
Abstract
Keywords
“Our study advances the understanding of lifestyle impact on health, particularly in the context of global health research.”
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death globally. In 2021, the Global Burden of Disease estimated that 8.9 million and 7.2 million people died from ischemic heart disease and stroke, respectively. 1 Both conditions have topped the list of mortality causes in high-income regions and Latin America for the past 30 years.1,2
Major risk factors for CVDs and their associated burden include lifestyle and cardiometabolic (CMB) factors such as low physical activity, a diet low in fruits and vegetables, alcohol consumption, smoking, high blood pressure, high low-density lipoprotein cholesterol, high fasting blood glucose, and a high body mass index (BMI).2-4 CMB risk factors also constitute other CMB diseases such as hypertension, diabetes, dyslipidemia, and obesity, which in turn are likewise affected by lifestyle factors. 4 Growing evidence has shown that sleep health, mental health, and social connections are also crucial for cardiovascular and metabolic health.5-11
The impact of lifestyle on CVDs and CMB diseases has prompted researchers from various research groups and health organizations to develop scales and frameworks based on lifestyle medicine principles. This recognizes lifestyle medicine as an emerging discipline that leverages the central role of lifestyle factors in reducing the prevalence and burden of these conditions and facilitates the implementation of management tools.12-15 The American College of Lifestyle Factors proposed the 6 pillars of lifestyle medicine, which encompass the major lifestyle factors associated with physical and mental health: physical activity, restorative sleep, diet, stress management (mental health), avoidance of risky substances, and social connection. 16
Despite the recognizable positive effects of each healthy lifestyle factor on the prevention of major CVDs and CBM diseases, studies assessing the 6 pillars framework of lifestyle medicine at population level are scarce.17,18 Indeed, no studies have evaluated this framework in the Brazilian population. The National Health Survey (Pesquisa Nacional de Saúde, PNS) was launched in 2013 to establish ongoing epidemiological surveillance to accurately map the prevalence of chronic diseases and associated lifestyle factors in Brazil. 19 This initiative aligns with the Brazilian Ministry of Health’s Strategic Action Plan for Coping with Chronic Diseases 2021-2030. 20 The most recent version, the PNS 2019, was conducted in 2019 and completed in 2020. This edition provides updated prevalence estimates of CVDs, CMB diseases, and other chronic non-communicable diseases (NCDs) in Brazil, along with related lifestyle information factors. 19
Therefore, the PNS 2019 presents a unique opportunity to test hypotheses regarding associations between the six pillars of lifestyle medicine and the prevalence of CVDs/CMB diseases nationwide. Thus, we aimed to assess the prevalence of major CVDs and CMB diseases and their association with a healthy lifestyle score based on the six pillars of lifestyle medicine. Our hypothesis is that CVDs and CMB risk factors would be more prevalent in Brazilian adults with lower healthy lifestyle scores, while higher lifestyle scores would be linked to a lower likelihood of CVDs and CMB risk factors, even after controlling for socioeconomic and geographic disparities.
Methods
This is a subanalysis of the PNS 2019 database, a nationwide, cross-sectional, door-to-door survey of a representative sample of the civilian noninstitutionalized Brazilian population. The Ministry of Health conducted the survey in partnership with the Fundação Oswaldo Cruz (Fiocruz) and Instituto Brasileiro de Geografia e Estatística (IBGE) between August 2019 and March 2020.
The PNS2019 adopted a complex sampling design, 19 based on three-stage cluster sampling with stratification of primary sampling units (PSU) from census tracts or sets of tracts and selection of PSUs for the main sample. Households were selected from the National Register of Addresses for Statistical Purposes, and finally, the definition of the PSU sample size. 19 The survey sampling weights were defined considering the weight of the corresponding PSU. Corrections for non-response and calibration of the estimates were made according to the population totals estimated by the IBGE. 19
The PNS2019 sample consisted of 8015 PSUs, comprising 574 strata. In the sample with individual responses from the dwellers, there were 94,111 household visits and 90,846 participants interviewed (96.5% response rate). In this study, the data were obtained from Brazilian adults aged 18 years and older who answered questions about general sociodemographic information, lifestyle behavior (Module P), and chronic diseases (Module Q).
The National Research Ethics Committee (3.529.376) has reviewed and approved PNS2019. All participants provided written consent before enrollment.
Assessment of Variables
Outcomes: Cardiovascular and Cardiometabolic Diseases
CVDs and CMB disease diagnoses were based on self-reported medical diagnosis, considering the following question for each condition: “Has any doctor ever diagnosed you with ______?”. CVD options were heart diseases (“myocardial infarction,” “heart failure,” “arrhythmia,” “angina,” or “other”) or stroke. CBM disease options were “hypertension,” “diabetes,” and “dyslipidemia.” Obesity was included as a CMB disease and was defined by a body mass index (BMI) ≥ 30 kg/m2, according to the WHO classification. 21 BMI was calculated based on self-reported weight and height.
Exposure to Lifestyle Factors: The Healthy Lifestyle Score
Categories and Scores of the 6 Pillars of Lifestyle Medicine and Their Components.
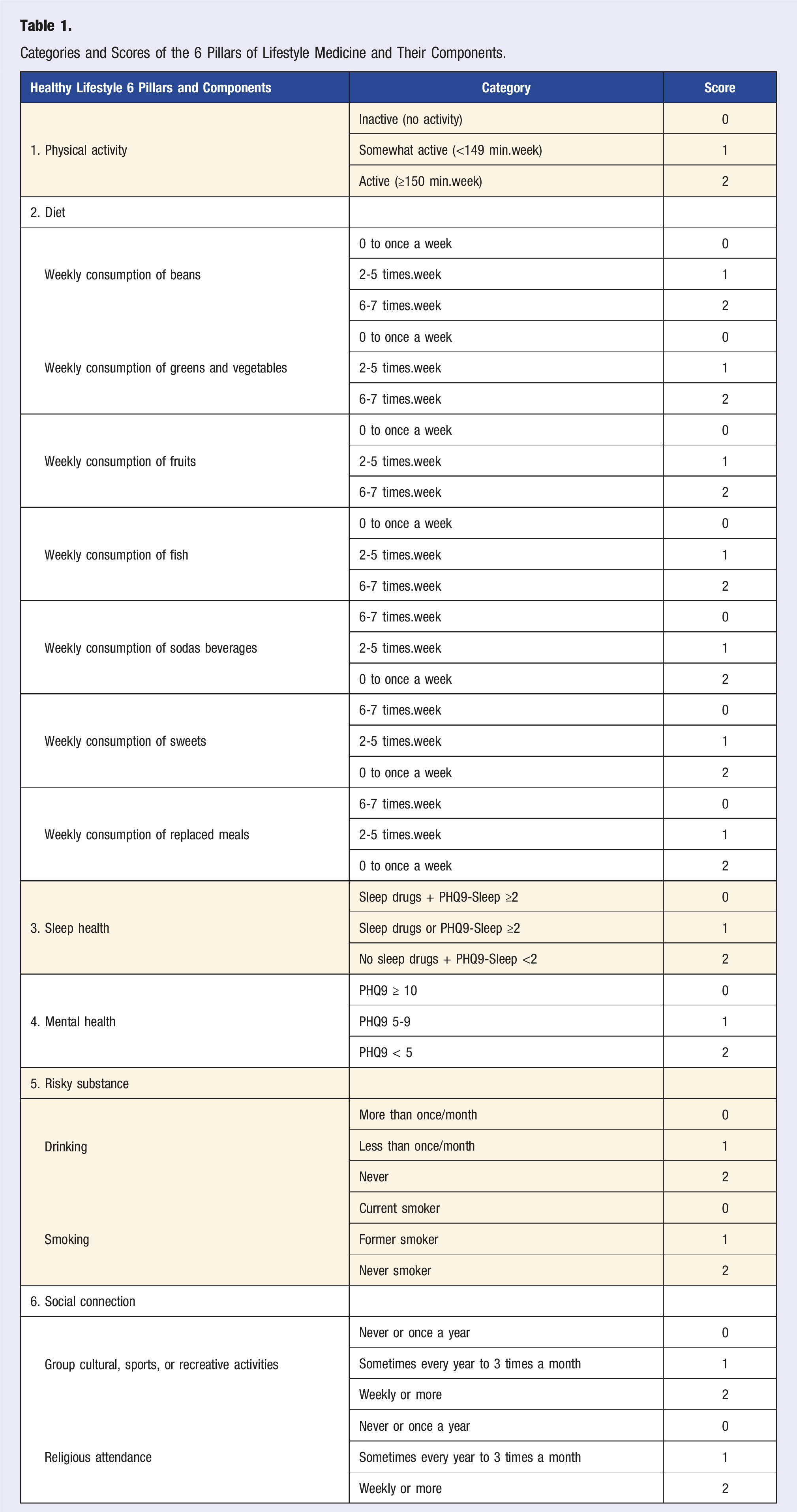
Lifestyle components were scored as 0, 1, or 2 points, corresponding to the poorest, intermediate, or healthiest options, depending on exposure levels. For diet and social connection, which consisted of multiple questions, unweighted mean scores were calculated. Scores for unhealthy food groups were inverted; thus, the values of 0 and 2 points represented the highest and lowest consumption frequencies, respectively (Table 1).
Given the significant impact of alcohol consumption 22 and smoking 23 on mortality and CVD burden, these factors were analyzed separately under the “risky substances” pillar. Consequently, the total healthy lifestyle score included 7 items, ranging from 0 to 14 points as the unweighted sum. Higher scores reflected a healthier lifestyle profile. The details of the assessment of each component and the methodology of the scoring system adopted for each pillar of lifestyle medicine are described in the following subsections.
Assessment of the 6-Pillar Lifestyle Medicine Framework
Physical Activity
Leisure-time physical activity (LTPA) was the domain of interest due to its more consistent associations with reduced CVDs and CMB risk.24-26
Participants provided self-reported data on their LTPA, including moderate-to-vigorous aerobic exercises and muscle-strengthening activities over the past 3 months. They recorded whether they engaged in these activities (yes/no), their typical weekly frequency (0-7 days), the duration (in minutes or hours per day), and the specific activity type (i.e., aerobic or muscle-strengthening activities) from a list of 16 options. The activities were categorized as follows: aerobic activities: walking, treadmill walking, running or jogging, treadmill running, aerobic gymnastics/spinning/step/jumping, water aerobics, swimming, martial arts/combat sports, biking or stationary biking, soccer, basketball, volleyball, tennis, dance classes. Muscle-strengthening activities include weightlifting, localized gymnastics, Pilates, or yoga.
The total weekly minutes of LTPA were calculated and classified according to the World Health Organization’s 2020 guidelines, which recommend at least 150 minutes per week of total moderate-to-vigorous aerobic physical activity, including muscle-strengthening exercises at least twice per week. 27 Participants were defined as “active” if they met at least one of the following criteria: engaging in a minimum of 150 minutes per week of moderate-to-vigorous physical activity or 75 minutes per week of vigorous physical, including muscle-strengthening exercises at least twice per week. Those who reported no physical activity were defined as “inactive.” Participants who engaged in physical activity but did not meet the thresholds for the “active” category were defined as “somewhat active.” 27 The score values of 0, 1, and 2 were attributed to inactive, somewhat active, and active, respectively.
Diet
Dietary patterns were assessed using the Food Frequency Questionnaire (FFQ), which enquires about the frequency of food consumption over the past week (0 to 7 days). For our scoring, we selected the following food groups: (a) beans; (b) raw and cooked vegetables (lettuce, carrots, tomatoes, chayote, collard greens, eggplants, zucchini, etc) ; (c) fruits; (d) fish; (e) sodas; (f) sweets (such as cakes, pies, chocolates, candies, cookies, or sweet biscuits); and (g) meals replaced with sandwiches, hot dogs, snacks, or pizzas. Each food group was assigned a score ranging from 0 to 2. For healthy food groups (a to d), a weekly consumption frequency of 0 to 1 time was scored as 0, 2 to 5 times as 1, and 6 to 7 times as 2. In contrast, for unhealthy food groups (e to g), a weekly intake of 0 to 1 time was scored as 2, 2 to 5 times as 1, and 6 to 7 times as 0. The diet score was calculated as the unweighted average of the scores across all food groups.
Sleep
The categorization of sleep health was based on the questions: “In the past 2 weeks did you take any sleep medicine?” (answer options were yes/no) and item 3 of the Patient Health Questionnaire-9 (PHQ-9), “In the past two weeks, how often have you had sleep problems, such as difficulty falling asleep, waking up frequently during the night, or sleeping more than usual?” The response options and their respective values were “Not at all” (0), “Several days” (1), “More than half the days” (2), or “Almost every day” (3). 28 The score value of 0 was assigned to participants who reported taking sleep medicine and/or experiencing sleep problems “More than half the days” or “Almost every day.” A value of 1 was given to respondents reporting sleep problems on “Several days,” while a value of 2 was attributed to respondents who reported no sleep problems (“Not at all”).
Mental Health
Because PNS 2019 does not have a specific question on stress, the pillar of mental health was operationalized based on the PHQ-9 score, which has been translated and validated for the Brazilian population.28,29 The PHQ-9 assesses the severity of depression through 9 questions regarding symptoms experienced over the past 2 weeks, utilizing a 4-point Likert scale. Depression severity is classified into five levels based on the PHQ-9 scores: minimal or none (0-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20-27). For our healthy lifestyle scoring system, the following PHQ-9 categories and values were assigned: minimal or none (0-4) = 2, mild (5-9) = 1, and scores over 9 = 0.
Risky Substances
Smoking Status
The questions assessed current smoking status: “Do you currently smoke any tobacco products?” or “Did you use to smoke any tobacco products?”. The answer options for both questions were “yes” or “no.” The score value of 0 was assigned to current smokers; the value of 1 was assigned to former smokers; and the value of 2 was assigned to non-smokers.
Alcohol Consumption
We used the question “How often do you usually consume any alcoholic beverage?” to assess drinking habits. The response options were “never,” “less than once/month,” and “once or more/month.” A score value of 0 was assigned to the drinking frequency “once or more/month,” a value of 1 was assigned to “less than once/month,” and a value of 2 was assigned to abstemious participants (“never”).
Social Connections
We selected the following 2 questions to assess social connection: “In the past 12 months, how often have you met with others to engage in sports, recreational, or cultural activities?” and “In the past 12 months, how often have you attended collective activities of your religion or another religion, excluding situations such as weddings, baptisms, or funerals?” For both questions, response options were: “More than once a week,” “Once a week,” “From 2 to 3 times a month,” “A few times a year,” “Once a year,” “Never.” Religious attendance was selected as a component of social connection, based on the high prevalence of religious affiliation in Brazil and its significance as a major social activity with potential impact on health.30-33 The social connection score was calculated as the average of the 2 scores, without weighting questions.
Covariates: Sociodemographic Factors
Sociodemographic variables included the five main geopolitical regions of Brazil (North, Northeast, Central West, Southeast, and South), age, sex assigned at birth (Female, Male), housing location (Urban, or Rural), self-reported skin color (White, Black, Brown, Others—Asian, Indigenous), 34 marital status (Single, Married, Separated/Divorced, or Widower), household income (per capita), categorized into quartiles: Q4 Income (lowest), Q3 Income, Q2 Income, and Q1 Income (highest); educational attainment (No formal/incomplete primary, Complete primary, Complete high school, and Complete college); labor force status (Inside the labor force, Outside the labor force), excluding pension income; and job status (Employed or Unemployed). People inside the labor force were defined as working-aged people employed or unemployed, and outside the labor force. People outside the labor force were defined as working-aged people who were not employed or unemployed.
Statistics
The population estimates were based on the number of strata, the number of selected PSUs in each stratum, and the number of households and residents included in the PSU, along with their respective expansion factors and sample weighting. The data on weights, number of PSUs, and strata were provided in the dictionary of variables file along with the PNS2019 database. In the PNS2019 survey, it was necessary to define the expansion factors or sample weights of the PSUs, of the households and all their residents, and of the selected residents. The weights of the PSUs considered the probability of selection for these units in both the main sample and the research sample.
In the descriptive analyses, we reported the weighted prevalence of CVDs and CMB diseases as a proportion (%) with a 95% confidence interval (CI). Continuous variables were expressed as means with standard deviations (SD). In the hypothesis tests, we utilized weighted Poisson regression models with robust variance to assess the relationship between the quartiles of healthy lifestyle scores and CVDs and CMB diseases. This statistical approach is considered adequate for cross-sectional surveys and treats time at risk as a constant to ensure accurate estimation of prevalence ratios. 35 The results were presented as Prevalence Ratios (PR) and 95% confidence intervals (95% CI). We performed crude and adjusted models, with the latter controlled for the effects of age, sex, skin color, marital status, educational attainment, household income, housing place, region, and labor force status.
To identify potential non-linear relationships between the continuous values of healthy lifestyle scores and CVDs and CMB diseases, we modeled these relationships using restricted cubic splines with four knots positioned at the 5th, 35th, 65th, and 95th percentiles of healthy lifestyle scores, following Harrell’s 36 method. Reference values for healthy lifestyle scores (0 to 14) were set at 9 points, which was the whole sample´s median value. The regression models built for the cubic splines were also adjusted for age, sex, skin color, marital status, educational attainment, household income, housing place, region, and labor force status.
To address the potential underreporting of CVDs and CMB diseases due to the self-reported nature of the PNS 2019 data, we performed a sensitivity analysis of the weighted Poisson regression models. This involved excluding participants who had not consulted a physician in the preceding 2 years. The timing of the most recent medical consultation was determined based on responses to the question: “When did you last consult a doctor?” The available response options were: “within the last year,” “1 to 2 years ago,” “2 to 3 years ago,” “more than 3 years ago,” and “never consulted a doctor.” A total of 9645 participants reported no medical appointments in the past 2 years.
A type I error rate of <0.05 was accepted as statistically significant in all analyses. All analyses were conducted using Stata software (version 17.0, StataCorp LLC). Complex sampling design svy commands with weights for non-response sample corrections and post-stratification adjustments were applied.
Results
Prevalence of CVDs/CMB Diseases
In this study, 88,531 participants provided complete data regarding the variables of interest. The mean (SD) age was 47.1 (17.1) years, and 52.9% were female. Figure 1 illustrates the flowchart of the participants included in this study. Participants’ flow in the study.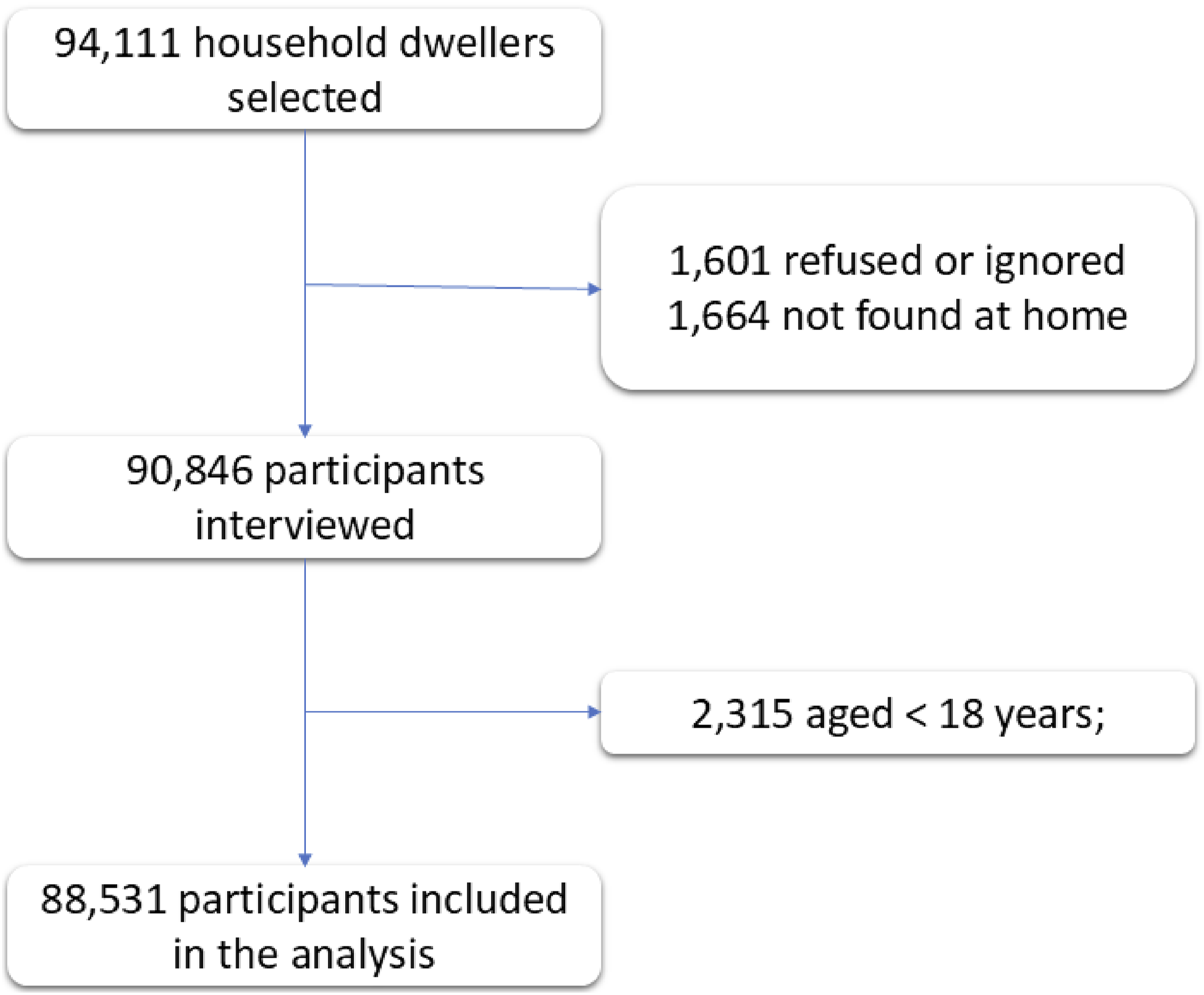
The weighted prevalence (unweighted number) of heart diseases, stroke, hypertension, diabetes, dyslipidemia, and obesity in Brazil was 5.3 % (n = 4711). 1.9 % (n = 1974), 25.9 % (n = 23,819), 8.5 % (7358), 15.7 % (n = 13,396), and 20.1 % (n = 18,026), respectively. The relative standard error for these estimated prevalences was between 1.08% (hypertension) and 4.2% (stroke), indicating the estimates are reliable. The proportion of Brazilian adults that fell below the median healthy lifestyle score (<9 points) was 43.3 % (n = 37,563), while only 13.0% (n = 11,619) reached the highest quartile (≥12 points).
Distribution of Sociodemographic Characteristics and Prevalence of CVDs and CMB Diseases by Quartiles of Healthy Lifestyle Score in 88,531 Brazilian Adults in the National Health Survey 2019
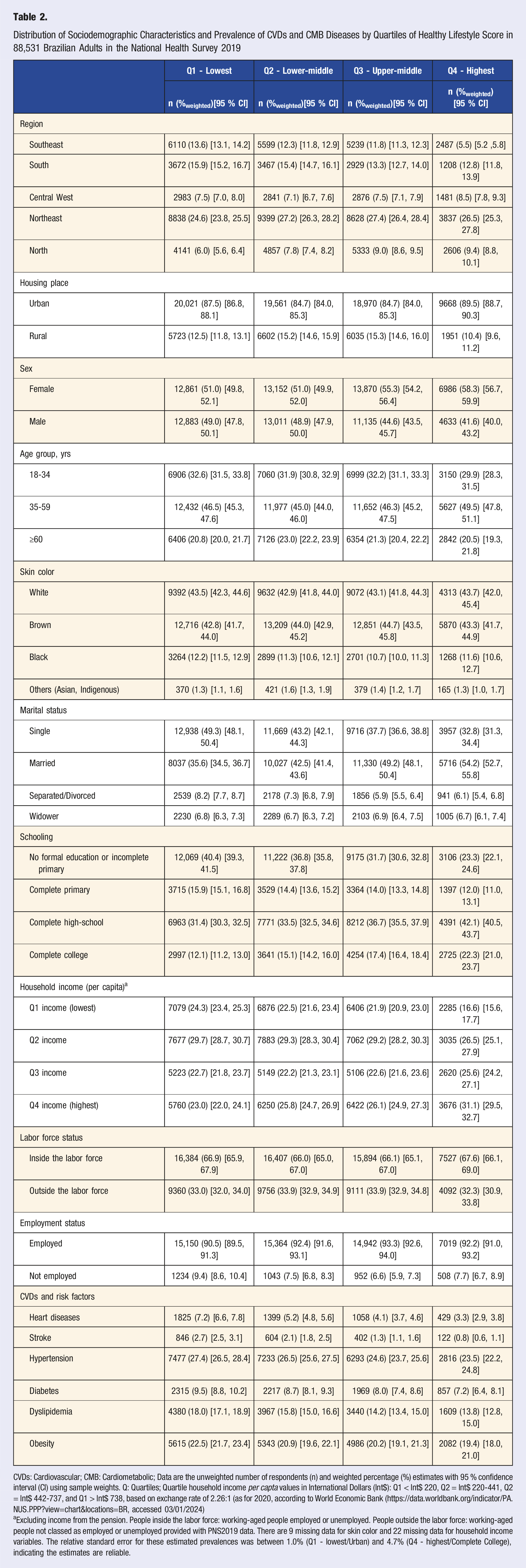
CVDs: Cardiovascular; CMB: Cardiometabolic; Data are the unweighted number of respondents (n) and weighted percentage (%) estimates with 95 % confidence interval (CI) using sample weights. Q: Quartiles; Quartile household income per capta values in International Dollars (Int$): Q1 < Int$ 220, Q2 = Int$ 220-441, Q2 = Int$ 442-737, and Q1 > Int$ 738, based on exchange rate of 2.26:1 (as for 2020, according to World Economic Bank (https://data.worldbank.org/indicator/PA.NUS.PPP?view=chart&locations=BR, accessed 03/01/2024)
aExcluding income from the pension. People inside the labor force: working-aged people employed or unemployed. People outside the labor force: working-aged people not classed as employed or unemployed provided with PNS2019 data. There are 9 missing data for skin color and 22 missing data for household income variables. The relative standard error for these estimated prevalences was between 1.0% (Q1 - lowest/Urban) and 4.7% (Q4 - highest/Complete College), indicating the estimates are reliable.
Associations Between Healthy Lifestyle Score Quartiles and Prevalence of CVDs and CMB Diseases Among 88,531 Brazilian Adults in the National Health Survey 2019
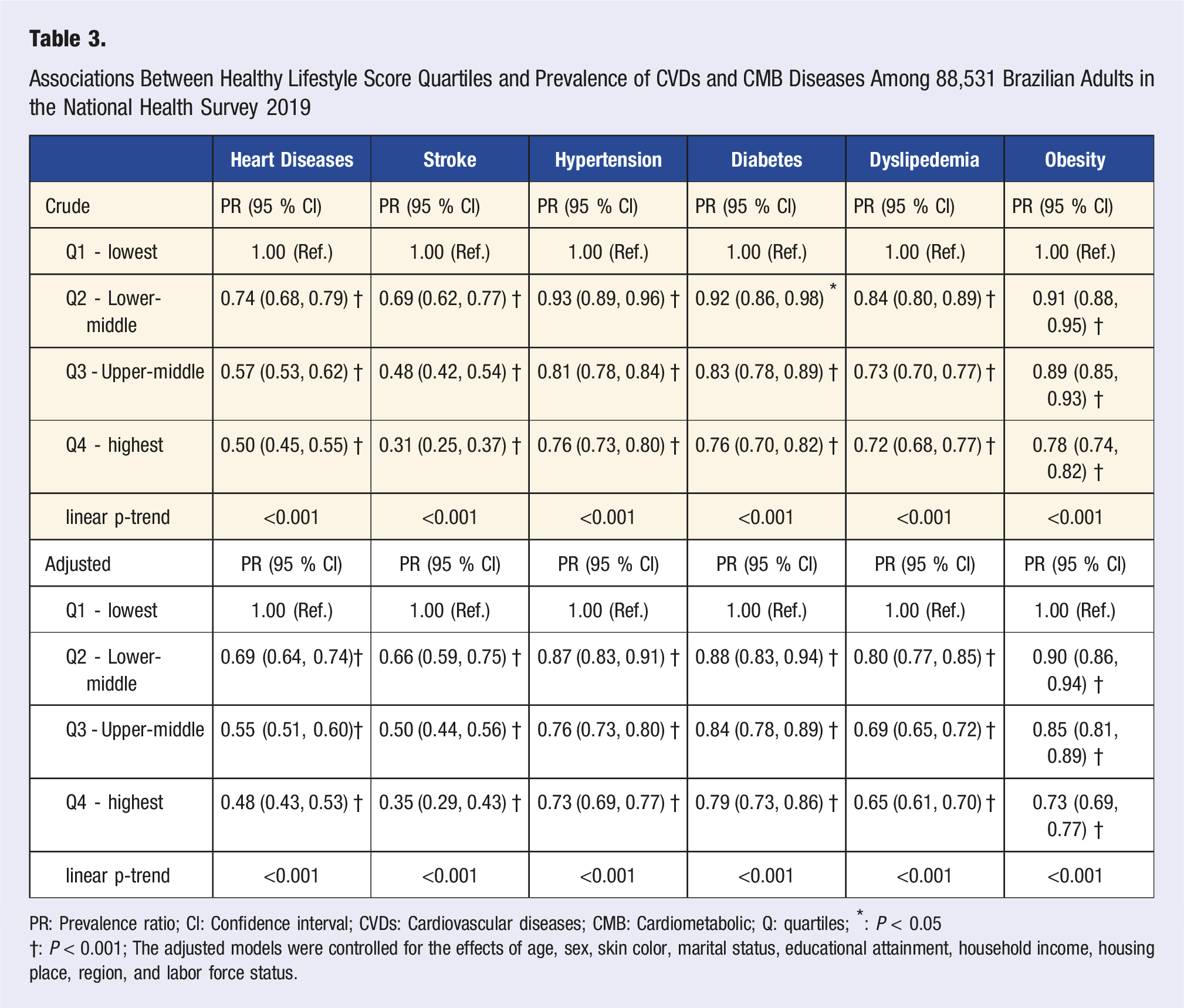
PR: Prevalence ratio; CI: Confidence interval; CVDs: Cardiovascular diseases; CMB: Cardiometabolic; Q: quartiles; *: P < 0.05
†: P < 0.001; The adjusted models were controlled for the effects of age, sex, skin color, marital status, educational attainment, household income, housing place, region, and labor force status.
These associations remained significant after excluding participants who had not had a medical consultation in the past 2 years or more (n = 9645) (Table 4). The plots with restricted cubic splines for the adjusted models revealed linear, inverse relationships between healthy lifestyle score and prevalence of any CVDs/CMB disease (Figure 2). Restricted cubic splines of the associations between healthy lifestyle score and prevalence of CVD and CMB diseases in 88,531 Brazilian adults from the National Health Survey 2019 PR: Prevalence ratio; CI: Confidence interval; CVD: Cardiovascular; CMB: Cardiometabolic; the X-axes were trimmed at the 0.5th to 99.5th percentile of the healthy lifestyle score. The models were controlled for the effects of age, sex, skin color, marital status, educational attainment, household income, housing place, region, and labor force status.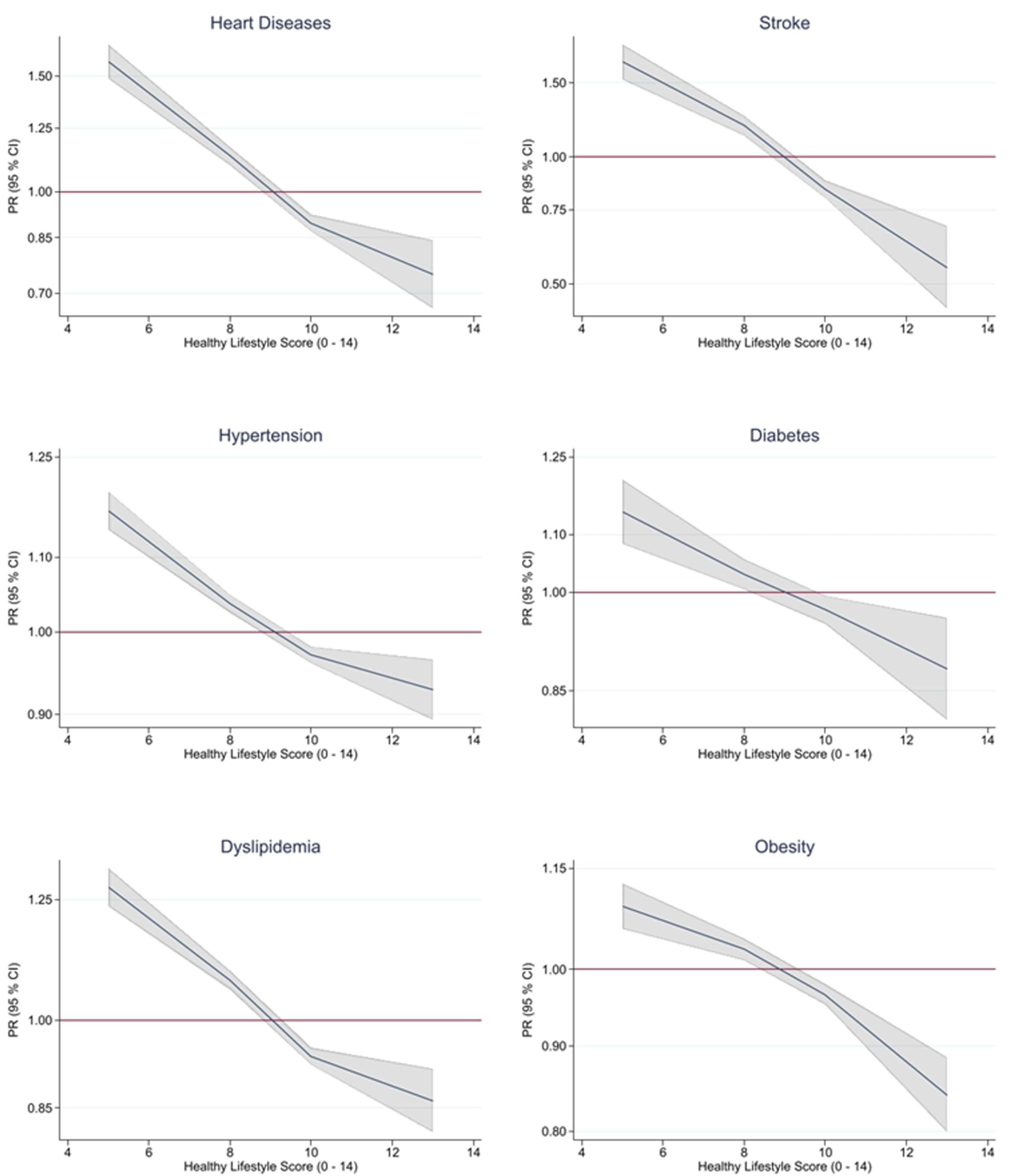
Discussion
In a representative sample from Brazil, our study revealed an inverse relationship between the prevalence of major CVDs and CMB diseases and adherence to a healthy lifestyle, as defined by the six pillars of lifestyle medicine. Individuals with the highest healthy lifestyle scores exhibited a 15% to 62% reduction in the likelihood of being diagnosed with these conditions compared to those with the lowest scores. Notably, the most significant reductions were observed for stroke (62%) and heart diseases (54%).
Sensitivity Analysis of the Associations Between Healthy Lifestyle Score Quartiles and Prevalence of CVDs and CMB Diseases Among 78,886 Brazilian Adults in the National Health Survey 2019 a .
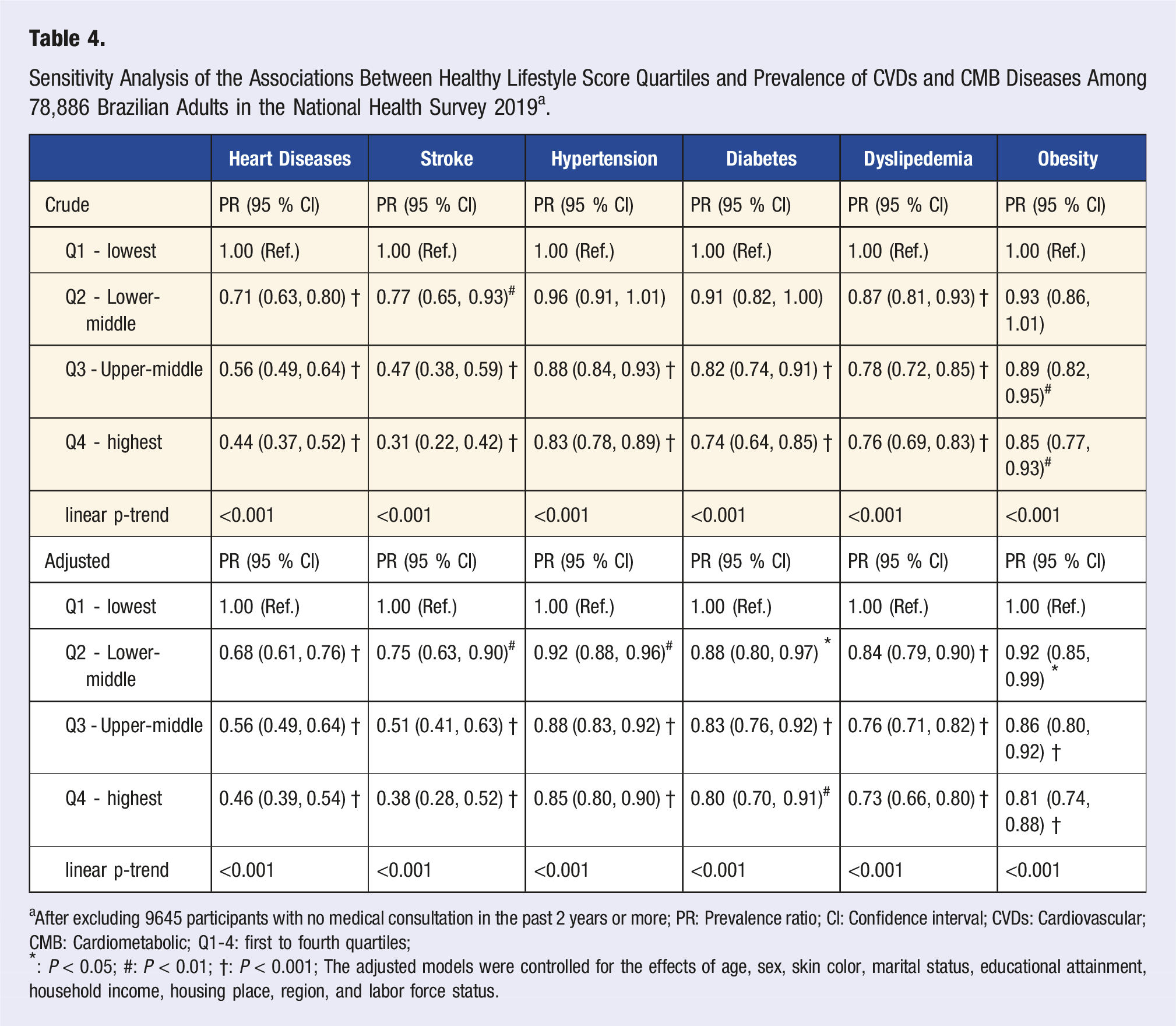
aAfter excluding 9645 participants with no medical consultation in the past 2 years or more; PR: Prevalence ratio; CI: Confidence interval; CVDs: Cardiovascular; CMB: Cardiometabolic; Q1-4: first to fourth quartiles;
*: P < 0.05; #: P < 0.01; †: P < 0.001; The adjusted models were controlled for the effects of age, sex, skin color, marital status, educational attainment, household income, housing place, region, and labor force status.
Albeit the interpretations of these results are limited by the cross-sectional and self-report nature of the PNS 2019 data, our findings align with prospective studies37,39,40 and the GBD risk factor estimates2-4,41 for most lifestyle factors composing the 6-pillar lifestyle medicine framework. Moreover, we observed that only a minority of Brazilian adults exceeded the median for healthy lifestyle scores, which agrees with findings from the United States. 17
Despite unequivocal evidence pointing to the influence of mental health10,11 and social connections7-9,42 on cardiovascular health, these factors are often evaluated separately in cardiovascular research and neglected in other lifestyle scores.6,15,43,44 The linear relationship between the prevalence of CVDs/CMB diseases and lifestyle factors reinforces the clinical and epidemiological utility of integrating these 2 psychosocial factors into the 6-pillar framework to maximize the mitigation of these conditions.
Validating this lifestyle score falls outside the scope of our study, and the healthy lifestyle score presented here does not include weighting to reflect the independent effects or relative importance of each component on specific conditions. Unweighted lifestyle scores, while simple to calculate, may oversimplify complex interactions, reduce precision, fail to account for population differences, and introduce bias. 43 Additionally, complex components of the 6 pillars framework should be considered. For example, the diet pillar is focused on plant-based diet to reduce the risk of NCDs, however, the scores should include the intake of animal sources with negative impact on cardiovascular risk, such as red meat.45,46 Regardless, these limitations, our findings emphasize the importance of implementing multimodal programs to tackle multiple unhealthy lifestyle habits in at-risk populations.
From a public health perspective, the PNS 2019 results revealed the urgent need for a fundamental paradigm shift in public health policies, health care systems, research funding priorities, and resource allocation, all of which should emphasize primary and secondary prevention through lifestyle medicine. 47 Despite achieving some goals of the previous Brazilian Ministry of Health’s Strategic Action Plan for Coping with Chronic Diseases, such as reducing smoking, 48 and increasing LTPA levels, 49 it is evident that there are still multifaceted and broader health challenges that require comprehensive attention. For example, despite a general increase in physical activity among the Brazilian population over the years, only 3.7% of the elderly meet international recommendations for muscle-strengthening activities. 50 This is concerning, as the elderly are at higher risk for CVDs/CMB diseases and often exhibit poorer functional indicators, such as reduced strength. 51
Our study advances the understanding of lifestyle impact on health, particularly in the context of global health research. Most published data in the field of lifestyle medicine and chronic disease epidemiology come from the Global North (e.g., North America, Europe).6,17,37,39,43,52-55 The inclusion of data from Brazil, a large and diverse country in the Global South, helps to address this knowledge gap and provides insights into the health experiences of populations in low- and middle-income countries. Brazil has a diverse population, comprising people of European, African, Asian, and Indigenous descent. 19 This diversity allows researchers to examine the relationships between lifestyle factors and disease prevalence across different ethnic and socioeconomic groups, which can inform more tailored interventions. Furthermore, Brazil’s experiences and challenges in addressing lifestyle-related chronic diseases can be informative for other low- and middle-income countries facing similar health transitions. As such, by using data from Brazil, the study’s findings are more likely to be generalizable to other populations in the Global South, which can help to increase the external validity of the research. Overall, the use of data from Brazil is a significant strength of the study, as it helps to address the imbalance in global health research and provides valuable insights into the relationships between lifestyle factors and disease prevalence in a large and diverse population.
This study presents relevant strengths. The study utilized data from the 2019 Brazilian National Health Survey, which included 88,531 adults, providing a robust sample size for analysis. The study incorporated a healthy lifestyle score based on the six pillars of lifestyle medicine, allowing for a holistic examination of lifestyle factors. Furthermore, the study’s reporting of unweighted counts alongside weighted proportions with 95% confidence intervals demonstrates rigorous handling of complex survey data. Complex samples often exhibit clustered/stratified variability. Pairing weights with robust standard errors ensures both bias correction and appropriate uncertainty quantification. By applying appropriate weighting, the authors ensure representativeness of the target population, while the relative standard errors indicated reliable inference. By incorporating sample strata weights and reporting design-adjusted confidence intervals further reflects proper variance estimation for complex sampling. Together, these methods bolster the validity and generalizability of the findings and guarantee a more accurate representation of the Brazilian population.
The main limitation of this study is its cross-sectional design, which may lead to reverse causality. Data on diagnoses, lifestyle factors, and anthropometrics were self-reported, introducing potential recall and social desirability biases, especially for anthropometric data. The healthy lifestyle score created in this study did not consider the weighted effect of each lifestyle factor on the outcomes. Nevertheless, unweighted scores such as the Life’s Essential 8 factors proposed by the American Heart Association are increasingly utilized and considered valuable in clinical practice. 15 Further analyses, such as categorizing scores based on clinically relevant thresholds for components that have not been studied, such as social connection, may provide more insightful results. Variables like smoking and alcohol intake were categorized broadly, limiting detailed associations with CVDs/CMB disease. Physical activity was focused on the leisure-time domain, excluding potential effects of other domains, such as active commute. Lastly, the survey did not include institutionalized populations, who may present a higher prevalence of CVDs and CMB diseases.
In conclusion, embracing the six pillars of lifestyle medicine is associated with a marked decrease in the prevalence of major CVDs and CMBs. These findings advocate for the promotion of lifestyle medicine as a crucial strategy in combating chronic diseases within the Brazilian population.
Footnotes
Authors’ contributions
Conception and design: ABO, YWW; Acquisition of data: ABO; Analysis and interpretation of data: ABO, JM, YWW, MFPP, and ACG; Drafting the manuscript: ABO, JM, YWW, LKP, LAMSO, MFPP, and ACG; Revising it for intellectual content: ABO, JM, YWW, LKP, LAMSO, MFPP, and ACG; Final approval of the completed manuscript: ABO, JM, YWW, LKP, LAMSO, MFPP, and ACG.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the YWW is a recipient of an NIH/NINDS grant award, K01NS124911. The other authors do not have a specific grant to report in relation to this study.