
Abstract
“Beliefs about lifestyle as a cause of psychological distress were associated with greater pity towards those with mental illnesses.”
Introduction
Mental health stigma is an important factor relevant to mental health outcomes as it has been associated with reduced treatment-seeking behaviors, 1 reduced self-esteem for people with mental illness, 2 and poorer social and occupational functioning.3,4 Of the three main types of mental health stigma—self-stigma, public stigma, and structural stigma1,5—the present study focuses specifically on public stigma, which can be defined as negative and discriminatory attitudes and beliefs that the public holds towards others with mental illness. 6 This study investigated a set of factors which may contribute to public mental health stigma, including perceptions of the degree to which psychological distress is caused by lifestyle factors and one’s own engagement in healthy lifestyle factors. The understudied associations between perceptions of lifestyle as a cause of mental illness and engagement in lifestyle behaviors with stigma, may be important to understand in the application of lifestyle medicine to the prevention and treatment of mental health. Increasing our understanding of these associations may also provide targets for stigma reduction interventions.
Corrigan and colleagues, 6 assert that one of the most important contributing factors to public mental health stigma is a person’s belief about what causes mental illness, also known as the Attribution Model. This model is widely researched and posits that attributions about the cause of mental disorders predict what the public believes about people with mental illnesses, 7 which in turn predicts responses to those with mental illness such as helping behaviors or seeking social distance. 6 Within attribution theory, there are 2 well-researched pathways to public stigma: personal responsibility and dangerousness.8,9 The responsibility pathway postulates that if someone attributes personal responsibility to a negative event that is purportedly caused by mental illness (e.g., “she really just lost her job because she was lazy and chose not show up to work on time”), then that person’s stigma beliefs translate into them being less likely to display helping behaviors (“I’m not helping her pay rent this time!”). Conversely, if someone’s causal beliefs do not include personal responsibility for the situation (“her depression kept her in bed all month so she lost her job”), then they are more likely to display helping behaviors (“I will send her some money until she can get back on her feet”). In contrast to the responsibility pathway, the dangerousness pathway theorizes that when people attribute dangerousness to those with mental illness, their stigma will decrease their helping behaviors and increase their desire for social distance. 10 In support of this, when people are given vignettes that attribute personal responsibility to the cause of mental illness, they report less pity and greater anger; when people are given vignettes that attribute dangerousness, they report greater fear. 11 By looking at a person’s causal beliefs about mental illness, we may be better able to understand and predict the ways that public stigma manifests itself towards those with mental illnesses.
The likelihood of attributing either personal responsibility or dangerousness to someone with mental illness is influenced by a person’s belief that mental illness itself is due to a biological or psychosocial cause.12,13 These different etiologies have varying effects on stigma. For example, the National Alliance on Mental Illness (NAMI) suggested that mental illness is a biological brain disorder, 14 which was intended to decrease the attribution of personal responsibility to mental illness and thereby increase positive helping behaviors towards people suffering from mental illness. 13 Instead, biological attributions of mental health have been linked to an increase in various types of stigma including dangerousness and desire for social distance.12-14 Even though the public’s belief that mental illness is caused by biological factors has greatly increased since the turn of the century, research has shown that this has not been associated with reductions in stigmatizing behaviors.13,15 Pescosolido and colleagues 16 concluded that while mental health stigma beliefs have decreased overall, the biological explanation for the cause of mental illness has not decreased stigmatizing behaviors towards others.
Lifestyle Factors and Mental Health Stigma
Lifestyle factors and health behaviors are being increasingly recognized as important contributors to mental health, well-being, and both the onset and maintenance of various mental disorders. 17 For example, results from a meta-analysis of randomized trials and cohort studies reveal that lifestyle factors including physical activity, diet, sleep, and tobacco use can contribute to both treatment and prevention of various mental health disorders including depression and anxiety. 17 Despite much research supporting healthy lifestyle behaviors as a way to treat mental illness,18,19 less is understood about how perceptions of lifestyle factors as contributors to mental illness may affect stigma. Some research indicates that the degree to which individuals believe lifestyle behaviors cause mental illness varies by disorder type, with recent research suggesting that some disorders, including depression, are more strongly associated with the belief that lifestyle behaviors impact mental illness compared to other types of mental disorders.20,21
Beliefs about the role of lifestyle behaviors as causes of psychological distress may have important links to stigma. 22 This may be because lifestyle behaviors are seen as modifiable factors influenced by self-control, potentially causing individuals to be viewed as responsible for the development and maintenance of their mental illness. 23 Sometimes considered a lifestyle behavior, substance use is also an important factor to consider in etiological beliefs of mental illness. In some studies, substance use was cited as a top reason that individuals developed depression and schizophrenia.21,24 In these studies, increased stigma was associated with decreased helping behaviors and increased social distance. Due to the impact that causal perceptions of mental illness have on different forms of stigma (e.g., increasing or decreasing anger, blame, fear), and the growth of the lifestyle medicine perspective for mental health, it is important to examine how lifestyle attributions are associated with multiple aspects of stigma.
The degree to which perceptions of lifestyle as a contributor to psychological distress impacts stigma may also depend on other personal characteristics. One avenue worth exploring is how an individual’s own personal lifestyles—the degree to which they personally engage in health-related behaviors such as diet, physical activity, alcohol consumption, tobacco use, and sleep—may moderate the relationship between lifestyle attributions of mental illness and stigma. For example, the strength of the relationship between lifestyle attributions and stigma may depend on one’s own ability to maintain a healthy lifestyle, as this might impact perceptions about controllability and responsibility. Given the well-known negative impact of mental health stigma, the current study aims to fill this gap by looking at whether a person’s own lifestyle profile moderates the relationship between the belief that lifestyle factors cause mental illness and their own public stigma. We hypothesized that lifestyle attributions would negatively predict pity and fear but positively predict anger. Additionally, we hypothesized that personal lifestyle profiles would significantly moderate each of those relationships.
Methods
Participants and Procedures
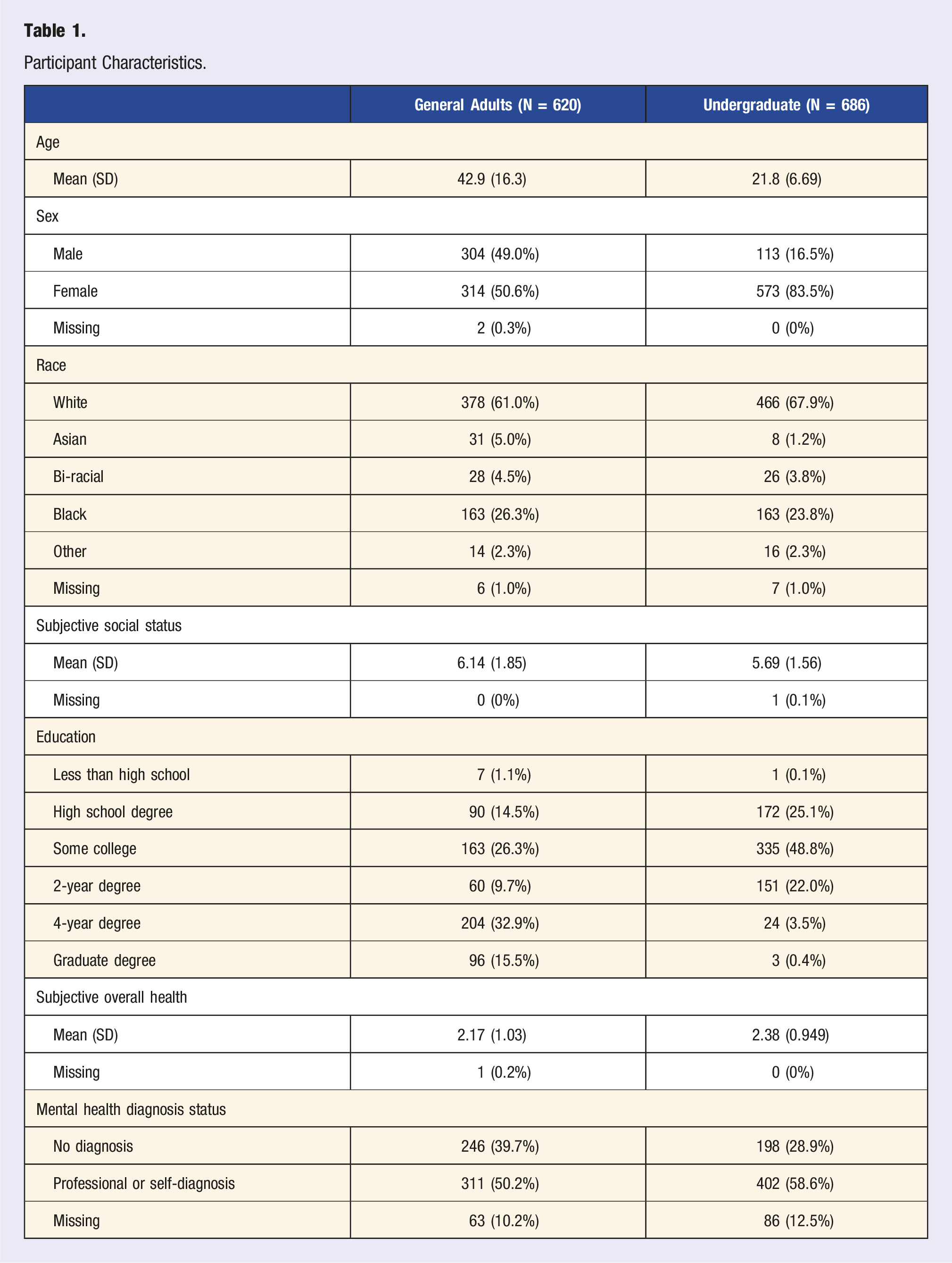
Participant Characteristics.
Measures
Attribution Questionnaire
Stigma was assessed using the Attribution Questionnaire-20. 6 The AQ-20 measures attributions about individuals with serious mental illness and includes 7 subscales: pity, personal responsibility, anger, helping behavior, dangerousness, fear, and avoidance. The participants were asked to rate their agreement from 1 (not at all) to 9 (very much) on statements measuring beliefs about people with mental illness (e.g., “I would feel threatened by a person with mental illness”). This study utilized exploratory and confirmatory factor analyses to reassess the structure of the AQ-20, to identify subscales to measure pity, anger, and fear. The original 3 items for the anger subscale were used (anger items: 1, 4, 8; undergraduate αpooled = .86; general adult αpooled = .85;). Item 6, which was originally designed to be part of the pity subscale, had relatively high loadings on other factors and was removed. Item 17 (“How sorry do you feel for persons with mental illness”), was included as an indicator of pity (pity items: 14, 19, 17; undergraduate αpooled = .85; general adult αpooled = .83;). The items from the original fear subscale loaded onto a common factor with the dangerousness items and an additional relevant item (“I think persons with mental illness pose a risk to other people unless they are hospitalized”; fear items: 2, 3, 5, 9, 10, 11, 16; undergraduate αpooled = .94; general adult αpooled = .96;). Using the AQ-20, previous research has shown associations between attributions of dangerousness and personal responsibility with coercive treatment and less desire to help. 7
Lifestyle Attribution
Causal beliefs about mental illness were assessed using items from the Lifestyle and Substance use subscales of the Mental Illness Attribution Questionnaire 27 along with additional newly designed items following the same format as the MIAQ items. As the original lifestyle factors included in the MIAQ were a blend of behaviors (e.g., “Improper diet”) and environmental factors (e.g., “Unhealthy living conditions”) and this study was more interested in modifiable behaviors, eleven additional items were created. These items were used to thoroughly assess attributions of lifestyle and substance use factors as contributors to emotional distress. Participants were asked to consider and rate a list of “possible causes of emotional distress (e.g., depression & anxiety).” Responses were assessed on a 7-point Likert scale ranging from “This cause is not at all important” to “This cause is very important.” The original items were “Improper diet,” “Lack of physical activity,” “Vitamin deficiency,” “Smoking marijuana,” “Drinking alcohol,” and “Drug use.” New items were “Not getting enough sleep,” “Lack of social engagement,” “Bad sleep habits,” “Lack of sunlight,” “Lack of time spent in nature,” “Lack of religious/spiritual activity,” “Lack of relaxation,” “No engagement in hobbies,” “No volunteering,” “Caffeine consumption,” and “Tobacco use.” Based on exploratory factor analyses (see results below), the items resulted in 2 factors—a lifestyle causal belief factor (undergraduate αpooled = .88; general adult αpooled = .89;) and a substance use causal belief factor (undergraduate αpooled = .87; general adult αpooled = .83;).
Lifestyle and Substance Use Profile Scores
To measure a person’s own lifestyle behaviors, a Lifestyle Profile Score was created based on known research regarding healthy and non-healthy behaviors. Participants’ responses were assigned a value of 1 for each category when their self-report of lifestyle behaviors matched the recommended standard (e.g., 1 point for a score of five or lower on the brief Pittsburg Sleep Quality Index measuring sleep quality) and a zero when they did not meet each of the pre-determined cutoff scores (e.g., consuming less than the daily recommended amount of vegetables). This method of assessing an individual’s lifestyle has been commonly utilized in studies measuring disease risk and associated lifestyle factors.28,29 Self-reported lifestyle behaviors used in this study were physical activity, sleep quality, daily vegetable intake, daily sugar intake, and time spent watching TV. Each variable received a binary score of 1 (healthy) for meeting the relevant cutoff and a zero (not healthy) for not meeting the cutoff. A sum score was created, ranging from 0 to 5 (undergraduate Mpooled = 2.83; SDpooled = 1.05; general adult Mpooled = 2.90; SDpooled = 1.13) and higher scores representing more healthy lifestyles. For physical activity, a score of 14 or greater on the Godin Leisure Time Questionnaire 30 was assigned a 1 (undergraduate n = 467 (70.0%); general adult n = 397 (64.0%). For sleep, participants who scored less than a 5 on the Brief Version of the Pittsburgh Sleep Quality Index31,32 were assigned a 1 (undergraduate n = 320 (46.6%); general adult n = 293 (47.3%). For daily sugar intake, participants were asked to specifically report their sugary drink consumption (instead of other sugar sources such as sugary pastries or snacks) due to past research that has shown that sugary drink consumption was more strongly correlated with overall poorer diet quality among adults and children than other sugar sources. 33 Participants who consumed less than one sugary drink per day were assigned a 1 (undergraduate n = 589 (85.9%); general adult n = 554 (89.4%).33,34 Participants who reported watching less than 2 hours of TV per day were assigned a 1 (undergraduate n = 170 (24.8%); general adult n = 137 (22.1%). 28 Due to an error in survey design, TV time was only collected for half of the participants, but values were imputed during multiple imputation. Five or more servings of fruits and vegetables on a given day was scored a 1 (undergraduate n = 243 (35.4%); general adult n = 243 (39.2%).35,36
A similar score was created for substance use, using self-reported tobacco use, alcohol use, and cannabis use to create a substance use score. Any tobacco use in the past 7 days was assigned a 1 (undergraduate n = 243 (35.4%); general adult n = 243 (39.2%), with any cannabis use in the past 7 days also being assigned a 1 (undergraduate n = 91 (13.3%); general adult n = 123 (19.8%). 28 For alcohol use, male participants who consumed more than 14 drinks and female participants who consumed more than 7 drinks per week were assigned a score of 1 (undergraduate n = 77 (11.2%); general adult n = 93 (15.0%) 37 ; otherwise, they were assigned a score of 0. After adding these scores together, the substance use score could range from 0 to 3 (undergraduates, Mpooled = 0.34; SDpooled = 0.65; general adults, Mpooled = 0.58; SDpooled = 0.84), with higher scores representing greater substance use.
Control Variables
Control variables included age, sex, race, subjective social status, and education as all of these variables were expected to potentially have some impact on stigma and attributions. Also included as potential predictors of stigma and attributions were personal mental illness status (diagnosed or undiagnosed mental illness = 1, no mental illness = 0) and the number of individuals the participant knows with mental illnesses.
Analyses
All data management and analysis were carried out in the R statistical software. 38 Participants who failed two or more attention checks were excluded from the study. To handle missing data, multiple imputation was used in the mice package 39 to create 20 imputed datasets which were used in subsequent analyses. An initial step in the study was to determine which lifestyle attribution items might be used to represent an overall lifestyle attributional style of the participants. Exploratory factor analysis on a random subset of 180 of the undergraduate students, was carried out to examine the initial structure of the original items MIAQ and the added items. Then confirmatory factor analyses in the rest of the undergraduate sample and the general adult sample were carried out to confirm the measurement structure.
Next, structural equation models in the lavaan package 40 were used to look at the association of lifestyle attributions and substance attributions with the 3 aspects of stigma. Next, using semTools 41 the lifestyle profile and substance use profiles were added to the model to examine whether it moderated the relationships between the 2 types of causal beliefs with stigma. Acceptable model fit was determined by Chi-squared values, Comparative Fit Index (CFI ≥.93), Root Mean Square Error of Approximation (RMSEA <.10), and Standardized Root Mean Square Residual (SRMR ≤.10 42 ;). Models were estimated using maximum likelihood estimation with robust standard errors to help account for non-normality in the Likert-style items. Structural equation models were run separately for each sample.
Results
The data from the random subset of undergraduate students (N = 180) was used to examine the initial factor structure of the lifestyle and substance use causal belief items using exploratory factor analysis. The analyses revealed that 3 factors captured much of the variance, although one of the factors only included 2 variables: volunteering and religious participation. As such that factor was excluded from analyses, as was the caffeine use item, which did not load highly on any factor. The remaining 2 factors were comprised of substance use and lifestyle casual belief items respectively. Confirmatory factor analyses using the rest of the undergraduate sample, and the general adult sample revealed reasonable model fit (undergraduate sample: X2 (64) = 156.42, CFI = .96, RMSEA = .05, 95% CI [0.05, 0.07], SRMR = .04; general adult sample: X2 (64) = 201.01, CFI = .95, RMSEA = .06, 95% CI [0.06, 0.08], SRMR = .04).
Undergraduate Sample
The structural equation model for the undergraduate sample resulted in adequate fit (X2 (455) = 880.53, CFI = .94, RMSEA = .04, 95% CI [ 0.04, 0.05], SRMR = .04). Of the hypothesized relations, pity was unexpectedly positively associated with lifestyle attributions (β = 0.18, b = 0.28, 95% CI [0.02, 0.53], P = .03). Women reported less anger stigma (β = −0.12, b = 0.37, 95% CI [-0.70, −0.05], P = .02), while those with a self-reported mental health diagnosis reported less fear stigma (b = −0.42, 95% CI [-0.71, −0.12], P = .01). Of the predictors of the attributions, females reported more causal beliefs related to substance use (β = .12, b = 0.59, 95% CI [0.12, 1.05], P = .01).
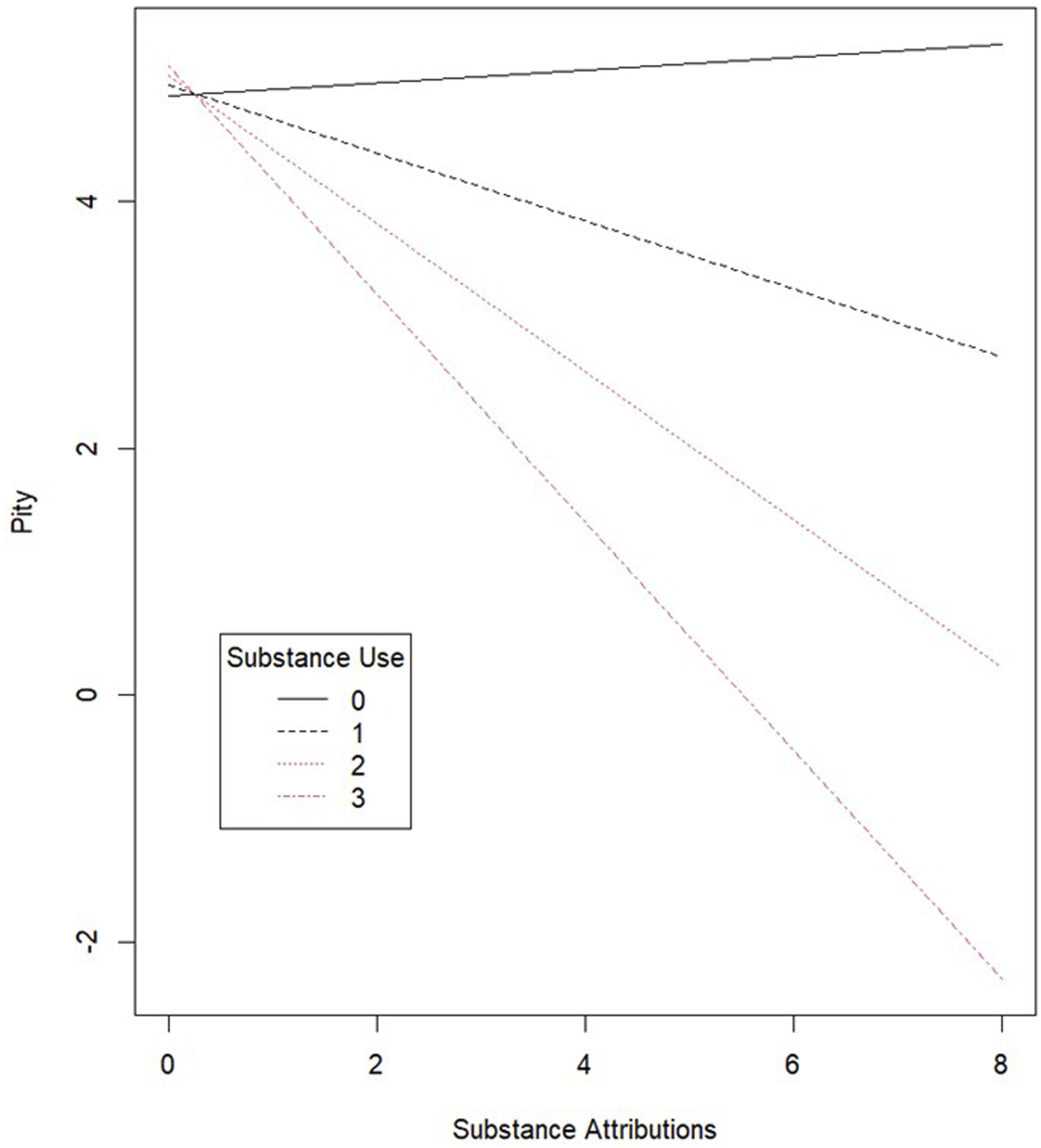
Next, interaction terms were entered into the model resulting in adequate fit (X2 (1027) = 1494.23, CFI = .94, RMSEA = .03, 95% CI [0.03, 0.04], SRMR = .04). There were significant interactions between substance use and substance use causal beliefs as predictors of anger (β = .16, b = 0.19, 95% CI [0.03, 0.35], P = .02), fear (β = .11, b = 0.14, 95% CI [0.004, 0.28], P = .04), and pity (β = −.15, b = -0.28, 95% CI [-0.47, -0.08], P = .01). An examination of the simple slopes indicated that the strength of the relationship between substance use attributions and anger was stronger for those who personally used more substances (b = 0.01, P = .79 for non-substance users, b = 0.20, P = .05 for those who used 1 substance, b = 0.39, P = .03 for those who used 2 substances, and b = 0.58, P = .03 for those who used 3 substances). The relationship between substance attributions and pity was only significantly negative for those who used 2 (b = -0.50, P = .02) or 3 substances (b = -0.78, P = .01). And lastly, the relationship between substance attributions and fear was only significantly negative for those who used 1 (b = 0.18, P = .05), 2 (b = 0.32, P = .04), or 3 substances (b = 0.47, P = .04). In other words, substance use causal beliefs positively predicted anger and fear, while they negatively predicted pity only for the heavier substance users (see Figures 1 and 2; As the figure representing Fear Stigma was very similar to Anger Stigma it was not included here but is available as supplemental material). Substance use causal attributions and anger stigma for the undergraduate participants. Substance use causal attributions and pity stigma for the undergraduate participants.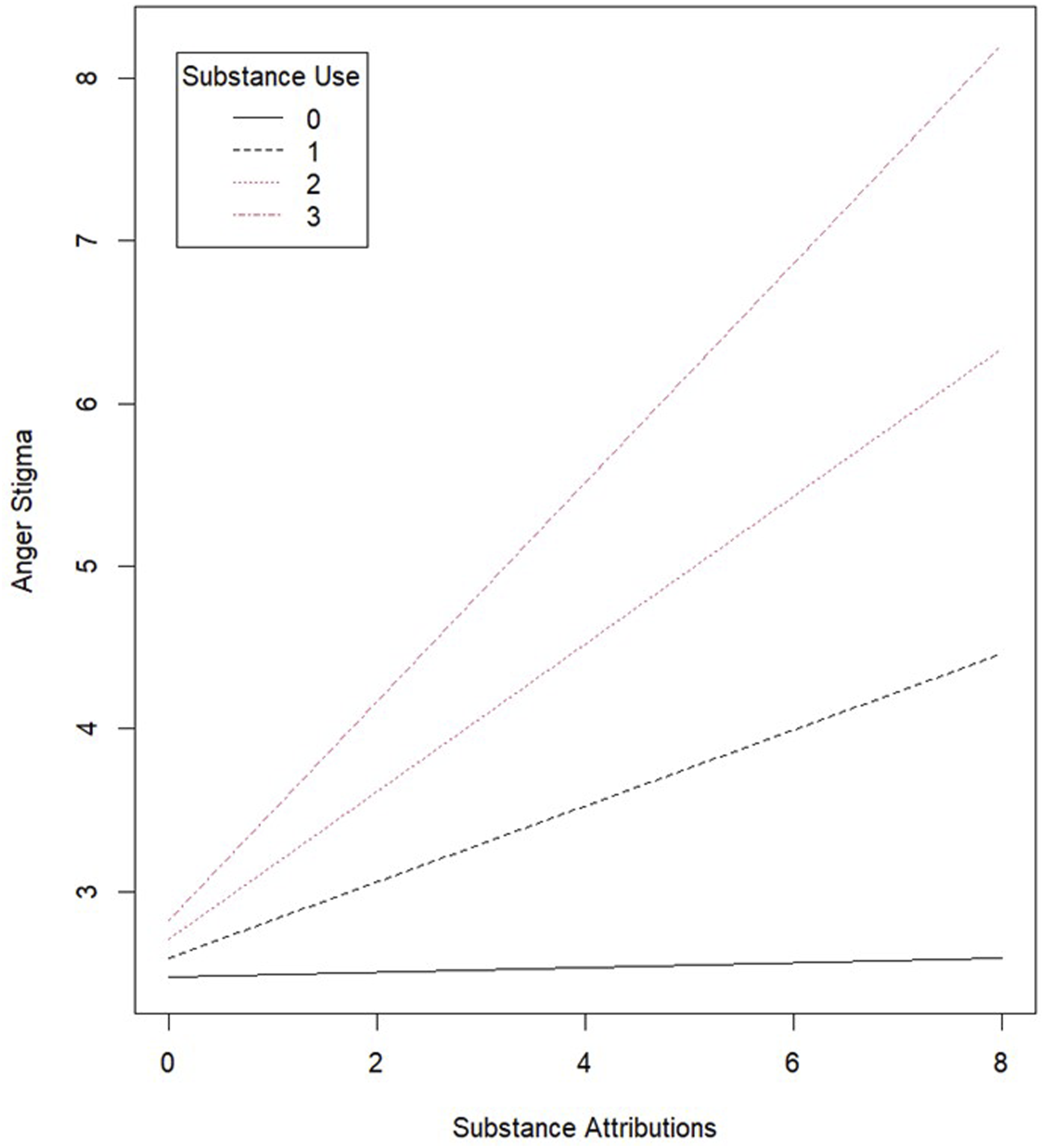
General Adult Sample
The first structural equation model for the general adult sample resulted in adequate fit (X2 (455) = 1100.49, CFI = .93, RMSEA = .05, 95% CI [0.05, 0.06], SRMR = .04). Lifestyle attributions predicted greater anger (β = .19, b = 0.21, 95% CI [0.02, 0.40], P = .03) and fear (β = .17, b = 0.22, 95% CI [0.03, 0.40], P < .02), but also greater pity (β = .45, b = 0.50, 95% CI [0.29, 0.71], P < .001). Substance use attributions predicted reduced pity (β = −.21, b = −0.17, 95% CI [-0.31, −0.03], P = .02). Anger was also negatively associated with number of close relations with mental illness (β = −0.16, b = −0.07, 95% CI [-0.10, −0.04], P < .001), but positively associated with age (β = 0.17, b = 0.02, 95% CI [0.01, 0.03], P = .001). Pity was positively associated with age (β = 0.26, b = 0.02, 95% CI [0.02, 0.03], P < .001). Fear was negatively associated with number of close others with mental illness (β = −0.22, b = −0.10, 95% CI [-0.14, −0.07], P < .001) and one’s own diagnosis (β = −0.10, b = −0.34, 95% CI [-0.65, −0.03], P = .03). Belief in lifestyle attributions was positively associated with the number of close others with mental illnesses (β = 0.14, b = 0.05, 95% CI [0.02, 0.08], P = .001) and was endorsed more by females (β = 0.13, b = 0.36, 95% CI [0.13, 0.59], P = .002). Belief in substance attributions was lower for those with a mental health diagnosis (β = −0.12, b = −0.46, 95% CI [-0.83, −0.09], P = .02) and lower for those with higher subjective social status (β = −0.10, b = −0.11, 95% CI [-0.20, −0.01], P = .03).
The model that included the moderation relationships fit the data adequately (X2 (1027) = 1810.66, CFI = .93, RMSEA = .04, 95% CI [0.04, 0.04], SRMR = .05). However, none of the moderation relationships were significant in the general adult sample.
Discussion
This study attempted to examine the ways that beliefs about the causes of psychological distress, especially viewing psychological distress as the result of poor lifestyle choices, might interact with stigma towards those with mental illnesses. Further, we were interested in whether these associations might vary based on the degree to which one is living a healthy lifestyle. All of the study’s analyses controlled for various potential confounders, such as one’s own self-reported mental health diagnosis status, their familiarity with others with mental illnesses, subjective social status, and education.
One of the most surprising consistent findings across both samples was that beliefs about lifestyle as a cause of psychological distress were associated with greater pity towards those with mental illnesses. This was counter to the hypothesis, which was that lifestyle behaviors would be seen as a modifiable set of behaviors under the control of the person with a mental illness, and thus not worthy of pity. Moderation analyses indicated that this finding did not depend on one’s own level of engagement in healthy lifestyle behaviors. What might explain this relationship is that people are aware that healthy lifestyle behaviors are not easy to maintain, with most U.S. adults not eating enough fruits and vegetables, 43 not getting the recommended amount of daily exercise,44,45 engaging in too much sedentary behavior, 46 and sleeping poorly. 47 Additionally, recent research examining barriers to adherence to healthy lifestyle factors suggested that finances, lack of motivation, lack of time, competing priorities, and lack of motivation were factors that limited their engagement in healthy diet and physical activity. 48 Other barriers that impact engagement in healthy lifestyle behaviors include lack of self-discipline, lack of access to facilities that promote healthy lifestyle engagement, and education about lifestyle behaviors. 49 These extensive barriers to living a healthy lifestyle are likely well-known and understood via first-hand experience by college students and adults alike, resulting in greater empathy and understanding and, in return, greater pity towards those with mental illness as demonstrated in both the adult sample and college student samples.
While lifestyle behavior attributions were associated with greater pity stigma for both samples, the general adult sample showed that lifestyle beliefs were also associated with greater anger and fear stigma. The positive association with anger aligns with our hypothesis, where causal factors that are seen as under one’s control would be associated with a sense of personal responsibility, leading to greater anger stigma at the perceived ability to prevent psychological distress. Relevant cultural norms and social expectations about personal responsibility for health 50 may fuel the anger towards those with psychological distress among individuals who see lifestyle behaviors as the cause. Finally, a misunderstanding of the determining contributors to health 51 may lead to oversimplified judgments about the degree to which someone is able to control their health, in turn, prompting anger stigma towards those with mental illness.
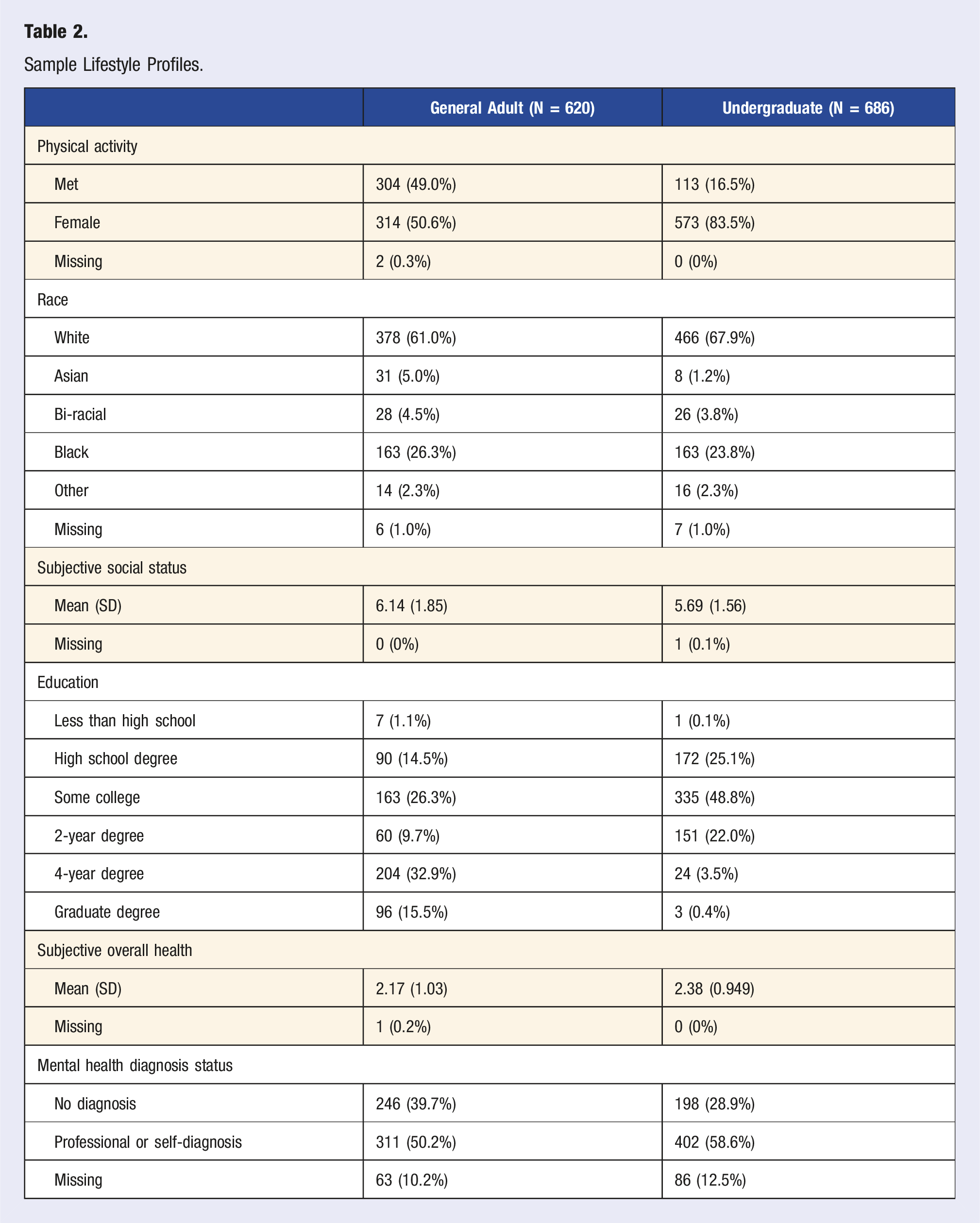
Sample Lifestyle Profiles.
Of the moderation relationships, 2 were significant in the undergraduate sample, both related to substance use; and beliefs that substance use causes mental illness as predictors of both anger and pity. The belief that substance use causes psychological distress was associated with greater anger stigma and reduced pity, but only for those who used two to three substances. This may arise from the numerous types of stigma that substance users face, both from others and themselves. 54 It is possible that negative internal beliefs about substance use contributed to these findings, as substance users have been shown to endorse high rates of self-stigma. 55 Additionally, substance use has been linked to significant levels of perceived public stigma and discrimination.56,57 This pre-existing stigma may work to reinforce an individual’s stigmatizing attitudes towards others, especially when someone uses multiple substances and has internalized various forms of stigma. For higher substance users, messages about the link between substance use and mental illness may be problematic as they may have less pity and greater anger towards those with mental illnesses.
Limitations and Future Directions
The present study included several limitations. First, the data was cross-sectional, and non-representative in scope. While there were 2 unique populations included in the study, the findings are limited in generalizability outside of these samples, especially considering that the undergraduate sample contained many more participants who identified as women (n = 573) than those who identified as men (n = 113). Second, this study employed several new and unique measures for attribution and lifestyle. In particular, the lifestyle score was a novel measure based on evidence-based cutoff scores for various lifestyle behaviors. As with all novel measurements, there is room for improvement. One limitation of the lifestyle behavior measurement is the difference in measurement of various substance use behaviors. While alcohol was measured by quantity and frequency (e.g., how many drinks consumed per week), tobacco and cannabis use were measured on whether a participant used either substance at all in the last 7 days, creating a potential difference in meaning and interpretability. Additionally, this study added items to the Mental Illness Attribution Questionnaire (MIAQ) to better assess for lifestyle factors that contribute to causal beliefs of mental illness, which were particularly relevant to this study’s purpose. These measures, while showing adequate model fit for these samples, need to be further validated. Finally, the proposed models were complex and would benefit from replication with larger samples.
Future research would benefit from continuing this line of questioning through experimental studies looking at the impact of lifestyle medicine messaging on public stigma. It would also be important for future research to look at longitudinal experimental designs with representative samples in order to better understand how perceptions of lifestyle factors and stigma change over time and context. This study, while benefiting from a broad and general discussion of mental illness, would be supported by future research examining beliefs about mental illness and stigma related to specific mental illnesses (i.e., anxiety, depression, schizophrenia, anorexia nervosa). This would help to further address stigma-related interventions and better direct lifestyle medicine applications.
Conclusion
The lifestyle medicine approach to mental health indicates that lifestyle choices carry significant weight in the development, maintenance, and treatment of mental illness. However, it is not totally clear how these messages might be associated with stigma towards those with mental illness, especially because the lifestyle perspective is aligned with the idea that personal choices can impact mental illness, indicating potential high levels of personal responsibility. In 2 samples, this study examined how these beliefs about lifestyle behaviors as causes of psychological distress might impact various aspects of stigma towards those with mental illness. The consistent finding across both samples was that believing that lifestyle behaviors predict psychological distress was associated with greater pity towards those with mental illness. The associations of lifestyle beliefs with pity may be due to the known challenge of maintaining healthy lifestyles. In the general adult sample, lifestyle beliefs were also associated with greater anger and fear, but these findings were not present in the undergraduate sample. There is some evidence that believing substance use causes psychological distress is associated with lower pity and greater anger, but only for those using more substances themselves. To best implement the lifestyle medicine approach to mental health, the field must attend to the way these perspectives might impact stigma with future experimental work and research with representative samples.
Footnotes
Author Contributions
Conceptualization: A.A., L.H., L.O., I.R., J.B.; Data curation: A.A.; Formal Analysis: A.A.; Funding acquisition: A.A.; Investigation: A.A.; Methodology: A.A., L.H.; Project administration: L.H.; Resources: A.A.; Software: A.A.; Supervision: A.A.; Validation: A.A.; Visualization: A.A.; Writing—original draft: L.H., L.O., I.R., J.B.; Writing—review and editing: L.H., A.A., L.O., I.R., J.B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was provided by The University of Southern Mississippi.