
Abstract
Keywords
“The critical findings are that participants reported increased knowledge, confidence, and practice of LM after completing the Essentials course.”
Introduction
The practice of lifestyle medicine draws on behavior change principles to encourage patient adoption of healthy lifestyles to prevent and treat chronic illness. A growing body of evidence supports the efficacy of lifestyle medicine (LM) to treat and prevent non-communicable (chronic) diseases (NCDs), 1 especially cardiovascular disease,2,3 type 2 diabetes,4,5 cancer, 6 and obesity.7,8 The American College of Lifestyle Medicine (ACLM) defines LM as the “medical specialty that uses therapeutic lifestyle interventions as a primary modality to treat chronic conditions,” 9 and has identified 6 pillars of lifestyle medicine: whole-food, plant-predominant eating pattern; physical activity; restorative sleep; stress management; avoidance of risky substances; and positive social connections. 10 Such lifestyle recommendations are already incorporated into clinical practice guidelines for NCD11,12; however, implementation is limited as compared to other aspects of the standard of care, such as pharmaceutical treatments.13,14
Inadequate knowledge, skills, and confidence in LM and behavioral counseling are cited as barriers to LM practice.14-17 The role of these individual factors also appears in behavioral and healthcare practice models, such as the Theory of Planned Behavior and the Longitudinal Education for Advancing Practice, which identify knowledge and self-efficacy as factors influencing individual health and clinical practice behaviors.18,19 Although the biological functions impacted by nutrition, physical activity, and sleep behaviors are included in medical training, physicians report a lack of skill and confidence to advise patients in changing these behaviors.14,16,17,20 Additional counseling skills, (e.g., motivational interviewing), are also lacking among many physicians and other clinicians. 21
As part of a larger strategy to address this gap in training, ACLM launched an educational course in 2022 in support of the White House Conference on Hunger, Nutrition, and Health. The Lifestyle Medicine & Food as Medicine Essentials Bundle (Essentials course) was designed to introduce physicians and healthcare professionals to lifestyle medicine and encourage LM practice. The 5.5-h training program is online, asynchronous, and meets continuing medical education (CME) requirements for physicians and continuing education (CE) for many clinician types, including nurses, pharmacists, registered dietitians, social workers, and national board-certified health and wellness coaches. 22 This program is unique in its brief and scalable qualities. As of early January 2024, Essentials course registration reached almost 35,000 individuals, including approximately 9000 from ACLM’s partnering health systems.
Literature suggests that knowledge, attitudes, confidence, and, to some extent, clinician practice behaviors are likely to respond to CME exposure, and online courses have similar effects to in-person interventions with the added benefit of being flexible and lower cost. 23 These findings are supported in the case of lifestyle medicine and behavior change training programs, having shown to improve attitudes, knowledge, and confidence towards practicing LM, and the adoption of behavioral counseling practices.15,24 Much of this work, however, is in small, homogenous populations, and often delivered through intensive, in-person, multi-component formats.15,25 The impact of a widely available, brief (<6 contact hours) online education course, such as the Essentials course, is not yet known. The purpose of this study is to determine if and how clinician knowledge, confidence, attitudes, and practice change after participation in the ACLM Essentials course.
Methods
Education Description and Dissemination
The Essentials course is composed of 3 modules: Introduction to Lifestyle Medicine (1 h); Food as Medicine: Nutrition for Prevention and Longevity (3 h); and Food as Medicine: Nutrition for Treatment and Risk Reduction (1.5 h). 22 Course development was led by LM certified physician and registered dietitian subject matter experts and included multiple rounds of review and iteration by the ACLM Continuing Medical Education (CME)/CE Planning Committee, which includes a LM certified physician, licensed nurse practitioner, registered dietitian, pharmacist, and psychologist. The accredited CME course is approved by the Accreditation Council for Continuing Medical Education, the American Nurses Credentialing Center, the Accreditation Council for Pharmacy Education, and many other credentialing bodies for allied health professionals. 26
The content encompasses all 6 pillars of lifestyle medicine and is guided by Core Competencies in Lifestyle Medicine. 27 Because dietary risks are shown to be a leading factor in morbidity and mortality, 28 there is an emphasis on nutrition and the Dietary Guidelines for Americans. 29 Course learning materials include interactive presentations, quizzes, case studies, and surveys. The education modules are housed in BrightSpace Community, a virtual learning management system (LMS) used widely in academic settings. 30 Instructional designers advise on course formatting to meet Universal Design for Learning. 31 Participants self-enroll and complete the course at their own pace, and take approximately 30 days to complete.
The CME opportunity is available free-of-charge from ACLM (https://portal.lifestylemedicine.org/Portal/ACLM/Education/Campaigns/White-House/WHconference-SignIn.aspx). 32 Course licenses were disseminated in fall 2022 in collaboration with the White House Conference on Hunger, Nutrition and Health. Additionally, the ACLM provided course licenses to ∼150 health systems, which promoted the course throughout their usual communication channels.
Survey
All participants were invited to complete an optional pre- and post-course survey hosted within the LMS. Questions included assessment of: clinician demographics (age, gender/sex, race, clinical degree/licensure, and ACLM membership status); practice setting; LM attitudes, knowledge, and confidence; and self-reported practice of LM.
The pre-course survey consisted of 57 questions, and the post-course survey had 54 questions; 53 questions were identical in both survey timepoints. LM knowledge and confidence were assessed by a series of 7 five-point Likert questions—one for general knowledge (“LM overall”) and one for each of the six LM pillars. The five-point Likert scales ranged from “none/no knowledge” or “not at all confident” (1 point) to “advanced/expert knowledge” or “very confident” (5 points). Five-point Likert scales also assessed attitudes and self-reported practice behaviors. Interest was assessed by the question reading, “How interested do you feel in using lifestyle intervention as a core component of medical practice?” Experience was assessed by the question reading, “What is your level of experience in practicing lifestyle medicine?” Intention was assessed by the question reading “How likely are you to provide lifestyle recommendations to patients for treatment/prevention of chronic disease?” Frequency was assessed by the question reading, “How often do you ask your patients if they are interested in trying a lifestyle-based approach to their care?” Reach was assessed by the question reading, “With how many of your patients do you currently practice lifestyle medicine?”
Analysis
This analysis was restricted to individuals who reported being healthcare professionals in active practice and completed the pre- and post-course surveys by September 14, 2023. Results were stratified by self-reported clinical degree/licensure. Physicians/APPs include MDs (medical doctors), DOs (doctors of osteopathic medicine), APNs (advanced practice nurses), PAs (physician associates), and NPs (nurse practitioners).
SAS Analytics Software (version 9.4) was used to clean and analyze the data. Each question was analyzed individually. Questions with Likert responses were scored in one-point intervals and ranged from 1-5 points. Descriptive statistics were generated for the sample overall and by practitioner type. A repeated-measures linear model was run to test for changes in the outcomes of interest within each practitioner group, while controlling for age, gender/sex, race, ethnicity, clinical degree/licensure, and presence of health system value-based care model (any or none). After applying a Bonferroni correction to adjust for 20 multiple comparisons, a critical value of P < .0025 was used.
Ethics
The University of New England Institutional Review Board reviewed and approved the study protocol. All participants received a participant information sheet. As stated in the survey, completion of the survey implied consent.
Results
Survey Respondent Demographic and Practice Setting by Clinician Type.
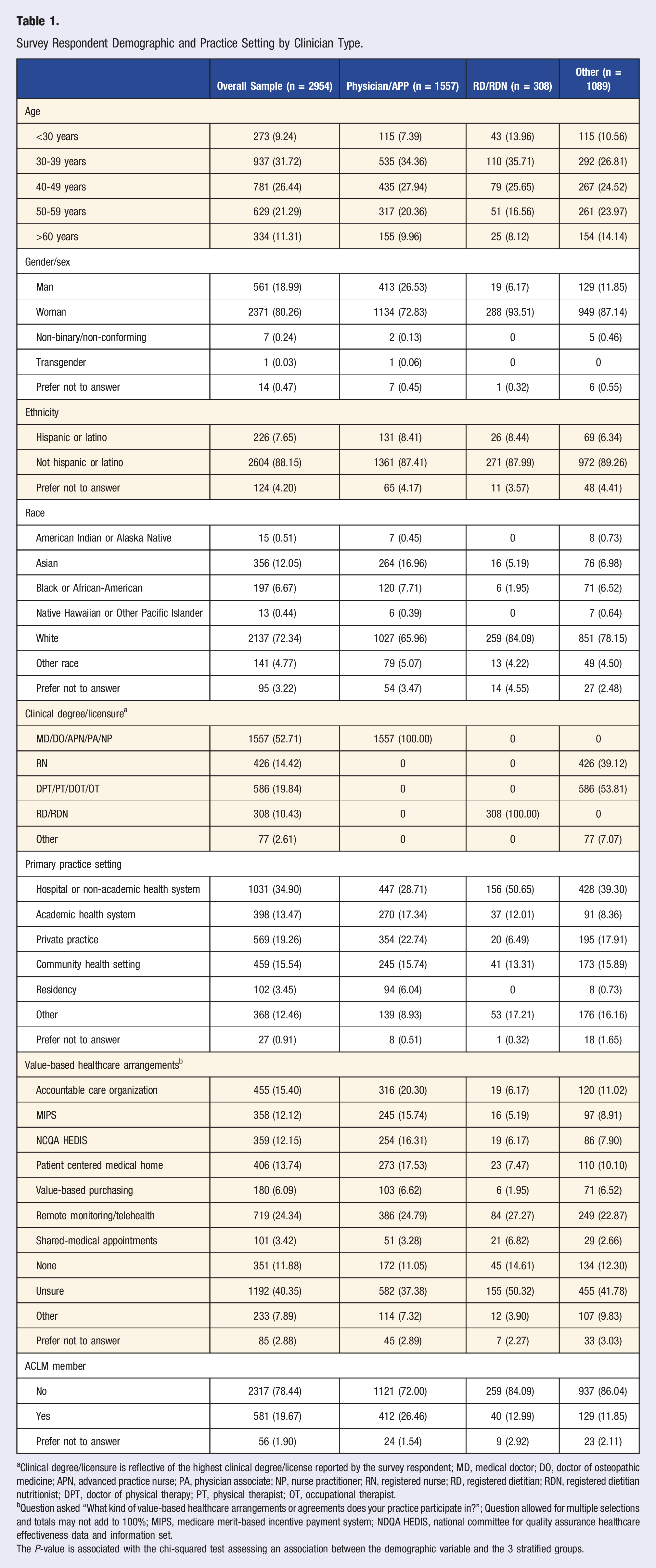
aClinical degree/licensure is reflective of the highest clinical degree/license reported by the survey respondent; MD, medical doctor; DO, doctor of osteopathic medicine; APN, advanced practice nurse; PA, physician associate; NP, nurse practitioner; RN, registered nurse; RD, registered dietitian; RDN, registered dietitian nutritionist; DPT, doctor of physical therapy; PT, physical therapist; OT, occupational therapist.
bQuestion asked “What kind of value-based healthcare arrangements or agreements does your practice participate in?”; Question allowed for multiple selections and totals may not add to 100%; MIPS, medicare merit-based incentive payment system; NDQA HEDIS, national committee for quality assurance healthcare effectiveness data and information set.
The P-value is associated with the chi-squared test assessing an association between the demographic variable and the 3 stratified groups.
Changes in Lifestyle Medicine Knowledge and Confidence
Change in Lifestyle Medicine Knowledge by Clinician Type.
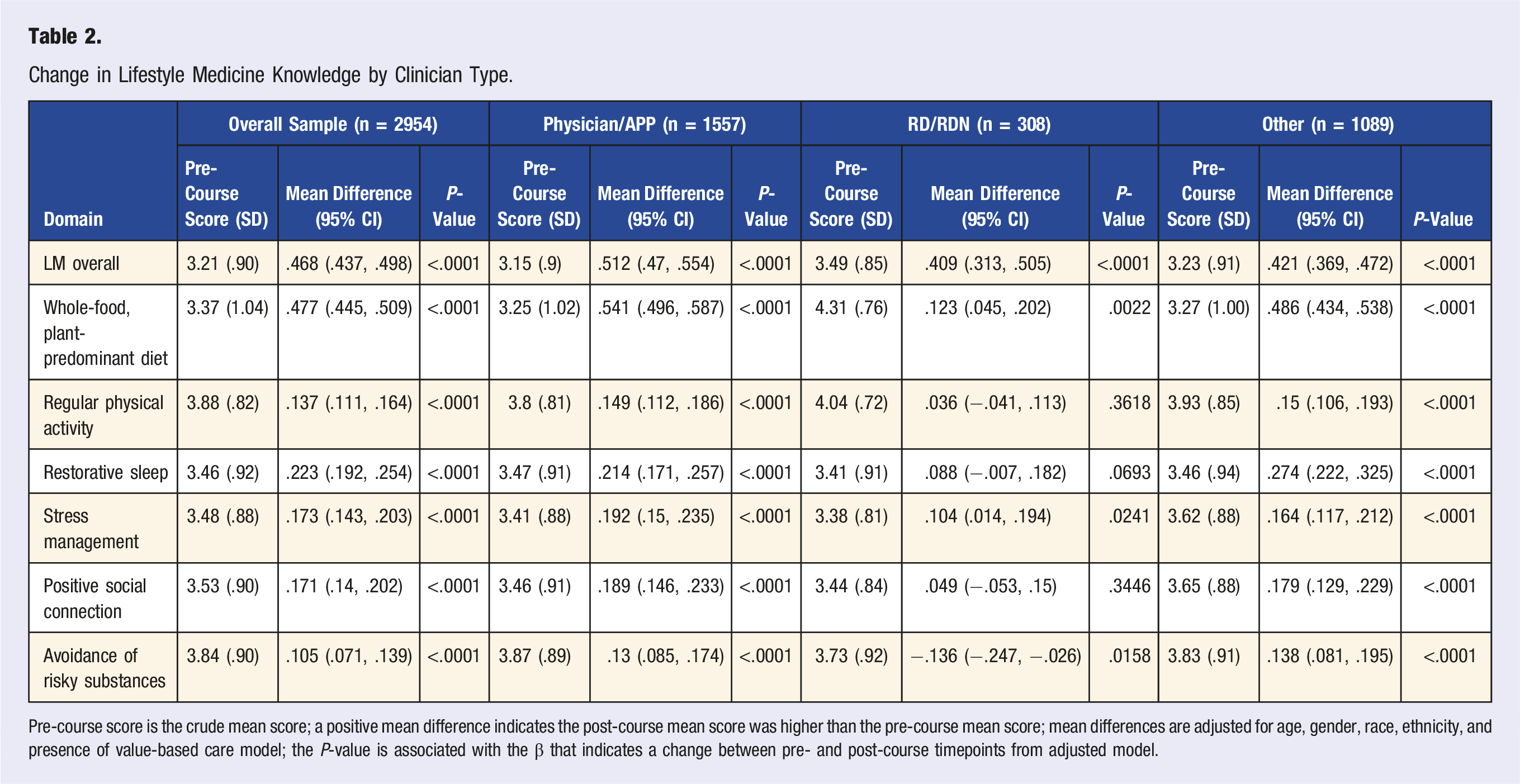
Pre-course score is the crude mean score; a positive mean difference indicates the post-course mean score was higher than the pre-course mean score; mean differences are adjusted for age, gender, race, ethnicity, and presence of value-based care model; the P-value is associated with the β that indicates a change between pre- and post-course timepoints from adjusted model.
Change in Lifestyle Medicine Confidence by Clinician Type.
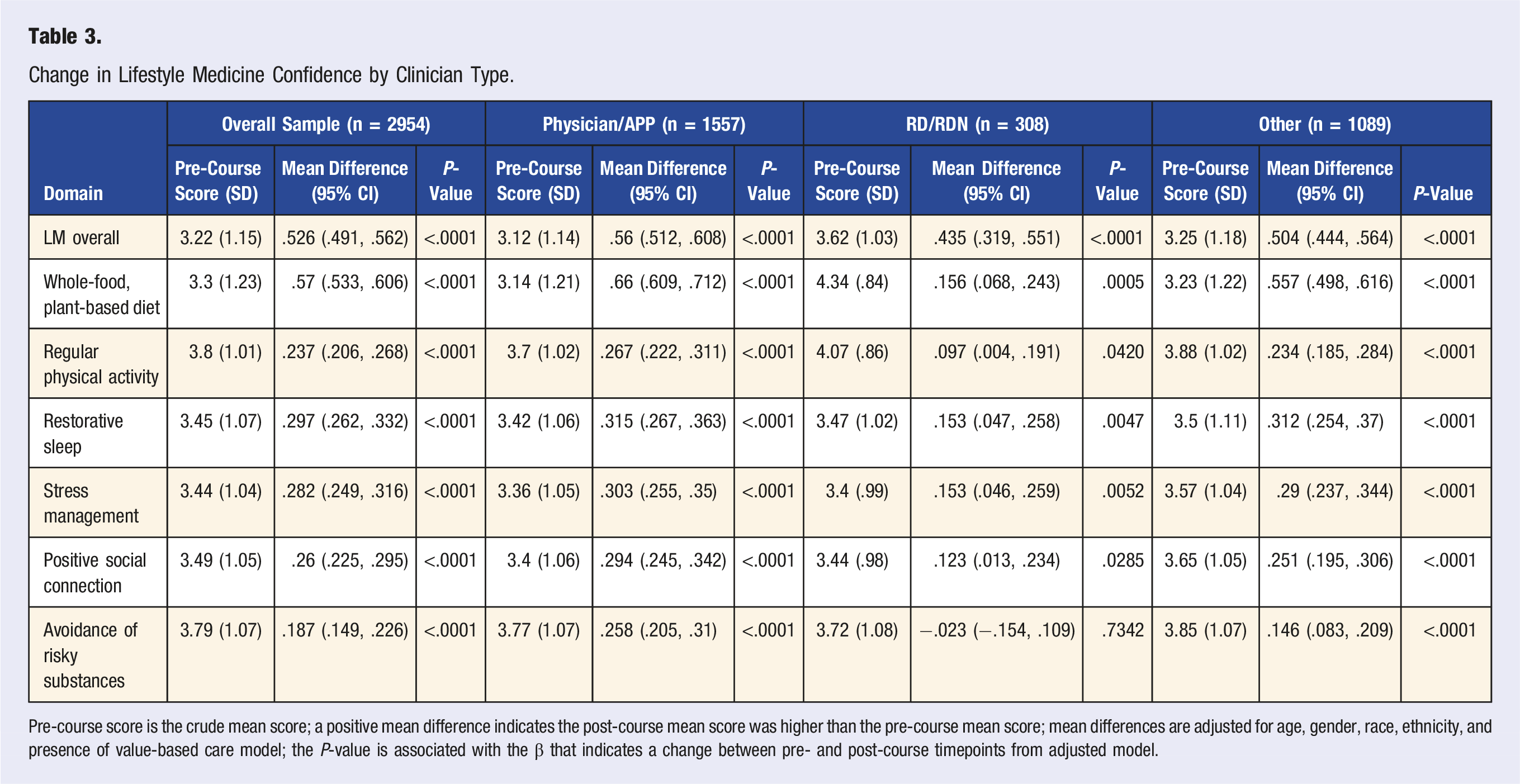
Pre-course score is the crude mean score; a positive mean difference indicates the post-course mean score was higher than the pre-course mean score; mean differences are adjusted for age, gender, race, ethnicity, and presence of value-based care model; the P-value is associated with the β that indicates a change between pre- and post-course timepoints from adjusted model.
Changes in Attitudes and Intentions Related to Lifestyle Medicine Practice
Change in Lifestyle Medicine Attitudes and Practice by Clinician Type.
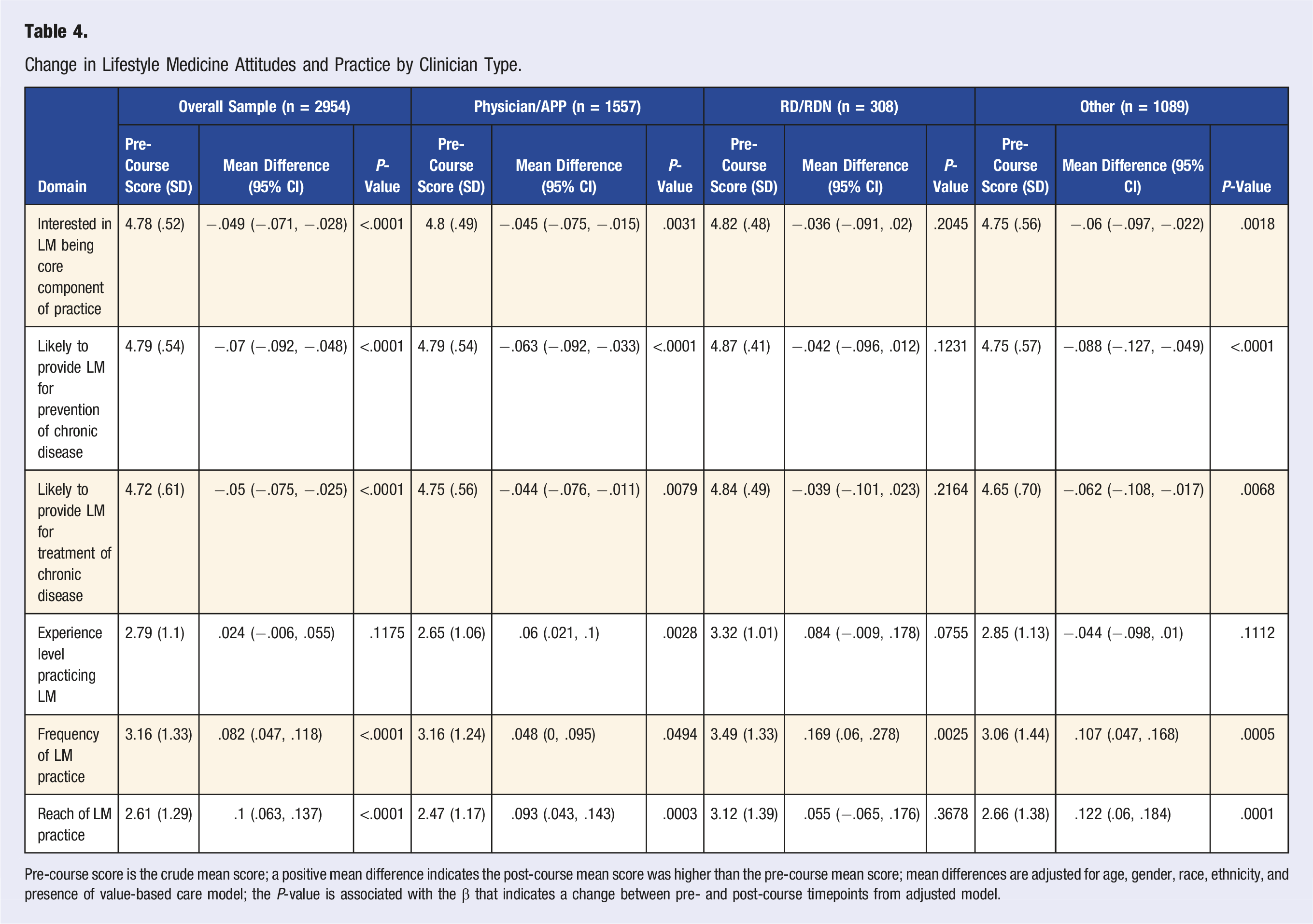
Pre-course score is the crude mean score; a positive mean difference indicates the post-course mean score was higher than the pre-course mean score; mean differences are adjusted for age, gender, race, ethnicity, and presence of value-based care model; the P-value is associated with the β that indicates a change between pre- and post-course timepoints from adjusted model.
Change in Lifestyle Medicine Attitudes Stratified by Baseline Clinician Attitude.
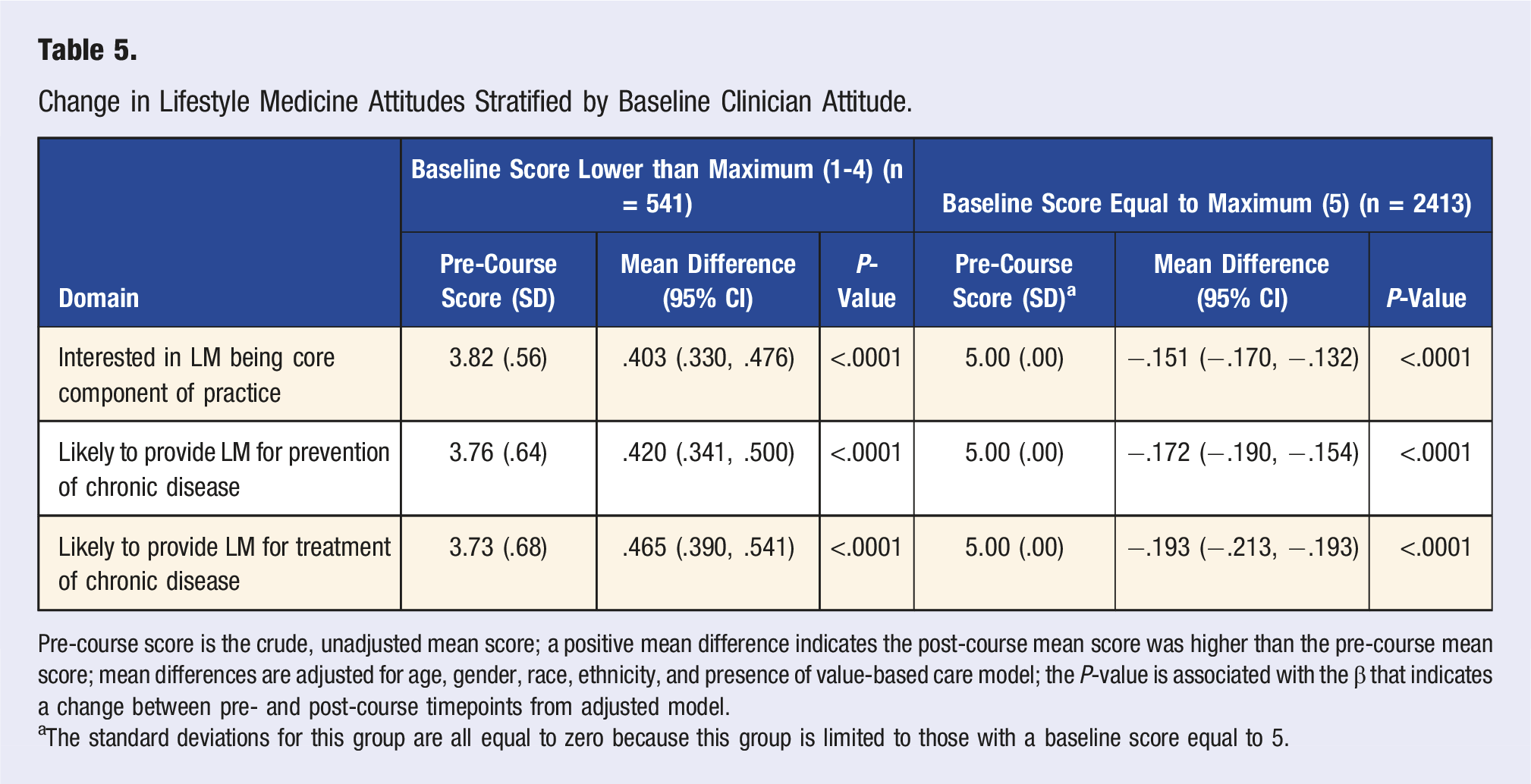
Pre-course score is the crude, unadjusted mean score; a positive mean difference indicates the post-course mean score was higher than the pre-course mean score; mean differences are adjusted for age, gender, race, ethnicity, and presence of value-based care model; the P-value is associated with the β that indicates a change between pre- and post-course timepoints from adjusted model.
aThe standard deviations for this group are all equal to zero because this group is limited to those with a baseline score equal to 5.
Changes in Lifestyle Medicine Practice
The overall sample reported statistically significantly increased scores in frequency (+.082, P < .0001) and reach (+.10, P < .0001) of LM practice (Table 4). Statistically significant improvements in reach were reported among physicians/AAPs and other clinicians, but not among registered dietitians. About a quarter (26.0%) of the overall sample reported to have substantial or advanced/extensive experience at baseline. This included 20.5% of physicians/APPs and 49.0% of registered dietitians.
Discussion
This study is the first to assess changes in LM knowledge, self-efficacy, attitudes, and practice following participation in the 5.5-h online Essentials course. 22 It is a scalable intervention, reaching about 35,000 healthcare professionals in 18 months, and is a promising approach to plant the seed of LM in the minds of practitioners and providers and motivate them to seek out additional training and expertise. The critical findings are that participants reported increased knowledge, confidence, and practice of LM after completing the Essentials course.
Most importantly, the overall clinician sample reported increased practice of LM after participation in just a 5.5-h online training course, suggesting that brief, online training is an accessible and cost-effective way to produce modest increases in the implementation of lifestyle medicine and health behavior change in medical practice. This aligns with other studies which have shown that online CME courses have a moderate influence on clinician practice behaviors.33,34 At baseline, interest in LM practice was generally high, but only about one quarter of the sample reported high levels of LM practice experience, suggesting a relatively motivated but inexperienced training audience.
Healthcare professionals participating in the course report statistically significant improvements in overall LM knowledge and confidence. This is consistent with other findings that brief trainings (<6 contact hours) can improve knowledge and skill in the short term.23,24 At baseline, registered dietitians reported slightly higher knowledge and confidence scores than the rest of the sample and subgroups, possibly indicating differences due to their previous professional training in nutrition. Similarly, physicians are known to receive less preparation in lifestyle change counseling (especially around dietary behaviors) than other health professionals, including registered dietitians. 35 This could indicate that physicians have greater potential benefit from participating in this training.
Surprisingly, overall participants reported a decreased interest in and intention to practice LM, contradicting the increase in self-reported LM practice behaviors. One possible explanation is that the wording of the questions, “How interested do you feel in using lifestyle intervention as a core component of medical practice?” suggested that LM would be the primary type of practice, rather than one of multiple practice approaches. Additionally, the baseline interest score was already high (4.78 out of 5 points), leaving little room for improvement, and selection bias due to individuals with an existing interest in LM was possible. This is supported by the stratified analysis showing that likelihood to practice scores increased among individuals who reported scores less than 5 at baseline. Finally, this survey did not assess environmental factors (e.g., billing challenges, business management, etc.) that are cited as barriers to LM adoption. 36 Environmental factors can impact clinician attitudes, and even augment the effect of training. 37 Thus, it is possible that if respondents developed new awareness of system-level challenges, their motivation and intention to practice LM could lessen, despite the increased knowledge and confidence. Additional exploration of these findings is warranted to understand if any of the above theories are supported. Further analysis may explore whether this trend is associated with certain individual (e.g., demographic or knowledge perception) or system-level (e.g., perception of leadership or environmental support) factors.
Although many of the outcomes assessed were statistically significant, they were often moderate in magnitude. This is not surprising due to the brief, introductory nature of the course. A systematic review of interventions to prepare medical students to counsel patients on physical activity yielded changes with magnitudes similar to what we observed. 24 Clinician training research suggests that education alone can often result in improvements in knowledge and confidence but has less of an impact on practice behaviors and patient outcomes. 23
These survey results highlight the ability of a free and widely scalable intervention to yield changes to healthcare professionals’ practice behaviors. The Essentials course is unique in its content and format. Lifestyle medicine is a relatively new field of practice that has had widely accepted core competencies for less than 5 years (originally released in 2022). 27 Consequently, there has not been a lot of research on LM education, and much of the literature is focused on medical student populations.38,39 Studies examining LM continuing education programs tend to include smaller (less than 200 participants) and more homogenous populations, often from one region or practice setting.15,25 For example, a study exploring changes in participant knowledge, confidence, and practice associated with LM education included 200 healthcare professionals in a major US city. 15 The Essentials program reaches a large and heterogenous national audience with the goal of educating 100,000 healthcare professionals. 32 Although the impacts are modest, the combined effect of these incremental changes on tens of thousands of healthcare professionals is notable.
Previous research on continuing medical education shows that potential impact is increased in the presence of supplementary training components—such as consultation, supervisor training, or booster trainings. 23 Measurement and assessment of additional supports is needed to determine the full extent of the effect of taking the course, in combination with analysis on supplementary training components.
There were several strengths and limitations of the methods used in this study. Some participants were self-referred to the training program, while others were referred or required to participate by their employer, which could differentially bias their attitudes and exposure towards LM. The longitudinal nature of the study design allows for individuals to serve as their own control; however, the inclusion of a control group could isolate the impact of this intervention and control for cultural and operational facilitators that increased practice behaviors beyond the influence of the course. Individual baseline factors (i.e., knowledge and interest) should also be assessed as a potential predictor of changes in knowledge, confidence, attitudes, and practice. The participant practice behaviors were self-reported and susceptible to response bias. Future research is needed to understand the lasting impacts of this training program and how they interface with individual and environmental factors, as well as how the experience differs between clinician types. A study investigating results at 8-12-months following program participation is planned to assess the sustained impact of the training.
Conclusion
The ACLM Essentials course is a cost-effective and scalable tool to deliver moderate increases in LM knowledge and practice to far-reaching and diverse groups of healthcare professionals. Health systems looking to increase LM implementation can promote this program as one component in a more comprehensive strategy that also addresses cultural and environmental barriers to LM practice. Additional research can advise on specific audience demographics that most benefit from the training, as well as supplemental activities that are most beneficial in different clinical settings.
Footnotes
Acknowledgments
We thank the ACLM Education Team for developing and administering this curriculum. We also thank all the individuals who participated in the training as well as the health system partners who aided in disseminating the CME opportunity.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KLS, AK, KF, PS, and MCK are employed by ACLM. MLA and JG receive consulting payments from ACLM.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the American College of Lifestyle Medicine.