
Abstract
Introduction
This study analysed the differences in play performance between preschool children with cerebral palsy and those with typical development and investigated the factors influencing functional mobility and manual dexterity on play in children with cerebral palsy.
Method
Sixty preschool children (30 with cerebral palsy; 30 with typical development), were assessed by the revised Knox Preschool Play Scale, being that children with cerebral palsy were also classified according to their functional mobility and manual dexterity.
Results
On average, all measures were significantly smaller in the cerebral palsy group than the typical development group (p≤ .002). Manual function and functional mobility were negatively correlated with material (r = −.456, p = .011; r = −.487, p = .006) and space (r = −.494, p = .006; r = −.784, p = .000). Also the results pointed out a significant correlation with topography and manual function (r = .404, p = .027) and functional mobility (r = .718, p = .000). Pretend play and participation showed no correlation with topography (r = −.051, p = .788; r = −.312, p = .093), manual function (r = −.019, p = .921; r = −.322, p = .083) and functional mobility (r = −.085, p = .657; r = −.308, p = .097).
Conclusion
Play performance of children with typical development was superior to those with cerebral palsy. The degree of impairment of functional mobility and manual function negatively was negatively associated with play exploration but did not relate to pretend play or social interaction in play.
Introduction
Among the possible neurological disorders, cerebral palsy (CP) is the main cause of physical disability in childhood (Morris, 2007). It is estimated that 17 million people are afflicted with CP worldwide (Novak, 2014). Motor disorders of CP are commonly presented with difficulties in perception, cognition, communication and behaviour, sensory disturbances, epilepsy, and secondary muscle problems (Rosenbaum et al., 2007). Since CP results in changes in the structure and function of the neuromusculoskeletal system, its clinical classification can include spastic, ataxic, or dyskinetic. Spastic CP can be further classified as unilateral or bilateral, based on anatomical distribution (Ciasca, Moura-Ribeiro, & Tabaquim, 2006). The clinical classification and anatomical distribution of the disease is based on the diversity of CP manifestations, but it can also be classified according to the levels of motor impairment and manual function using the Gross Motor Function Classification System – Expanded and Revised (GMFCS – E&R) (Palisano, Rosenbaum, Bartlett, & Livingston, 2008) and Manual Ability Classification System (MACS), respectively (Eliasson et al., 2006).
Because of changes in the structure and function of the system, children with CP often develop muscle weakness, have difficulty controlling agonist and antagonist muscles, have a restricted range of motion, and changes in tone and sensitivity. These changes may interfere with activities, including reaching, touching, manipulating, walking, writing, playing, etc. which are required for these children to function both at home and school (Beckung & Hagberg, 2002; Rae, Copley, & Ranka, 2010).
Playing stands out as one of the most important activities at preschool age, since it encourages the development of social, cognitive, emotional, and physical abilities, as well as the expansion of language (Lifter, Foster-Sanda, Arzamarski, Briesch, & McClure, 2011). Play assessment enables the identification of how child development occurs. By observing a child at play, it is possible to assess skills such as dexterity and coordination, cognitive functions, expression of feelings, and social skills (Ferland, 2006). Thus, standardized methods that assess play may be used to determine the eligibility of a child for therapeutic services, monitor progress throughout the treatment process, and assist in determining the most appropriate and effective intervention for each case (Richardson, 2010).
The revised Knox Preschool Play Scale (KPPSr) is a play assessment method that provides a description of the evolutionary skills involved in play of children aged 0–6 years (Knox, 2002). This scale was cross-culturally adapted for the Brazilian population and was found to be reliable and repeatable (Pacciulio, Pfeifer, & Santos, 2010; Sposito, Pfeifer, & Santos, 2012).
Although literature indicates that the levels of motor impairment and manual function of children with CP can influence play (Pfeifer, Pacciulio, Santos, Santos, & Stagnitti, 2011), there are no studies with a particular focus on the specific correlation between play and motor skills. Therefore, the current study evaluated play performance of children with CP, using the KPPSr, and compared it to children with typical development (TD). Further, we also assessed the influence of the level of functional mobility and manual function on play in preschool children with CP.
This study aimed to compare the play performance of preschool children in TD and children with CP, and investigate the relationship between the level of functional mobility and manual function on play in these children. The results of this study provided new information for occupational therapists to understand which abilities contributed to their play performance.
Methods
This was an applied, non-experimental, cross-sectional research study with a quantitative and descriptive design. This study was approved by the ethics board of Clinical Hospital of Ribeirão Preto Medical School – Ribeirão Preto, Brazil (reference number: 1.188.998).
Recruitment and consent
The research cohort, which consisted of 30 children with CP and 30 children with TD, comprised both boys and girls, aged 3–6 years (with a tolerance of four months after the sixth birthday). All children with CP were undergoing treatment at rehabilitation centres in the municipality of Ribeirão Preto, while children with TD were enrolled for regular education in schools located in the same municipality. The parents of all children (TD and CP) signed informed consent form (prepared by the authors), authorizing their participation in this study.
The inclusion criteria of children with CP were (1) diagnosed with CP, (2) age 3–6 years, (3) able to understand simple commands, and (4) consented by parents to participate in this study. All children who had fulfilled these criteria were recruited to the study by means of convenience sampling. The group of children with TD was compared to the group of children with CP in terms of age and sex.
Assessment measures
Children with TD were evaluated using the KPPSr alone, while children with CP were evaluated using the KPPSr, GMFCS – E&R, and MACS.
The KPPSr is a play assessment that provides a description of the evolutionary skills of performance involved in play of children aged 0–6 years. The KPPSr is divided into four dimensions: Spatial Management, Material Management, Pretense/Symbolic Play, and Participation (Knox, 2002). The Spatial Management is related to how a child moves his/her body and interact with the world around him/her. It involves two areas: gross motor coordination (related to recreational activities that involve the whole body) and interest (the choices of recreational activities). The Material Management is related to how a child manipulates toys and objects, and involves four areas: manipulation (recreational activities that involve fine motor skills), construction (the combination of objects and the making of products), objectives (purpose of activity), and attention (the attention time the child paid during recreation). The Pretense/Symbolic Play is related to how the child imitates his/her world understanding and separating reality from fantasy. It involves two areas: the imitation (the child reproduces the behaviours of its immediate environment) and the dramatization (the child performance on some of the papers). Finally, the Participation is related to how a child interacts socially and involves four areas: the type of interaction (during recreational activity), the cooperation (ability to deal with others in the recreational activity), the humour (understanding and expression of humorous words or episodes), and language (used during recreation) (Knox, 2002).
The KPPSr is divided into nine age groups (0–6, 6–12, 12–18, 18–24, 24–36, 36–48, 48–60, and 60–72 months), and the number of items depends on each age. In this study, we used the Brazilian version of KPPSr (Pacciulio et al., 2010) in order to identify how participants dealt with play.
The GMFCS – E&R, which was also cross-culturally adapted for Brazilian population (Silva, Pfeifer, & Funayama, 2010b), classified the functional mobility of children with CP into five levels: I, walks without limitations; II, walks with limitations; III, walks using a manual device mobility; IV, auto-mobility with limitations; and V, transported in a manual wheelchair. The MACS, which was also cross-culturally adapted version for Brazil (Silva, Pfeifer, & Funayama, 2010a), classified the manual function of children with CP to five levels: I, manipulates objects with success; II, manipulates most objects with reduced quality or speed; III, manipulates objects with difficulty; IV, manipulates a variety of easily usable objects; and V, does not manipulate objects.
Data collection
Evaluations were performed individually in a private room, provided by the rehabilitation centre (for children with CP) or at school (for children with TD), without the interference of external stimuli. In the CP group, the three assessments were performed during the consultation time, without incurring extra costs to the family. In the control group, the KPPSr was applied during school hours.
The data were collected by three evaluators (undergraduate students of occupational therapy) trained by the third author of this study through classes, video analysis, and practical activities using the scale.
A list of recreational activities, favouring the interest and active involvement of children, which in turn allowed the assessment of the components described by each dimension of the scale, were evaluated according to the age group using the KPPSr. The scoring criteria used in this study were proposed by Pfeifer (2006): 2 points for ‘displays confident behaviour’, 1 point for ‘displays hesitant behaviour’, −1 point for ‘does not display behaviour’, 0 points for ‘behaviour not observed’. These scoring criteria had been used in other studies and found to be valid (Mannini & Pfeifer, 2011; Pacciulio et al., 2010; Rombe, 2012; Solai & Pfeifer, 2007).
Data analysis
Data were analysed using descriptive statistics and multivariate correlation analysis. Results between 0 and 0.9 are considered as a very low correlation; 0.20–0.39 considered as low correlation; 0.40–0.59 considered as moderate correlation; 0.60–0.79 considered as a good correlation and 0.80–1.0 considered as a very good relation (Bisquerra, Sarriera, & Martínez, 2004). Mean values of the CP (study) and TD (control) groups were compared using an independent t-test. Correlations between motor aspects (functional mobility, manual function) and play in children with CP were analysed using a Spearman’s correlation test (Siegel & Castellan, 2006).
Results
The detailed characterizations of the two groups are outlined in Table 1, while Table 2 shows the scores of the two groups for each dimension in the KPPSr.
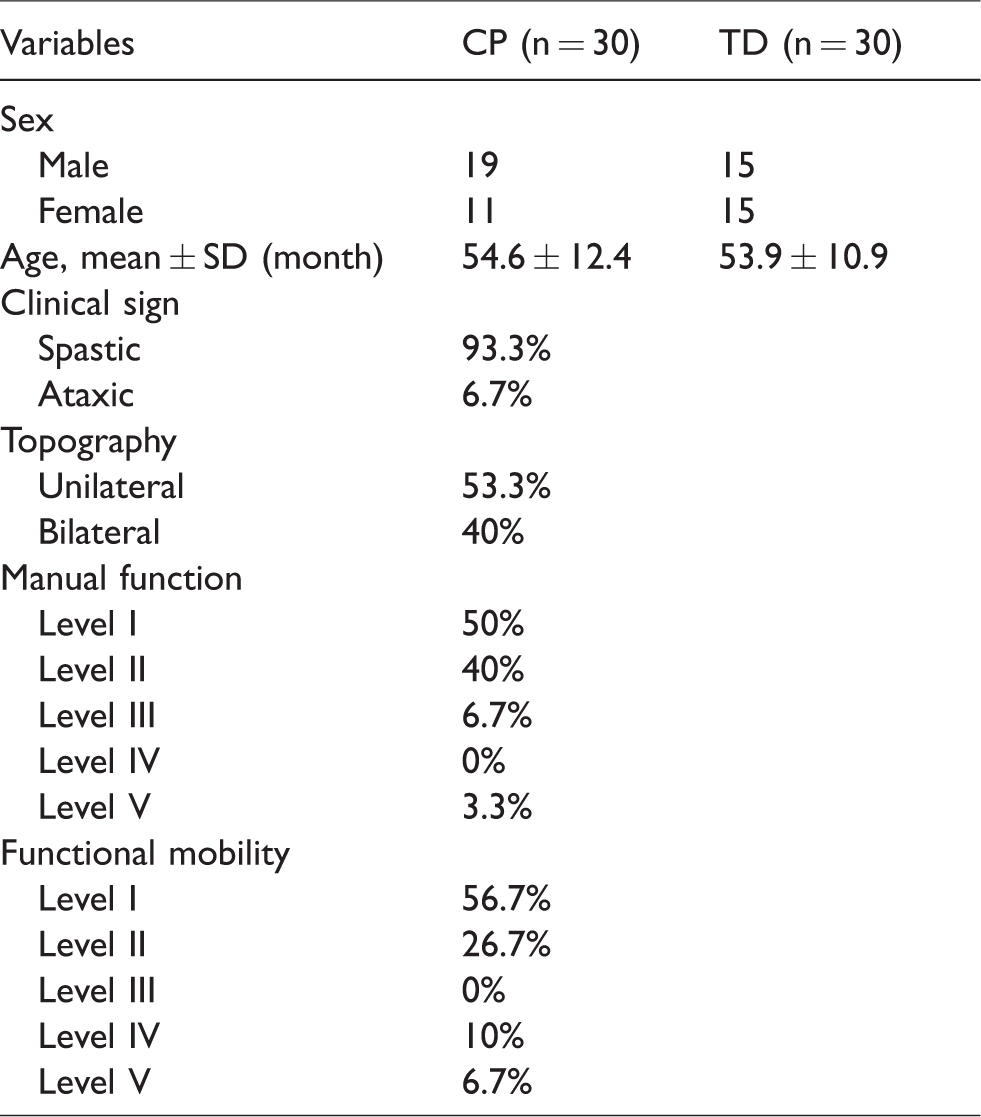
Participants’ demographics.
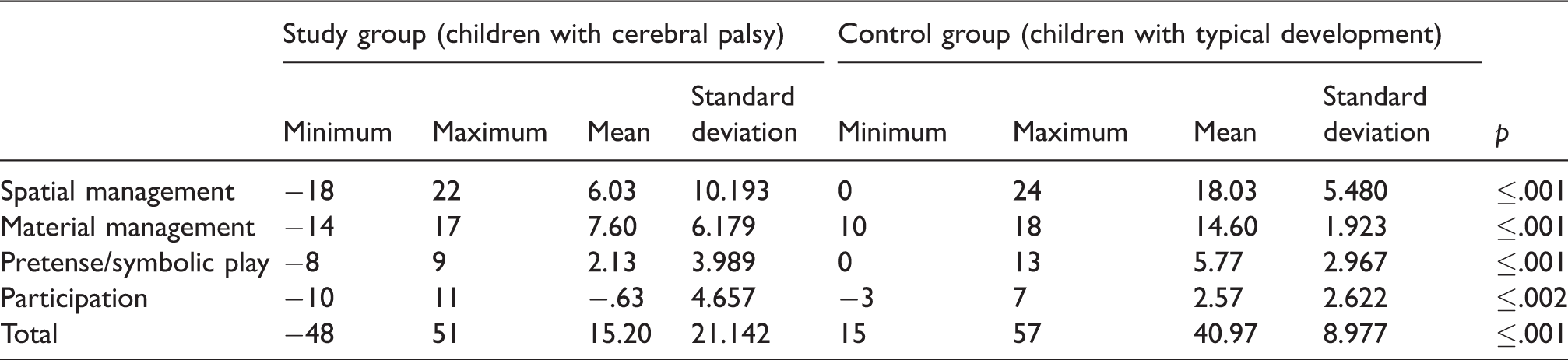
Scores obtained in each dimension of the scale and the total scores in both groups (n = 60).
As shown in Table 1, the study group consisted of a predominantly male sample, while the control group consisted of a homogeneous sample. Regarding the clinical classification of children with CP most of the sample was classified as spastic (worldwide prevalence). Within the topography, the unilateral classification was the highest incidence. As for manual function and functional mobility, the majority of children was classified as having the lowest motor impairment.
Table 2 presents the scores of each participant (study and control groups) in the dimensions created in KPPSr. It is observed that the mean obtained by the study group was always lower than the mean obtained by the control group, presenting difference statistically evident between the groups in all dimensions, using a t-test for independent samples.
Table 3 outlines the correlation between each dimension of the KPPSr with results of the MACS, GMFCS – E&R, and topography of the study group, aiming to verify if motor aspects, such as functional mobility and manual function, influenced play in children with CP. A significant negative correlation was obtained between manual functions and materials and between manual function and spatial management of the KPPSr. Further, the functional mobility was negatively correlated with performance in the spatial and material of the KPPSr. These results indicate that a greater impairment of manual function and functional mobility led to poor engagement with recreational activities requiring those functions.
Correlations between variables analysed in the study group (n = 30).
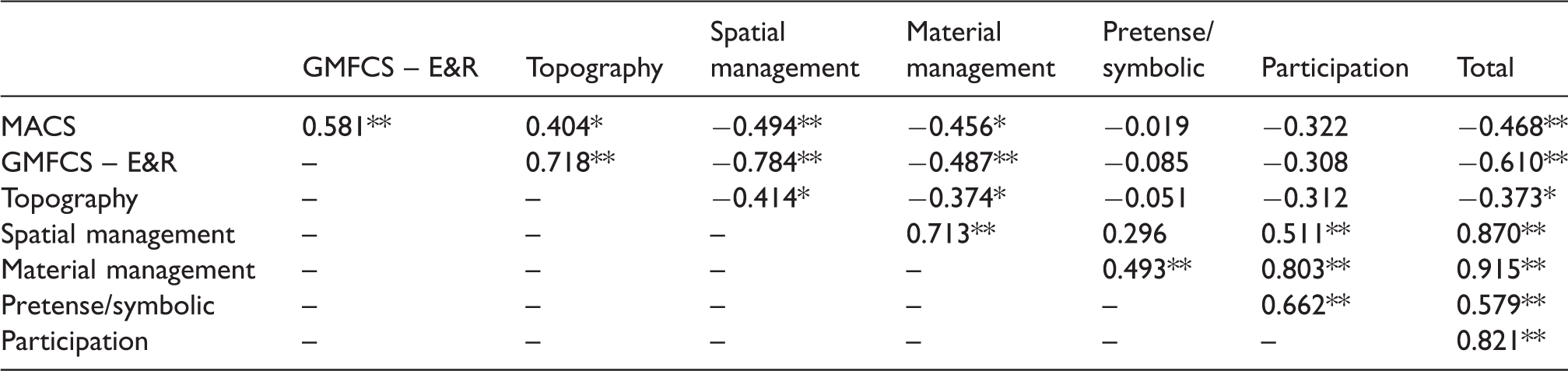
GMFCS – E&R: Gross Motor Function Classification System – Expanded and Revised (Palisano et al., 2008); MACS: Manual Ability Classification System (Eliasson et al., 2006).
**: The correlation is significant at the 0.01 level.
*: The correlation is significant at the 0.05 level.
However, there were no significant associations between the manual function and functional mobility and the pretense/symbolic play and participation dimensions of the KPPSr. This suggests that these dimensions are not directly influenced by motor skills in children with CP.
Manual function and functional mobility were also correlated, which indicates that children, who had difficulty in skills requiring functional mobility, also had greater difficulty in activities that involved manual function.
On comparing the KPPSr dimensions between themselves, a significant correlation must be noted between participation and material management. During data collection, the child was alone with the assessor and the participation was evaluated only by a relationship between child and assessor. The correlation can be explained, probably by the fact of the activities presented to assess the material management have been to be carried out with the child seated allowing focus on the activity and increasing the possibility of establishing contact with the appraiser. The material and spatial managements were also correlated, since children with CP who had difficulties in performing ample motor activities also faced difficulties in performing activities that required fine motor coordination.
Further, the topography of CP directly influenced the manual function, functional mobility, and the spatial and material management of KPPSr, being that children with unilateral CP recorded higher scores than those with bilateral CP in both dimensions. A similar result was not recorded for the dimensions of pretense/symbolic play and participation; therefore, the motor disorders do not influence these dimensions because they are more related to the cognitive abilities of these children.
The age or sex of the child had no significant effect on any of the variables.
Discussion
Epidemiological studies have demonstrated the greater frequency of CP in boys and the higher incidence of the clinical spastic type, which was also reported, and it is like the profile observed in the current study (Brasil, Ministério da Saúde, 2013; Caraviello, Cassefo, & Chamlian, 2006; Pfeifer et al., 2011; Rethlefsen, Ryan, & Kay, 2010). Although epidemiologically, there is a greater incidence of bilateral CP, the incidence of unilateral CP in the current study was greater (MacIntyre, Morgan, Walker, & Novak, 2011; Novak, 2014). This could be attributed to the fact that, despite the children’s participating in this study have been located at rehabilitation centres that serve different levels of complexity, the service that caters to the children most seriously affected as for motor skills (levels III–V), encompassing bilateral children, displays an intervention protocol that prioritizes children until three years of age.
The KPPSr, which was cross-culturally adapted for Brazilian population, had previously been used to assess the play performance of preschool children in situations of social vulnerability premature birth, chronic diseases, and CP (Grigolatto, Pacciulio, Panuncio-Pinto, & Pfeifer, 2016; Mannini & Pfeifer, 2011; Pfeifer et al., 2011; Rombe, 2012). In the current study, KPPSr was used to evaluate and compare the performances among preschool children with CP and those with TD, during play, proving to be effective in this process, being the only study to use KPPSr with children with CP using a control group for comparison.
The first dimension that constitutes the KPPSr, spatial management, defines how children learn to move their body and interact with the world around them through the process of exploration and experimentation. This dimension encompasses gross motor function concerning recreational activities involving the whole body, in addition to the choices of recreational activities (Knox, 2002). Significant divergence was recorded between the minimum and maximum group scores when this measure was analysed in children with CP, which can be explained by the heterogeneity of the sample because participants from different ability levels were included. When the performance of children with CP in this dimension was compared to those with TD, the average score of the study group was significantly lower than the control. Santos, Pfeifer, Silva and Panuncio-Pinto (2011), in their studies, also found low-performance indexes in children with CP in this dimension, especially in cases of serious motor impairment, because greater motor impairment lower was the capacity of these children to play a variety of games.
The second dimension, material management, is based on how a child explores and provides function to objects, which includes manipulation (involving fine motor skills), construction (understanding how to combine objects to manufacture a product), understanding the goal of the activity, and focussing on the recreation (Knox, 2002). The discrepancy between the minimum and maximum scores in this dimension can also be explained by the heterogeneity of the sample. The average material score obtained by the study group was lower than the control. Children with CP displayed patterns of movements (i.e. limited or inhibited movements) that affected the upper limbs, which in turn affected the scope, comprehension, and manipulation of objects, and led to the use of abnormal motor patterns to reach a goal (Autti-Ramo, Larsen, Taimo, & von Wendt, 2001; Cruz & Pfeifer, 2006). The topography had an association relationship with the material management, being that children with unilateral impairment had scores frequently better than children with bilateral impairment. Since the sample group comprised the most of children with spastic CP, their comprehension patterns were immature and incompatible with their chronological age, which affected school activities, daily life, play, and social relations (Russo et al., 2007). Consequently, these children performed poorly in the exploration of the material management of play.
The pretense/symbolic play dimension of the KPPSr is characterized by the way a child learns about the world through imitation and the ability to separate fact from fantasy. Further, it encompasses imitation, which is the reproduction of behaviour from the child’s immediate environment, and dramatization, which is the introduction of novelties and role-play (Knox, 2002). In this dimension, there was no discrepancy between the average scores obtained by children in both groups. Since both means were relatively low, however, this finding could be related to the types of toys available for the assessment and/or the interest of the child in a more attractive stimulus (Pfeifer et al., 2011). Ferland (2006) highlights the importance of availability and variability of materials during play. Further, the attitude of the evaluator in offering these materials to the child is also fundamental. Studies evaluating pretend play in children with CP using the Child-Initiated Pretend Play Assessment (consisting of an evaluation method that is specific to pretend play) also noted that the majority did not demonstrate skills for this type of play or they had significant limitations (Pfeifer et al., 2011; Santos, Pacciulio, & Pfeifer, 2010). However, these studies did not compare the scores with those obtained from children with TD.
The fourth dimension of the KPPSr, participation, refers to the quantity and quality of social interaction, including the type of interaction during recreational activity, cooperation with others during play, humour (encompassing understanding and expression of words or humorous episodes), and the language used for communication with others (Knox, 2002). In this dimension, there was no great discrepancy between the average scores obtained from children in both groups; however, averages from both groups were low. A study evaluating the behaviour of playful children with CP found that most of the children expressed increased interest in the presence of an adult, evident through their verbal and nonverbal expressions and their actions, which were unaffected by motor difficulties (Santos et al., 2011).
The manual function and functional mobility of children with CP was also evaluated, which showed significant negative correlations with the material and space managements on the KPPSr. This finding suggests that the greater the impairment of manual function, the poorer is the performance of children with CP in activities that require such skills. Further, manual function and functional mobility were also correlated, indicating that children, who had difficulty in skills involving manual function, also had difficulties with functional mobility skills, contributing to greater limitations on play. A study stated that the greater the severity of CP, the more it affected the motor performance of these children. Further, an increased limitation of voluntary movement or mobility subsequently markedly affected play, which is highlighted by the recorded negative correlations (Santos et al., 2011). Other authors demonstrated that children with CP were more restricted in their exploration of the environment, which corroborates with previously described findings in the current study. Therefore, it is essential that the therapist act as a facilitator, providing an opportunity for the child to obtain those experiences (Cruz & Pfeifer, 2006).
Another point to stress that, although the sample of this study include most of children with mild CP (level I/II on GMFCS and MACS), some of them performed poor scores in all dimensions of KPPSr, suggesting that children might have cognitive delay, and some of them might not feel comfortable with the assessors who were stranger to the children. In future study which includes a cognitive evaluation, the assessor should establish prior rapport with the children before assessment.
This study has some limitations. One of them was the small sample size and a uniform distribution between motor classification levels. Most of the children were of mild impairment, thus limited the comparison of the play performance between children with TD and children with CP with different clinical manifestations. It is suggested that new studies should be done, not only in rehabilitation centres but also in other centres so as to ensure a greater clinical heterogeneity of the study group, and that the data would not contemplate the evaluation of the play performance in children with CP with limited level of impairments. We also observed that the social class of the children influenced their relationship with the toys, consequently, their way of playing. Thus, it is suggested that the future survey should consider the social class as a demographic variable for statistical analysis.
Conclusion
The degree of impairment of functional mobility and manual function of children with CP is associated with the exploration of play, especially in activities that requiring gross motor coordination, dexterity, and fine motor coordination. Motor deficits, however, do not seem to directly relate to symbolic play and social interaction during play. This study highlights the important role of an occupational therapist in performing a detailed assessment for each child, and identifying the individual degree of motor impairment and delayed development of play, which contribute to children’s participation in play in daily life.
Footnotes
Acknowledgement
Conselho Nacional de Desenvolvimento Científico e Tecnológico.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.