
Abstract
Endometriosis and adenomyosis are chronic, debilitating, inflammatory conditions affecting women of reproductive age. Current management primarily focuses on pharmacologic therapies and surgical interventions; however, many individuals adopt self-directed lifestyle modifications despite limited evidence-based guidance to support these approaches. This scoping review aimed to collate and evaluate the available evidence for lifestyle interventions in the management of pelvic pain among women with endometriosis and/or adenomyosis, with consideration of key lifestyle medicine domains including nutrition, physical activity, mind–body practices, social connection, sleep, substance cessation, and self-management. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). Electronic databases (MEDLINE [OVID], CINAHL, and Scopus) were systematically searched to identify relevant interventional studies. Following abstract and full-text screening, 21 studies met inclusion criteria. Included studies demonstrated substantial heterogeneity in methodology, sample size, intervention type, and duration of follow-up. Only one study specifically included participants with adenomyosis. Findings suggested potential benefits of dietary modification, physical activity, mindfulness-based interventions, yoga, digital health programs, and transcutaneous electrical nerve stimulation (TENS) for pelvic pain management. However, small sample sizes and methodological variability limit the strength of conclusions. Overall, the current evidence base remains limited and underscores the need for rigorously designed interventional studies. Future research should incorporate broader outcome domains, including quality of life, fertility, and mental health, and should more comprehensively address lifestyle domains such as sleep and substance use. Greater inclusion of individuals with adenomyosis is also essential to inform evidence-based lifestyle recommendations in this population.
Keywords
“Hormonal treatments aim to slow or suppress the growth of endometriosis lesions or stop bleeding and thus reduce the pain and severity of endometriosis”.
Introduction
Endometriosis is a common, chronic, debilitating women’s health condition which impacts at least 1 in 9 Australian women by the age of 44. 1 It is a chronic inflammatory condition diagnosed by the presence of endometrial-like tissue outside of the uterus. 2 The endometrial-like tissue can occur in the pelvis (such as superficial peritoneum and ovaries), as well as extra-pelvic sites including the abdominal organs, lungs and nervous system with sites and severity varying from person-to-person. This results in various symptoms in sufferers including period pain (dysmenorrhoea), heavy menstrual bleeding (menorrhagia), chronic pelvic pain, painful sex (dyspareunia), painful defecation (dyschezia), fatigue and infertility. 3 Symptoms vary between women and the degree of disease does not always correlate to symptom severity. 3 These symptoms often negatively impact daily living and quality of life. 4
Adenomyosis often co-exists with endometriosis and occurs when the endometrium grows into the muscular wall of the uterus (myometrium). It can also cause debilitating symptoms including pelvic pain, dysmenorrhoea, menorrhagia, infertility and poor pregnancy outcomes. 5 Prevalence estimates of adenomyosis vary widely from 8.8% to 61.5%. 6
Previously, the ‘gold standard’ for diagnosis of endometriosis was through laparoscopy and biopsy of suspicious lesions with histological confirmation of endometriosis, however there is a growing role for the use of specialised ultrasound (US) and magnetic resonance imaging (MRI) in the diagnosis and evaluation of the extent of disease. 7 Despite increasing awareness and improved diagnostic techniques, there is an average delay of 6.4 years from symptom onset to diagnosis of endometriosis in Australian women. 8 Historically, adenomyosis was a histopathologic diagnosis after hysterectomy, however due to imaging advancements, it can now be diagnosed by non-invasive techniques such as US and MRI. 5
Current endometriosis management is focused on analgesia to manage pain (with non-steroidal anti-inflammatories (NSAIDs) being first line), hormonal medical treatments to regulate oestrogen, laparoscopic surgery for excision of extra endometrial tissue or a combination of all three. 9 Importantly, it is unclear whether excision of endometriosis reduces pain or improves quality of life when compared to diagnostic or placebo/sham laparoscopy only. 10 Even with complete excision of all endometriosis lesions in the pelvis, pain recurrence at 5 years is approximately 50%. 11 In some cases, hysterectomy is also performed. Hormonal treatments aim to slow or suppress the growth of endometriosis lesions or stop bleeding and thus reduce the pain and severity of endometriosis. Hormonal treatment options include the combined oral contraceptive pill (COCP), progesterone (oral form, subcutaneous implant or intrauterine device) or gonadotrophin-releasing hormone agonists and antagonists. 9 Reported discontinuation rates of COCP and progesterone hormonal treatment is reportedly up to 50% owing to unwanted side effects (Brown et al., 2014).
Adenomyosis has a similar treatment approach with medical options to help with pain and menorrhagia (including NSAIDs, tranexamic acid and hormonal options as listed above) or surgical options (including endometrial ablation, excision of adenomyosis and hysterectomy). 12 Uterine artery embolisation may also be performed in adenomyosis. 12
Previous Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) endometriosis and adenomyosis guidelines published in 2021 only contained a brief segment on non-pharmacological and non-surgical recommendations for management of pain associated with these conditions. The recommendations included are low evidence for the role of Chinese herbal medicines and very low to moderate evidence for the role of acupuncture in endometriosis. The guidelines report there is little to no evidence for non-pharmacological interventions in the management of adenomyosis. 9
Women with endometriosis are often unhappy with their current health care, with a 2018 study illustrating that only 54.6% of women were satisfied with the medical care received. 13 Many women take their health care into their own hands, with an online Australian survey demonstrating 76% of those with endometriosis currently utilising self-care or lifestyle choices to manage their condition. 14 These women report improved pain outcomes with a mean self-reported effectiveness in pain reduction of 6.52 points for heat therapy and 6.39 points for dietary changes on a 10-point scale. 14
Lifestyle medicine is a growing field of multi-disciplinary health care which is defined as ‘the application of environmental, behavioural and motivational principles including self-care and self-management, to the management of lifestyle-related health problems in a clinical setting’. 15 It is often considered in broad pillars including nutrition, physical activity, mind-body, sleep, social connection and substance cessation. Lifestyle interventions are effective in reducing systemic inflammation.16-18 There is emerging research indicating potential benefit for these interventions in chronic disabling inflammatory conditions such as rheumatoid arthritis or inflammatory bowel disease.19,20
A systematic review and meta-analysis in 2024 examined the effect of dietary intervention on endometriosis. 21 It analysed 11 randomised control trials; however, the studies included all focused on dietary supplementation and did not include analysis of non-supplement based dietary interventions. There was suggested evidence for the role of vitamins C and E, fish oil (omega 3/6), wobenzym vital (an enzyme supplement containing the enzymes bromelain, papain, trypsin & chymotrypsin, bioflavonoids and vitamins C, D and E) and garlic supplementation for dysmenorrhoea. There was mixed evidence for vitamin D; however, the overall quality of included studies was poor with high heterogeneity and risk of bias limiting the clinical applicability. 21 Given this review has already taken place, and supplementation is not traditionally included in lifestyle medicine, further analysis of the role of dietary supplementation in endometriosis and adenomyosis will not be included in this review.
Despite the high prevalence of women with endometriosis utilising self-care strategies and lifestyle changes to optimise their management, there have been no previous reviews identified on the lifestyle management of endometriosis and adenomyosis. This scoping review aims to assess the current available state of evidence for lifestyle interventions in endometriosis and adenomyosis analysing the impact of diet, physical activity, social connection, sleep, mind-body interventions, substance cessation and self-care strategies on pelvic pain management.
Methodology
Scoping reviews are a research methodology which can be utilised to meet several objectives including; analysis of the extent of evidence on a topic, summarising findings from a body of knowledge and identifying gaps in the literature to aid planning of future research. 22 Given the non-pharmacological and lifestyle management of endometriosis and adenomyosis is a poorly researched area, a scoping review was considered the most appropriate methodology to map the current restricted evidence and thus answer the research question of ‘What is the evidence of lifestyle interventions for the symptom management of pelvic pain in women with endometriosis or adenomyosis?’.
Guidelines in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) were followed during this review. 23
To identify relevant studies, the following bibliography databases of Medline (OVID), Cumulated Index in Nursing and Allied Health Literature (CINAHL) and Scopus were utilised. The search strategy was drafted by author BJ with guidance from experienced librarian, Stephen Anderson, and further refined through team discussion. A combination of MeSH subject headings and keyword searches was used in Medline and CINAHL, and keyword searches were used in Scopus utilising a
Patient/population – women with endometriosis and/or adenomyosis.
Intervention – lifestyle intervention.
Comparison – no lifestyle intervention (either with comparison of a control group or pre-intervention)
Outcome – Pelvic Pain
When reflecting on lifestyle interventions, each lifestyle medicine pillar was considered individually to ensure a search strategy which covered the breadth of lifestyle interventions. Self-management and self-care key words were also included to cover lifestyle interventions not categorised in the traditional pillar model. Synonyms of pelvic pain, such as chronic pelvic pain, dysmenorrhoea and dyspareunia, were included.
Appendix A contains a table of the complete search strategy.
Inclusion Criteria/Exclusion Criteria
Following the PICO approach, inclusion and exclusion criteria were developed. The population was limited to human studies of women with endometriosis and/or adenomyosis. To address the research question, any intervention which focused on one or more of the pillars of lifestyle medicine, or another self-management strategy, and the impact of this intervention on pelvic pain were included.
Any intervention which required long-term direct allied health/specialist involvement and could not be self-managed long-term were excluded. This included interventions such as acupuncture or massage. Interventions which required allied health input initially for education but could then be self-managed were included (such as psychology in mindfulness education, physiotherapy in a physical activity program or dietician in a dietary intervention). Dietary interventions had to be wholly diet based and could not involve supplementations.
Given primary searches demonstrated limited randomised controlled trials in this area, the decision was made to include all interventional trails. This also includes interventional trials with a control group that are not randomised, along with intervention trials which do not have a control group, but instead, compared the research group to themselves pre and post intervention. Any non-interventional studies, review articles, editorials, letters, conference proceedings, poster presentations, commentaries or protocols were excluded.
Results
Study Selection
The complete search took place on Medline (OVID), CINHAL and Scopus on the 31st of March 2025. The search from Medline (OVID) returned 482 references, CINHAL returned 66 references and Scopus returned 3653 references. These references were all uploaded onto Covidence with a total of 294 duplicates removed. The remaining 3907 articles underwent title and abstract screening by two reviewers independently (authors BH and ND) against the inclusion and exclusion criteria. Disagreements were noted and discussed between the reviewers, and 25 articles were included for the full text screening. Six articles were excluded following this full text screening with 19 articles included in the final review. Three of these articles were excluded due to wrong outcomes, two due to wrong study design and one as it was a protocol and the interventional trial had not been completed. Two additional articles were added from reference searching.
Given that a scoping review aims to understand the extent of the literature rather than synthesise the data, a risk of bias was not considered in study selection.
23
Figure 1 below is a PRISMA chart illustrating the selection of studies for the scoping review. PRISMA chart showing selection of studies for the scoping review
Data Extraction, Charting and Synthesis
Data extraction was carried out using a data charting form by one author (BH). The completed data charting form is attached in Appendix B.
Individual Characteristics of Each Included Study.
Table 2 acronyms: FODMAP – fermentable oligosaccharides, disaccharides, monosaccharides and polyols, VAS – visual analogue scale, GIQoL – gastro-intestinal quality of life, EHP – endometriosis health profile, NRS – numeric rating scale, PSS – perceived stress cale, SF-36 – short form health survey, GAD – generalised anxiety disorder 7, PHQ – patient health questionnaire 8, PCS – pain catastrophising scale, PPT – pressure pain thresholds, FSFI – female sexual function index, DDS – deep dyspareunia scale, ESSS – endometriosis symptom severity score.
Study design
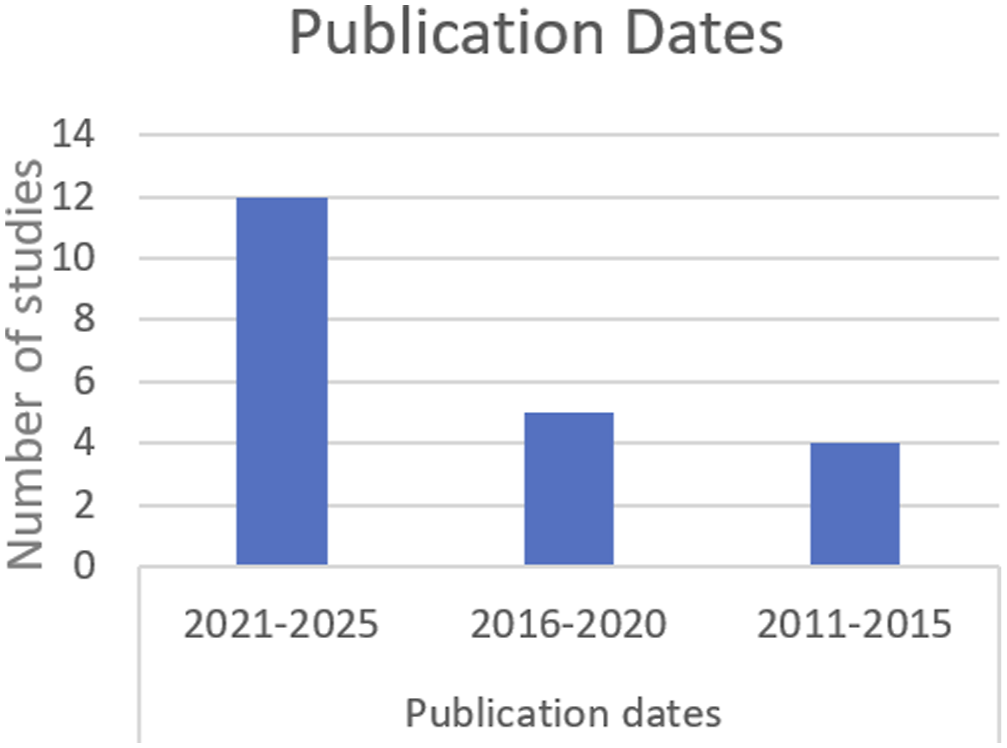
Publication dates
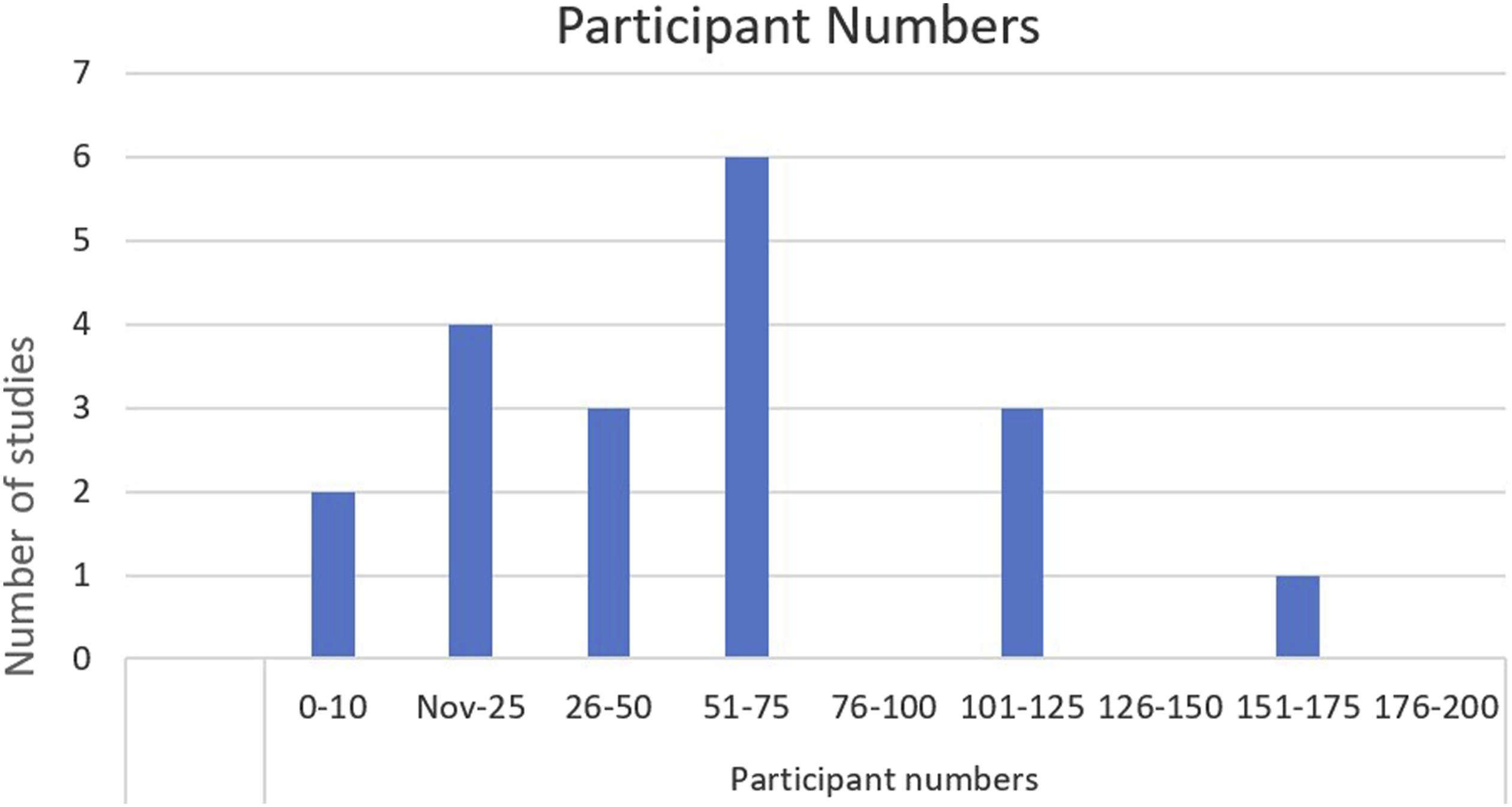
Participant numbers
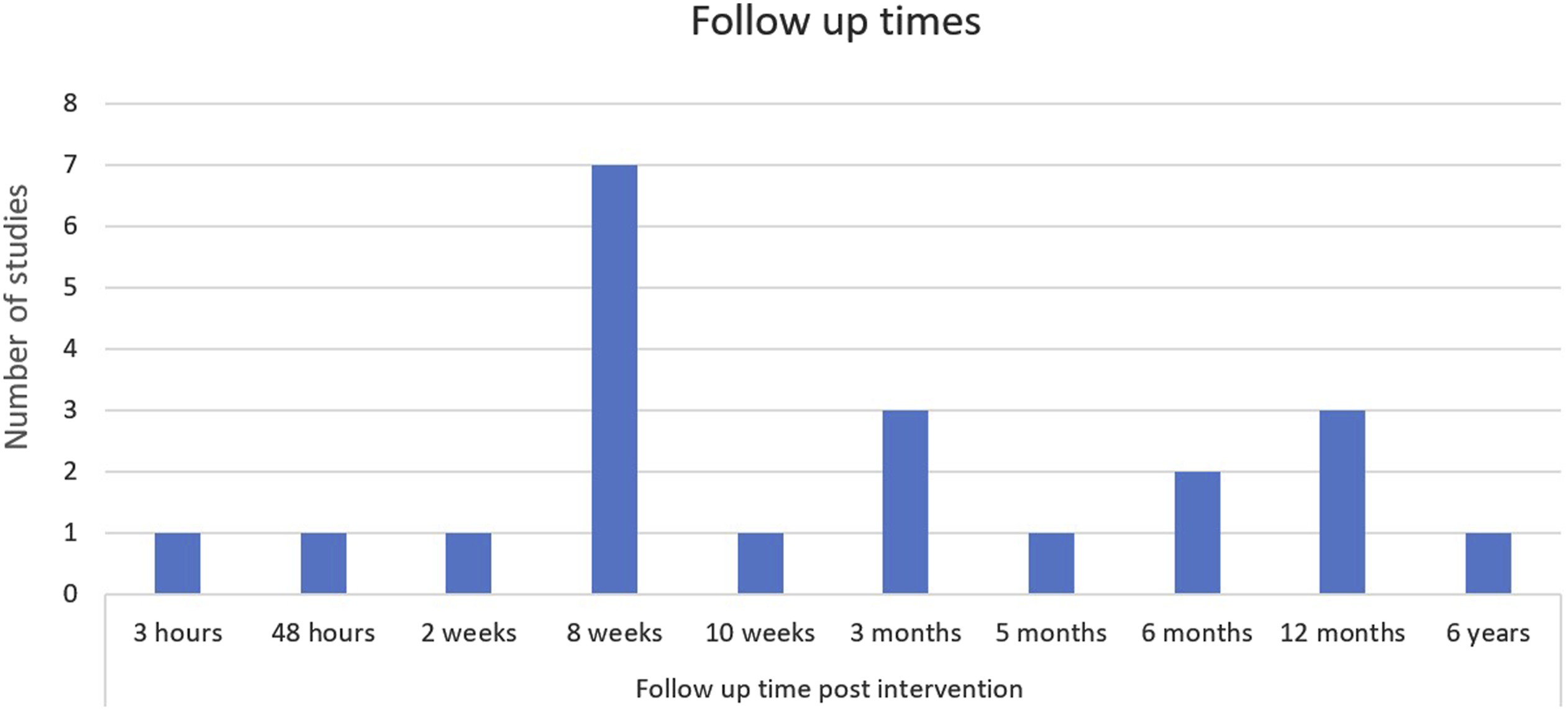
Follow-up times
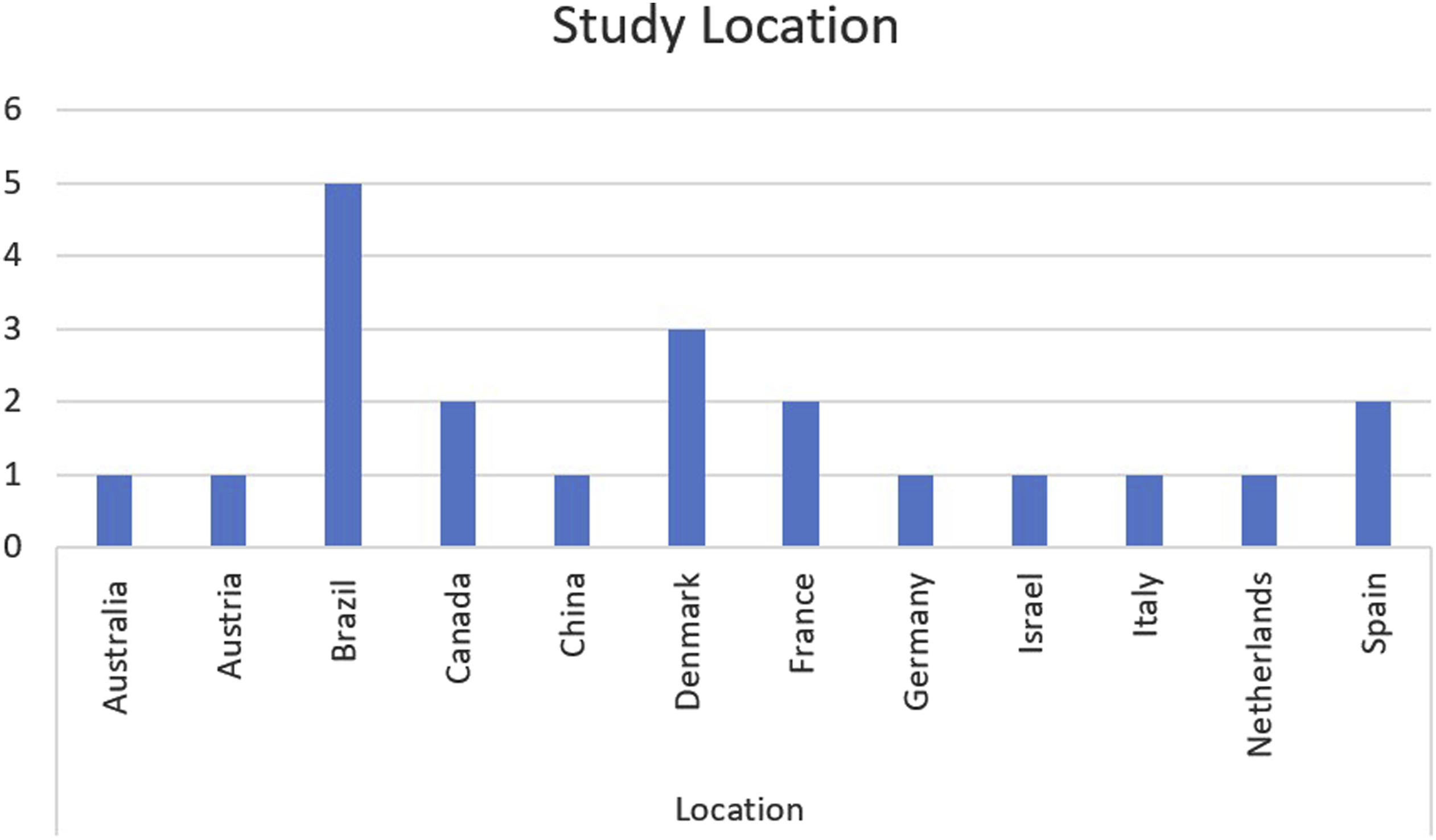
Study location
Summary of Outcome Measures of Included Studies.
Table 3 acronyms: FODMAP – fermentable oligosaccharides, disaccharides, monosaccharides and polyols, VAS – visual analogue scale, GIQoL – gastro-intestinal quality of life, EHP – endometriosis health profile, NRS – numeric rating scale, PSS – perceived stress cale, SF-36 – short form health survey, GAD – generalised anxiety disorder 7, PHQ – patient health questionnaire 8, PCS – pain catastrophising scale, PPT – pressure pain thresholds, FSFI – female sexual function index, DDS – deep dyspareunia scale, ESSS – endometriosis symptom severity score.
Table 3 below provides a summary of the outcomes of each included study. This includes pain outcomes and other domains (such as quality of life).
All 21 studies included consisted of different methodologies. Nine were randomised controlled trials, three were other experimental design with a control group while the remaining nine did not have a control comparison. Seven were pilot studies. Participants in each study were women over the age of 18 with a diagnosis of endometriosis. This diagnosis was either clinical, or through imaging (ultrasound or MRI) or surgery. One study included participants with a diagnosis of adenomyosis. 42 Participant numbers varied from ten to 300, with 50% of studies including less than 30 participants. The follow-up time ranged from 3-hours to 6 years post intervention. There were four studies analysing the impact of the lifestyle domain of nutrition, two for physical activity, eight for mind-body interventions and seven for other interventions. Two of the articles analysed the impact of social connection as a secondary outcome.
Positive results obtained with the following interventions demonstrated a statistically significant positive impact on pelvic pain management in women with endometriosis: - Nutrition – The low FODMAP diet and dyspareunia,
28
Mediterranean diet and dyspareunia, non-menstrual pelvic pain, dysuria and dyschezia,25,27 gluten free diet and pain symptoms
26
- Physical activity – ‘Physio-EndEA’ and dyspareunia
29
- Other interventions – The virtual reality program ‘Endocare’ on acute pain intensity,
42
‘School of Endo’ digital health tool on neuropathic pain,
40
‘Endo-App’ on pain,
45
TENS on pain,
39
chronic pelvic pain, dyspareunia and dyschezia43,44
Discussion
This scoping review returned 21 relevant studies which examined the impact of different lifestyle interventions in pain management in women with endometriosis and/or adenomyosis. The 21 studies all varied in terms of methodology, participant numbers, intervention and follow-up time. This heterogenicity between studies impacts the ability to develop comparisons between interventions while the methodologies and low participant number impact the external validity of the results obtained.
Despite this, the positive pain outcomes identified are consistent with other chronic pain research which has demonstrated positive impact with nutritional, 46 physical activity 47 and mind-body31,38 interventions, however, further well-designed, rigorous, and large-scale trials are also required in this chronic pain area.
There were mixed results from mindfulness-based interventions. With two studies demonstrating a positive impact from mindfulness-based intervention on pain (Kold et al. (2012) and Moreira et al. (2022))34,37 while two studies (Hansen et al. (2023) and Miazga et al. (2024)) demonstrated no improvement on pain.35,36 Miazga et al. (2024) hypothesises that the limited impact on pain in their study may be due to participants experiencing chronic pain for an average of 13 years and thus the neurological changes that occur with chronic pain may require a longer intervention with mindfulness to build new neuronal pathways. 36 The participants in Hansen et al. (2023) also had an average length of pain of 13 years prior to the intervention while those in the study by Moreira et al. (2022) only had a 7-year history of pain.35,37 There was no chronic pain timeframe recorded in the study by Kold et al. (2012). 34
Suggested Management Plan Clinician May Choose to Implement With Their Patients.
Research Gaps & Future Priorities
Significant research gaps have been identified. Firstly, there were no interventional trials identified examining sleep, or substance cessation interventions on pain associated with endometriosis. This is despite many observational studies illustrating that often women with endometriosis experience poor quality sleep and high levels of insomnia.48,49 It is also known that poor sleep has a direct impact on inflammation and the pain response. 50 Consequently, it can be hypothesised that interventions which aim to improve sleep quality and quantity in women with endometriosis may be associated with improvement in pain.
Similarly, there have been studies which illustrate an association between moderate alcohol use and endometriosis development. 51 Alcohol is also known to be associated with increased inflammation.52,53 Thus, it could also be hypothesised that decreasing alcohol intake may improve pain associated with the chronic inflammatory condition of endometriosis.
Adenomyosis was only included as a diagnosis in one of the included studies despite at times co-existing with endometriosis and impacting between 8.8% and 61.5% of women. 6 Given that adenomyosis and endometriosis share similar features, it is predicted that many of the lifestyle interventions which show positive outcomes in endometriosis may show similar results in adenomyosis. However, intervention trials involving patients with only adenomyosis would be paramount to confirm this hypothesis. This is particularly important when considering non-pain outcomes (such as infertility), given current fertility sparing treatment for adenomyosis is largely limited to hormonal options.
Both endometriosis and adenomyosis are chronic conditions impacting women of childbearing age with symptoms potentially lasting from menarche to menopause. Despite this, most of the intervention trials included had a follow-up period of less than 6 months. It should be a priority for future research to have longer follow-up periods or follow-up studies conducted to analyse the long-term impact of specific lifestyle interventions on these chronic conditions.
It is interesting to consider the developing role of digital media in the lifestyle management of endometriosis and/or adenomyosis. There were five studies identified which utilised digital programs as intervention, and all were published since 2023.30,36,40,42,45 A digital program has the possibility of impacting a greater number of endometriosis sufferers and does not require any initial or ongoing allied heath support which also improves access.
Digital programs also have the possibility of being multi-modal, covering different lifestyle pillars with education and interventions across the breadth of lifestyle medicine. Given that all lifestyle pillars included in this review demonstrated some positive outcomes, it can be hypothesised that multi-modal lifestyle interventions may be effective in long-term management in endometriosis and adenomyosis. This was demonstrated by Breton et al. (2025) 40 and Rohloff et al. (2024) 45 both of which had a multi-modal intervention and reported positive impacts on both pain and quality of life. This multi-modal lifestyle approach is consistent with current recommendations for the management of chronic pain. 54 Further well-designed, rigorous, and large-scale randomised controlled trials looking at multi-modal interventions in the pain management of endometriosis and adenomyosis are vital.
Of the intervention trials included in this review, seven were pilot studies, six of which were published within the previous three years. This is over one quarter of the studies included. This may demonstrate that there is growing interest in the lifestyle management of endometriosis and thus in subsequent years there may be further, higher quality, intervention trails published in this area. Consistency in methodology and intervention in these future studies would allow for the completion of systematic reviews and meta-analysis.
Strengths & Limitations
There are several limitations to this review. Firstly, as outlined in the introduction, endometriosis can cause not only pelvic pain, but also negatively impact other factors such as fertility, quality of life, mental health or need for repeat surgery. A limitation of this scoping review is the focus on pain management as the primary outcome. Many of the studies analysed the secondary outcomes of quality of life and mental health and illustrated significant benefits, however, these outcomes were not the focus of this review. Given the search protocol and inclusion criteria were limited to studies with pain as an outcome, studies with only non-pain outcomes were either not identified during the search or excluded during the screening process. Consequently, there may be other published interventional research which demonstrates benefits in outcomes, such as quality of life, fertility or mental health, in women with endometriosis which were not included in this review. This is clinically relevant as improvement in these outcomes are likely to be of interest to endometriosis or adenomyosis sufferers. Of the studies included in this review, there were three studies included which demonstrated improvement in quality of life or mental health domains despite no impact on pelvic pain including the environmental enrichment program 41 and two psychological interventions.35,36 When developing future review or intervention trials it would also be important to expand the analysed outcomes of lifestyle interventions to include factors such as fertility, surgery use, quality of life and mental health in addition to the pain symptoms.
Secondly, the database search for this scoping review was limited to only English language studies. This is a limitation as it does not include the whole scope of the topic as there may have been non-English trials conducted and published. Given the breadth of lifestyle medicine, developing a search protocol which covered all the pillars and self-management strategies may be challenging. The authors feel that the included search was comprehensive however it is possible that an alternative search protocol may harness different results. Two additional papers were identified and incorporated when hand-searching the reference list of originally included studies from the search protocol.
Finally, title, abstract and full text screening was conducted by two authors (BH & ND) however data extraction was only conducted by one author (BH). Previous studies have demonstrated a 10.76% error rate by human reviewers during abstract screening. 55 Having two reviewers decreases this error rate. 56 Consequently, having two authors involved in abstract and full text screening is a strength of this study as it reduces the risk of errors during study selection. However, having only one author for data extraction is a limitation as studies have illustrated a high rate of data extraction errors of up to 50%. 57 Thus, it is recommended to have dual-reviewer data extraction to reduce this risk of error. 58 There is a risk of bias in this review with the potential for biased results and wrong conclusions drawn.
Conclusion
This report aimed to retrieve and examine the evidence for lifestyle interventions in the management of pelvic pain associated with endometriosis and/or adenomyosis. 21 relevant articles were retrieved which varied significantly in trial design, participant numbers and follow-up. Outcomes illustrated potential effectiveness for dietary changes, physical activity, brief mindfulness interventions, yoga, multi-modal digital programs and TENS, however due to study heterogeneity and often low participant numbers, definitive conclusions cannot be drawn.
Further research is paramount in this area and should also be extended to include further outcome domains in addition to pain, such as quality of life, fertility and mental health. It will be equally important to include interventions involving the lifestyle pillars of sleep and substance use. Participants with adenomyosis must also be included in future research.
Future well-designed, rigorous, and large-scale randomised controlled trials studies would allow for systematic reviews or meta-analysis to be undertaken and ensure high quality evidence is collated. This could lead to updated guidelines, and improve care, for the many women suffering from endometriosis or adenomyosis.
Supplemental Material
Supplemental Material - What is the Evidence on Lifestyle Interventions for the Symptom Management of Pelvic Pain in Women With Endometriosis or Adenomyosis? A Scoping Review
Supplemental Material for What is the Evidence on Lifestyle Interventions for the Symptom Management of Pelvic Pain in Women With Endometriosis or Adenomyosis? A Scoping Review by Bethany Hough, Sam Manger, Natalie Drever in American Journal of Lifestyle Medicine
Footnotes
Ethical Considerations
There are no ethical requirements for this project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, BH, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online