
Abstract
Introduction
Cognitive difficulties have been reported to have the greatest effect on function and quality of life in people with multiple sclerosis, affecting 50–60% of people. To date, few interventions have been developed to treat cognitive issues in multiple sclerosis. Here we report on a Cognitive Occupation-Based programme (COB-MS) for people with Multiple Sclerosis an evidence-based intervention to address everyday problems encountered due to cognitive difficulties. The aim of this research was to explore the views of people with multiple sclerosis and occupational therapists on the programme and its potential implementation in practice.
Methods
Data were elicited from a purposive sample of 12 people from two stakeholder groups, people with multiple sclerosis (n = 5) and occupational therapists (n = 7), through focus groups and interviews. The programme and related materials were presented, and contributions recorded, transcribed and thematically analysed.
Results
Two main themes were identified from analysis of the data: response to the intervention and challenges to implementing the programme. Occupational therapists agreed that the COB-MS is client-centred. People with multiple sclerosis thought that it was a validating intervention. The overall format was viewed to be useful and feasible.
Conclusion
The COB-MS for people with Multiple Sclerosis is the first known cognitive intervention using an occupation frame of reference to address difficulties faced among persons with multiple sclerosis and was found to be timely and relevant to the needs of the population.
Introduction
Rehabilitation with people with multiple sclerosis (MS) comes with unique considerations such as the fluctuating nature of the disease, patient fatigue and emotional and psychological well-being of the individual (Siepman et al., 2008). Difficulties with cognition have been reported to be present in 50–60% of people with MS (Amato, Zipoli, & Portaccio, 2006). ‘Cognitive rehabilitation is a process whereby people [with cognitive difficulties] work together with health professionals to remediate or alleviate cognitive deficits’ (Wilson, 1996, p. 637). To date however, there is a paucity of evidence as few programmes have been developed for people with MS that decrease the detrimental effects of impairment, and support patients by helping them to function well in everyday life (Rosti‐Otajärvi & Hämäläinen, 2014).
In two Cochrane systematic reviews, one in memory rehabilitation in MS (das Nair, Martin, & Lincoln, 2016) and one in neuropsychological rehabilitation in MS (Rosti‐Otajärvi & Hämäläinen, 2014), the authors found either no evidence (number of included studies = 8) or low level evidence (Rosti‐Otajärvi & Hämäläinen, 2014; number of included studies = 20) that rehabilitation reduces cognitive symptoms in MS. Despite the findings from individual studies being generally positive (in 18 of the 20 studies included), the pooled results of a meta-analysis by Rosti‐Otajärvi and Hämäläinen (2014) suggest that the effectiveness of cognitive rehabilitation for people with MS is far from conclusive. The included studies used computerised training, external aids and compensatory strategies, supporting awareness of cognitive deficits through education and awareness or a combination of these. The conclusions of these reviews were based on the limited quality of the research that is available. Both reviews emphasised a need for more robust randomised controlled trials (RCTs) that are of strong methodological quality in the area before any firm conclusions can be made on the possibility of improving functioning through cognitive-directed interventions.
Goverover et al. (2018) updated the review by O’Brien, Chiaravalloti, Goverover and DeLuca (2008) where they noted substantial progress has been made in the area of cognitive rehabilitation in MS since the initial review was published (40 studies included). They conclude that much work has yet to be done to develop the best evidence base for cognitive rehabilitation in MS. Methodological rigour and strong design are essential components to developing the evidence base in the area. Khan and Amatya (2017) carried out a systematic review of systematic reviews in the area of rehabilitation in MS. Though, not specifically looking at cognitive rehabilitation they also found that overall there is a lack of high quality evidence for a range of rehabilitation techniques in MS and that evidence is inconclusive in many areas, including cognitive rehabilitation. The authors found ‘low-quality’ evidence for occupational therapy interventions for participants with MS (96 trials) and in the area of cognitive rehabilitation (32 RCTs). Here authors again conclude that more rigorous trials are needed.
In contrast, das Nair and Lincoln (2013) found evidence that group-based memory rehabilitation improved insight and acceptance. The findings indicate that there are positive impacts on daily life, mood, fatigue and quality of life of cognitive rehabilitation that are being captured through qualitative means, but not quantitatively.
O’Brien et al. (2008) recommend that research should focus on function and context and aim to generalise to daily life and not be domain-specific. New interventions should aim to increase participation (O’Brien et al., 2008) and have outcomes that measure impact on daily living (O’Brien et al., 2008; Rosti‐Otajärvi & Hämäläinen, 2014). Rosti‐Otajärvi and Hämäläinen (2014) also recommend that all future studies should have a clear aim that is determined before beginning and the primary outcome should reflect this. They also suggest detailed reporting of the content of the intervention. Khan and Amatya (2017, p. 365) call for intervention that ‘engage, educate and empower patients’. Findings and recommendations from this summarised review of the literature provide strong rationale for the development of the cognitive occupation-based programme for people with multiple sclerosis (COB-MS) given the marked clinical treatment gap.
From the recommendations provided and the evidence that exists to date there is a clear need for a new individualised cognitive intervention that is measured by and taught through occupational participation, meaning that the focus will be on daily life activities such as self-care, productivity and leisure. The focus of the COB-MS is on managing daily life, employment and community engagement using routines, compensatory strategies and streaming demands. The emphasis is on helping people to participate more effectively in the daily occupations that they find difficult due to their cognition. The programme is an adapted version of an intervention that was designed and used as part of a computer-based training programme for older people that included instructional videos (Hynes, 2016). The instructional videos (Hynes, 2016) were transcribed and included in the handbook and the content was then modified for use with people with MS. Many of the successful aspects of previous research with people with MS (e.g. Chiaravalloti, DeLuca, Moore, & Ricker, 2005) and other populations (e.g. people with brain injury; Levine et al., 2000) were incorporated into the intervention. A preliminary version of the COB-MS, including facilitator handbook detailing the intervention and handbook for people with MS, was thus developed. This new programme has yet to be used with chronic conditions.
Following the MRC guidelines for developing and evaluating complex interventions (Craig et al., 2008) the first step is ‘Development’ which includes identifying the evidence base and appropriate theory and evaluating facilitators and barriers to implementation and acceptability of the intervention. Only following this should feasibility or pilot testing in future trials take place. To support this, we undertook a consultation process with occupational therapists and people with MS to elicit their views on the proposed intervention. In particular, we set out to answer the following research questions:
Is the COB-MS an acceptable intervention for people with MS and occupational therapists? What are the facilitators and barriers of the potential implementation in practice of the COB-MS for occupational therapists working with people with MS?
Method
This is a qualitative descriptive study. This design was chosen as it is suitable for obtaining straight and largely unadorned answers to questions of special relevance to health care practitioners (Sandelowski, 2000) including the development and acceptability of a new intervention such as the COB-MS. A generic qualitative approach was taken here as it was not guided by explicit assumptions (Kahlke, 2014).
Participants
Non-probability purposive sample was chosen for this study. Recruitment of people with MS was through the local Multiple Sclerosis Clinic. Posters were hung in the reception area of the MS clinic. The study was also promoted through the local chapters MS Society of Facebook Page. Researchers had no access or involvement in promoting the study through Facebook – this was done by the Community Services Coordinator. Participants contacted researchers if they were interested in taking part. Occupational therapists were recruited through an E-blast that was sent to clinicians working in the area. Clinicians then contacted researchers if they were interested in taking part. Written informed consent was obtained from all participants. Ethical approval for the study was provided by the University of British Columbia Behavioural Research Ethics Board (H15-02333).
Participants with MS were eligible if they were: (1) 19 years or older, (2) fluent in written and spoken English, (3) diagnosed with MS, (4) reported cognitive difficulties (this was not assessed by the researcher unless there was a need to assess capacity), (5) clinically stable, and (6) living in the community. People with MS were excluded if they had cognitive difficulties that would affect reliable participation or capacity to give informed consent. Guidelines from the British Psychological Society (2008) were followed in relation to capacity assessment. There was no need to assess capacity for anyone who self-selected for the study.
Occupational therapists were eligible to participate if they were: (1) working clinically at the time of the study, (2) agreed not to distribute the COB-MS material and return it following interview, and (3) had clinical experience with people with MS or people with cognitive difficulty of a minimum of one year.
Data collection
Both interviews and focus groups were used to explore participants’ views on the COB-MS. Interviews were used with occupational therapists due to difficulties scheduling a focus group with this group. A focus group was used with participants with MS. This type of health care consultation is being used more frequently to develop interventions with people with various health conditions, including people with cognitive difficulties such as dementia (Hynes et al., 2015). Focus groups were chosen as group members build off each other’s responses leading to more in-depth answers.
Participants with MS received a hard copy of the COB-MS handbook at least seven days before the focus group took place. They were asked to read the handbook and make any relevant notes prior to the focus group and take these to the group. During the focus group the facilitator followed a topic guide (see Appendix I) to elicit the views of participants on the COB-MS programme. Both authors were present at the focus group, one facilitated the group (SMH) and the other took field notes (SF) and was available to support members if required. The focus group lasted for one hour. Both researchers are occupational therapists and have experience of conducting focus groups. The programme was first explained in detail and discussion around its content and that of the handbook were recorded. Topics covered included impressions of the COB-MS, what they liked/disliked and thought was missing from the programme. Specific questions about the handbook were also covered. The discussion was flexible and led by the participants. Field notes were taken and the session was audio recorded. The group recordings were transcribed and analysed and no identifying names or details were included in the transcription.
Occupational therapists who met the inclusion criteria were provided with the facilitator COB-MS handbook. They were also given detail of the project either by phone or by email and had at least seven days to read the handbook before being contacted for a semi-structured interview. Participants were able to complete the interview by phone if it was not possible to interview in person. The interview followed a semi-structured format, lasting about 30 min, and used a pre-defined topic guide (see Appendix II). Occupational therapists were asked for their views on the feasibility of the programme and the usefulness and relevance of the content of the handbook. Any changes suggested were noted and interviews were audio recorded and transcribed.
COB-MS programme
The COB-MS programme consists of eight sessions – two individual and six group-based. Session one involves an initial visit with an occupational therapist who explains the programme in more detail and helps the participant set some personal goals. There are then six once-weekly group sessions with a small group (between five and eight people). The group sessions are then be followed by individual sessions that take place two weeks after the last group session.
The focus of the COB-MS is on managing the demands of employment and daily life by using compensatory strategies, routines and learning new techniques that can be integrated into daily occupations and contexts in order to make it meaningful to the participant. The programme takes a three-pronged approach to cognitive rehabilitation, using education, remediation and adaption to help people meet their goals while managing their cognitive challenges. Cognitive challenges in MS usually consist of deficits in complex attention; slowed processing speed; and problems with information processing, executive functioning and long-term memory (Chiaravalloti & DeLuca, 2008). The programme is informed by The Person–Environment–Occupational Performance model (Christiansen et al., 2011). Table 1 summarises the content of each of the 60 min sessions.
COB-MS sessions.
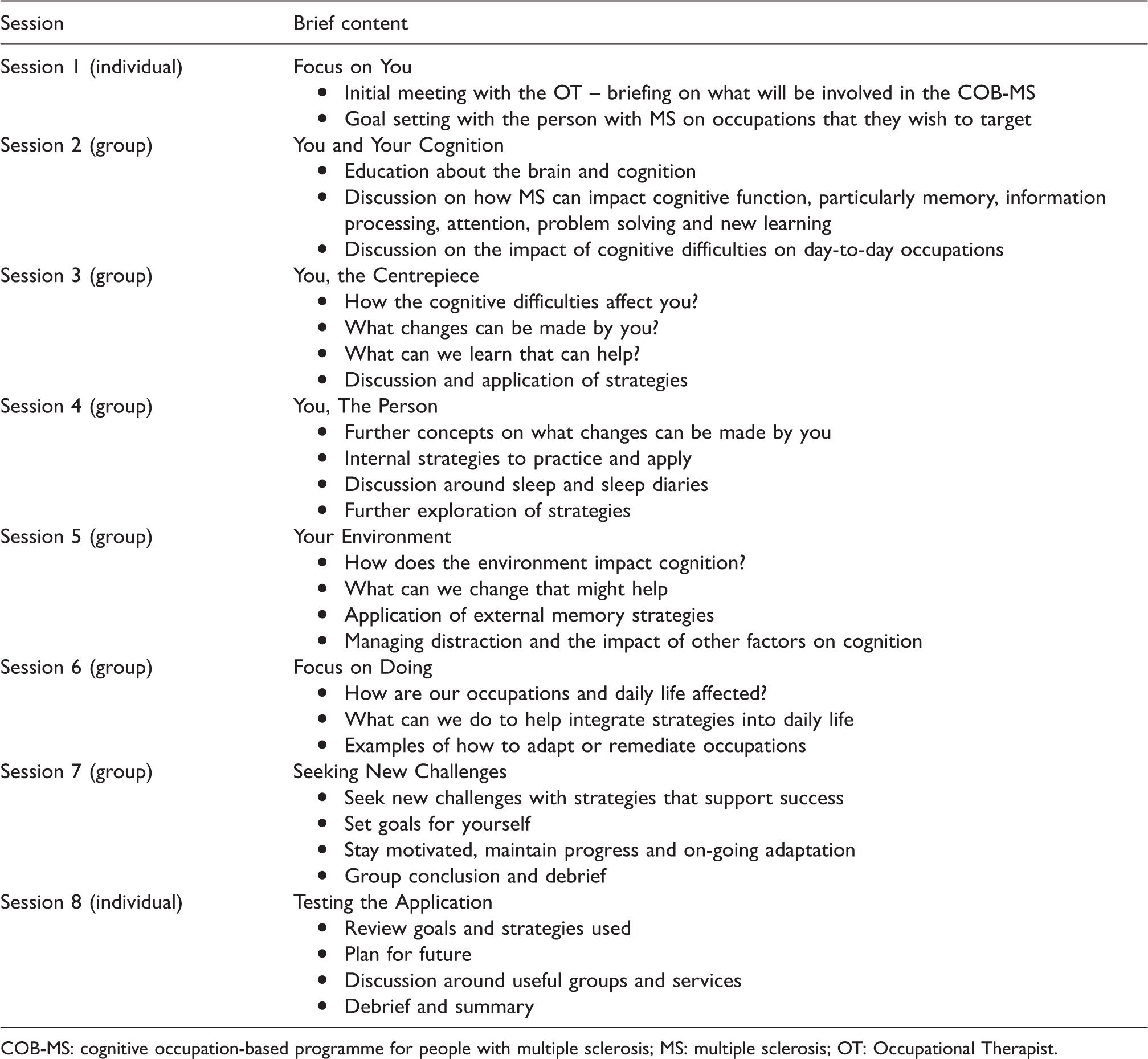
COB-MS: cognitive occupation-based programme for people with multiple sclerosis; MS: multiple sclerosis; OT: Occupational Therapist.
The handbook that was provided to people with MS and occupational therapists was approximately 125 pages in length. It contained detailed information on what is covered in the COB-MS sessions. The exercises, activities and strategies that are covered in the programme are available in the handbook to practice and apply.
Analysis
An inductive approach was taken to data analysis. The audio recordings were transcribed by an individual outside of the research team and the transcripts were then checked for accuracy by the lead author (SMH). The transcripts were not checked by participants because the lead author relocated shortly following the focus group and this was not possible as a result. Analysis of the data, which consisted of audio recordings of focus groups and interviews and field notes, was through an inductive thematic approach (Braun & Clarke, 2006) and carried out by the lead author using the QSR International’s NVivo 10 Software (2012). The following steps were followed:
Once the transcripts were checked by the researchers to ensure content was correct the transcripts were read (by SMH) several times to ensure emersion in the data. The transcripts were read again (SMH) and this time a list of codes were produced for each one of the transcripts. From this list of codes, themes were generated and discussed with the second author (SF). Both the themes and codes were re-checked and revised, changed or dropped if appropriate, in the context of the full set of transcripts. The themes were then defined by the researcher (SMH), using the codes that were related to each theme. The relevant quotes from the transcripts were then assigned to each theme to ensure that the evidence for each theme was clearly shown (See Appendix III for example from Theme 1). Transcripts, themes, codes and definitions were checked again with the second author (SF) before analysis was concluded.
Results
Participant demographics
Eight occupational therapists and ten people with MS volunteered for the study. One occupational therapist was excluded because they reported not having enough expertise working with people with MS. Five people with MS were also excluded as they were unable to commit to the requirements of the study – two people were unable to attend the focus group and three people were unable to review the handbook in the timeframe required. As a result, seven occupational therapists and five people with MS participated in the consultation (see Tables 2 and 3). All participants were female.
Demographic characteristics of participants with MS.
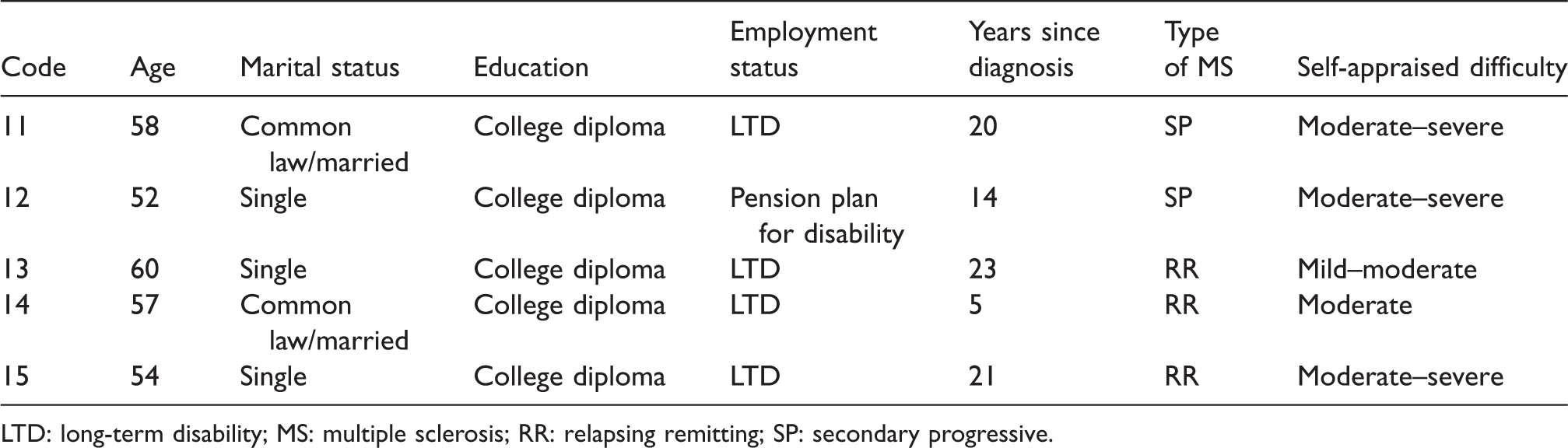
LTD: long-term disability; MS: multiple sclerosis; RR: relapsing remitting; SP: secondary progressive.
Characteristics of occupational therapist participants.
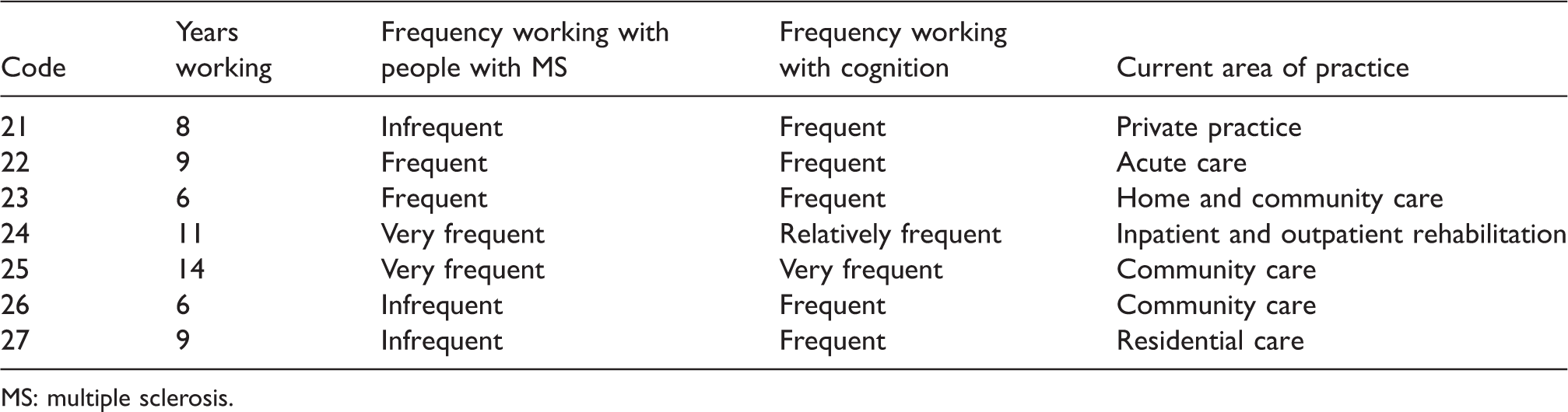
MS: multiple sclerosis.
Only one participant reported having received treatment for cognition – this treatment was reported to have been provided by an occupational therapist. Another participant reported trialling various methods of self-treatment including Lecithin, meditation and massage.
Themes from the data
Themes and sub-themes from data.
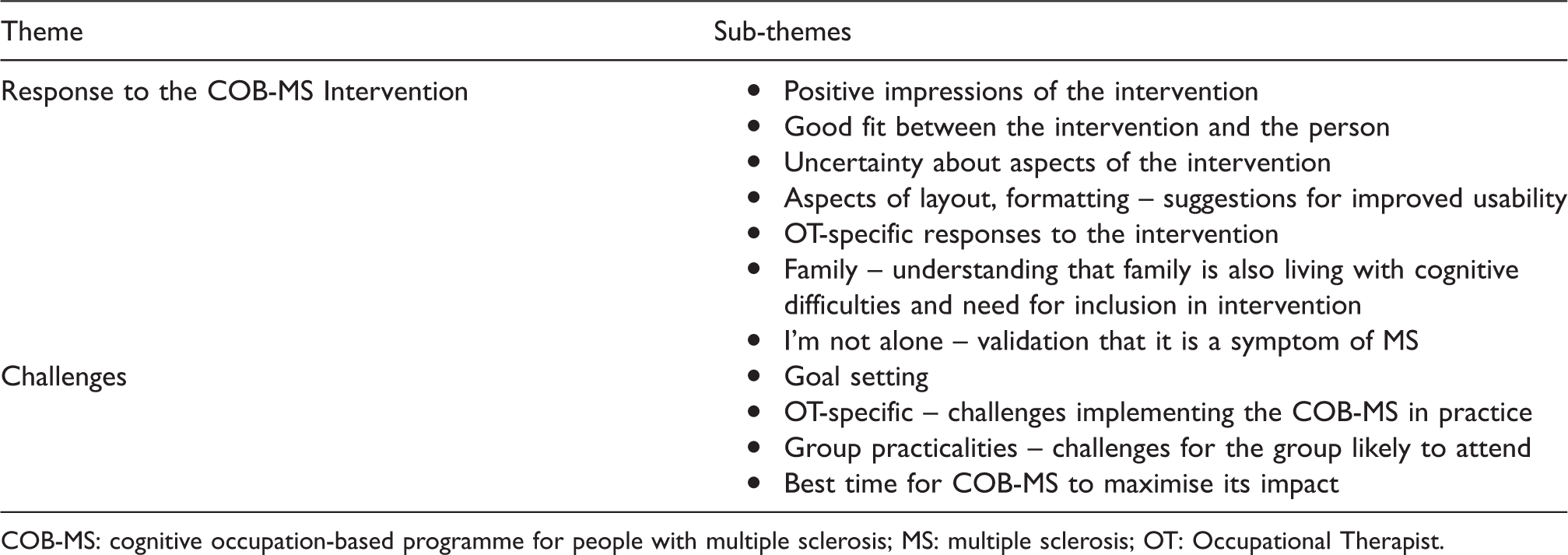
COB-MS: cognitive occupation-based programme for people with multiple sclerosis; MS: multiple sclerosis; OT: Occupational Therapist.
Response to the COB-MS intervention
When participants were asked what their first impressions of the COB-MS was all participants responded positively, participants with MS particularly. Many spoke of the significance of having a handbook and intervention that they feel was a good fit for them and the difficulties they encounter in their daily life. I couldn’t believe it. It described my memory to a T. (PMS15) It’s like a bible, basic instruction, it’s like I’m so glad! It’s gold, yeah, it’s really gold. (PMS11) It really was obviously client-centred, giving them the control and all those things I really, really like…I really like that it’s so occupation-based and occupation-focused… I would love to be able to implement this program because it just seems very, very comprehensive and very much you know, having that occupation focus um and client centred focus really resonated with me. (OT27) I like how it incorporates the holistic view of the person, like it…doesn’t just isolate cognition. (OT26) ‘I like how there’s a section on seeking new challenges…I’m not just gonna exist, I’m gonna live fully and I think I really like that’ (PMS11).
All participants with MS stated that they were unaware that MS could cause cognitive difficulties until quite recently. It was something that had in the past caused them to feel negatively about themselves: ‘When you get with people you don’t know very well, they just think you’re stupid’ (PMS14).
One participant said that she had wanted to continue working but felt forced to leave her job because she was becoming overwhelmed and did not feel capable of dealing with work. I honestly think that if I had been aware when I was working of a lot of these…I might have been able to lengthen my tenure…not to have to just say ‘ok I gotta get out of here, there’s no way to deal with this'. (PMS14) ‘It validates you. Yeah, you stop blaming yourself and the outside yourself says “this isn’t you, this isn’t what makes you you’ (PMS12).
Having that information had a positive impact on this group of participants. They found that it ‘was just a relief to say “ok, it’s not me, it’s the disease”’ (PMS14) and that ‘it was almost like it gave permission’ (PMS11). One of the occupational therapists stated that one of the obvious strengths of the COB-MS is that the group format may offer informal peer support and re-assurance. This could be very valuable to people who have yet to know the commonality of their experience. One participant with MS and one occupational therapist spoke about how the COB-MS could help to inform family members about the difficulties with cognition that they are experiencing. One participant stated that she was able to use the COB-MS handbook to describe her experiences to her sister: ‘It was such a great way to say to [my sister] “this is what I’ve never been able to explain to you”… for me to understand that and see that was just fantastic!’ (PMS13).
One occupational therapist suggested including family members in the group sessions, particularly in the first group session. The occupational therapist thought that it would serve two purposes – educating the family member and also making them aware of the importance of committing to the intervention. None of the participants with MS stated that they felt that their family or support network should be included in the group.
Occupational therapists and participants with MS valued that current issues in MS were dealt with in the programme: ‘What I really like about it, it brings up the trending stuff now’ (PMS11). To give details of different research that was done or experiments I think engages people in a different way where they go “oh! This has been shown to work” and it just kind of adds credibility to what you’re saying and may be the breaking point of actually getting them to try strategies…I just felt that was a really nice thing to include. (OT27) ‘I think the flexibility within the program leaves it vulnerable to not being as standardized as you might wish for it to be’ (OT26).
The occupational therapists were asked if they thought that the COB-MS would require training. Four of the therapists thought that training would not be necessary and three thought it would. Of the three people who thought training would be necessary, two thought it only necessary for newly qualified therapists or people with minimal experience working with people with MS. There was agreement that training should be optional and the most common suggestion was for online training.
Challenges
The area that there was some uncertainty about was goal setting, and this was stated by both stakeholder groups. Participants agreed that it might be difficult to come up with goals so early in the intervention. ‘They haven’t been given information so it’s hard to create goals when you don’t have any strategies’ (OT22).
There was discussion around this issue during the focus group and some participants were hesitant about setting goals. ‘Setting objectives, that’s something I find very hard to do…I find it intimidating to be told I have to set goals… It’s not that I cannot do it but I probably need a lot of help actually verbalising it’ (PMS14).
Although this was a concern that was identified by both groups not all participants thought that it would be a problem. Two of the occupational therapists specifically identified the goal setting as a positive and thought it was well-placed at the beginning of the intervention. One participant with MS stated how she thought that the goal setting was clear and comprehensive. ‘This is so well illustrated, written, on how to make a goal, it’s just incredible’ (PMS12).
Both groups believed although the intervention would be useful at almost any stage of MS, in order to get the most impact the right time to implement the COB-MS would be relatively soon after diagnosis. All participants with MS agreed with this timing and would have liked to have been offered the COB-MS when they were first diagnosed. If I had any of this when I was early in my diagnosis and still in the business world, I may have been able to stretch my time in the business world before I finally conceded to it…The material probably would have at least saved two of my jobs. (PMS12) ‘If you were doing it in the early MS population, people who are still functioning relatively well…we know from experience that if people learn these strategies before they absolutely require them, carry over’s a lot better’ (OT24).
The occupational therapists also spoke about the challenges that come with running a group if people are experiencing significant cognitive difficulties, including difficulty processing information, people not having insight into their difficulties and possible motivational problems.
One occupational therapist worked in private practice and stated that for her a group intervention would not be an option. Most of the occupational therapists also stated that they would have two main barriers in running a group in their current practice – getting to sessions and getting the numbers for a group. Many of their clients would not be able to make a weekly group session because they live too far away and driving long distances would be a barrier. For others it would be too difficult for the clients to attend the weekly sessions as they already are having difficulty with their daily activities. ‘What I see is people are trying so hard just to manage their daily activities, like getting themselves dressed, getting their meals cooked, just maintaining their very, very basic ADLs…you’d be hitting a very select population’ (OT23).
Four of the occupational therapists stated that they would struggle to get the numbers to run a group like this. Having people in a group who have similar levels of cognitive function may also prove challenging according to two of the occupational therapists interviewed. That said there were also benefits seen to running the COB-MS as a group as stated by one occupational therapist in the context of working resourcefully. ‘Having the group format is a selling point because it’s such a great use of the therapist’s resources’ (OT27).
Another occupational therapist said that they would like to see the COB-MS available in an individual format.
The occupational therapists also stated that having the time available to them to run the group would be an important factor. With large caseloads and urgent and palliative clients for some of the occupational therapists they could not guarantee that they would be able to prioritise running a weekly group unless they had someone to cover for them. Having support from managers was noted by one of the occupational therapists as being ‘The most significant consideration’ in deciding whether to implement the COB-MS. The occupational therapists were, however, positive about the future of the COB-MS. ‘I think it would work really well actually…I loved it! I wanna keep it, I don’t want to give it back to you!’ (OT25).
Discussion
Here we found that people with MS and occupational therapists welcomed the development of the COB-MS and were positive about its usefulness and implementation. Some challenges exist when implementing a group-based programme such as the COB-MS with a population that has a chronic condition but the programme was well received with little divergence of opinion evident from the data.
Participants in both groups expressed their appreciation for having available an intervention that is such a fit to their own experiences. Similar to das Nair and Lincoln (2013) participants spoke about the control that an intervention like this would have given them over their condition, particularly in the early stages of the condition. Participants with MS were not newly diagnosed but they suggested that the group would be best suited to a newly diagnosed group format. This would also lessen some of the challenges that were identified by the occupational therapists in relation to running a group with a more severely affected population. Based on the feedback from participants some changes will be made to the COB-MS programme such as the inclusion of information on a number of online resources and some grammatical and language changes in places for people with MS. For occupational therapists, the updated COB-MS will include more information on goal setting and guidance on follow-up, as well as tips on running groups and suggested outcome measures for use by occupational therapists. The length and structure will stay the same as they were well received. Das Nair and Lincoln (2013) report that participants had an appreciation for the benefits that exist from a therapeutic point of view from having a group format, which was also the case here. The exercises, strategies and the content of the handbook will also largely remain unchanged. The focus of the COB-MS is on an holistic approach to cognitive rehabilitation.
Researchers have shied away from holistic and client-centred approaches in preference for repetition and remediation (Wilson, 1997) which are less likely to have any real impact on patient’s lives. We can see evidence in the cognitive rehabilitation literature in populations with and without MS that research has tended to focus on one cognitive function (e.g. Cerasa et al., 2013) or used one modality, such as computerised training (e.g. Hildebrandt et al., 2007). The COB-MS takes a broader approach to rehabilitation. Cognitive abilities have been shown to correlate with other symptoms and functional difficulties that present in MS including fatigue and depression, as well as ability to maintain employment, social activities, managing in the home and self-care (Finlayson, Impey, Nicolle, & Edwards, 1998). This indicates that an occupation-focused approach is likely to be particularly effective for this population. As clinicians may not have experience working with specific needs of a population of people who have MS and cognitive difficulties it would be essential that therapists be trained in the COB-MS before intervening with clients.
A limitation of this research was the small number of participants that were consulted. In addition, participants were female and thus it is not known if a male perspective on the COB-MS differs. For the participants with MS, there were no newly diagnosed participants and given the important suggestions around the timing of the intervention it would have been valuable to have had the voice of someone who was newly diagnosed. There may also be important views missing as the participants were diagnosed a relatively long time ago and were also of similar education levels and ages – the age band was quite narrow for both occupational therapists and participants with MS. Data saturation was achieved with occupational therapists but it is unlikely that saturations were reached with people with MS following one focus group in a single location.
Conclusion
The views of the COB-MS by people with MS and occupational therapists were largely positive but overcoming logistical challenges is key to successful intervention implementation. The range of difficulties seen in MS impacts all aspect of life and clearly suggests an urgent need for a targeted approach to cognitive rehabilitation intervention. The foundational evidence required to develop and refine the COB-MS has been established and it should serve this role, with further feasibility testing. This is the first known cognitive rehabilitation intervention in MS that focuses on occupation and participation and has the potential to positively impact the lives of people living with MS.
Footnotes
Acknowledgement
Thank you to Hina Mahmood for help with completing the handbooks and to Jodie McCormick for data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded in part by a National MS Society Postdoctoral Fellowship Award #MB 0016 and the Occupational Science & Occupational Therapy Research Initiative Fund Seed Grant 2015.
Ethical approval
Ethical approval for the study was provided by the University of British Columbia Behavioural Research Ethics Board (H15-02333).