
Abstract
“Our study findings highlighted a notable difference in adhering to positive lifestyle patterns and OHRQoL between Whites and Asians living in a blue zone.”
Introduction
Blue Zones are areas scattered across the globe where people consistently exceed conventional lifespan expectations, often surpassing the centenarian mark. These rare locations include Okinawa, a pacific island situated at the southernmost of Japan, Ikaria, a mountainous Greek island located in the Eastern Aegean Sea, Sardinia, a mountainous terrain that is located along the western coast of Italy in the Mediterranean Sea, Nicoya, a northwestern region of Costa Rica located along the Pacific Ocean, and lastly, Loma Linda, a Southern Californian city in the United States, which is predominantly inhabited by Seventh-Day Adventists.1,2 Researchers, including Dan Buettner, have focused on understanding the secrets behind their unique longevity and seeing whether these traits can be adopted by the general population. Buettner and his team unveiled the “Power 9®,” a compilation of evidence-based lifestyle habits common across these zones. According to the concept, Blue Zone residents have a clear sense of purpose, are physically active, manage stress effectively, and practice dietary moderation. Residents typically prioritize plant-based diets or minimal meat consumption and often enjoy wine in moderation, supported by religious and family values that create strong social networks essential for holistic well-being. 3
In contrast to their remote counterparts, Loma Linda is an urban city situated in San Bernardino County, California, USA, with a population of around 25,000 as per the 2020 census. 4 Nearly one-third of Loma Linda’s residents are Adventists, who embrace a lifestyle characterized by wholesome nutrition, ample rest, regular exercise, and abstinence from deleterious substances like alcohol, tobacco, and narcotics, all founded by a steadfast devotion to faith and hope to give meaning to life. 5 Numerous studies have linked the Adventist lifestyle to longevity and health.5-8 One study highlighted that Adventist students were more likely to follow healthier lifestyle behaviors compared to non-Adventist students, and that these behaviors were strongly linked to lower obesity risk and reduced risky eating patterns. 5 Notably, vegan diets, were associated with decreased risk of cardiovascular diseases, obesity, hypertension, type-2 diabetes, and certain types of mortality. 6 Moreover, adopting healthy eating habits could help effectively prevent long-term weight gain. 7 Additionally, vegetarian diets showed significant benefits in reducing mortality related to cardiovascular conditions, non-cancer diseases, renal issues, and endocrine disorders. 8 Despite the existing literature on the relationship between lifestyle and health, there remains a lack of exploring the relationship between lifestyle patterns and oral health.
Hence, to assess the relationship between lifestyle and oral health the short version Oral Health Impact Profile (OHIP-14) was used in this study. OHIP-14 is a widely used tool to assess the impact of oral problems on the perceived quality of life of individuals.9-12 The OHIP-14 questionnaire is composed of 14 questions that each address a specific facet of oral health and its impact on an individual’s daily life. Responses are scored and summed to provide an overall measure of oral health’s impact on quality of life, with higher scores indicating a more significant negative effect. 13
The objective of the study was to assess the relationship between lifestyle patterns and oral health related quality of life in the Blue Zone of Loma Linda. We aimed to determine how participants living in this Blue Zone adhere to the “Power 9®” characteristics relevant to Loma Linda. We hypothesized that most participants would adhere to a lifestyle pattern unique to Loma Linda. Furthermore, we sought to examine the link between these lifestyle traits and oral health related quality of life. We hypothesized that there would be predictors related to oral health related quality of life.
Methods
Cross-Sectional Study Design and Sample Size Calculation
The study involving adults aged 18 years and above residing in Loma Linda, California, was conducted upon the approval by the Loma Linda University Institutional Review Board (IRB #5230470). Prospective participants were approached by a member of the research team at venues including Loma Linda University School of Dentistry as well as through outreach efforts at local churches and community centers. Participation involved the completion of a survey, with participants having the liberty to proceed at their own pace and not respond to all inquiries. As a token of appreciation, participants received a complimentary pen upon completing their involvement in the study.
The questionnaire used in this study was developed by integrating questions from a previously validated OHIP-14 questionnaire 9 and others specifically designed for this research. Consisting of 28 items, the questionnaire was structured into 3 sections. Previous research suggested that a sample size of 130 in each group would be necessary to find a 35% difference in cumulative OHIP-14 score between Whites and Asians for 80% statistical power. 14
Section I. Demographics
Demographics included residency in Loma Linda, age, gender, education level, race (categorized as White, African, Asian, Indian, and Hawaiian), and ethnicity.
Section II. Power 9® Lifestyle
This section of the questionnaire covered level of adherence to the Power 9®. These dimensions included adherence to Sabbath observance, regular exercise, social engagement, nut consumption, volunteering activities, dinner timing, vegetarian diets, and water intake. Lifestyle adherence was assessed with a focus on nut consumption and exercise. Participants rated their adherence on a 4-point Likert scale, ranging from 1 (strong adherence) to 4 (poor adherence). The cumulative score for lifestyle adherence ranged from 8 to 32, with lower scores indicating greater conformity to the Power 9®.
Section III. OHIP-14
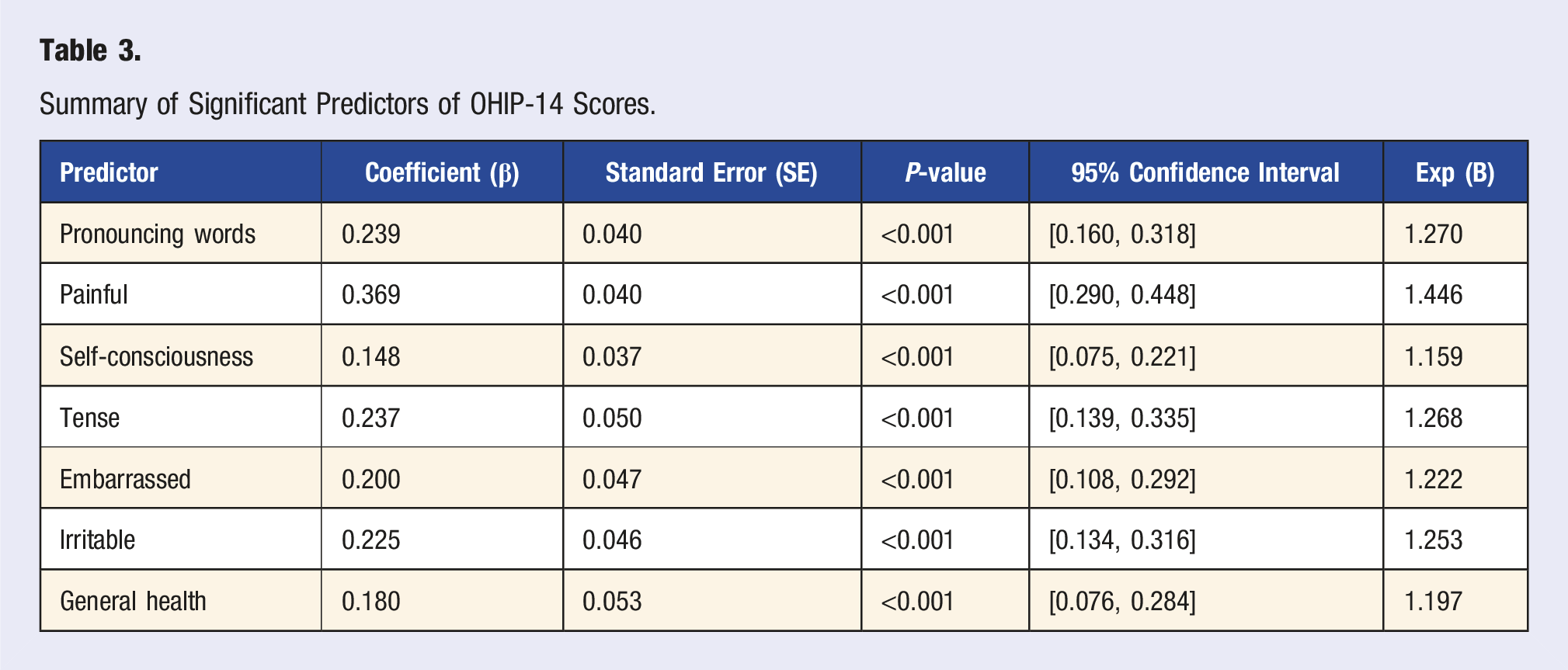
To assess Oral Health Related Quality of Life (OHRQoL), the study utilized OHIP-14, which addresses functional limitations, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and other handicaps. The severity of OHRQoL impacts was quantified by calculating a cumulative OHIP-14 score, ranging from 0 to 56. Higher OHIP-14 scores indicating worse OHRQoL, while lower OHIP-14 scores indicating better OHRQoL. Specific oral health indicators, including difficulties in pronouncing words, experiencing pain, feeling self-conscious, tense, embarrassed, irritable, and general health status, were measured and included as predictors in the model.
Data Analysis
The findings of descriptive analyses for cumulative score for lifestyle and OHIP-14 score, were reported as Mean ± SD. One-way analysis of variance (ANOVA) followed by Tukey HSD post-hoc test was used to test differences in OHIP scores by race. A Negative Binomial regression model was used to analyze the relationship between OHIP-14 scores (dependent variable) and the predictors, including race, lifestyle factors (nut consumption and exercise), and oral health indicators. This model was selected due to the overdispersed nature of the OHIP-14 scores. The log link function was used, and the model fit was assessed using the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), deviance, and Pseudo R-squared. Model diagnostics were performed to check for overdispersion and multicollinearity among predictors. We used several R (v4.4.1) and Python (v3.12) packages for data analysis and visualization.
15
The R packages “
In Python, the “
Results
Descriptive Analysis
A total of 350 surveys were collected, with 20 ineligibles due to non-residency in Loma Linda and 10 exhibiting incomplete responses, with over 50% of questions unanswered. Ultimately, 320 participants residing within Loma Linda were included in the study. Participants’ age ranged from 18 to 88 years (Mean = 51.51, Standard deviation (SD) = 19.70). Gender distribution indicated that 60% were female, with the remaining being male or other. With respect to education, the majority of participants reported completing higher education (94.7%). Whites and Asians were the predominant racial groups within the participants, making up 48.6% and 45.3%, respectively.
Power 9® Lifestyle
The cumulative lifestyle score was measured by the overall sum of “Power 9®” adherence and ranged from 8 to 24 (Mean = 13.9, SD = 3.6). Figure 1 illustrates how participant adherence to these lifestyle habits varied, from strongly agree to strongly disagree within each item. Among the “Power 9®” lifestyle items, spending time with friends was the most adhered to activity, with 96% of participant engagement. Following closely, 90.3% of participants frequently ate plant-based foods, and 88.8% reported high water consumption. Conversely, the least followed habits were eating an early dinner (71.2%) and snacking on nuts (75.3%). Bar Graphs of Adherence to “Power 9®” Lifestyle.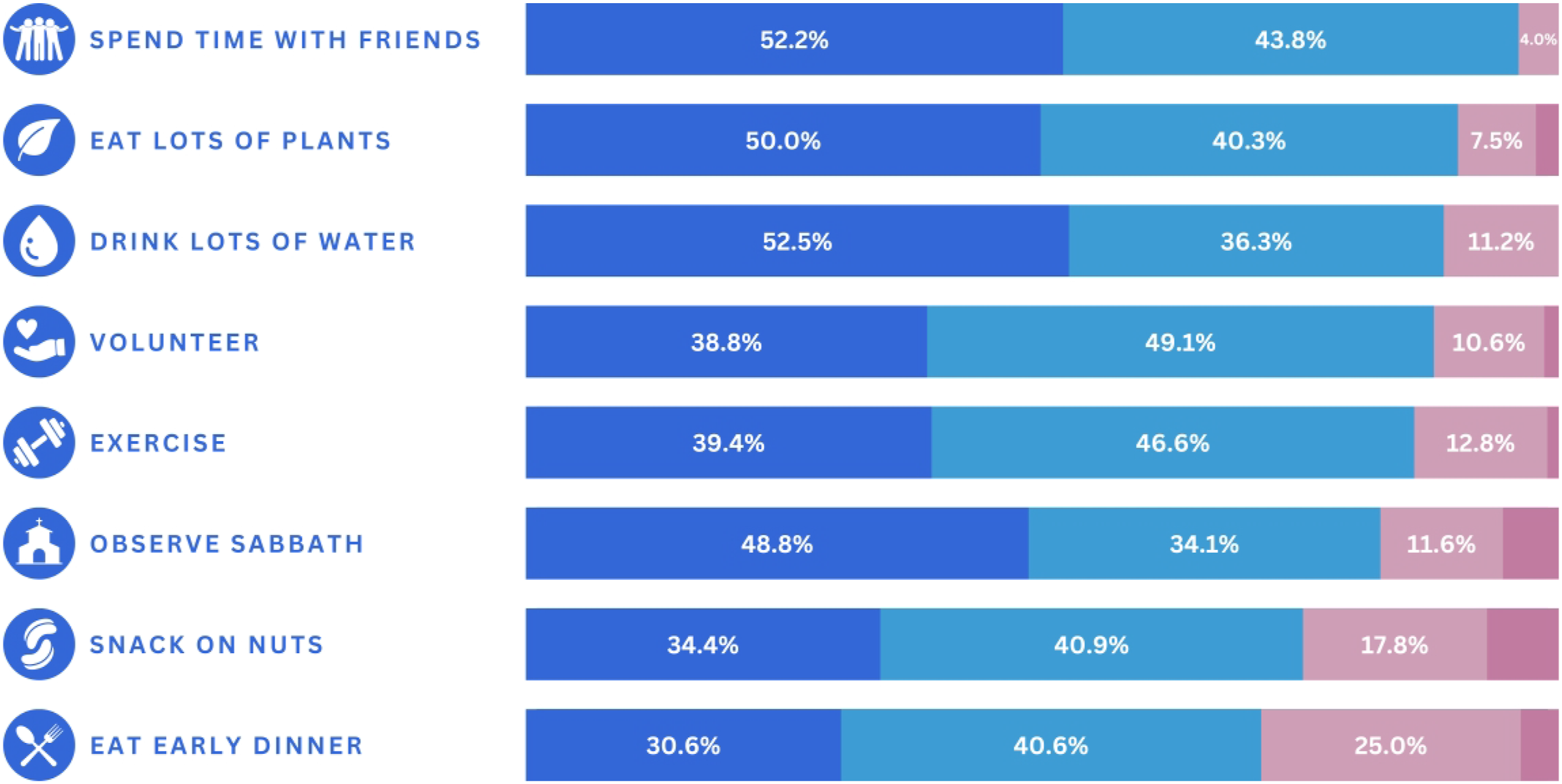
OHIP-14
OHIP-14 Scores (Mean/SD) by Domain and by Race.
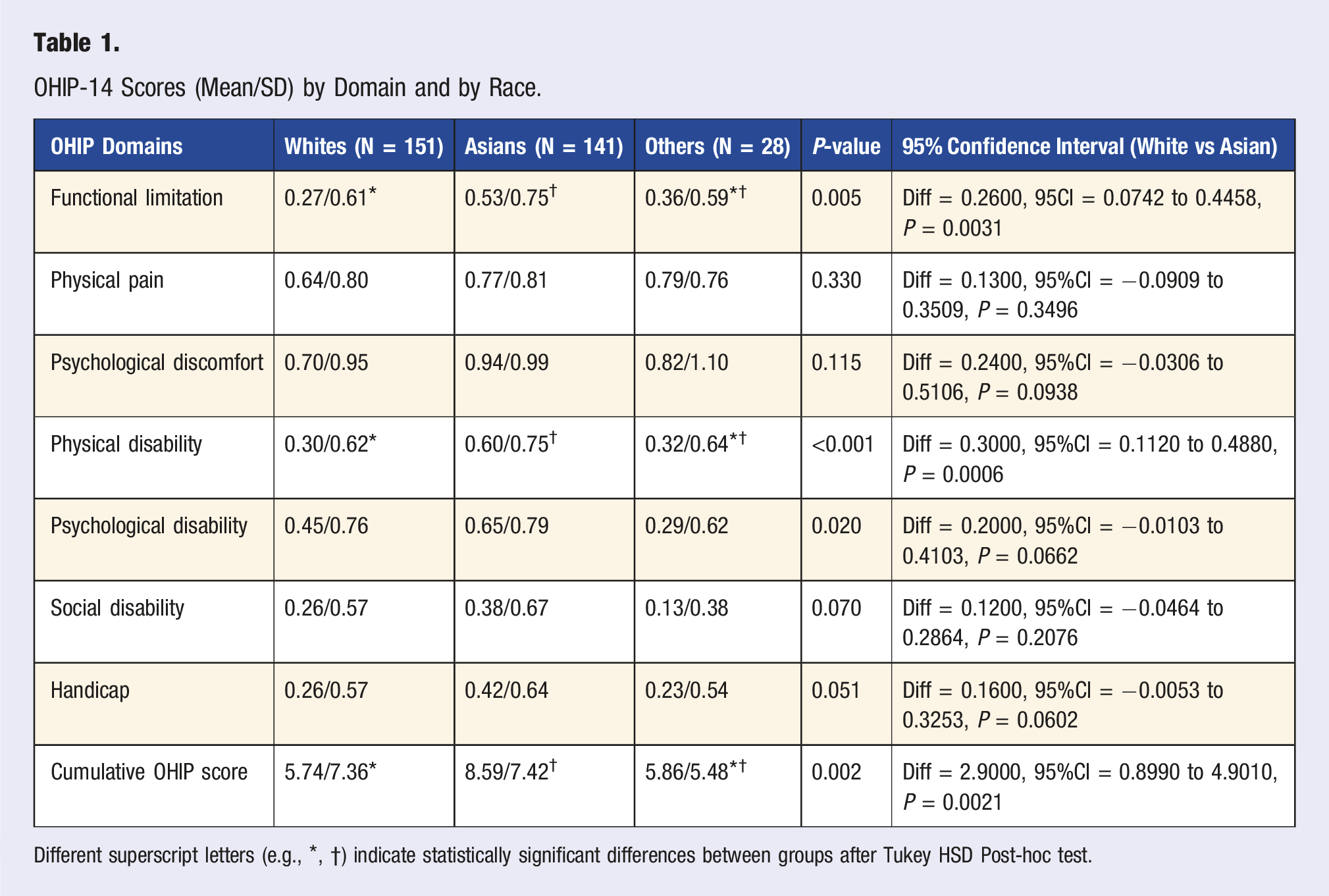
Different superscript letters (e.g., *, †) indicate statistically significant differences between groups after Tukey HSD Post-hoc test.
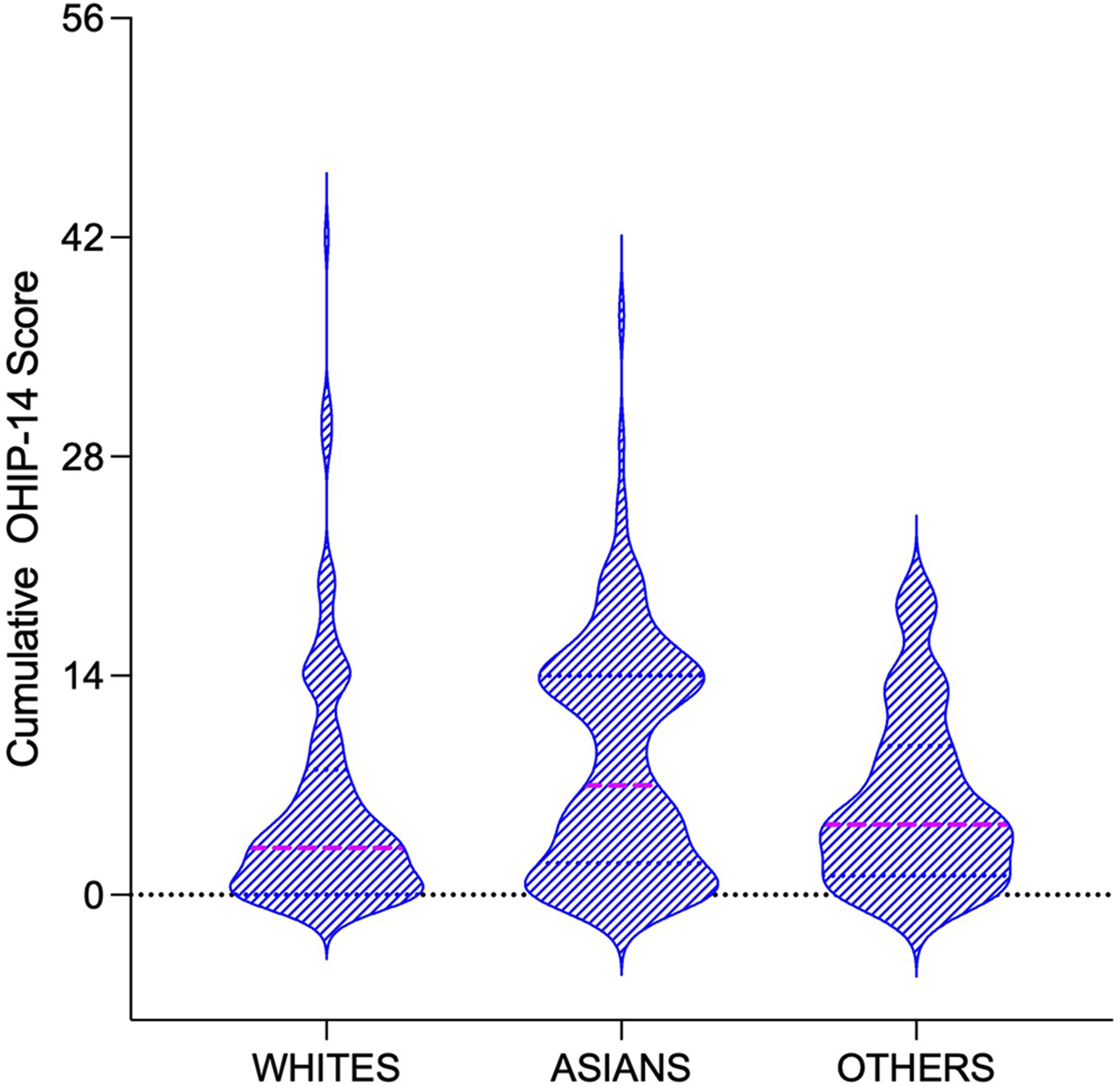
Violin Plots of Distribution of Cumulative OHIP-14 by Race.
Negative Binomial Regression
Negative Binomial Regression Model and Outcomes of Predictors.
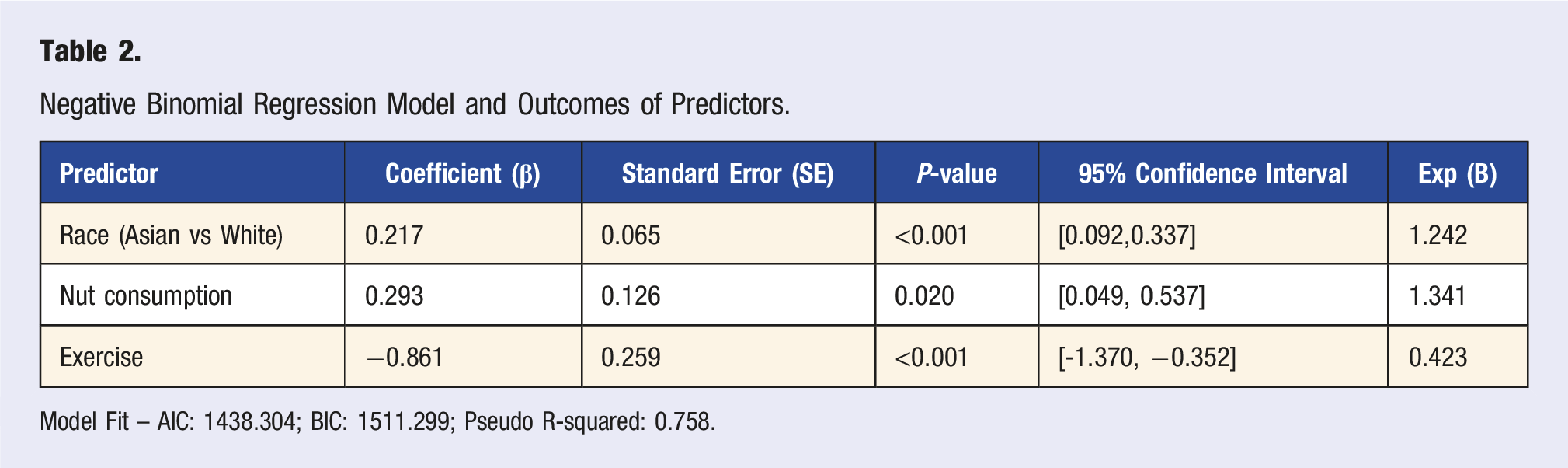
Model Fit – AIC: 1438.304; BIC: 1511.299; Pseudo R-squared: 0.758.
Summary of Significant Predictors of OHIP-14 Scores.
Model Diagnostics
The model was well-fitted, as indicated by a Chi-squared/DF ratio of 0.967, which suggests that the model appropriately accounted for overdispersion. Residual analysis showed no significant deviations from the model’s assumptions, and multicollinearity among predictors was not problematic, ensuring the robustness of the model.
Limitations of the Model
Despite the strong fit, the model’s complexity could still pose risks of overfitting, particularly with the inclusion of multiple predictors. Simplifying the model by focusing on the most significant predictors can further reduce this risk while maintaining explanatory power.
Discussion
Scientists are hard at work trying to understand what causes aging and exploring strategies to extend human lifespan, often looking to the characteristics of blue zone residents for inspiration. While studies have identified evidence-based lifestyle patterns unique to these areas, few have assessed residents’ adherence to these patterns. Our study is the first to evaluate the adherence of urban blue zone residents to these lifestyles and their correlation with oral health related quality of life. We found remarkably high adherence to positive lifestyle patterns. Out of ten residents 9 adhered well to activities such as “spending time with friends” and “volunteering” which appears crucial in fostering community connection and preventing isolation. This social aspect may indeed play a vital role in promoting a healthy, long life—a notion supported by research indicating that the presence of family members or supportive social systems correlates with increased life expectancy.16,17 Moreover, prioritizing a plant-rich diet and ample water intake highlighted the significance of diet in the lives of blue zone residents which is in accordance with an Adventist Health study that reported that vegetarian dietary patterns were associated with lower mortality. 8
It is important to note that the 2 major chronic oral diseases, periodontal disease and dental caries, could benefit from decreasing the intake of processed, high-glycemic carbohydrates. In contrast, consuming complex carbohydrates that are rich in fiber, such as fruits, vegetables, legumes, nuts, and seeds, could help reduce periodontal inflammation.18,19 This observation supports our hypothesis that residents of Blue Zones, who typically follow a plant-rich diet and snack on nuts, may demonstrate better oral health and an enhanced quality of life. This is also in accordance with another study that showed that salad or fresh vegetable consumption was positively associated with lower cumulative OHIP‐14 scores. 20 It is important to note though that based on the regression analysis, the plant-based diet was not a statistically significant predictor for OHRQoL. Based on our findings, we accepted our hypothesis as lifestyle traits such as nut consumption and exercise were significant predictors for oral health related quality of life. Loma Linda blue zone residents’ cumulative mean OHIP-14 of about 7 was lower than a comparable cohort of older adults residing in San Bernardino County, California where the cumulative mean was 16. 14 The study also reported a notable disparity in oral health related quality of life among different racial groups which is in accordance with findings of our study. Another study that used the cross-sectional NHANES 2003-2004 survey of a nationally representative sample of US adults where the mean age was 43a0years reported a cumulative mean of 2.8. 21 However, it is important to note that the Sanders study used a subset of OHIP-14 consisting of 7 questions and it is not clear how it can be compared to the cumulative score using 14 questions.
Our study findings highlighted a notable difference in adhering to positive lifestyle patterns and OHRQoL between Whites and Asians living in a blue zone. It is noteworthy that the 3 largest ethnic groups in Loma Linda are Whites (35.2%), Asians (25.3%), and White Hispanics (8.75%). 4 There are several limitations to the study. One significant limitation is the lack of representation of the White Hispanic group. Other limitations include the self-reported nature of data for lifestyle adherence and oral health related quality of life, which can introduce biases and inaccuracies. Additionally, the cross-sectional design of the study limits the ability to establish a causal relationship between lifestyle factors and oral health outcomes. Lastly, the limited sample size could negatively affect the validity and generalizability of our study findings.
A major outcome of our study is augmenting awareness about the unique opportunity oral health care providers can assume in promoting healthy lifestyles. Currently, most dental professionals do not include nutritional counseling or healthy lifestyle promotion such as exercise in their services, highlighting a significant gap in recognizing the dentist’s role in healthy diet and lifestyle choices. 22 Our findings indicate that future studies are warranted to investigate the benefits of proactive diet and lifestyle counseling by dental professionals. These initiatives could not only help in preserving oral health but may also improve overall quality of life and longevity.
Within the limitations of the study, we conclude that Loma Linda residents adhere well to the Power 9® lifestyle and demonstrate overall favorable oral health related quality of life. There are significant predictors such as nut consumption and exercise for increased oral health related quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.