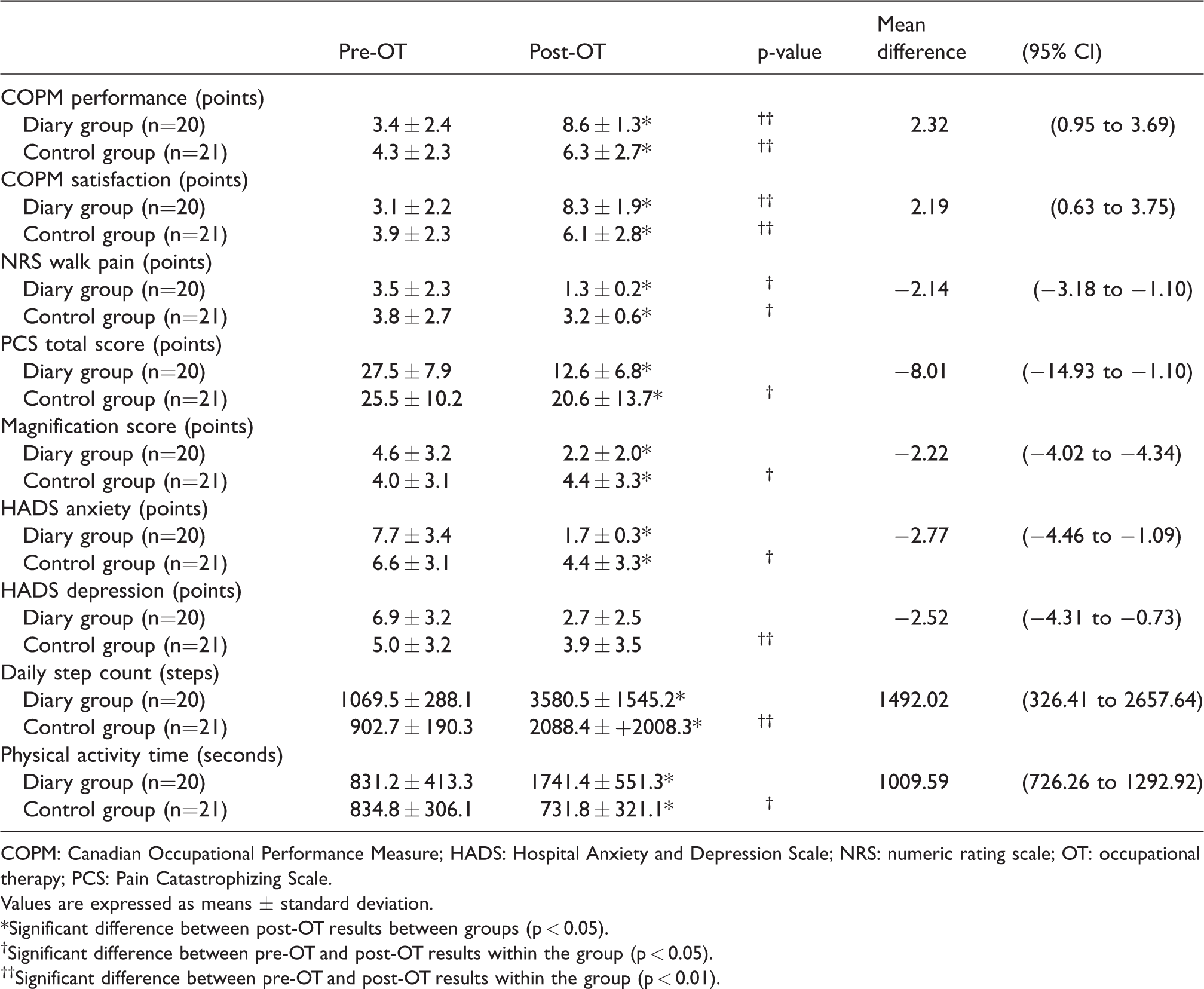
COPM: Canadian Occupational Performance Measure; HADS: Hospital Anxiety and Depression Scale; NRS: numeric rating scale; OT: occupational therapy; PCS: Pain Catastrophizing Scale.
Values are expressed as means ± standard deviation.
*Significant difference between post-OT results between groups (p < 0.05).
†Significant difference between pre-OT and post-OT results within the group (p < 0.05).††Significant difference between pre-OT and post-OT results within the group (p < 0.01).
Discussion
In this study, we examined the effects of using an activity diary during OT on pain, psychological factors, and physical activity after TKA. Post hoc tests in the diary and control groups revealed within-group (diary group) and between-group improvements in COPM performance score, COPM satisfaction score, NRS walking score, HADS anxiety score, daily step counts, and physical activity time. Therefore, OT that included an activity diary was found to be beneficial for patients after TKA. It is also meaningful that the number of days in the diary group was shorter than that of the control group.
Harkin et al. (2016) reported on the use of an activity log and found that when goals were set and progress was recorded, achievement was increased and additional goals were formed. Furthermore, use of education incorporating self-management showed that length of stay in hospitals were reduced (Yoon et al., 2010). In addition, Seminowicz et al. (2013) reported that feedback resulted in improvement in positive emotion, pain catastrophizing, and mental health. Based on these studies, reporting negative comments such as stubborn pain in the comment section of an activity diary can result in improvement of activity levels and achievement of goals. If consciousness changes from positive emotion to positive activity levels, improvement can be observed in the HADS anxiety score. Furthermore, the length of hospital stay was shortened. However, deterioration in physical activity was observed in the control group, which may be related to the possibility of falling, particularly these patients may have exhibited fear avoidance (Vlaeyen & Linton, 2000).
A previous study (Somers et al., 2012) demonstrated improvement in pain self-efficacy after education and pain self-management programme at 24 weeks postoperatively among knee osteoarthritis patients. The present study did not show any effects of activity diary use on pain self-efficacy. This is likely because the course of OT practice with the activity diary was limited to two weeks. However, use of the activity diary produced various significant effects within a relatively short period of time. This study directed patients in the diary group to use the activity diary for self-management, in order to achieve an established goal in physical activity and pain management. We found that the performance score, satisfaction score, NRS walking score, HADS anxiety score, daily step counts, and physical activity time had been improved with use of the activity diary in the OT protocol.
The limitations of this study are that it was a longitudinal study with a non-randomised design. The long-term effects of using activity diary on activity limitation after chronic pain remain unknown as this study only examined short-term effects. Furthermore, the history effects of physical therapy and medication therapy were not considered, and future studies must investigate those factors.
Conclusion
Our OT programme was previously shown to be effective in improving psychological factors in Japanese TKA patients. Use of the activity diary in this study increased the effectiveness, reduced patients’ pain, and prevented a decline in physical performance. The OT programme and activity diary were also well accepted by TKA patients in this study. We conclude that the use of an activity diary is an effective and feasible addition for TKA patients.
Footnotes
Acknowledgments
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.