
Abstract
This study assesses the prevalence of cardiovascular risk factors, such as diabetes, obesity, high blood pressure, and stress, as related to healthy lifestyle behaviors among healthcare professionals (HCPs), including medical doctors, nurses, pharmacists, laboratory scientists, and radiologists, in medically underserved regions (MURs). Using a cross-sectional study design, an online survey was administered to HCPs in MURs of West Central Illinois. A total of 316 HCPs completed the survey. The study population was predominantly White, female, and aged 55 or older. The findings of this research imply that HCPs in medically underserved regions (MURs) with high cholesterol generally do not engage in physical activity. The study showed a correlation between HCP age, high blood pressure, Type 2 diabetes, and high cholesterol, implying that as HCPs age like every other individual, the likelihood of developing these conditions increases. This study emphasizes the role of time constraints and a lack of motivation in limiting HCPs’ participation in physical activity in rural areas. Additionally, the study suggests that inadequate access to nutritious food and exercise facilities in rural regions contributes to lower rates of healthy eating and physical activity. Findings demonstrate how essential it is for healthcare professionals to remain vigilant about cardiovascular disease risk factors.
Keywords
“The data reveals the presence of some cardiovascular disease risk factors, including high cholesterol, high blood pressure, and Type 2 diabetes, among healthcare professionals in MUR.”
Introduction
The United States has considerable difficulties in realizing adequate healthcare accessibility, with over 6000 regions identified as primary care Health Worker Shortage Areas (pcHPSAs) and thousands of other regions and communities categorized as medically underserved. 1 By 2025, the United States is predicted to be lacking nearly 20 000 medical practitioners, with substantial labor gaps in underserved and rural areas, according to the National Center for Health Workforce Analysis, a division of the federal Health Resources and Services Administration (HRSA). 1 To effectively deliver healthcare services to medically underserved regions (MURs), which are characterized by a shortage of healthcare providers, it is necessary to establish a high level of service delivery efficiency and effectiveness. 2 Increasing clinical capacity can be achieved by identifying professional traits of healthcare workers who are best suited to work in medically underserved communities and subsequent recruiting of such individuals. 2 The lack of healthcare professionals (HCPs) is most likely to affect communities with greater percentages of people from economically disadvantaged backgrounds or members of racial and ethnic minorities. Rural Healthcare Information Hub, 2010). It has been estimated that by 2034, an extra 102 400 to 180 400 physicians will be needed in rural areas. 3
HCPs play a critical role in improving the public’s health and addressing the health concerns of the populace. 4 They do not only provide medical and surgical care but also counsel individuals on leading healthy lives. 4 The global categorization of HCPs includes primary care doctors, specialists, nurses, midwives, specialists in complementary and alternative medicine, paramedics, orthodontists, pharmacists, environmental and occupational health and hygiene consultants, physical therapists, registered dietitians, nutrition experts, audiologists, speech and language therapists, ophthalmologists, and ophthalmic opticians. 5
In the United States healthcare system, healthcare professionals fulfill various roles. Nurses are licensed to utilize their clinical expertise to provide care for patients and their families. Physicians offer primary care services such as routine examinations, but may also specialize in a particular area, such as dermatology, pediatrics, or urology. Surgeons are specialized doctors who assess and treat conditions that may necessitate surgery or are qualified to make physical alterations to the human body. Radiographers are licensed to perform medical examinations using X-rays to produce medical images of specific body parts for diagnosis or screening. Dietitians are healthcare experts in nutrition and the human diet. Physical therapists are licensed healthcare professionals who aid in improving physical movements and functionality of the body.7,8 Laboratory scientists conduct scientific testing on samples and relay the results to physicians. 8
According to Mohanty et al 5 HCPs engage in activities intended to improve the health of patients. Their responsibilities include diagnosis, treatment, prevention, and management of disease, injuries, and other health conditions, according to their patients’ needs. To expand the use of research-based practices, HCPs also engage in research and develop or enhance ideas, concepts, and practical approaches. Their duties also include the supervision of other HCPs. The scholarly literature indicates an abundance of research on the evaluation of patient care and well-being; however, the evaluation of the care and well-being of HCPs has received less attention.
The health of HCPs is not well understood. 6 Medical doctors are less likely than other HCPs to take care of their physical and mental health, even though they experience higher levels of despair, stress, exhaustion, and substance abuse. 6 HCPs often face difficulties in accessing medical care for their health concerns, as they may feel they are letting down their patients or colleagues or the stigma of diagnosis and potential negative consequences on their careers. 6 Obiebi et al 7 stated that despite having lower rates of diseases and deaths than the general population, healthcare professionals (HCPs) are susceptible to illnesses that can potentially compromise the health of their patients. 8 Their circumstances might be made worse by a perception of safety that causes them to misjudge their vulnerability. The number of patients being cared for by fewer healthcare professionals (HCPs) has resulted in an increased workload and demand on HCPs, which in turn increases the likelihood of patient mortality. 9
West Central Illinois is known for its array of small towns and mid-sized cities, as well as its prominent agriculture and manufacturing sectors. According to the Illinois Department of Public Health IQuery, cardiovascular disease stands as the leading cause of death in all counties in West Central Illinois as well as in the United States. The health behaviors and related cardiovascular well-being of healthcare professionals can significantly influence the quality of care they deliver, and consequently, impact health outcomes. In medically underserved areas, such as West Central Illinois, healthcare professionals often grapple with burnout due to extended work hours stemming from workforce shortages. 10 In essence, enhancing the cardiovascular health of these populations would undoubtedly yield positive effects on the communities they serve.
Healthcare professionals are constantly under pressure to meet healthcare expectations and provide patient care. This has resulted in increased stress, depression, and anxiety, leading to extended burnout. Consequently, their overall health and well-being are compromised, which in turn affects their work output and the care they provide to patients in the long term. 11
Prevalence of Cardiovascular Disease Among Healthcare Professionals
HCPs are concerned about other people’s health, but infrequently take care of themselves despite the lifetime risk of cardiovascular disease exceeding 60%. 12 Stress-related disorders are very common among HCPs. Their knowledge of harmful health behaviors may not be mirrored in their state of health. 12 This high CVD death rate is linked to psychosocial variables, alcohol misuse, poor food choices, hypertension, inactivity, obesity, and hyperlipidemia. A research study carried out in the United States involving healthcare workers revealed that 18% of them had hypertension, 6.1% were current smokers, and 7.1% had diabetes. 13 A study conducted in Taiwan by Lin and Li (2009) found that medical technicians such as laboratory technicians, radiology technicians, emergency medical technicians, and pharmacy technicians had a significantly higher prevalence of hypertension than non-medical workers. According to this study, the presence of CVD risk factors was higher among female HCPs who were overweight or obese compared to male HCPs in the same BMI ranges. 14 Younger women who were overweight were shown to have significantly higher numbers of CVD risk factors.
The increasing tendency among healthcare professionals to disregard their health has brought to light the necessity of placing a greater emphasis on personal well-being within the medical profession. 5 As healthcare professionals strive to remain informed about the latest research and advancements, the burden of maintaining this knowledge can lead to significant levels of stress and burnout. Additionally, their workloads have increased substantially, which further compounds these feelings. Furthermore, there is often a lack of balance between their professional and personal lives. 5
Purpose of the Study
The goal of this study was to determine the prevalence of cardiovascular risk factors, such as diabetes, obesity, high blood pressure, stress, and attitudes about and barriers against healthy lifestyle choices, among HCPs in medically underserved regions in West Central Illinois. This study also investigated the impact of workplace stress on lifestyle decisions, such as dietary patterns, physical activity, and medical conditions. According to the Illinois Department of Commerce and Economy Opportunity, 15 Illinois is broadly divided into three major regions. These regions are the Northern, Central, and Southern regions. Central Illinois is further divided into East and West. West Central Illinois, the focus of this study, is largely characterized by small towns and mid-sized cities. Illinois Department of Commerce and Economy Opportunity 15 further stated that counties included in the West Central region of Illinois are Brown, Henderson, Knox, Schuyler, McDonough, Pike, Hancock, Adams, and Warren. This region has an approximate population of 213 370 and a workforce of 95 000. These counties listed are classified by the Health Resources & Services Administration as medically underserved regions. 16
Methods
Research Design
This study utilized a questionnaire adapted from research conducted in Saudi Arabia, 12 which was administered with the authors’ prior consent and modified to align with the objectives of this present study. The modified questionnaire can be found in Supplemental Materials. The survey collected demographic information and respondent answers to multiple-choice questions, as well as items using a 5-point Likert scale. The survey was composed of five sections. Section A focused on respondent demographics, including age, gender, job role, and body mass index (BMI). The clinical category included doctors, pharmacists, nurses, radiologists’ students, and other clinical employees. The Centers for Disease Control and Prevention (CDC) defines underweight as having a BMI of less than 18.5 kg/m2. A BMI of 18.5 kg/m2 to 24.9 kg/m2 is within the healthy weight range, a BMI of 25.0 kg/m2 to 29.9 kg/m2 is overweight, and a BMI of 30.0 kg/m2 or higher is obese. Section B asked about health conditions, including check-ups, smoking, diabetes, hypertension, and high cholesterol. Section C included questions about eating habits and leisure activities. Section D pertained to physical activity related to work. Section E included general questions about wellness associated with work.
Sample and Data Collection
A cross-sectional study was carried out in West Central Illinois, utilizing a self-administered online questionnaire via Google Forms to facilitate data collection and completion. The sample size was calculated using the Roasoft sample size calculator with a confidence level of 95% and an error margin of 5%. The Institutional Review Board (IRB) at two of the authors’ universities approved the study before the data collection began. The study was conducted in hospitals and clinics, which only included clinical hospital employees. Written informed consent was obtained from all study HCPs. All employees meeting the inclusion criteria were allowed to participate by being sent an email. Reminders were sent three times during the data collection period. Responses were collected until the end of the 8-week time frame for evaluation.
Data Analysis
To guarantee the highest level of participant confidentiality, the datasets were not inclusive of any identifiable information. Multiple-choice questions and Likert scale items were used to collect data, allowing for a ranking of responses regarding how the HCPs see their work and the challenges of leading a healthy lifestyle. IBM SPSS version 28 was used to analyze descriptive data. Python 3.0 “Jupyter Notebooks” was used to create the correlation table “heat map.” The heat map visually demonstrates the intensity of the correlation between variables. Means and frequency were used for the descriptive data, whereas percentages and proportions were used to describe categorical data. Comparisons were done using a chi-square test and an independent t-test for statistical inference.
Results
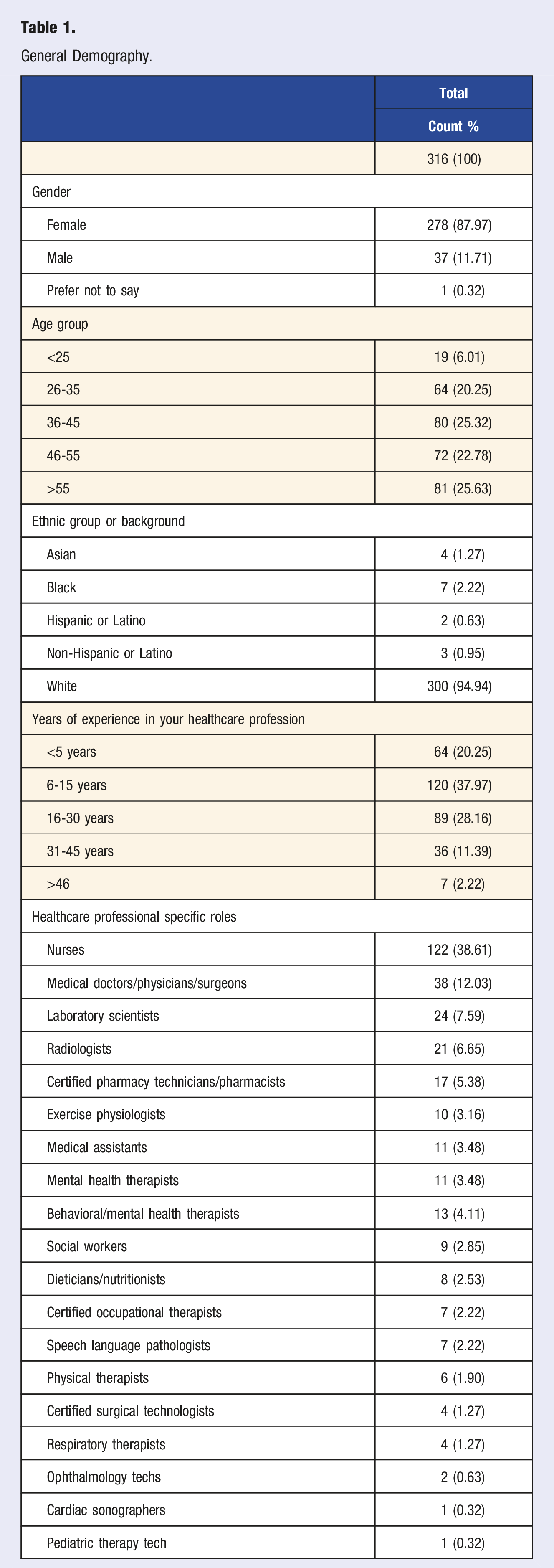
General Demography.
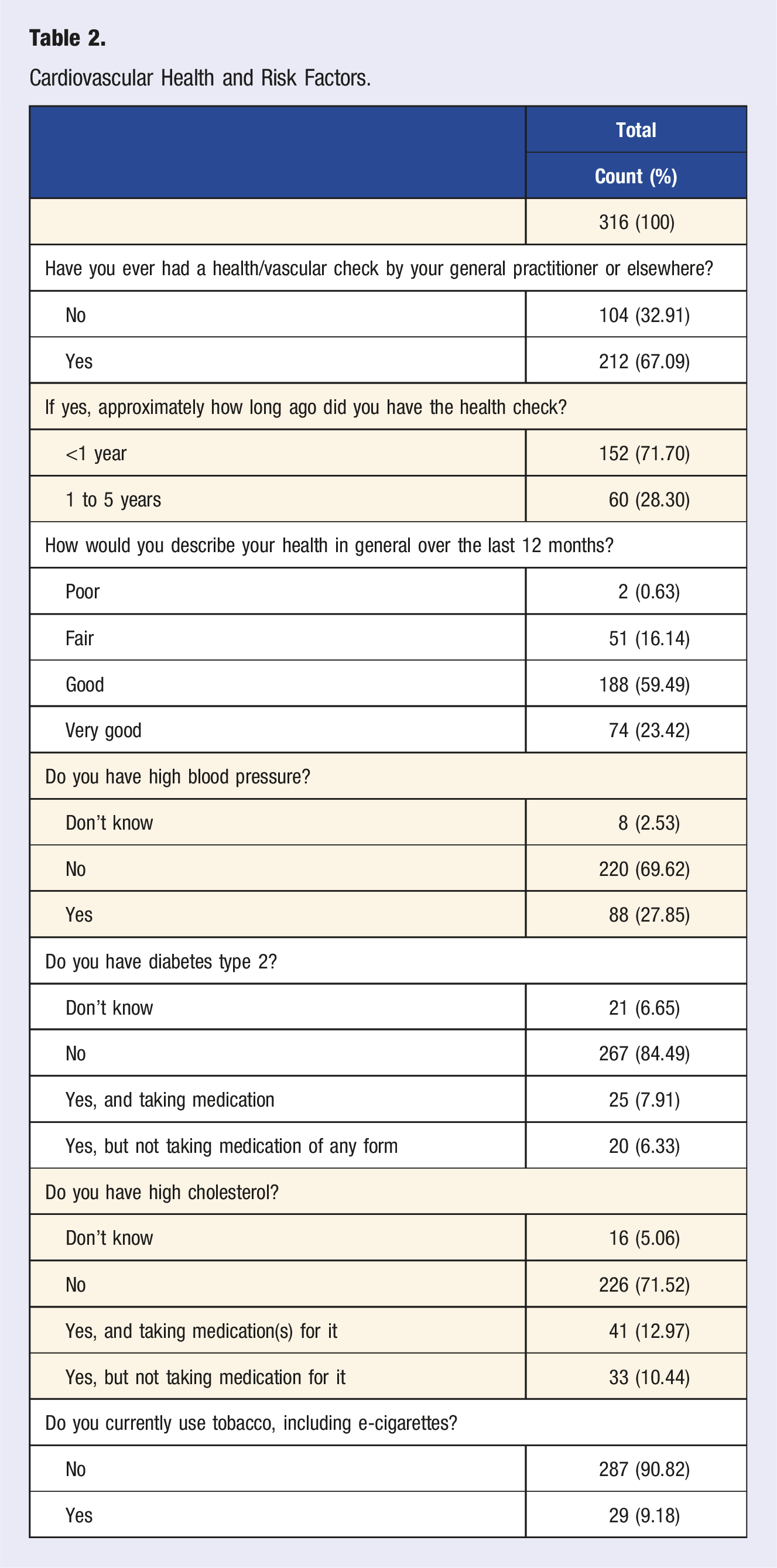
Cardiovascular Health and Risk Factors.
Regarding body weight, all healthcare professionals (HCPs) had average weights ranging between 100 and 199 pounds, with a mean weight of 165.5 pounds and a mean height of 5′7″. Consequently, the mean body mass index (BMI) was 27. Of the sample, 1.9% (6 people) of the sample were classified as underweight, 32.1% (101 people) as having a healthy weight, 42.1% (130 people) as overweight, and 25% (79 people) as obese. The mean of the BMI of the sample was approximately 27 kg/m2 and the median 28 kg/m2, with a range of 14.94 to 67.34 kg/m2.
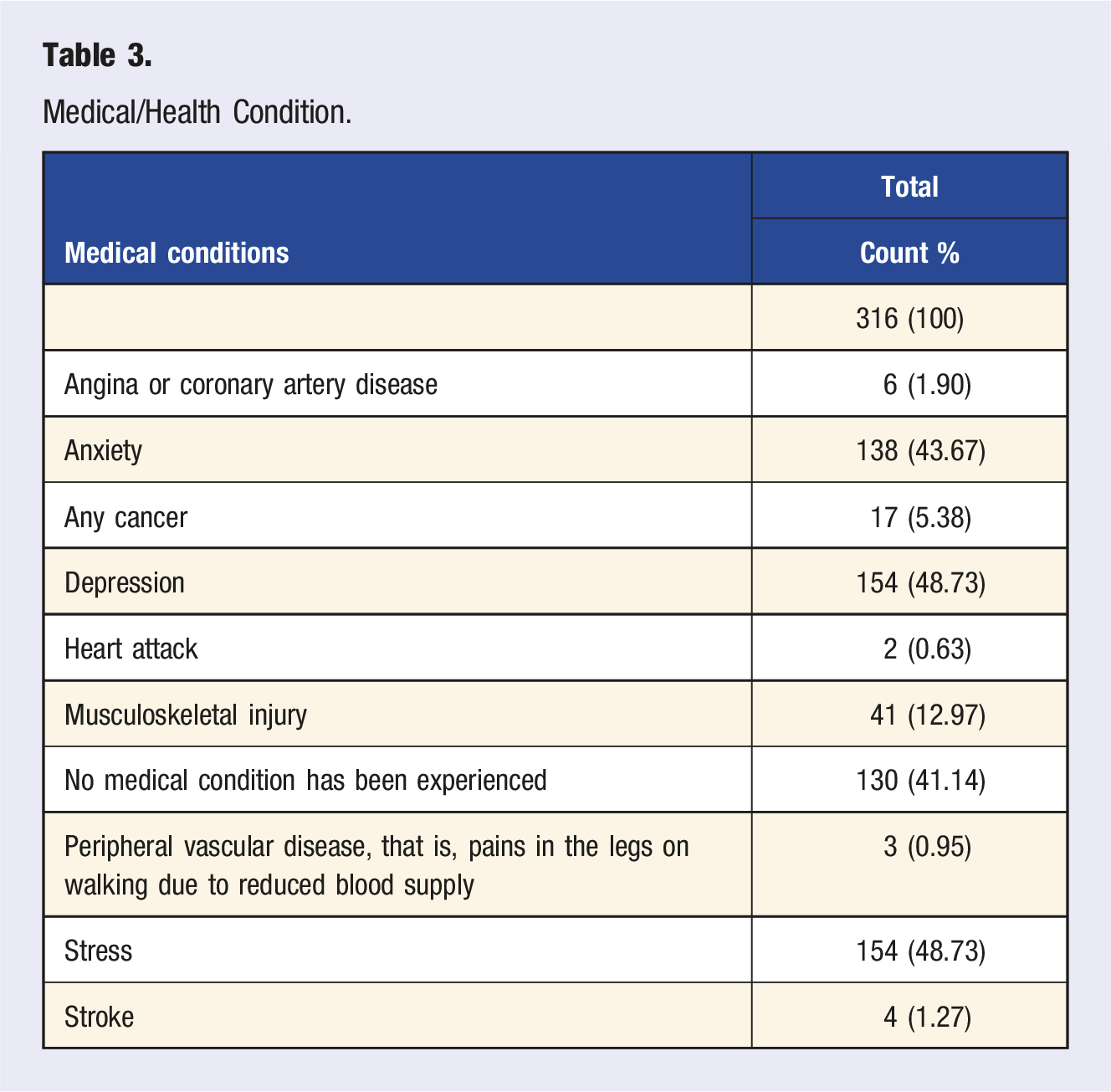
Medical/Health Condition.
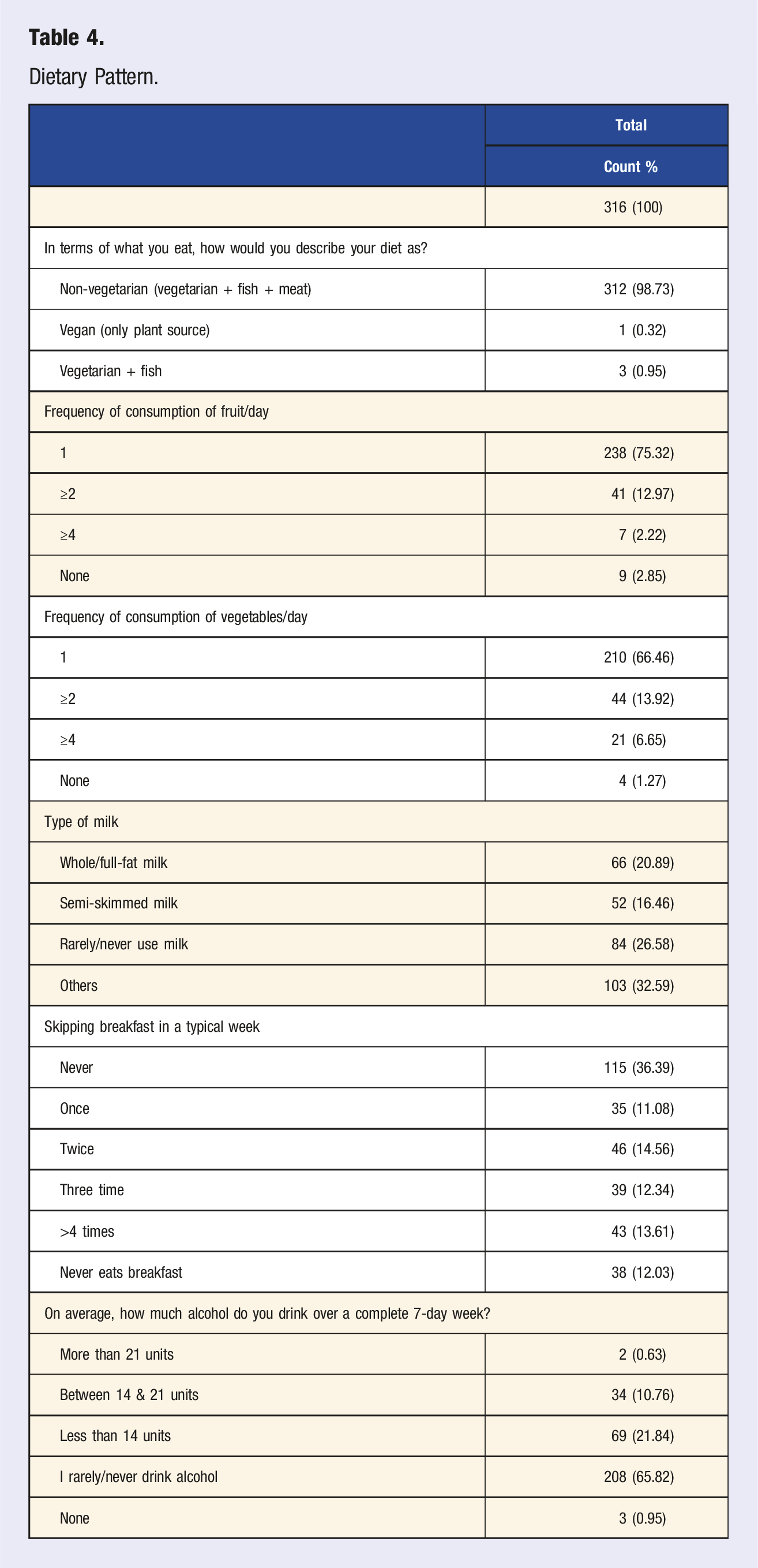
Dietary Pattern.
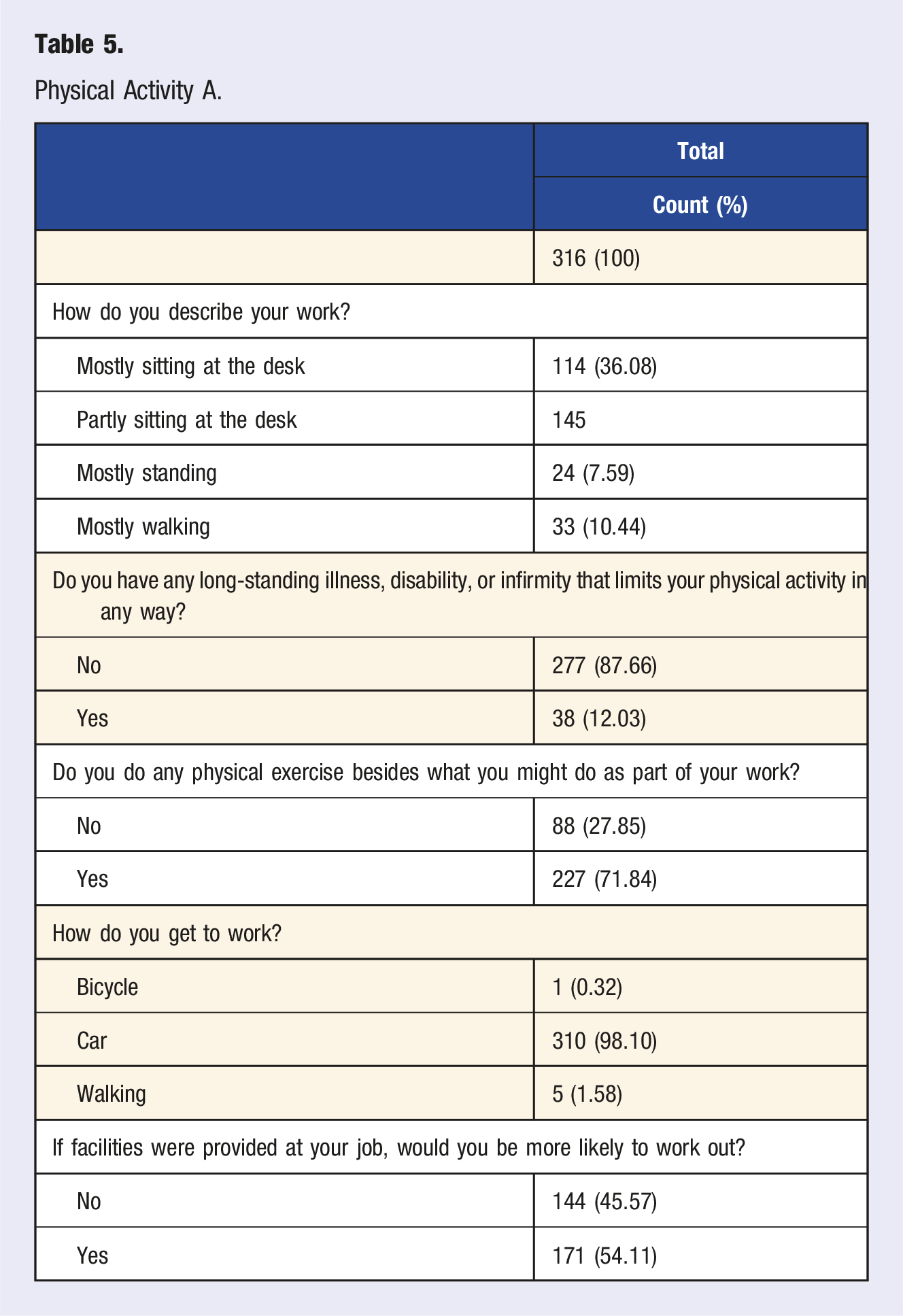
Physical Activity A.
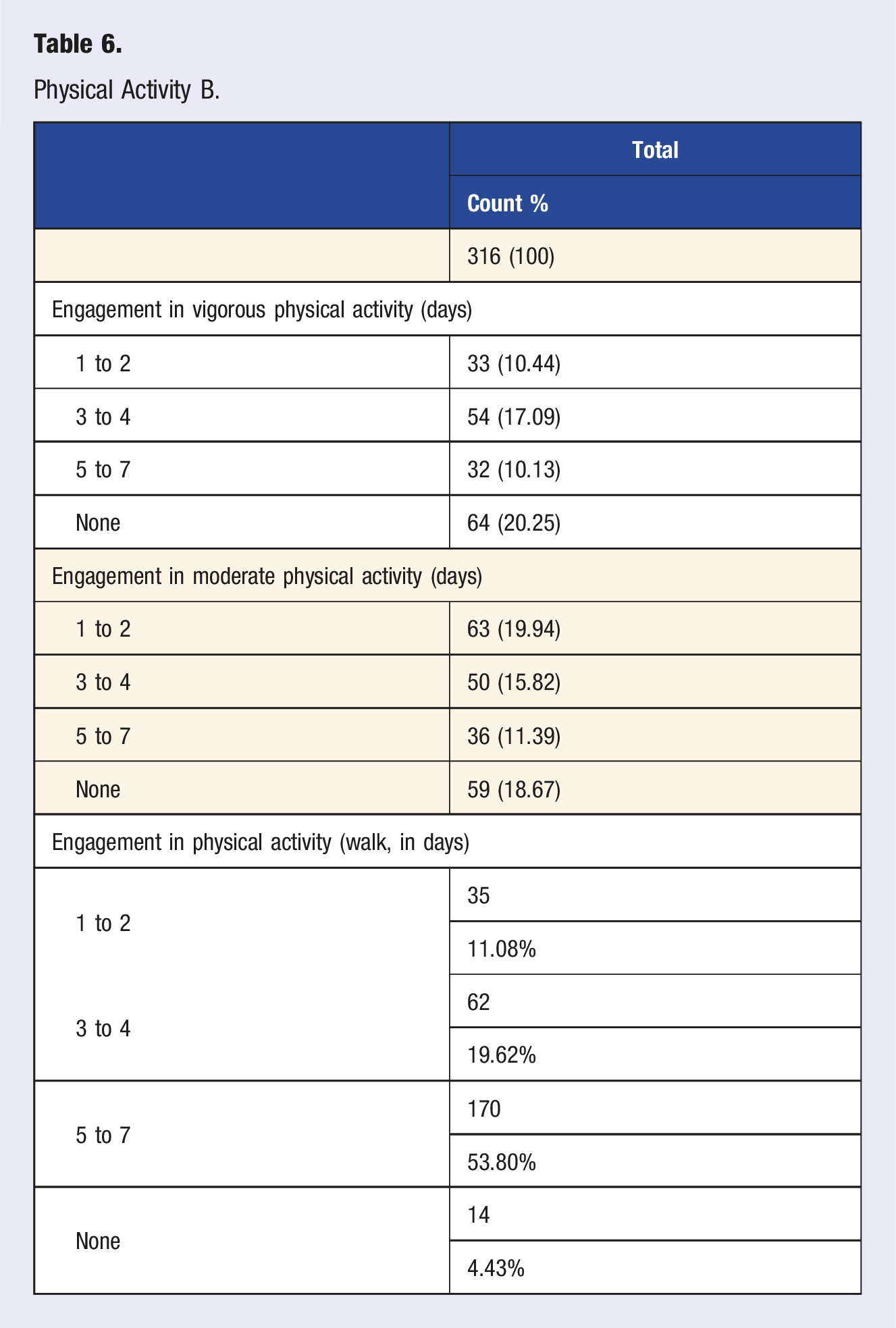
Physical Activity B.
General Questions.
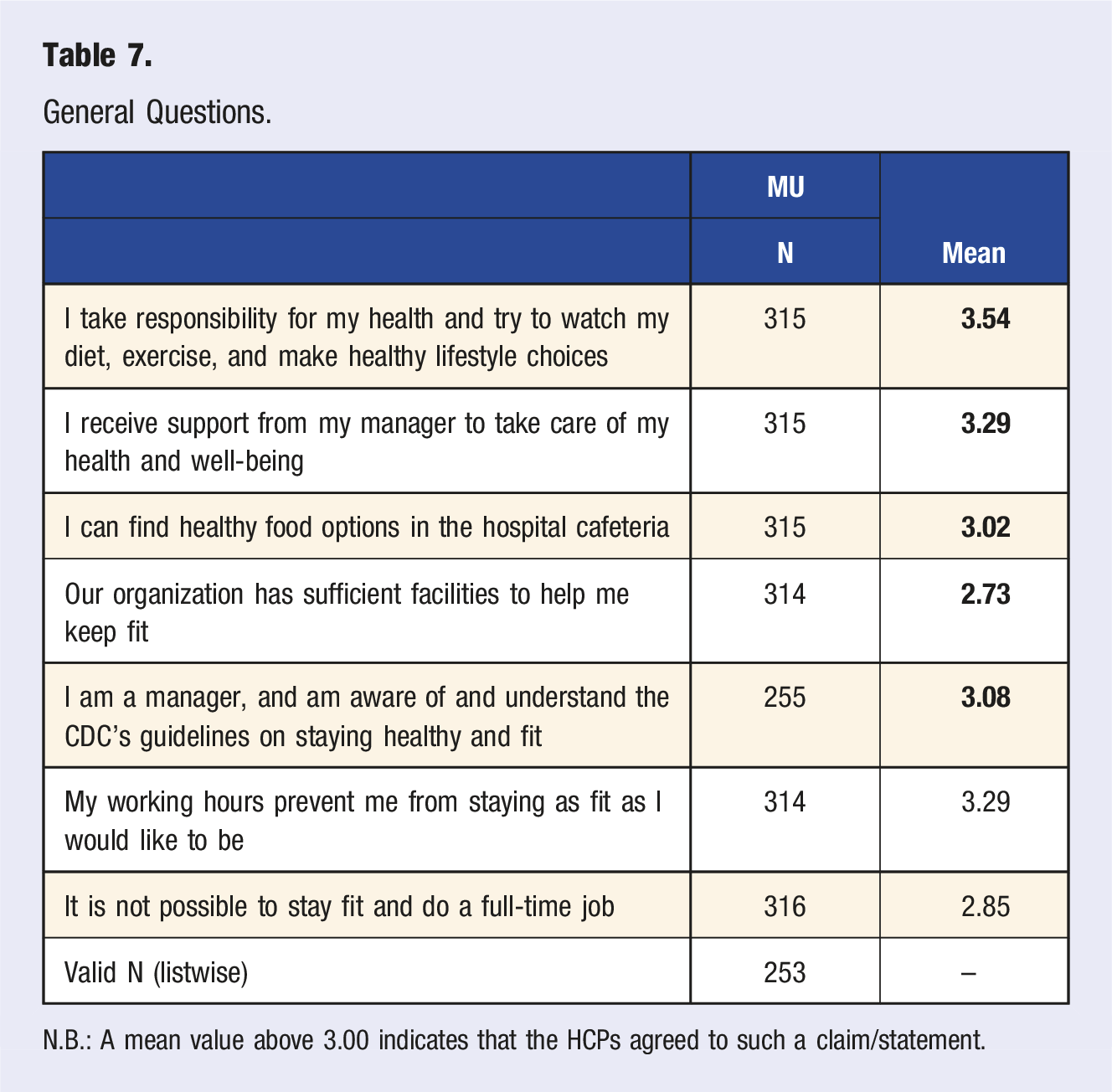
N.B.: A mean value above 3.00 indicates that the HCPs agreed to such a claim/statement.
Figure 1 heat map gives the basis for understanding how the health factors in the dataset are correlated with one another. The scale on the right side of the figure in the heatmap is known as a color bar or a legend. It represents the range of values for the correlation coefficients the heatmap depicts. The color bar shows a gradient of colors corresponding to the values of the correlation, ranging from −1 to 1, where −1 indicates a perfect negative correlation, 0 indicates no correlation, and 1 indicates a perfect positive correlation. The colors transition from one end of the spectrum to the other to visually represent the strength and direction of the correlations between variables in the heatmap. The figures near the scale on the right side are correlation coefficients. These coefficients quantify the strength and direction of the linear relationship between two variables. Variables Correlation Coefficients Heatmap.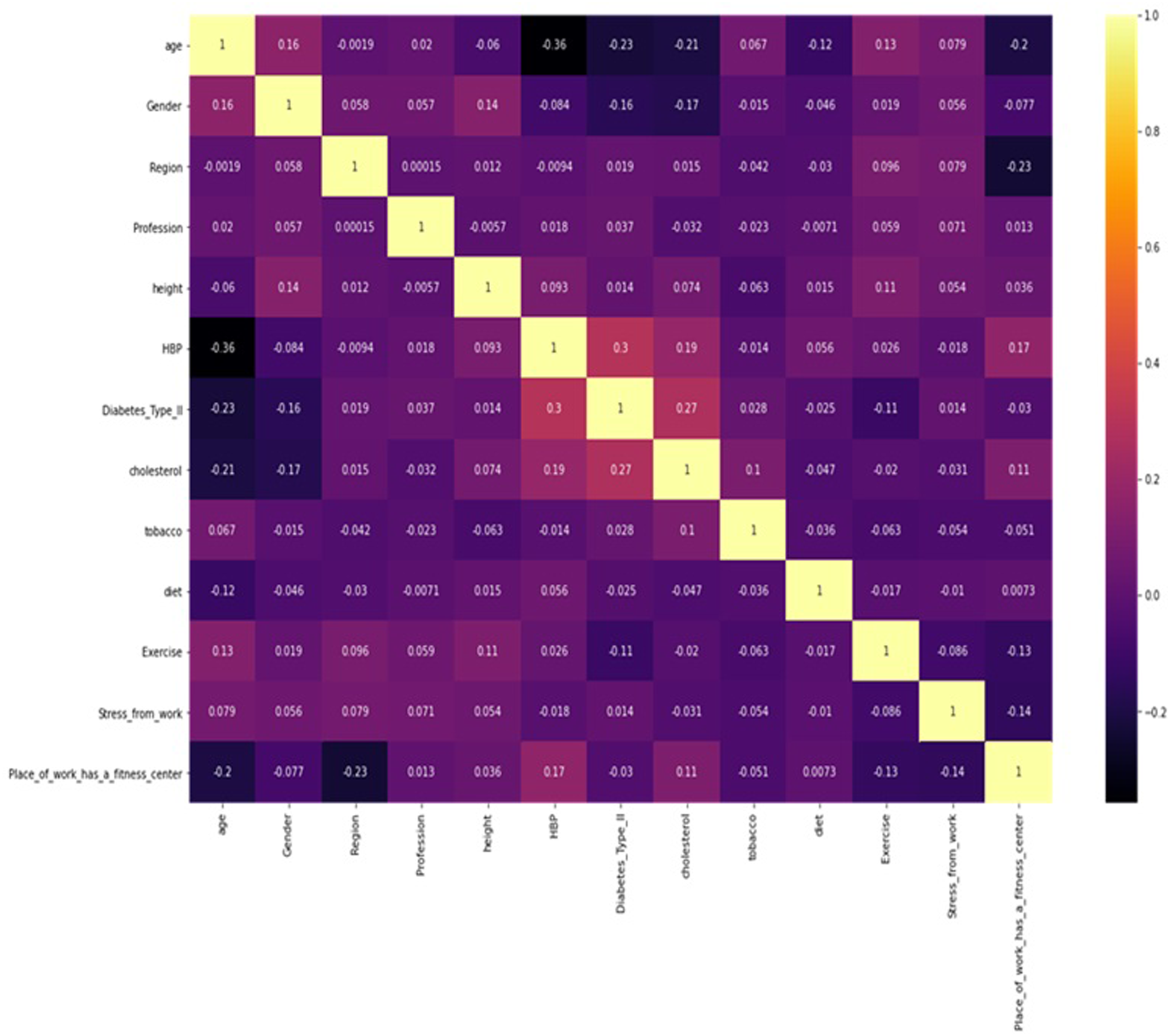
The heat map indicates in the age column, that HBP (Presence of High blood pressure or not), Diabetes type 2 (Diabetes type 2 or not), and Cholesterol (High Cholesterol or not) are the strongest correlated factors with age. The heatmap also indicated that those with high cholesterol are those who do not engage in physical activity.
Discussion
According to Holtzclaw et al 17 HCPs are considered experts in promoting a healthy lifestyle. Despite this, living a healthy lifestyle can be challenging for HCPs in the healthcare workplace.17,18 Holtzclaw et al 17 further stated that HCPs are more likely than the general population to suffer from type 2 diabetes, coronary artery disease, obesity, and stroke. A healthy lifestyle consists of following a good eating pattern, participating in frequent physical activity, preventing tobacco products, getting enough sleep regularly, and controlling stress. 19 To better understand the health of HCPs, this study assessed the prevalence of cardiovascular risk factors such as diabetes, obesity, high blood pressure, and stress among healthcare professionals in medically underserved regions (MURs) of West Central Illinois, as well as attitudes towards and barriers to healthy lifestyle choices.
The present study indicated that HCPs in MURs face similar challenges to the general population when maintaining a healthy lifestyle. While most HCPs reported taking responsibility for their health and making healthy lifestyle choices, they also reported facing barriers, such as a lack of support from their managers and limited healthy food options in hospital cafeterias. Interestingly, the prevalence of medical conditions such as anxiety, depression, and stress were high among HCPs in MURs. This suggests that HCPs may face unique stressors such as unpredicted long work hours, work pressures, witnessing sick patients, and emotions from exposure to deaths at places of work related to their work that contribute to these conditions. 20
Most of the HCPs in MURs had an average weight (100–199 pounds), which falls between the range of normal weight and slightly overweight. Furthermore, upon calculation of the Body Mass Index (BMI), it was found that HCPs in MURs have high BMIs. In a comparable study conducted in Saudi Arabia, 31% of HCPs were overweight. 12
The data reveals some medical conditions such as coronary artery disease, cancer, and musculoskeletal disorders across MURs. A study by Khani et al (2024) revealed that healthcare professionals who work shifts worldwide, both in rural and urban areas, have higher blood pressure compared to those who do not work shifts. According to another study by Benn et al 21 HCPs displayed a mean prevalence of 58.5% for cardiovascular disease (CVD) and a mean prevalence of 22.1% for varicose veins. A study conducted in Malaysia by Hazmi et al 22 revealed that approximately 42% of the 330 selected healthcare workers had at least one medical condition, including dyslipidemia which affected 30.8% of the workers, hypertension (14.3%), or diabetes mellitus (10.4%).
The present study showed that HCPs in MURs have high blood pressure, type 2 diabetes, and high cholesterol. According to Kurtul et al, 23 hypertension affected 13.5% of physicians and 13.9% of other healthcare professionals. Interestingly, Bosu 24 reported that the prevalence of hypertension among healthcare workers varied from 17.5% to 37.5%. However, a worldwide analysis study conducted by Vedanthan et al 25 revealed that hypertension was prevalent among healthcare workers in the 68 countries investigated in their study between 1990 and 2010.
The Dietary Guidelines for Americans advise what should be consumed to meet nutrient requirements, enhance good health, and prevent disease. 26 In the current study, for dietary patterns, the HCPs in MURs showed that most HCPs consumed at least one serving of fruits and vegetables daily and avoided skipping breakfast. In South Africa, a study by Kunene & Taukobong 27 reported that most of the HCPs skipped most of their breakfast, which resulted in poor eating habits among the HCPs in a district hospital in Kwazulu-Natal. In another study, Huang et al 28 found that the healthy eating habits and patterns of HCPs in Singapore decreased with work changes related to the COVID-19 lockdown. Meanwhile, in Mexico, it was also reported that healthy dietary patterns related to being physically active among the healthcare professionals studied, whereas unhealthy dietary patterns were correlated with being less than 22 years old, male, and a tobacco user among healthcare professionals. These findings imply that knowing about healthy practices is not a guarantee that people are going to participate in healthy behaviors. 29
The present study found that lack of time and motivation to work out were the major reasons why the HCPs in MURs did not engage in workout activities. The lack of healthy food options and fitness facilities were noted by participants. A study conducted by Kua et al 30 indicated that a decrease in physical activity levels among healthcare professionals has been observed since the onset of the COVID-19 pandemic. Ironically, Marques-Sule et al 31 reported that physical activity was evaluated among healthcare professionals using the European Health Interview Survey-Physical Activity Questionnaire (EHIS-PAQ), and it was found that 93.51% of all healthcare professionals in Europe were physically active such as walking or using fitness facilities at work. Transport-related physical activity and health-enhancing physical activity were significantly lower in female healthcare professionals. Therefore, future studies must be conducted to focus on specific attention and intervention for HCPs who experience these barriers to physical activity and related lifestyle choices. Doing so may foster a better and healthier working environment. Enabling these behaviors may result in the prevention of cardiovascular illnesses, promotion of longevity, and total well-being in rural regions.
The correlation results (heat map) suggested a connection between a lack of exercise or physical activity and high cholesterol (correlation = 0.02) among HCPs in MURs. This suggests that as age increases, their chances of having high blood pressure increase, the risk of type 2 diabetes increases, and their maximum cholesterol level tends to also increase. In support of our findings, Kua et al, 30 reported that physical activity and diet modification significantly contribute to reducing CVD by improving long-term health, weight management, and lowering high blood pressure. These modifications also help in reducing blood glucose and cholesterol levels, as reported in their study on healthcare professionals’ cardiovascular health. Physical activity and exercise have been shown to play a crucial role in reducing cholesterol levels, particularly among healthcare professionals, as reported by George et al. 32 However, high cholesterol levels can act as a barrier to engaging in physical activity. Brunet et al 33 also found that many nurses suffer from poor health outcomes and risk factors, such as excess weight, high cholesterol, hypertension, type 2 diabetes, anxiety, depression, back problems, and arthritis, which are linked to their professional workload and the crucial role they play in society. The present study also found that the conditions prevent them from being physically active or engaging in exercise.
The heat map also shows a connection between age among HCPs in MURs and high cholesterol, diabetes, and high blood pressure. Similarly, Singh et al 34 reported that cardiovascular disease (CVD) incidence typically increases with age in most populations, including healthcare professionals, although the relationship between age and CVD varies across countries and has evolved. This association is thought to be partly because major CVD risk factors, such as blood pressure, cholesterol, and diabetes, tend to rise with age, and the effects of these risk factors accumulate over the life course. 34
Recommendations
These findings of this study have important implications for healthcare organizations and policymakers. Interventions and policies are needed that target HCPs in rural regions, aimed at promoting healthy lifestyle behaviors and improving access to healthy food options in hospital cafeterias, thereby creating a healthier workforce in the MURs in the United States. Healthcare organizations should also consider providing more support for their employees to take care of their health and well-being. Future research could build on existing longitudinal studies to track healthcare professionals’ cardiovascular health, by examining barriers and facilitators to behavior changes. This would provide further insights into how these variables and risk factors impact their general health and well-being. The study finding was that the barriers to participating in physical activities and exercises are lack of time, motivation, and access to facilities, developing interventions should be put in place to overcome these barriers and increase their participation. Also, given the high prevalence of stress, depression, and anxiety, future research could create interventions that would focus on the mental health of these healthcare professionals in medically underserved regions. Furthermore, future research could examine HCPs numbers for cholesterol, hypertension, and diabetes to gain insight into how healthcare providers are managing these conditions and adhering to the health recommendations they give to their patients. Additionally, it would be valuable for future studies to explore sleep patterns, work hours, and cardiovascular health of healthcare professionals to inform policies related to their work-life balance, especially concerning long work hours and shift work. Overall, the results suggest that there is a need to address the health-related behavior and lifestyle choices between healthcare professionals in rural regions of Illinois to improve the overall health and well-being of this population.
Limitations
The study’s findings represent only healthcare professionals in West Central Illinois and may not reflect other regions. Due to the study’s cross-sectional nature, the findings capture a specific moment in time and would benefit from longitudinal tracking of participants. The self-selected and self-reported nature of the study, as well as the approximately 88% female representation, limit the data accuracy and generalizability of the data. Additionally, cultural differences may exist in the survey tools adapted from Saudi Arabia.
Conclusion
In conclusion, the current study’s outcomes reveal that HCPs in MURs experience obstacles in maintaining a healthy lifestyle. This study highlights the impact of time constraints and lack of motivation on HCPs’ participation in physical activity in rural regions. This study suggests that limited access to nutritious food and exercise facilities in rural areas contributes to lower rates of healthy eating and physical activity. Moreover, the study revealed that healthcare professionals have high cholesterol levels, a finding consistent with existing literature. This is likely due to their sedentary lifestyle, possibly resulting from limitations such as lack of time, work-related stress, and low motivation to exercise or engage in physical activity, as reported by healthcare professionals. Additionally, the study showed that as individuals age, their risk of developing cardiovascular disease increases. Implementing targeted interventions and increasing accessibility can enhance overall physical activity participation, improve healthy food consumption, and reduce health disparities, resulting in a healthier workforce among HCPs.
Supplemental Material
Supplemental Material - Understanding Cardiovascular Health and Lifestyle Choices Among Healthcare Professionals in Medically Underserved Regions in Illinois
Supplemental Material for Understanding Cardiovascular Health and Lifestyle Choices Among Healthcare Professionals in Medically Underserved Regions in Illinois by Grace Aruoriwo Agah, Lynn Katherine Herrmann, Maureen P. Bezold, and Moshood F. Yussuf in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.