
Abstract
Bone loss is a significant public health burden, with low bone mass affecting nearly all post-menopausal women. The Bone Health and Osteoporosis Foundation (BHOF) reports that over 10 million Americans have osteoporosis with 40-50 million at risk due to low bone mass. Bone deterioration culminates in fractures, shortened stature, disability, and premature morbidity and mortality. Low bone mass is under-diagnosed, despite the availability of preventive screening. Maximal bone mass acquisition is optimized during early adulthood in females after which bone remodeling can no longer replace old bone. Reducing women’s bone loss burden requires recommendations that improve overall health, maximize optimal bone mass during adulthood and minimize loss of bone following menopause. Total body composition, measurable by DXA (Dual-energy X-ray Absorptiometry), and maximum aerobic capacity (MAC) can reduce premature morbidity. Prevention strategies involve regular DXA screening beginning in adolescence to monitor whole body composition accompanied by cardiorespiratory fitness (CRF) assessment. DXA scans are now the gold standard for quantifying body composition metrics. Counseling by the Lifestyle Medicine provider should accompany and explain these evaluations. Whole-body DXA monitoring as well as fitness assessment throughout life, can provide women with improved awareness of health metrics and improve overall quality of life outcomes.
Keywords
“DXA studies are proven to be safe, quick, precise/reproducible, and inexpensive compared with CT or MRI.” “Living systems are worn out by inactivity and developed by use.” Albert Szent Gyorgyi
1
AIMS Statement
Expert opinion and review of women’s body composition, bone health and cardiorespiratory fitness with an emphasis on early prevention through lifestyle changes over the lifespan.
Introduction
Osteoporosis is the most prevalent metabolic bone disease worldwide, but often remains unrecognized until the occurrence of vertebral, hip, wrist or other fractures.
2
It is non-communicable but can be spread by the habit of inactivity. Cosman, et al, note that “bone mass in older adults equals the peak bone mass (PBM) achieved by age 18-25 minus the amount of bone subsequently lost.”
3
However, our present “post facto” patient education and testing is suboptimal to allow timely prevention. Current bone health surveillance guidelines recommend screening with DXA at age 65 which makes it a secondary or tertiary (i.e., salvage care) prevention modality, at best, rather than allowing primary prevention.4-6 Over 25 years ago, Bailey wrote: “One of the best predictors of bone mineral status in the elderly is the level of peak bone mass attained by the early adult years.”
7
Baxter-Jones, et al reported that “60% of the risk of developing osteoporosis is dependent upon the bone mass accrued in early adulthood.”
8
Gunter et al, cognizant of these “childhood antecedents,” cite the osteogenic potential of youthful physical activity and ground reaction forces (GRF) as “powerful preventive strategies in the fight against osteoporosis.”
9
They further suggest that physical activity (PA) “undertaken during or before puberty may have greater positive effects on bone mass than many pharmacological interventions undertaken by adults with osteoporosis.” In our management of bone health disorders, it is therefore important to recognize that skeletal growth is largely completed by the third decade of life. Revised and proactive bone health screening recommendations are needed. By the time a woman reaches age 65, when scanning is now typically initiated, she may already have lost substantial bone mass with limited opportunity for recovery or normalization (Figure 1). The full scope of osteoporosis prevention strategies: a new paradigm. Optimal accrual of peak bone mass by the third decade of life may significantly affect the bone health over the lifespan. Early childhood activity has important skeletal benefits in the adult. The projected trajectories of bone mineral density are highly dependent on nutrition, physical activity, genetics, environmental circumstances and lifestyle. This graphic represents projected trajectories based on theoretical modeling and adapted from known literature.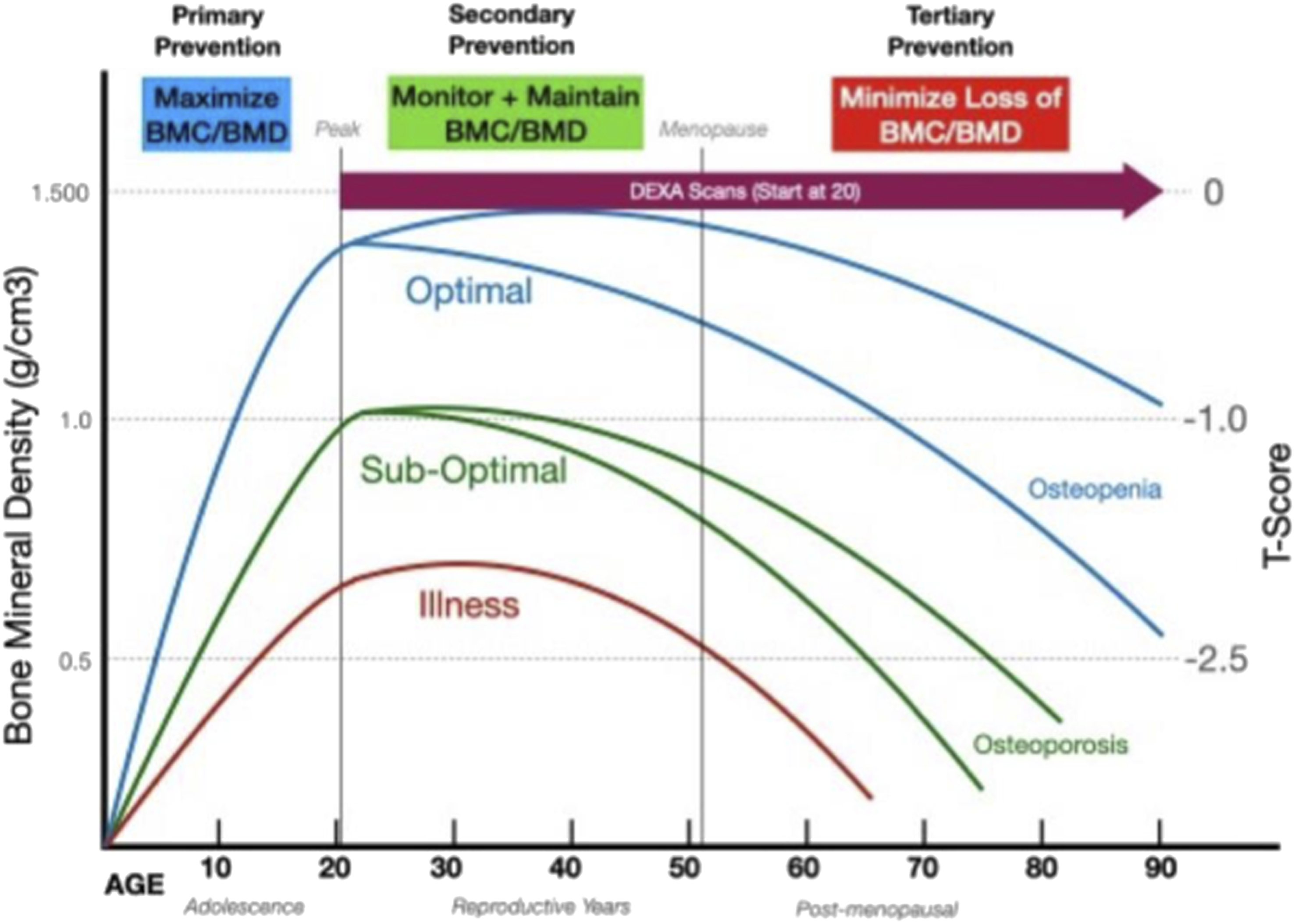
Innovative primary prevention bone health strategies would provide women with access to whole-body DXA assessments, as well as fitness testing, throughout their lifetime to optimize total body composition (TBC) and reduce risk for bone deterioration as seen in Figure 1. 10 Contemporary DXA scans are now the criterion method for evaluating bone mineral density (BMD) with T-scores (reference-based) and Z-scores (age-based). DXA can also provide whole body fat percentage (BF%), body fat mass (BFM) and non-fat/lean mass (NFLM) and NFLM%. 11 An additional DXA analytic is the Trabecular Bone Score (TBS) that adds a three-dimensional voxel metric to BMD to allow a more complete assessment of vertebral microarchitecture.12,13 This allows elaboration of the two dimensional quantitative areal BMD to a volumetric (voxel) BMD that provides a more qualitative assessment of the bone. 14
Whole-body DXA is significantly more accurate and effective at measuring adiposity, which can predict cardiorespiratory fitness and overall health, than body mass index (BMI), bioimpedance (BIA), body anthropometry (BodPod), skin calipers or similar metrics.15,16 Bosch, et al, have reported that higher fitness, measured as VO2 peak, is associated with significantly lower percent body fat and higher insulin sensitivity. 17 While these tests need to be expanded to the general population it appears that improved metabolic outcomes are better predicted by the interaction between fitness and fatness in both genders. The ability of DXA body composition, based on measurement of the muscle-fat axis, to predict maximum aerobic capacity and/or cardiorespiratory fitness (CRF) offers new insight as a quantitative predictor of all-cause mortality and cardiovascular events in men and women. 18
Scope of the Problem
Epidemiologic data from the BHOF sponsored “Clinician’s guide to prevention and treatment of osteoporosis” provides recommendations for osteoporosis management for “postmenopausal women and men aged 50 years and older.” 19 Citing NHANES III data from 2017-2018 they note that approximately 10.2 million American adults, (approximately 8 million women and 2 million men), age 50 and older have osteoporosis, and 43.4 million have low bone mass, that is, osteopenia. Lack of awareness of this disorder has led to its moniker of “the silent disease.” There are approximately 2 million cases of osteoporotic fracture per year which exceeds the number of cases of heart attack, breast cancer and prostate cancer combined. Women account for 71% of fractures and 75% of costs; 27% of fractures are vertebral, 19% wrist, 14% hip, 7% pelvis and 33% other. 20 Hip or spinal fractures are known to be associated with significantly reduced quality of life, chronic back pain, kyphosis, height loss, disability, loss of independence and shortened lifespan. Comorbidities exacerbate these injuries and about 30% of people with a hip fracture will die within a year. 21
Annually, AAOS Clinical Practice Guideline Summary notes >325,000 hip fractures in the US annually, with a mean age of 77 years, 2/3 female, a mean hospital stay of 5.3 days (then transfer to transitional care) and aggregate costs of $5.8 billion. 22 Most hip fractures occur in persons over age 65, 95% are due to falls, around 75% are in women, and require emergent surgical treatment with recovery in hospital. Additionally, hip fractures often limit subsequent independence and increase premature mortality. In 2021, the osteoporosis related fracture costs in a Medicare population with mean costs of $47,163 were: hip fracture -$71,057, spinal fracture -$37,543 and wrist fracture ∼$24,505. The one year death rate was 18% vs 9.3% for those without fracture. 23
Bone Health Integrity and Policy
Osteoporosis and osteopenia fall on the spectrum of common bone loss related conditions causing structural weakness and brittleness that predispose an individual to an increased likelihood of fractures.24,25 Historically, lifetime bone loss of up to 35% of peak cortical bone mass and up to 50% of trabecular bone or osteoporosis has been recorded since human origins. 26 Like all cells in the human body, bones undergo cellular senescence that contributes to age-related bone loss and fragility. 27 Nutritional and hormonal considerations are a vital concern as well. 28 As such, the challenge to optimizing/maximizing one’s peak bone mass and density in adolescence is all the more compelling.
Lifelong skeletal integrity is dependent on the accrual of maximal bone mineral during the growing years as measured by peak height velocity (PHV) which is a benchmark for maturity. 7 Peak Bone Mass (PBM) and peak BMD are only achieved during the dynamics of adolescent growth. Various studies have demonstrated that females reach peak total bone density between the ages of 16-22 and males between the ages of 17-25. In adults, remodeling is a coupled interaction of osteoblastic new bone replacing osteoclastic resorbed bone, that results in a net bone loss over time. As Bailey points out, the difficulty is in developing public health strategies to inform the behaviors of young people who will not be “at risk” for 40-50 years. “The ultimate target population for the prevention of osteoporosis may be the young and not the elderly.” 7
The direction of women’s bone health management derived largely from a 1992 meeting in Rome of the 16-member group that provided guidance in the 1994 Technical Report Series 843 titled: “Assessment of Fracture Risk and its Application to Screening for Postmenopausal Osteoporosis.” 29 They defined osteoporosis as “A disease characterized by low bone mass and microarchitectural deterioration of bone tissue, leading to enhanced bone fragility and a consequent increase in fracture risk.”
The present guidelines evaluating women for this problem of suboptimal bone mineral density were initially established by the WHO and endorsed by the United States Preventive Services Task Force (USPSTF) and other medical groups. 4 The USPSTF recommends bone density screening for women age ≥65 years and women age 60-64 years at increased risk for osteoporotic fractures (B Recommendation). They offer no recommendations for or against screening post-menopausal women age <60 years or women age 60-64 years without increased risk (C Recommendation).
In the United States, women and men are eligible for Medicare coverage for healthcare upon reaching the age of 65 years. The “Bone Mass Measurement Act of 1997” was enacted to assure the “Medicare recipients are potentially eligible for reimbursement of bone mass measurements.” This was specifically in the context of diagnosing osteoporosis and to assess efficacy of an FDA-approved drug therapy.
Payment by insurers for the evaluation of osteoporosis or osteopenia prior to age 65 or for body composition analysis is highly variable. 30 Some insurers deny payment of total body composition with DXA before age 65 because it is considered experimental, investigational, or unproven for body composition testing. Coverage is usually dependent on being deemed a medical necessity rather than an elective procedure or surveillance. The adherence of the WHO and the USPSTF to the age of 65 is based more on reimbursements rather than specific physiologic justification or indication of this age as a threshold. Either the age of menopause (51 years in the US) or peak bone density accrual by age 20-30 might be more logical test parameters.
Muscle Health and Osteosarcopenia
Closely coupled to advancing bone loss is concomitant muscle mass reduction (sarcopenia) to the point of deficiency throughout the lifespan. Although clinically overlooked it is an important determinant of bone health and quality of life. Recognition of the interwoven nature of this relationship has resulted in the term osteosarcopenia. 31 Individuals with pre-existing deficiencies in lean muscle mass have a reduced likelihood of normal recovery following a fall-related fracture or other injury. Due to this connection, over 50% of women 65 years or older having a hip fracture due to a fall are less likely to ever walk again. 32
Exercise is known to provide a medicinal effect which improves mitochondrial health, enhancing and preserving the function of aging muscle along with improving quality of life. 33 A decrement of muscle can occur because of an imbalance between muscle protein synthesis (MPS) and muscle protein breakdown (MPB). Muscle atrophy can occur due to aging, disuse, injury, or illness. Of concern is the fact that atrophy of muscle mass due to injury or disuse can typically be reversible in youth, but may be irreversible or progressive when associated with prolonged periods of disuse and aging. 34 High levels of pro-inflammatory cytokines can increase the MPB and suppress MPS. Reduced muscle lean mass is associated with a higher incidence of chronic diseases such as diabetes mellitus, cardiovascular disease, and depression. 35 Therefore, the ability to provide interval measures of body lean mass is important surveillance data for health intervention guidance.
The muscle-bone unit “mechanostat” theory demonstrates that bone mass follows muscle mass. The German anatomist, Julius Wolff, and later Frost, showed that bone competence depends on either impact from mass or strain forces from skeletal muscle contractions. 36 Notably, the dominant arm of a tennis player is typically larger in both muscle mass and bone structure due to the increased use of that extremity. 37 There is no direct weight bearing involved in a tennis player’s dominant arm, yet bone mass increases in response to the muscle traction and levering forces. 38 This is enhanced if the athlete is competitive before reaching skeletal maturity. 39 Belinda Beck in “Exercise Prescription for Osteoporosis: Back to Basics” writes: “muscles have the capacity to exert larger forces on bone than gravity, and the withdrawal of muscle force also is associated with bone loss. 40 Consequently, rowing, swimming, cycling and cross-country skiing are superb activities for building healthy muscles, bones, and cardiovascular fitness. 41 There are benefits from cross-training that combine resistance, anaerobic and aerobic activity, while helping to avoid injury and provide a well-rounded fitness program.
Dengel et al, has described the muscle-to-bone ratio (MBR) comparing athletes with normal controls to demonstrate the synergistic relationship between lean mass and bone mass. 42 Barber, et al emphasize the vital relationship between skeletal muscle (myokines) and adipose tissue (adipokines) in influencing overall metabolic health. 43 Sarcopenic obesity, which often accompanies aging, is a clinical modulator that compromises the body’s overall energy balance. Frailty or disablement are associated with loss of independent physical function and can be predicted based on metrics of cardiorespiratory fitness, grip strength, and gait speed. Skeletal muscle strength & power have a vital influence in preserving independent physical function during aging. 44
A common sign of aging is the head forward, drooped over the chest, shoulder-hunched posture of hyperkyphosis previously termed a “dowager’s hump.” Advanced kyphosis of the upper thoracic and cervical vertebrae occurs when the paranuchal and thoracolumbar fascia (TLF) and erector spinae extensor muscles that normally provide postural support to hold the head upright are no longer able to do so. To have good posture, one needs the muscle strength to “stand up straight” as our mothers advised. A modern society with excess time slumped in front of the screen, behind the steering wheel or at the computer has compromised our skeletal alignment. The weight of the head is 8-12 pounds and the downward force can cause anterior wedging compression fractures of the demineralized cervical and thoracic vertebra along with intervertebral disc desiccation/collapse over time that results in a marked curvature and shortened height. Some women (and men) can lose up to 10 cm (4 inches) of height over the lifetime. The current USPSTF guidance endorses vertebral scanning in post-menopausal women/and men who have “historical height loss of 1.5 inches or more” (>3.8 cms). Vertebral fractures are often described using the Genant classification in 3 grades of wedge, biconcave or crush deformity. 45 Quality of life, height, mobility, and lung capacity may be affected in the advanced age population by the loss of muscle mass and progressive sarcopenia that fails to stabilize the spinal column and skeletal structures. Successful rehabilitation and recovery depends on optimizing muscle mass and skeletal function. 46
Physical Activity and Cardiorespiratory Fitness
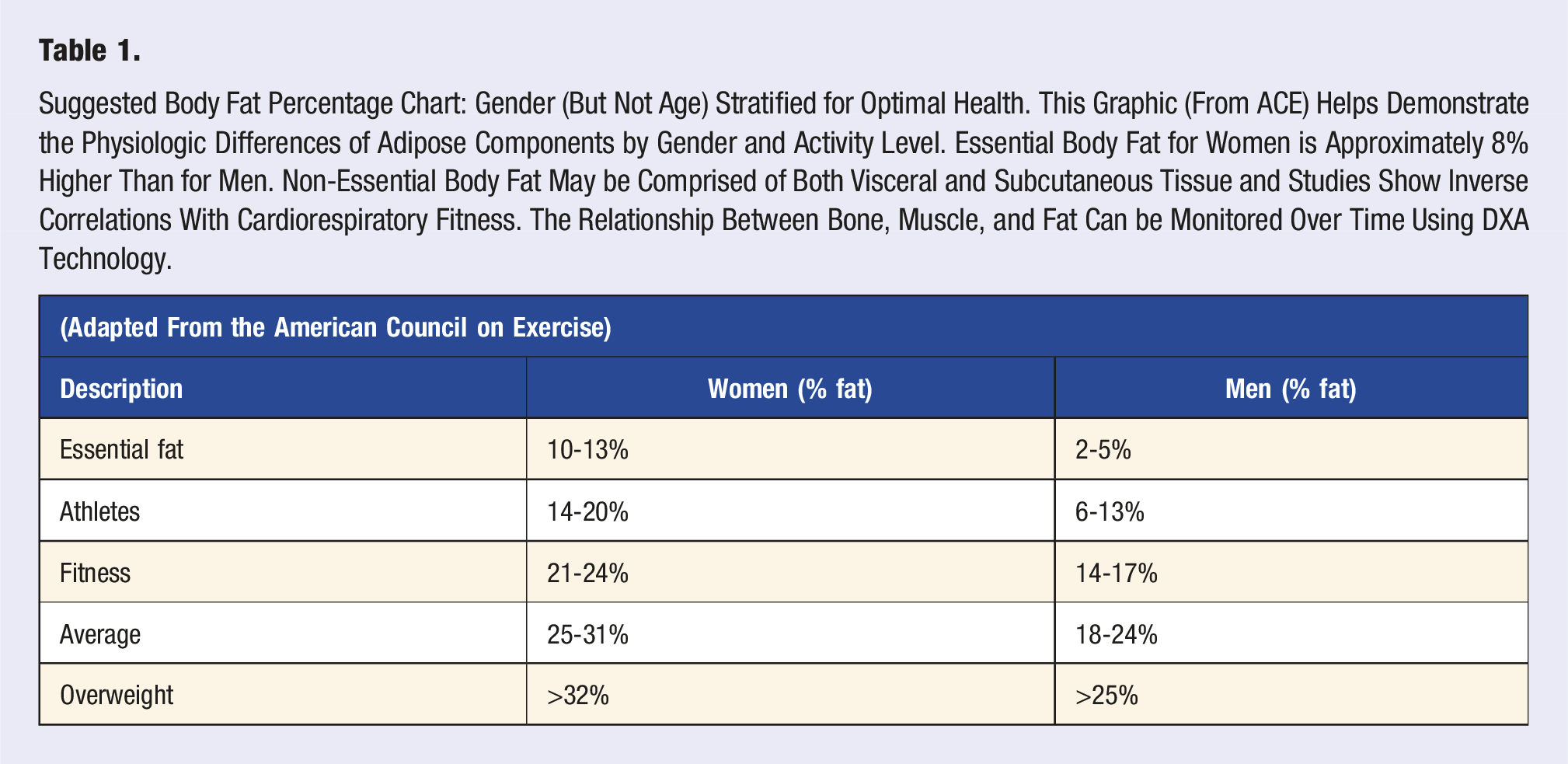
Suggested Body Fat Percentage Chart: Gender (But Not Age) Stratified for Optimal Health. This Graphic (From ACE) Helps Demonstrate the Physiologic Differences of Adipose Components by Gender and Activity Level. Essential Body Fat for Women is Approximately 8% Higher Than for Men. Non-Essential Body Fat May be Comprised of Both Visceral and Subcutaneous Tissue and Studies Show Inverse Correlations With Cardiorespiratory Fitness. The Relationship Between Bone, Muscle, and Fat Can be Monitored Over Time Using DXA Technology.
Few patients are familiar with body composition or know their actual body fat percentage or bone mineral content. Nor have many participated in an exercise stress test or know their maximal oxygen uptake (VO2max) capacity. Yet volumes of medical and exercise physiology literature have established the relationship between low levels of adiposity, high cardiorespiratory fitness (CRF) and overall wellness and longevity. 51 Many, like Ross and the American Heart Association (AHA), now assert that CRF is an individual’s most important predictor of mortality, and that it should be measured or estimated routinely as a “clinical vital sign” at office visits. 52 The literature is strong in its advocacy for such recognition and the creation of databases that allow age and gender stratification for this physiologic metric.53,54 A predictable degree of “fragility” and loss of independence is associated with a VO2max of about 5 METs (17.5 mL/kg/min) physiologic capacity.
The test that measures the ability to exchange oxygen is called a VO2 max test. 55 “Max” because ideally, we can exercise to a maximum effort that elevates heart rate and cardiac output to upper limits. This cardiorespiratory function is considered the most important measure of your biologic capacity and a predictor of longevity. Typically, the test is done running on a treadmill or spinning on a bike ergometer with a mask on the face to collect and measure the oxygen and carbon dioxide gases. Less precise, but less timely and costly, is the use of personal physical measurements and behavioral metrics that utilize a regression analysis formula to predict cardiorespiratory fitness (CRF). 56 The calculation of one’s VO2 can be compared to others based on gender, age, ethnicity to arrive at a “Fitness Age.” There are people who at age 65 have the fitness of someone 80 years, and some at age 65 who have the fitness level of a 40-year old. In America, there are young sedentary people who have the “Fitness Age” of a person decades older. 57 This decline may presage later premature frailty or fragility. The ACSM, 12th ed. Guidelines for Exercise Testing & Prescription provide age and gender, stratified charts for the assessment of activities, such as VO2 max, percent body fat, grip strength, push-ups, & waist circumference.
Optimal Aging
Walter Bortz, MD in his paper titled “How fast do we age? Exercise performance over time as a biomarker,” discusses the importance of cardiorespiratory fitness as “a global measure, not only of basal circulatory, respiratory, thermoregulatory, metabolic, musculoskeletal, and neurological function, but those under an exercise load.”
58
He noted that in the aging process all organ functions decline at approximately 0.5% per year even in the healthiest and most active individuals after age 35. The “masters athlete” provides a unique population for the study of healthy aging.
59
(Figure 2). Optimal aging depends on limiting the rate of decline of essential organ function over the lifespan. This graphic is based on theoretical modeling of known habits, behaviors, studies and case series. The projected trajectories derive from the work of Dr. Bortz showing 0.5% decline in body functions over time from age 35 through 65. This also reflects the work of Hayflick showing the inevitable homeostatic organ decline of approximately 50% by age 85.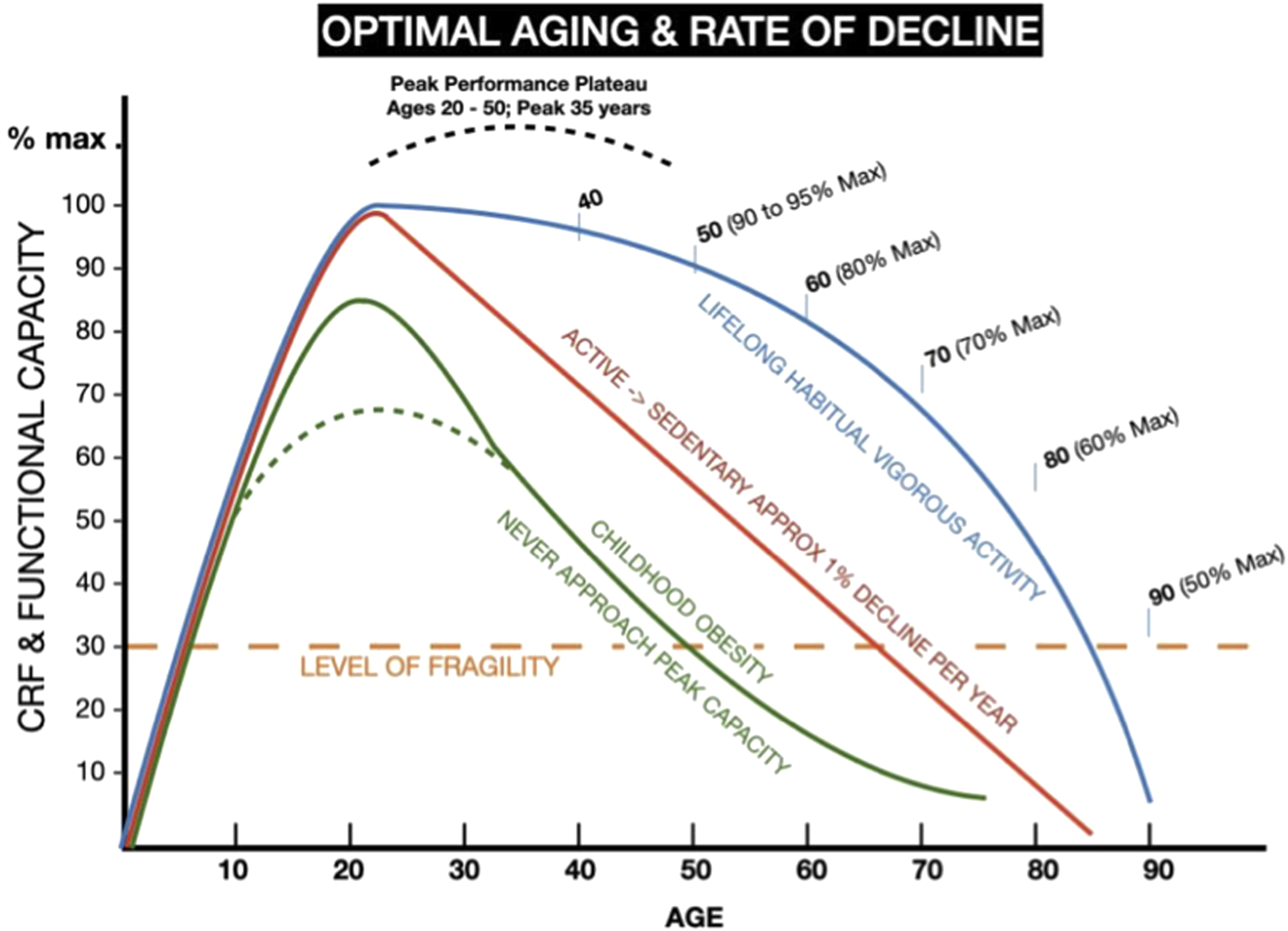
Master’s athletic organizations exist to provide adults, generally ages 19 to 100+, with opportunities to participate and compete in various sporting activities such as running, swimming, track & field, cross-country skiing, cycling, baseball, rowing, etc. Many sporting organizations have regional, national and international competitions that are generally stratified by gender and 5-year age groups for competitions. Olga Kotelko, was a Ukrainian-Canadian woman who competed in track & field running sprints, throwing and jumping events until age 95 and held over 20 world records. A book called “What makes Olga run?” documents her life. 60 Legendary Dave Costill, PhD, now 89, professor emeritus at Ball State University exercise physiology labs, has been a national champion masters swimmer in multiple events. Carlos Lopez of Portugal won the 1984 Olympic marathon at age 37. Johnny Kelly, who died at age 80, ran >30 Boston Marathons. Norwegian-Canadian, Herman “Jackrabbit” Johannsen, Nordic skied until he was 100 and lived to 111. Ron Johnson was a world masters swimmer from Arizona who said: “I don’t do it to look good; I do it to feel good.” Young athletes are often chagrined to find themselves bested by 40-50 year old competitors who just never stopped exercising and only slowly slowed down. Dara Torres, the 42 year old Olympic swimmer once remarked: “The water doesn’t know how old you are.”
The Physical Activity Guidelines for Americans (PAGA) offers exercise recommendations for healthy adults as 150 minutes of physical activity per week with two days of strength training. 61 Those who do not remain active can expect to experience a decline of cardiorespiratory fitness and end organs due to compromised vascular perfusion, mitochondrial dysfunction, and a cascade of medical problems at a rate of 1-2% per year. This rate of decline results in a decreased functional ability of 30-60% by the age of 65. Buettman et al, indicate “disuse and aging are known risk factors associated with bone mass and bone quality deterioration.” This is usually evidenced by preferential loss of bone at cancellous sites, cortical thinning, and loss of bone strength due to enhanced fragility. There is increased bone resorption and decreased bone formation with bone turnover rates subject to gender, genetic variability and sex. 62 For many people, a deterioration of greater than 70%, that is, to below 30% of baseline adult function, approaches the definition of “frailty” (a VO2 of 5 METs or 17.5 mL/kg/min) which is associated with a loss of independence and the need for residency in a senior care facility. 63
All organ systems inevitably decline over time. 64 The Hayflick limit conceptualizes the “natural aging” process by observing that cells undergo a limited number of cell division cycles before their programmed cell death or apoptosis. 65 Organ systems are defined by their resilience and capacity to withstand perturbations or injury and return to baseline function. In youth and early adulthood, the recuperative plasticity of an organ is thought to be 4-11 times greater than average demand but by age 85 capacity is reduced to 50% of baseline. 66 Throughout aging, organ reserve capacity, defined as the excess functional ability beyond that needed at rest, declines as well. Lung capacity and function predictably declines on average 20-30 milliliters per year, 67 bone mass is reduced, muscles shrink, and cognition declines. 68 A “rectangularized” lifespan is the concept of reducing rate of decline to prevent a prolonged period of dependence on others, a process Jim Fries calls “compressing the period of morbidity.” 69 Non-optimal age-related bone health indicates either insufficient peak bone mass in adolescence or substantial bone loss in adulthood, either of which determines if one will incur clinical or subclinical disease. 70
Body Composition
Initially, quantification of bone mass as bone mineral content (BMC) in kgs and bone mineral density (BMD) in gm/cm2 was the primary goal of DXA. Scanning technology was focused on three sites of common concern for fracture in the geriatric population: the femoral neck, wrist, and lumbar spine. 71 Using a 1994 group of 30-year-old European females as the “normal” BMD reference cohort, the WHO defined osteoporosis as a BMD that is 2.5 standard deviations (SDs) or greater below this “normal,” whereas osteopenia is defined as between 1 to 2.5 SDs below “normal.” 72 It is of interest that, some 30 years later, there has been no follow-up analysis of the bone health outcomes of this influential cohort of women.
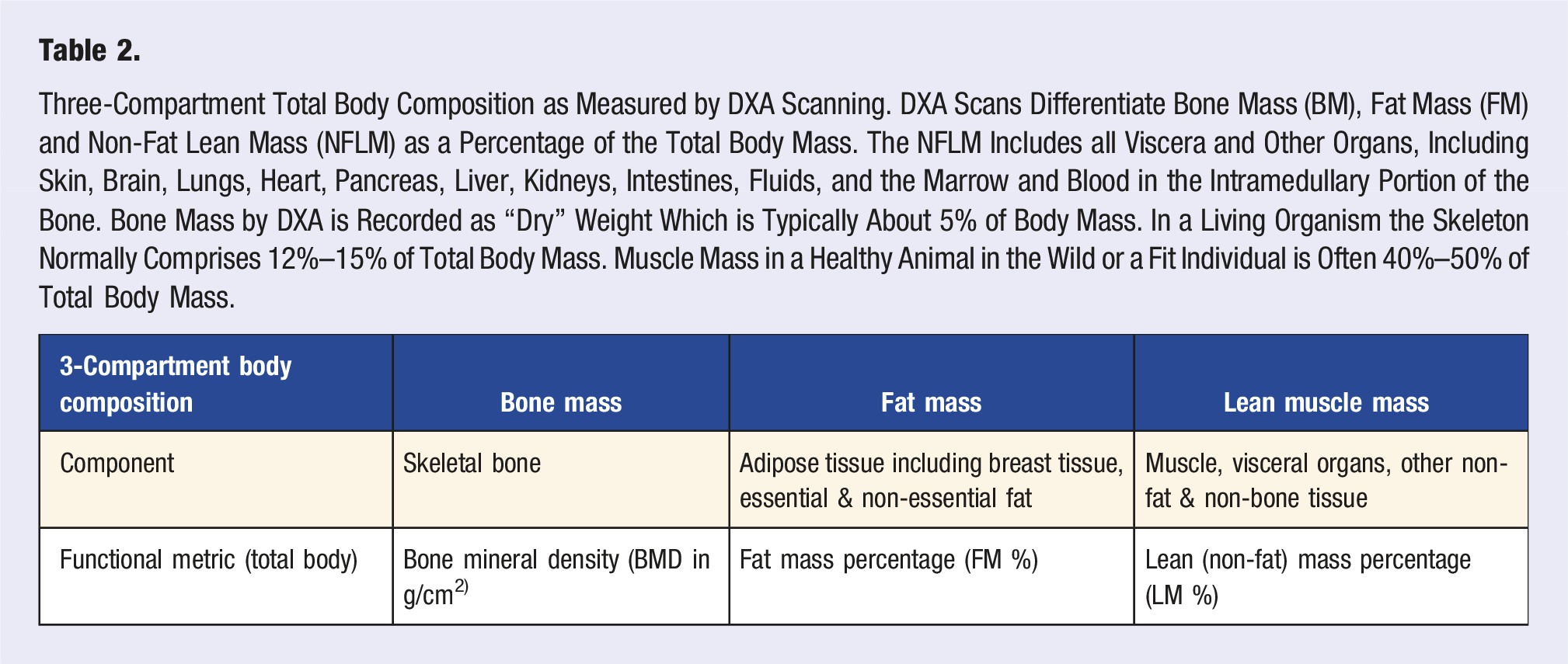
Three-Compartment Total Body Composition as Measured by DXA Scanning. DXA Scans Differentiate Bone Mass (BM), Fat Mass (FM) and Non-Fat Lean Mass (NFLM) as a Percentage of the Total Body Mass. The NFLM Includes all Viscera and Other Organs, Including Skin, Brain, Lungs, Heart, Pancreas, Liver, Kidneys, Intestines, Fluids, and the Marrow and Blood in the Intramedullary Portion of the Bone. Bone Mass by DXA is Recorded as “Dry” Weight Which is Typically About 5% of Body Mass. In a Living Organism the Skeleton Normally Comprises 12%–15% of Total Body Mass. Muscle Mass in a Healthy Animal in the Wild or a Fit Individual is Often 40%–50% of Total Body Mass.

Whole-body DXA scanner. Imaging typically takes less than 10 minutes of actual scan time. GE Lunar and Hologic are the two major DXA manufacturers in the US. The precision of these machines is typically less than 2% and they are regularly tested using phantoms for accuracy. Radiation exposure from a DXA scan is about a 10th of a normal chest x-ray or a mammogram and is equivalent to the radiation one receives at the airport scanner or a dental x-ray.
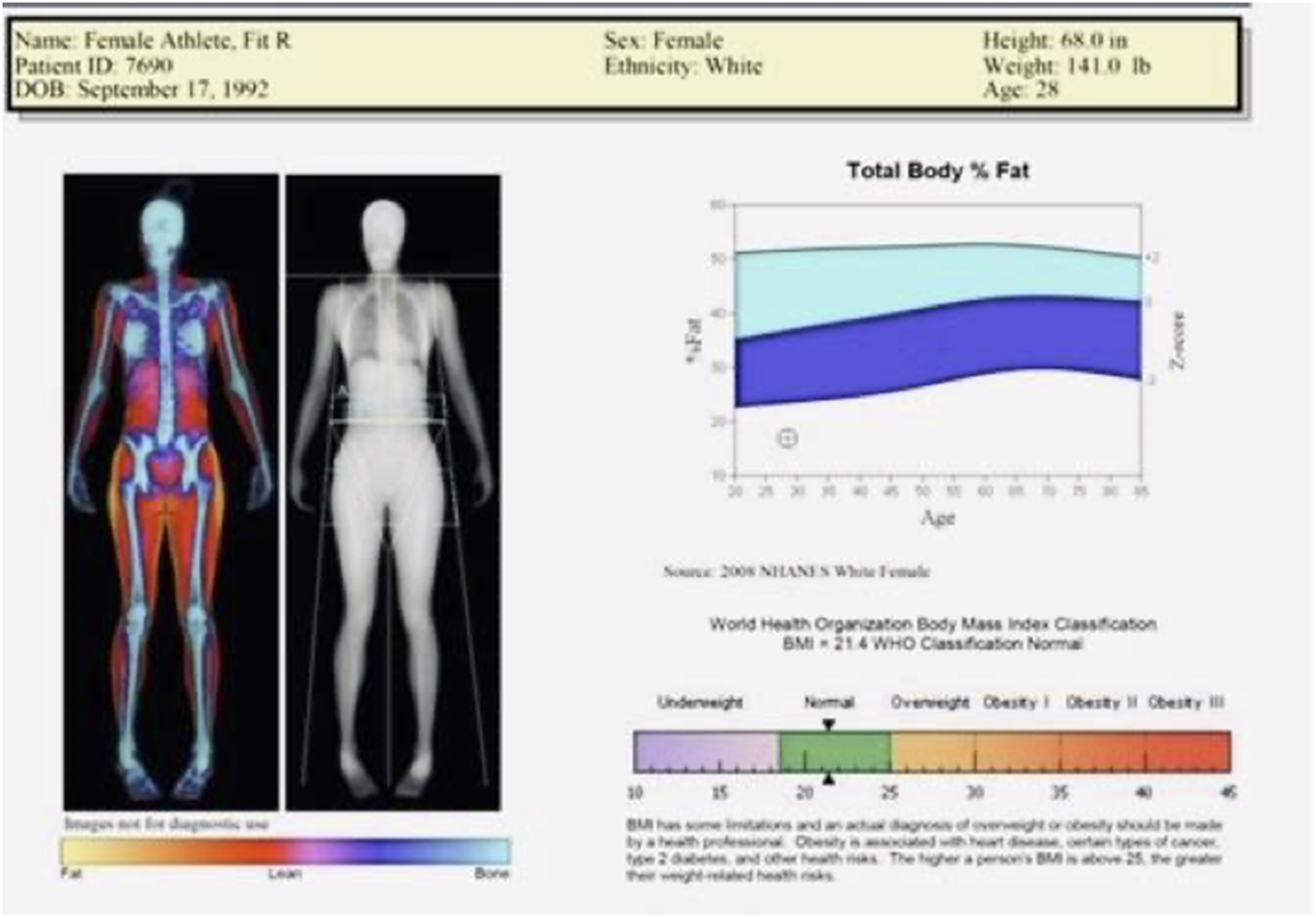
Sample DXA whole body composition report for body fat percentage. This DXA graphic demonstrates the scanning acquisition of the body, skeleton and skin layers. In this case, the total body fat percent is reported for this 33-year old female who weighs 141 pounds. Her percent body fat is ∼17%, which suggests that she is physically active with above-average cardiorespiratory fitness. Her muscle mass significantly exceeds her fat mass. The print out includes BMI; based on the WHO classification she would be categorized as “underweight” when, in fact, she is a healthy, athletic woman (see Table 1 above). Bone mineral density (BMD) and additional metrics would be elaborated on additional pages.
Increasingly it is recognized that the value of whole body composition, as reflected by the percentage and distribution of lean mass and adipose tissue in addition to skeletal bone analysis, is significantly more important than segmental analyses or body weight alone as a predictor of health & wellness. 76 Matilla et al showed in a group of 140 conscripts that increased adiposity (fat mass and fat mass percentage) identified by DXA were strong predictors of poor physical fitness. 77 DXA can uniquely provide this essential information over the lifespan with accuracy. See Image 2.
Radiation
The radiation from a DXA scan is ∼ 0.006 milli-Sieverts (mSv) which is roughly a tenth of a single CXR or a mammogram (0.04 mSv), similar to the radiation from an airport scanner, dental x-rays or a cross-country flight, and less than that received from routine environmental radiation exposure in a single day. 78 Americans typically receive approximately 3.0 milli-Sieverts (mSv) of annual exposure from cosmic radiation, household radon, and other environmental sources. Elective diagnostic imaging technologies such as computed tomography (CT) can expose the patient to 3.0 to 10.0 mSv (the equivalent of 1-3 years of environmental exposure in a single medical study). 79 The precept of As Low As Reasonably Achievable, in order to minimize radiation exposure, is readily achieved in DXA scanning due to the low mSv exposures. The Biological Effects of Ionizing Radiation (BEIR) VII report and executive summary provide recommendations and guidance regarding radiation exposure and cancer risk. 80 DXA offers a safe mode of preventative medicine.
The evolution of DXA scanning as a tool for evaluating the growing spine with longitudinal imaging can significantly reduce the radiation exposure to young scoliosis patients and individuals with cervical, thoracic or lumbar spine disease or injuries. There are also opportunities to improve spine assessment by incorporating a stadiometer into the scanner that allows more precise assessment of vertebral compression, disc narrowing, and also spinal curvature that can ultimately result in postural abnormalities, such as a cervico-thoracic kyphoscoliosis. DEXA scans can be performed with a minimal amount of radiation compared to CT scan and can be obtained much more quickly than an MRI or CT. Staffing and the need for clinical radiation shielding is also significantly reduced. A DEXA scanner can be obtained for less than $100,000, sometimes for under $50,000 (brand new), whereas CT and MRI scanners typically exceed $1,000,000.
Body Mass Index
In 1835 Adolphe Quetelet, a Flemish mathematician wrote a book called “The Average Man” [L’homme Moyen] to create a rule of proportions regarding male body habitus, and created BMI. 81 Quetelet’s notion was to divide body weight in kilograms by height in meters to the second power. The Quetelet Index, as it was originally called, was not widely applied in America until Ancel Keys, MD recommended it to the Metropolitan Life Insurance company. 82 BMI’s use should be limited to population demographics rather than individual evaluation.
BMI suffers from the significant flaws of not being age, gender or ethnically stratified. BMI does not differentiate muscle, fat, bone or any other body component. 83 BMI is not evidence of healthy weight or appropriate body composition status based on standard levels of statistical significance. BMI may be invalid 40% of the time with roughly equal number of false negatives to false positives. Yet BMI continues to be inappropriately used to make health care and policy decisions. 84 It is unfortunate that the misuse persists through most major societies and organizations in the medical arena as a surrogate for percent body fat simply because it is quick, free, and easy.
Flegal et al identified what they called the “obesity paradox” which is no paradox at all, but simply an invalid tool misapplied to its measurement task. 85 The category of males with BMI 25-29.9 kg/m2 and considered “overweight” in the BMI schema may be healthy, active individuals with a true body fat percentage of less than 20% and perhaps even down to 10% as demonstrated by Ode & Pivarnik. 86 Their study focused on college students however, the same phenomenon is seen in protective services, individuals and other adults who remain physically active. Other subjects, including many women, may have a “normal” range BMI, but have a body fat percentage of 30% or more.
Women typically have 7%–9% more body fat than men simply due to biology and BMI is neither age nor gender specific (Table 1). Aging is associated with a reduction in muscle and bone mass and with increased fat mass. 87 An individual with a BMI of 25 kg/m2 may have a body fat percentage of anywhere from 10% to 35%. BMI silos patients into categories that are not age, gender, or ethnically informed; it mislabels many fit and athletic individuals as “overweight” or “obese” and categorizes significant numbers of overweight or obese individuals as “normal.” Women often become amenorrheic when the body fat drops below 15%. Female athletes and the concerns of Relative Energy Deficiency in Sport (RED-S) formerly known as the “female triad” (disordered eating, menstrual dysfunction, and decreased bone mineral density) require careful evaluation in which the specificity of DXA can be invaluable. 88 In a study of 186 Norwegian female athletes and 145 controls, Torstveit found that of 96 controls with a “normal” BMI of 18-25, 50% had obese body fat levels averaging 33.1%. She concluded that “BMI is not a valid measure for assessing or monitoring body composition in female elite athletes and it should be use carefully in female nonathletes.” 89
Gender and Parity
Medical evaluations and outcomes have not always been gender equal. 90 In some cases, there are gender-based differences in disease, however it is imperative that we understand the risks and benefits of diagnostic procedures, available remedies, potential outcomes and consequences of treatment or lack of treatment. C-suite “executive” evaluations receive elaborative testing, which sometimes includes a DXA scan. Few Medicaid patients, patients of color, or women in general are offered such evaluations until they reach age 65 or experience a fracture. 91 These preventive services may be considered experimental or lacking evidence-based support and are rarely recommended to patients in general.
A “well-woman” assessment can be performed periodically and include a physical exam, counseling, discussions about testing, and options for treatments or optimization of health. 92 Ideally, a comprehensive assessment would begin in adolescence and covers the full lifespan. 93 Pediatric growth and wellness charts are diligently recorded through the adolescent years until being abruptly discontinued once the patient reaches 18 years of age. Whole-body DXA scans might easily be offered as part of these evaluations beginning in adolescence to assess and track bone mineral density (BMD), body fat and lean mass percentage. In addition to DXA scanning, to promote and optimize healthy aging, annual VO2 max exercise testing should be conducted to track cardiorespiratory fitness. Premature menopause occurring before the age of 50-51 can expose a woman to an increased risk of osteoporosis and cardiovascular disease. 94
Call to Action
Women lose bone mineral density as they age and do so more precipitously than men. However, we have the knowledge and tools to favorably influence the rate of bone loss over their lifetime. The challenge is compliance or adherence to a healthy diet, supplements with calcium and vitamin D, avoiding known risk factors, habitual exercise, and optimizing bone content/density/quality, muscle mass and cardiorespiratory fitness. The ability to measure a woman’s bone mass and track the arc of change allows interventions early to minimize the rate of decline over the lifespan and opportunities to preserve a healthy skeletal mass. Fragility fractures are preventable for women committed to a healthy lifestyle. 95 Early prevention is key and performing a first DXA scan at age 65 is too late.
Medical prevention strategies to address osteoporosis have traditionally focused on fall prevention, calcium supplementation, dietary interventions, balance concerns, physical environment modifications and weight bearing exercises. 96 In the past 30 years the use of various prescription pharmaceuticals, such as bisphosphonates (alendronate, risedronate, ibandronate or soledronic acid), selective estrogen receptor modulators (raloxifen or tamoxifen), hormone replacement therapy, monoclonal antibodies (Denosumab), calcitonin, or parathyroid hormone are prescribed to try to reduce bone loss and/or reduce the risk of fracture. 97 Present day screening methods and medical remedies are often not instituted until the damage to the skeletal system has already progressed to the point that little can be reversed. Post facto salvage care strategies and treatments have been largely ineffective. The notion of preventing or significantly limiting the progression of osteopenia or osteoporosis must be a priority of our contemporary health care system. Given our current knowledge of this “silent disease” of osteoporosis as a thief of the young, it would seem essential that we engage pediatrics, sports medicine and lifestyle medicine providers while our patients are still youthful, rather than tasking our geriatricians & surgeons with this dilemma of compromised bone integrity when the remedies are few and generally ineffective. Unfortunately, the message of “prevention” has for the most part been overwhelmed by the recommendations to “treat” low bone density (osteopenia) and osteoporosis by pharmaceutical remedies, none of which can reverse the long-term ravages of metabolically disrupted bone loss. 98
Conclusion
We know that a woman reaches her maximum bone density generally after peak growth velocity by age 20. This paper advocates for initiating DXA testing in adolescent females and creating a personal health record: a “Bone & Body Composition Life Chart” that tracks her whole body bone, muscle and adipose metrics, cardiorespiratory fitness, strength indices and other vital physiologic metrics over the lifespan. Dr Robert Gagel, BHOF Chairman in 2021 stated that “efforts to maintain bone mass must begin long before disease onset,” and added that “a lifelong commitment to bone health should be a priority for anyone who wishes to maximize their overall health and quality of life. Our programmatic initiatives and vision for the future reflect these values.” 99 We agree. DXA studies are proven to be safe, quick, precise/reproducible, and inexpensive compared with CT or MRI. The only contraindication is pregnancy.
Senescence may be our destiny, but we can, as Jim Fries counsels, “compress the period of morbidity” and preserve quality of life by our lifestyle choices. This is the unique opportunity of ACLM providers to be advocates for health and wellness. This flips on end the current paradigm of DXA testing late in life, by being champions for proactive wellness assessment throughout life. Physical activity levels, heart health, body composition and overall fitness are essential components of this mission. 100 Our goal is to pursue primary prevention strategies, use secondary resources when needed and avoid tertiary salvage care if possible.
Claire Gill, CEO of BHOF, commented that their organization was committed to a renewed emphasis on prevention and prioritization of bone health at all stages of life. From early childhood through young adulthood, we need to build bone strength and reach what is known as peak bone mass. As we age in particularly for women at menopause, we must focus on maintaining our bone density through good nutrition and exercise to avoid developing osteoporosis.
In summary, our advocacy is to (1) maximize healthy bone deposition from age 0-20, (2) monitor and maintain bone health in women ages 20 to menopause, and (3) minimize the gradual and often “silent” decline of bone mineral density following hormonal change from age 50 over the remaining lifespan to preserve & enhance quality of life. Optimal bone health argues for its intertwined relationship with overall cardiorespiratory fitness, muscular vitality, and generalize body leanness. A Life Chart can guide individualized recommendations or other interventions throughout life to optimize a woman’s bone health and cardiovascular fitness to promote lifelong wellness. 101 Lifestyle medicine providers are uniquely trained to educate and guide our patients in this process.
Footnotes
Author Contributions
RB-conceptual, writing, editing. AN-conceptual, writing, submission. MS-conceptual, writing, communication. DD-conceptual, writing, communication, submission. CG-conceptual, graphics. PA-conceptual, leadership.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.