
Abstract
Background
Resilience—the ability to adapt and recover from chronic stress—is a critical determinant of health, particularly among marginalized populations. Women, people of color, and LGBTQ+ individuals experience disproportionate levels of psychological distress due to systemic discrimination, trauma, and social exclusion.
Objective
To explore how lifestyle medicine, when applied through an equity lens, can serve as a powerful tool to promote resilience and mitigate psychological distress in underserved communities.
Methods
This narrative review applies the 6 pillars of lifestyle medicine: nutrition, physical activity, sleep, stress management, social connection, and avoidance of risky substances, to the lived experiences of marginalized populations. It integrates public health literature, minority stress theory, and insights from culturally responsive clinical practice.
Results
Structural inequities create barriers to wellness for marginalized individuals, including limited access to healthy foods, safe environments for movement, and affirming care. When adapted with cultural humility, lifestyle medicine interventions can improve emotional well-being, foster identity-affirming behaviors, and strengthen resilience.
Conclusion
Equity-centered lifestyle medicine provides a promising, accessible framework to help marginalized populations build resilience and reclaim well-being, offering a preventive strategy to reduce long-term psychological distress.
Keywords
“By honoring patients’ cultural strengths, lived experiences, and structural realities, clinicians can shift from prescribing behavior change to co-creating healing partnerships.”
Introduction
Resilience, the ability to withstand, adapt to, and recover from adversity, is an essential determinant of long-term health. For women, people of color, and LGBTQ+ individuals, resilience is not just a personal trait, but a survival mechanism shaped by persistent exposure to discrimination, chronic stress, and structural barriers to care. Psychological distress, including anxiety, sleep disturbance, and emotional exhaustion, is more common in these communities, not due to individual deficiency, but because of social determinants that undermine health and safety. Supporting resilience among marginalized groups is therefore both a clinical and ethical imperative.
Lifestyle medicine (LM), defined by the American College of Lifestyle Medicine as the use of evidence-based therapeutic approaches to prevent, treat, and reverse chronic disease through lifestyle interventions, offers a powerful yet underutilized path to cultivating resilience. The 6 pillars of lifestyle medicine: nutrition, physical activity, restorative sleep, stress management, social connection, and avoidance of risky substances, are foundational to mental and physical health. However, these pillars are often taught and implemented through a lens that assumes equal access, cultural neutrality, and individual control, assumptions that do not hold in structurally excluded populations.
As a double board-certified physician in primary care and lifestyle medicine, I have witnessed the transformational power of culturally responsive LM interventions in real world practice. When patients are invited to engage in healing strategies that affirm their identities, traditions, and lived experiences, they often feel more seen, more empowered, and more willing to make sustainable changes. This narrative review offers both evidence and practical insights on how to apply lifestyle medicine through an equity lens, with a focus on fostering resilience in women, people of color, and LGBTQ+ communities.
The sections that follow will explore each of the 6 LM pillars, emphasizing their relevance in primary care, the unique barriers faced by marginalized populations, and actionable strategies to improve clinical care. Composite patient narratives and case examples are used to illustrate how equity-centered approaches can build trust, engagement, and emotional strength. By shifting our focus from disease-centered care to resilience-centered healing, clinicians can become more effective partners in helping patients reclaim health, on their own terms.
Nutrition
Evidence-based dietary approaches that are culturally relevant, such as the African Heritage Diet, have been shown to improve cardiometabolic markers and patient engagement in Black communities. 1
The African Heritage Diet is part of the broader collection of Oldways Heritage Diets, a resource that celebrates traditional, culturally grounded, and health promoting eating patterns across diverse populations.
Importantly, many traditional diets around the world are predominantly plant-based, which provides a valuable entry point for clinicians to connect evidence-based nutrition with patients’ cultural foodways.
Access to affordable, culturally relevant food remains a barrier in many marginalized communities. The USDA reports that over 19 million Americans live in low access food areas, which disproportionately affects Black, Latino, and Indigenous populations. These environments, often called food deserts or more accurately food apartheid zones, reflect structural inequities in planning and economic disinvestment. 2
In addition to access challenges, cultural stigmatization of traditional foods contributes to disengagement. Western nutrition guidelines have historically pathologized deeply meaningful foods like plantains, fermented dishes, and root vegetables. Reframing these traditional foods as sources of nourishment and pride is not only clinically sound but also emotionally healing.
A 2021 study by Lee et al. showed that African heritage diets improved weight and blood sugar in Black patients with diabetes. In my practice, when a Caribbean patient felt she had to “give up” rice and peas, we reframed the meal using fiber and portion strategies. Her labs improved, and so did her confidence.
Clinicians are encouraged to screen for food insecurity using validated tools such as the Hunger Vital Sign. This two-question screening tool is brief but effective in identifying patients who may be skipping meals or unable to afford balanced nutrition. When food insecurity is identified, clinicians can refer patients to resources such as SNAP enrollment, food pharmacies, or community supported agriculture (CSA) programs.
In some settings, it may also be appropriate to connect with local cooperatives, mutual aid organizations, or cultural food hubs that offer culturally relevant produce and staples at low cost.
Incorporating nutrition into mental health care is another key opportunity. Growing evidence links dietary patterns with psychological outcomes via the gut–brain axis and microbiome function. Diets rich in fiber, fermented foods, and phytonutrients can support mood regulation and reduce inflammation, providing patients with an additional path to emotional resilience.
In one case, a South Asian woman shared how reconnecting with lentils and turmeric rich stews helped her manage her blood sugar and reduced her feelings of isolation. This outcome was possible not only because of the food itself, but because the meal reminded her of home, culture, and care.
Celebrating cultural foods enhances engagement and builds trust in the care relationship. Affirming ancestral nutrition is not just a dietary intervention, it is an act of dignity and inclusion. Clinicians are encouraged to ask open-ended questions such as, “What foods make you feel connected to your family or your roots?” to invite patients into the conversation in a respectful, strengths-based way.
Stress Management
In my clinical practice, stress is one of the most common and complex challenges patients face. Among marginalized individuals, it is rarely “just” stress. It often reflects the cumulative toll of racism, microaggressions, intergenerational trauma, and unsafe environments. Many patients initially present with physical complaints: headaches, fatigue, gastrointestinal issues that, upon further exploration, are rooted in unrelenting psychological strain.
Addressing Stress in Primary Care is not only Feasible, it is Essential to Supporting Resilience
Mindfulness and self-compassion-based interventions are well supported in the literature and have shown measurable benefits in reducing psychological distress, emotional exhaustion, and symptoms of burnout.3,4
However, traditional stress management tools may feel disconnected or irrelevant to patients whose distress stems from structural oppression.
Burnout in marginalized patients is compounded by chronic minority stress. According to Meyer’s Minority Stress Theory, identity-based stressors, including vigilance and microaggressions, create a chronic burden on mental and physical health. 5
Cultural adaptations to mindfulness and stress reduction increase relevance and impact. In my practice, a Muslim patient combined evening prayer with breathwork. A transgender patient listened to LGBTQ lead meditations. Both showed reduced anxiety and greater resilience.
Clinicians are encouraged to normalize spiritual practices, screen for trauma, and co-create small, feasible stress strategies that respect the patient’s context and time. In doing so, we offer stress recovery, not just stress reduction.
One simple but effective technique I frequently teach is the STOP method: • Stop: Pause what you’re doing • Take a breath: Regulate your nervous system • Observe: Notice thoughts, emotions, and body cues • Proceed: Continue with intention and self-awareness
This method can be practiced discreetly in clinical settings, during conflict, or even in the grocery store. I’ve had patients report using STOP in moments of overwhelm with their children or during tense workplace meetings, helping them avoid reactive behaviors.
Incorporating principles from Acceptance and Commitment Therapy (ACT) can also support psychological flexibility, a key component of resilience. Rather than eliminating discomfort, ACT focuses on aligning behavior with values. One Latina professional shared, “Instead of trying to fight my anxiety, I started asking myself what matters most in this moment.”
Healthcare systems must also acknowledge that for many patients, stress does not come from within, but from racism, poverty, and structural exclusion. Trauma-informed care, validation of lived experience, and culturally tailored stress support are essential elements of any resilience building strategy.
Movement
Physical activity is a cornerstone of preventive care, yet it is often one of the least addressed topics in primary care visits, especially with patients managing multiple social and structural barriers.
When approached with flexibility and cultural humility, movement can become a powerful tool to restore energy, reduce distress, and strengthen mind–body connection.
Movement is a cornerstone of physical and mental well-being, yet marginalized populations face disproportionate barriers to safe, accessible, and culturally affirming forms of physical activity. Transgender patients may avoid gyms due to safety concerns, misgendering, or lack of inclusivity in locker rooms. Communities of color may lack access to green spaces, safe sidewalks, or affordable fitness options. 6
In this context, clinicians can expand how movement is defined and discussed—moving beyond rigid prescriptions to embrace joy, culture, and autonomy. One Latina mother in my practice, for example, reframed dancing with her children and walking to the corner store as valid forms of exercise. Not only did her mood and sleep improve, but she also began to reconnect with her identity through joyful, culturally rooted activity.
By emphasizing movement as self-care, not punishment, we create space for patients to heal their relationship with their bodies. Community-based options such as AfroBeats classes, tai chi in parks, or walking clubs hosted by faith groups improve both engagement and cultural pride.
Clinicians are encouraged to assess for physical barriers, emotional readiness, and cultural values when recommending movement. Focusing on energy, emotional well-being, and daily function, rather than weight, can reduce shame and foster resilience. In doing so, we transform movement from a burden into a celebration of identity and vitality.
To further individualize recommendations, clinicians can ask, “What kinds of movement feel joyful or natural to you?” This question invites autonomy and reduces the stigma of exercise as a task to be endured. For individuals managing chronic pain or disability, functional movement goals such as stretching while seated, range of motion exercises, or water therapy, may be more appropriate than mainstream gym routines.
One queer Black man shared that learning West African drumming and movement improved his posture, decreased his anxiety, and reconnected him with a heritage that had often felt distant. This type of intervention was not just physical activity, it was cultural healing.
Ultimately, movement should be framed not as a means to control the body, but as a path to reclaim and celebrate it. Lifestyle medicine that embraces creativity, autonomy, and trauma-informed strategies helps patients rediscover joy and resilience through the act of moving.
Sleep
Sleep disturbances are one of the most common but under, discussed concerns in primary care, especially among women, patients of color, and LGBTQ+ individuals. Addressing sleep requires more than hygiene checklists, it calls for an understanding of trauma, environment, and the nervous system. In resilience building care, sleep is not just rest, it is recovery.
Sleep is an essential pillar of resilience and physiological recovery, yet sleep inequity is a critical and often overlooked health disparity. Research shows that people of color, particularly Black Americans, consistently report shorter sleep duration and lower sleep quality than their white counterparts, even after adjusting for socioeconomic status. 7 These disparities are attributed not only to neighborhood conditions, such as noise, safety, or overcrowding, but also to racial discrimination and anticipatory stress, which increase sympathetic nervous system arousal and cortisol dysregulation.
For women and LGBTQ+ individuals, the burden of sleep disturbance is compounded by caregiving demands, hormone related changes, and exposure to stigma related trauma. Transgender individuals are more likely to experience insomnia, nightmares, and disrupted sleep due to gender dysphoria, safety concerns, or poor access to affirming sleep environments. 8
In my practice, I often hear patients describe sleep as fragmented and elusive despite their best efforts. A queer patient of color once shared, “It’s not that I can’t sleep. It’s that my body doesn’t think it’s safe to rest.” This insight reflects how safety and dignity are preconditions for restorative sleep, especially in marginalized bodies.
Lifestyle medicine approaches to sleep must therefore extend beyond standard sleep hygiene. While guidelines such as reducing screen time and avoiding caffeine are helpful, they must be contextualized within the patient’s lived environment. For example, a low income mother living in a high crime area may benefit more from guided meditations and earplugs than from a strict 10 p.m. bedtime she cannot maintain.
Clinicians can also invite patients to reclaim cultural and spiritual sleep rituals. These may include herbal teas, prayer routines, body scans, aromatherapy, or ancestral storytelling practices. Framing these as intentional acts of care can improve both engagement and outcomes.
Encouraging patients to create “sleep sanctuaries,” even in shared or modest environments, can improve outcomes. One clinical tool I often recommend is the use of sleep diaries or smartphone sleep tracking apps to help patients identify patterns, triggers, and disruptions. For shift workers, who are disproportionately represented by BIPOC and LGBTQ+ individuals, we discuss how to mimic night conditions during the day (e.g., blackout curtains, eye masks, white noise). In these conversations, the focus is not only on circadian alignment but also on advocating for structural change: paid sick leave, protected rest time, and flexible work accommodations.
In a recent session, a Filipina nurse shared how reclaiming 90 minutes each week for uninterrupted rest helped reduce her irritability and improve her engagement at work. This was not a sleep intervention alone, it was an act of self-respect in a system that rarely offers it. As clinicians, we must understand that rest is not only physiological, it is political, cultural, and deeply tied to healing.
Social Connection
Loneliness and isolation are now recognized as public health threats, with risks equivalent to smoking or obesity. In primary care, patients rarely present with “lack of connection” as their chief complaint, but the emotional and physical consequences often surface through symptoms like fatigue, depression, or worsening chronic disease. For marginalized individuals, disconnection is not simply social, it is systemic.
Social connection is a vital buffer against psychological distress, but marginalized individuals often face exclusion from mainstream social spaces and health systems. Isolation, invisibility, and cultural disconnection increase the risk of emotional exhaustion and reduce access to health promoting relationships. In one national survey, nearly 40% of LGBTQ+ adults reported experiencing loneliness “frequently or always.” 9 For BIPOC communities, racism and lack of representation in healthcare settings further alienate individuals from sources of safety and belonging.
Social prescribing programs, such as referrals to walking groups, arts programs, or peer networks, have shown promise in improving mental health outcomes and care continuity, particularly for those experiencing social isolation. 10
Connection is not merely social, it is survival. The ability to confide in others, to belong in community, and to be witnessed without judgment helps regulate the nervous system and restore a sense of purpose. In lifestyle medicine, fostering social connection should be treated as a therapeutic intervention, not an afterthought.
While I am in the process of developing group offerings, I have seen how identity affirming conversations during one-on-one visits can serve as a powerful bridge to connection. When patients are asked about their cultural values, community ties, and social supports, they often feel a sense of recognition that is rare in clinical settings. One patient told me, “No one’s ever asked me about who I lean on. Just asking that made me think about rebuilding that part of my life.”
The power of peer connection is also evidenced in the literature. Community health programs that incorporate cultural affinity, such as Black barbershop health models, LGBTQ+ support groups, and Indigenous talking circles, have shown improvements in chronic disease management, mental health, and self-efficacy. 11
To build connection, clinicians may consider understanding the cultural and structural forces that drive isolation, and actively support opportunities for belonging. 16
Social prescribing, an emerging model used in several health systems globally, is another promising intervention. This model allows clinicians to refer patients to community-based, non-medical resources such as arts programs, walking clubs, or peer mentorship networks. One pilot program in a federally qualified health center connected isolated Latinx elders to local storytelling groups, resulting in improved mood, appetite, and adherence to medical visits 12
In my own clinic, we have started to incorporate “connection prescriptions” into care plans, simple commitments such as calling a friend weekly, joining a virtual support group, or attending faith-based community meals. Patients often find these goals more engaging than traditional medical advice and report that they feel more seen as whole people, not just diagnoses.
Ultimately, cultivating social connection requires that clinicians examine their own practices and biases. Who gets asked about loneliness? Who is assumed to have support? A trauma-informed, equity-centered lens can help us ask better questions and offer more meaningful pathways toward reconnection and healing.
Avoidance of Risky Substances
Avoiding risky substances—including alcohol, tobacco, and illicit drugs is a core pillar of lifestyle medicine. In primary care, this often means navigating conversations shaped by stigma, trauma, and inequitable systems of punishment. For marginalized populations, substance use is rarely just about choice; it often reflects attempts to self soothe in the face of chronic adversity.
Culturally tailored interventions are essential, particularly in communities where trauma, substance use, and stigma intersect. Lifestyle strategies are encouraged to integrate harm reduction and mental health support with attention to cultural safety. 13
Substance use is a complex and nuanced issue in marginalized communities. For many individuals, substances such as alcohol or recreational drugs are used not for recreation, but as coping mechanisms for chronic stress, trauma, and systemic oppression.
Although some data show similar or lower usage rates in certain marginalized groups, these populations often experience more severe consequences, including criminalization, social isolation, and lack of access to treatment.
For example, Black Americans are more likely to experience punitive consequences from drug use despite similar usage rates to white Americans. 14 LGBTQ+ individuals are nearly twice as likely to report substance misuse compared to heterosexual counterparts. 15
Substance use in this context must be addressed through a trauma-informed, nonjudgmental lens. The goal of lifestyle medicine is not to shame or punish behavior, but to understand its root causes and support healthier, sustainable alternatives. In my own practice, I have seen patients open up about substance use only after they felt safe from moral judgment. One patient, a gay man in recovery from methamphetamine addiction, told me, “Every other doctor just told me to stop. You were the first to ask why I started.”
Understanding the “why” behind substance use allows clinicians to explore emotional regulation, community belonging, and pain, whether emotional or physical, as key factors. Lifestyle medicine provides a pathway toward healing through improved nutrition, stress management, physical activity, and connection. Each of these can help fill the voids often numbed by substance use.
While full abstinence may be the goal for some patients, others may be better served by harm reduction strategies. For example, helping a patient reduce weekly alcohol consumption through meal planning, hydration goals, or social substitution (such as choosing group walks over happy hour) honors their autonomy and promotes success.
One strategy I use in practice is the “HALT” check-in, asking patients to reflect on whether they are Hungry, Angry, Lonely, or Tired before reaching for a substance. This tool, often used in addiction recovery settings, fosters self-awareness and slows impulsive behaviors.
Clinicians must also recognize systemic barriers to addiction care. Marginalized populations often face reduced access to culturally competent rehab programs, implicit bias in pain management, and lack of community-based support systems. Partnering with trusted local recovery networks, particularly those led by and for the communities they serve, can improve referral pathways and patient trust.
In a recent training with resident physicians, we explored how to use motivational interviewing to avoid judgment while uncovering ambivalence around substance use. Role plays using phrases like, “What do you enjoy about it, and what don’t you?” helped clinicians understand that change is more likely when a person feels heard, not corrected.
Ultimately, lifestyle medicine provides more than an alternative to risky substances, it offers a framework for belonging, healing, and reclaiming self-worth. When framed with compassion and equity, it can reach those who have long felt overlooked by traditional addiction care models.
Barriers to Implementation and Solutions for Equity
Despite the promise of lifestyle medicine, its integration into clinical practice, especially in marginalized communities, faces significant systemic, institutional, and interpersonal barriers. These challenges must be named and addressed to ensure equitable implementation and access.
One major barrier is time. Many clinicians cite the lack of time during routine visits to engage in meaningful behavior-change counseling. For patients with complex social needs, a 15-minute visit often prioritizes immediate crises over long-term prevention. This time pressure disproportionately affects practices serving Medicaid or under resourced populations, where provider to patient ratios are high and resources limited.
Reimbursement structures are another key obstacle. Despite growing evidence supporting lifestyle interventions, insurance often does not reimburse for dietary counseling, health coaching, or group visits unless tied to specific diagnoses. This disincentivizes clinicians from prioritizing lifestyle-based care, especially in safety net clinics where financial margins are thin.
Cultural mismatch remains a persistent challenge. Many existing educational materials and behavior-change models reflect majority cultural norms and assumptions about access, literacy, or motivation. Patients from BIPOC, immigrant, LGBTQ+, or low income backgrounds may not see themselves reflected in these interventions, which reduces trust and engagement. 16
Finally, clinician burnout and lack of training present internal barriers. Although this article focuses on patient resilience, it is worth noting that many clinicians are themselves navigating exhaustion, moral injury, and systemic stressors. Supporting their well-being is essential to sustainable, equity-centered care. Lifestyle medicine is not yet a core component of most medical curricula, and providers under chronic stress may struggle to model or implement health-promoting behaviors in their practice. 17
To support more equitable implementation of lifestyle medicine, solutions must occur across multiple levels: 1. Health System and Policy Level • Advocate for expanded reimbursement of lifestyle services, including group visits, nutrition counseling, and community referrals • Integrate lifestyle medicine into value-based care models and quality improvement measures • Fund and scale culturally tailored programs using community-based participatory design 2. Clinical Workflow Level • Redesign workflows to incorporate lifestyle screening tools and SMART goal templates directly into EMR systems • Develop interdisciplinary teams, including health coaches, behavioral health providers, and peer mentors, to extend the reach of lifestyle care • Offer affinity-based group visits (e.g., women of color wellness circles, LGBTQ+ stress recovery groups) to increase engagement and cultural resonance 3. Clinician and Education Level • Embed lifestyle medicine and equity training into medical education, CME, and residency programs • Normalize reflective practice and support clinician resilience through mentorship, mindfulness, and team-based debriefing • Provide scripts, tools, and case studies that reflect diverse lived experiences to build skill in culturally responsive counseling
One practical implementation model includes: • A lifestyle medicine intake that screens for food access, sleep safety, identity-related stress, and social supports • Co-created SMART goals that are culturally relevant (e.g., “Cook one traditional meal this week using a family recipe”) • Monthly lifestyle prescriptions spanning 2-3 pillars • Team-based support from health coaches, social workers, or community health workers • Warm referrals to trusted local resources, including culturally specific wellness programs
For example, I worked with a Black woman experiencing hypertension, insomnia, and emotional exhaustion. After screening, we identified food insecurity, isolation, and night shift work as key drivers. Her care plan included a culturally familiar meal prep routine, guided meditations aligned with her spiritual values, and enrollment in a virtual support group for women of color. Within 3 months, her blood pressure stabilized and her sleep improved.
By addressing barriers and applying multi-level solutions, we can move lifestyle medicine from aspiration to accessible reality, especially for the patients who need it most.
Conclusion
Equity-centered lifestyle medicine offers a transformative opportunity to promote resilience in communities that have long been underserved, overlooked, or pathologized by the healthcare system.
By honoring patients’ cultural strengths, lived experiences, and structural realities, clinicians can shift from prescribing behavior change to co-creating healing partnerships.
This article has explored how each of the 6 pillars: nutrition, physical activity, restorative sleep, stress management, social connection, and avoidance of risky substances, can be adapted to support psychological well-being in women, people of color, and LGBTQ+ individuals.
When implemented with cultural humility, trauma-informed care, and clinical creativity, these pillars can become pathways to empowerment rather than prescriptions for compliance.
To advance this work, future efforts should focus on: • Expanding research on the impact of equity-centered lifestyle medicine interventions in marginalized groups • Training clinicians in culturally responsive communication and trauma-informed behavior change counseling • Designing implementation models that integrate LM into safety-net settings through team-based, reimbursable care
For practicing clinicians, this is a call to action. Start by asking different questions: • “What helps you feel safe enough to rest?” • “What kinds of movement bring you joy?” • “What foods remind you of home, of love?”
These questions are not extra, they are essential. They signal to patients that they are seen not just as bodies, but as whole people shaped by culture, history, and community.
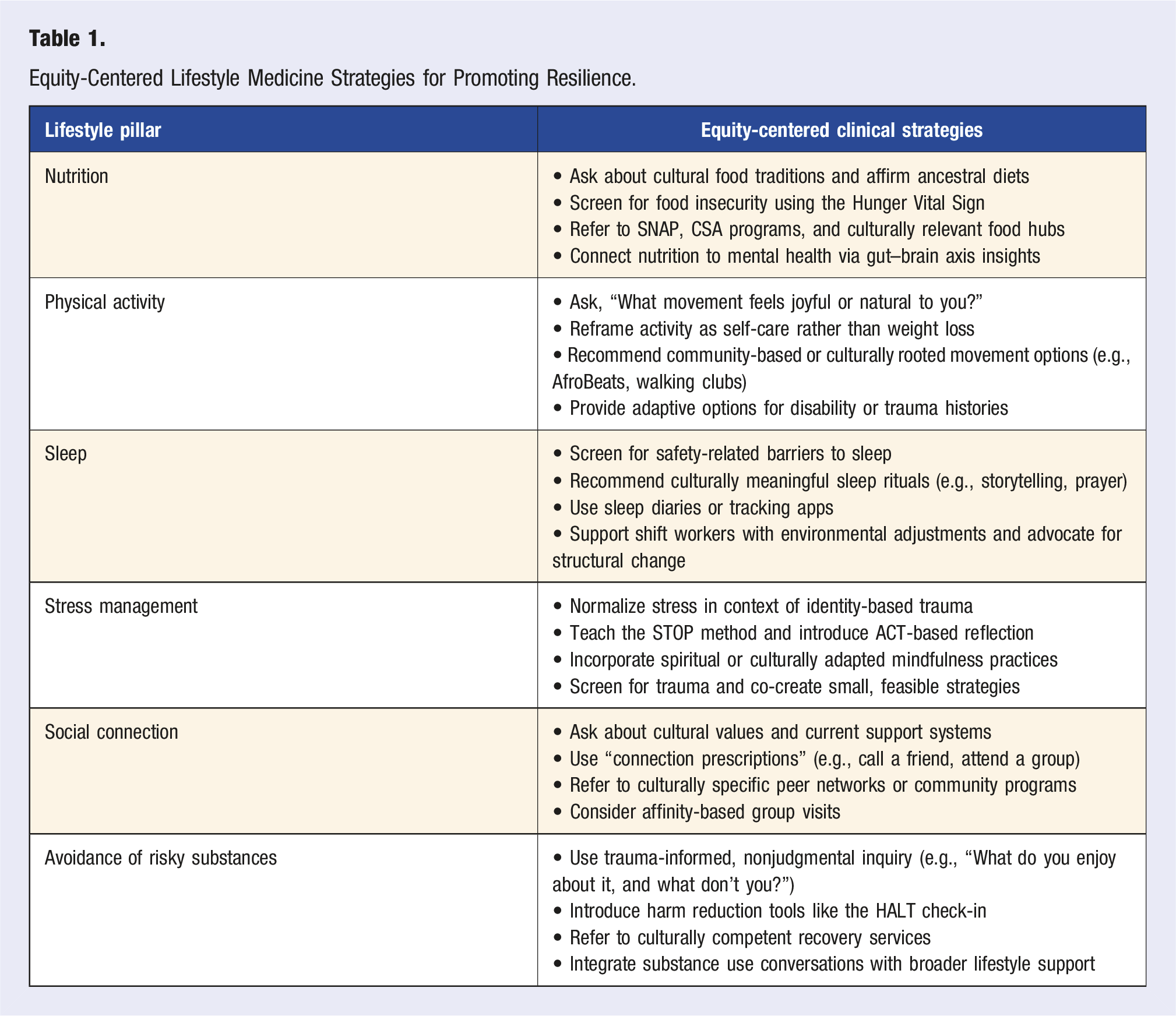
Equity-Centered Lifestyle Medicine Strategies for Promoting Resilience.
This is how we build resilience, together.
Footnotes
Acknowledgments
With appreciation for the diverse communities whose voices and experiences shape the path toward more equitable, healing care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consideration
All patient stories have been de-identified and presented in composite form, without identifiable information. No formal study or data collection was conducted. Therefore, IRB approval was not required.