
Abstract
Rural U.S. counties experience racial, geographic, and socioeconomic disparities in chronic diseases. Collaborations among stakeholders in rural areas are needed to make measurable changes in health care outcomes in South Carolina. The Chronic Conditions Care Collaborative (4C Collaborative) was developed to provide an opportunity for health care teams in medically underserved areas of South Carolina to convene to improve diabetes and heart disease outcomes. The 4C Collaborative was a quality improvement (QI) learning collaborative focused on the identification of patients with undiagnosed hypertension, team-based care through medication therapy management (MTM), and diabetes management. All QI work was approached through a health equity lens. Fifteen medical practices across two cohorts participated in the 4C Collaborative and gained access to more than 35 hours of educational content and guided action steps to create systemic changes specific to the needs of their patient population. Participation also conferred access to one-on-one technical assistance with faculty subject-matter experts. The activities within the 4C Collaborative allowed health care practices to identify areas of improvement within their practices and test improvement strategies through Plan-Do-Study-Act (PDSA) cycles. Best practices and lessons learned from learning collaborative participants were compiled into storyboards and presented during end of program celebrations.
“Barriers identified from the evaluation of the first and second cohorts of the 4C Collaborative included the lack of robust EHR systems, time constraints, staffing shortages, and competing priorities.”.
Introduction
The rural American South faces a disproportionate burden of diabetes and heart disease. 1 In South Carolina (SC), more than 13% of the adult population has diabetes, and nearly 35% of adults have prediabetes.2,3 Moreover, in 2019, it was reported that 34.3% of SC adults 18+ have been diagnosed by a health professional with hypertension. 3 These statewide statistics mask differences between rural and urban counties in the state. For example, 23.1% of adults have been diagnosed with diabetes in rural Williamsburg County, compared to 10.8% in urban Richland County. 3 Additionally, 2020 heart disease death rates were 369 per 100 000 in rural Marlboro County, compared to 148.7 per 100 000 in urban Greenville County. 4 About a quarter of South Carolinians reside in a rural county, where racial, geographic, and socioeconomic disparities in chronic disease are well-documented.5,6 Based on these statistics, collaborations among stakeholders in SC are needed to make measurable change in health care outcomes in rural communities. While changes in clinical outcomes can be challenging to attribute to population health initiatives, the use of quality improvement strategies have shown improvements in the management and control of chronic conditions when clinical care services are coupled with public health approaches. 7
Previous initiatives have demonstrated the significance of using learning collaboratives and other quality improvement (QI) strategies to address the prevention and control of chronic disease through data-driven action, clinical practice standardization, and the creation of community and clinical linkages. 7 Such initiatives in various states have modeled success in programs aimed at supporting federally qualified health centers (FQHCs) in using electronic health records (EHR) to identify and track patients with hypertension, as well as partnering with community pharmacists to identify patients with uncontrolled blood pressure and monitor patient medication adherence. 7 Moreover, a learning collaborative targeted toward primary care practices servicing the Medicaid-insured population in Ohio showed an increase in preventative education and screening rates for type 2 diabetes among women at high risk. 8
The Chronic Conditions Care Collaborative (4C Collaborative)
The 4C Collaborative was a QI learning collaborative developed to provide a space for health care teams (teams) from rural health centers (RHCs), FQHCs, free medical clinics, and other medical practices in SC to work together to improve patient health outcomes. The framework of the collaborative focused on identifying patients with undiagnosed hypertension, adopting team-based care through medication therapy management (MTM), and improving diabetes management. Work in all areas was approached through a health equity lens to explore relationships between biases and health disparities. Research has shown that clinicians’ racial biases can lead to differences in treatment and inequitable health outcomes among patients with diabetes and heart disease from marginalized populations.9,10 Under the guidance of subject-matter experts, who served as faculty, teams received technical assistance, guidance, and resources to assist them with testing and implementing change concepts. The 4C Collaborative had three goals: (1) Patient-centered care: Building strong primary care foundations to ensure all South Carolinians receive coordinated, patient-centered care. (2) Knowledge building: Providing resources and tools to health systems to support knowledge building and facilitate improvements in population health and health equity. (3) Quality improvement: Improving the quality, experience, and value of care.
Methods
4C Collaborative Framework
Medical practices that participated in the 4C Collaborative attended interactive learning sessions and webinars and were engaged in regular data collection activities. Moreover, the 4C Collaborative included one-on-one technical assistance in the form of guided action steps for systemic changes specific to the needs of each practices’ patient populations, access to faculty and other content experts, and more than 35 hours of educational content. The sections below describe the components of the collaborative’s framework in further detail.
Action Periods
The 4C Collaborative was organized into three, 4-month action periods titled: 1) Implicit Bias as a Lens for Quality Improvement and Identifying Undiagnosed Hypertension, 2) Embracing Team-Based Care and Integrating MTM to Promote Health Equity, and 3) Adopting Clinical Systems and Care Practices to Improve Diabetic Patient Outcomes. During action periods, teams tested and implemented change concepts in their medical practice and collected data to measure the impact of these changes. They were supported by conference calls, technical assistance site visits, e-learning modules, and web-based discussions that enabled them to share information and learn from experts and other participating practices. The aim was to build collaboration and support medical practices as they tested new ideas and strategies to be adopted into clinical policies, protocols, and procedures. The key elements utilized to ensure action periods ran smoothly were 1) a Change Package, 2) technical assistance, 3) PDSA (Plan, Do, Study, Act) cycles, and 4) an e-learning platform.
Change Package
The Change Package was a reference document that provided tools and resources to assist health care professionals with improving outcomes for patients with chronic conditions (e.g., heart disease and diabetes). It was a compilation of evidence-based strategies (i.e., “change concepts”) designed to help teams select and test changes that may lead to improved delivery of care and ultimately improved health outcomes. While there were many resources to choose from, teams were encouraged to select the most appropriate resources for their clinical setting. The Change Package included the following sections: 1) identifying undiagnosed hypertension, 2) MTM, 3) team-based care, and 4) clinical systems and care practices to improve diabetes care. Implicit bias underpinned all Change Package components (Figure 1). (1) Identifying undiagnosed hypertension (a) This section of the Change Package provided resources to assist health care teams in improving the identification of patients with undiagnosed hypertension through the adoption of policies, protocols, and procedures (see Supplemental Table 1 for an example chapter). These resources helped participants apply the Model for Improvement developed by Associates in Process Improvement to increase hypertension control, as well as understand how implicit bias affects undiagnosed hypertension.
11
(2) Medication Therapy Management (MTM) (a) MTM is a “spectrum of patient-centered, pharmacist-provided, collaborative services that focus on medication appropriateness, effectiveness, safety, and adherence with the goal of improving health outcomes.”12,13 This section promoted MTM between community pharmacists and physicians for the purposes of managing high blood pressure, high cholesterol, and lifestyle modification. (3) Team-based care (a) Team-based care has been shown to improve patient health outcomes and may reduce health care costs.14,15 The health care team may consist of physicians, nurses, pharmacists, and other health care professionals with a focus on preventing and treating disease. This section centered on integrating community-based pharmacists into medical practices to assist with the management of hypertension and high cholesterol. Key themes included a readiness assessment, resources for the development of collaborative practice and business agreements, measuring impact, and sustainability. Given that many RHCs, FQHCs, and free medical clinics have limited staffing capacity and do not often have pharmacists on staff, the Change Package encouraged collaborative practice and business agreements to support the engagement of community-based pharmacists in primary care settings. (4) Clinical systems and care practices to improve diabetes care (a) Despite advances in detection and treatment, the incidence of diabetes in the United States continues to rise,
16
especially among racial and ethnic minority populations.
17
This section of the Change Package focused on the adoption of clinical systems and care practices to improve health outcomes for people with diabetes, while also providing resources on how to address social factors that contribute to disparities in diabetes. Resources provided for addressing social factors included social determinants of health (SDOH) screening tools and community resource databases for referrals to meet patients’ social needs. (5) Implicit bias (a) Implicit bias was a foundational principle in the 4C Collaborative framework. Framework for the change package.
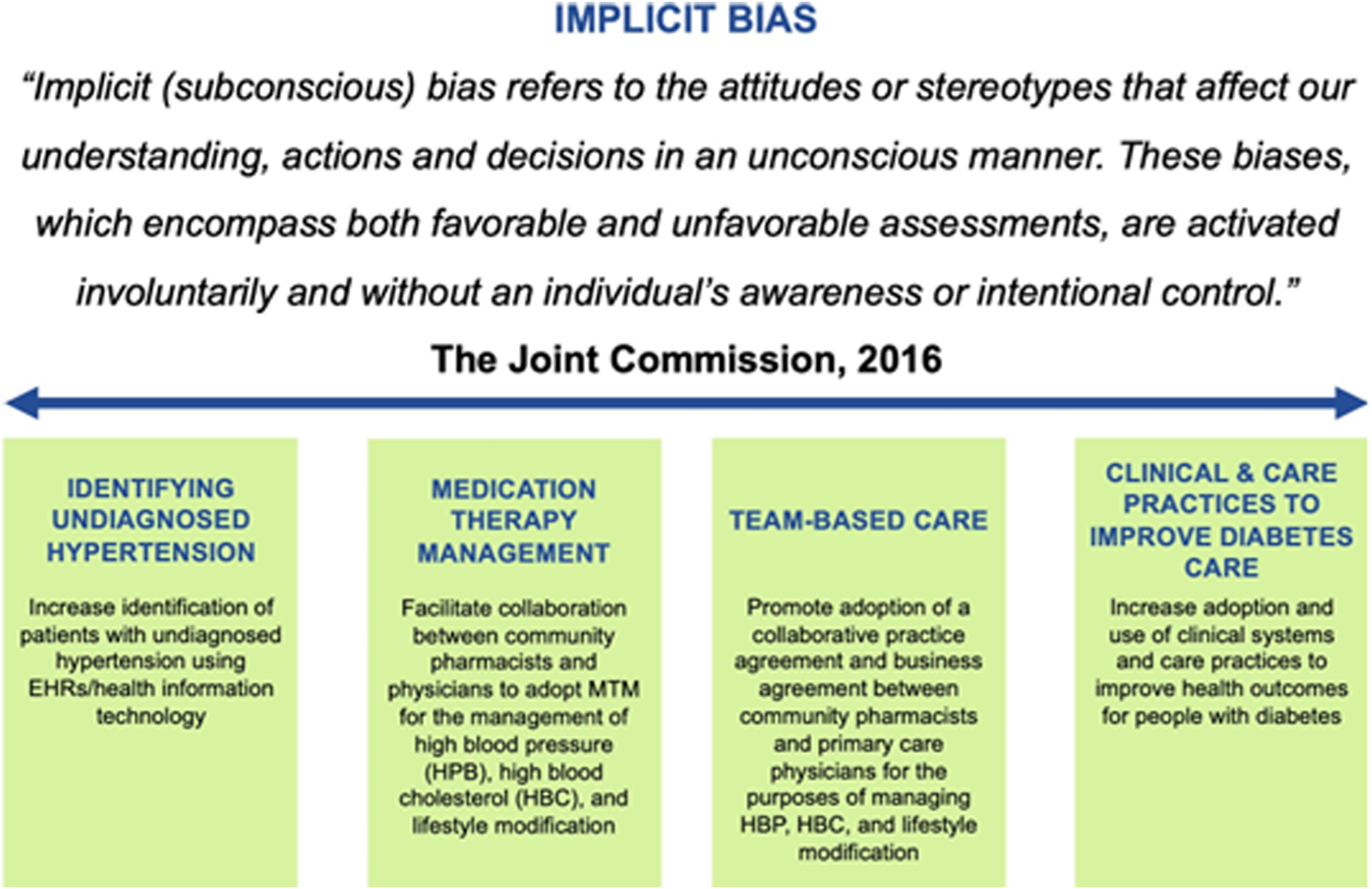
Implicit bias was defined as the influence of how information about an individual is processed and leads to an unintended bias in decision making.18,19 Implicit biases contribute to disparities in health care by shaping the behaviors of health care clinicians and other team members.18,20 Implicit bias was addressed in 4C Collaborative activities through the provision of resources and articles related to the impact of this construct on chronic disease management, as well as the incorporation of a webinar dedicated solely to implicit bias during the program schedule. By integrating this construct throughout its activities, the 4C Collaborative sought to address health disparities at the practice level.
PDSA Cycles
During the first and third action period of the 4C Collaborative, participating medical practices utilized PDSA cycles, a QI methodology for testing and implementing health care changes. 21 The four stages of the PDSA cycle are: (1) plan the change to be tested or implemented (Plan); (2) carry out the test or change on a small scale (Do); (3) collect and analyze data to measure results (Study); and (4) conduct the next change cycle or full implementation (i.e., develop a policy) (Act). Teams used PDSA cycles to test evidence-based strategies chosen from the Change Package. PDSA cycles enabled teams to test changes on a small scale and build on findings from each cycle.
E-Learning Platform
E-learning materials were accessible to participants through a course developed on the SC Area Health Education Consortium Learning Portal. 4C Collaborative faculty published learning modules to provide additional context to the work the teams conducted during each action period. Modules provided opportunities for participants to explore examples of how to plan and implement changes within their own practices. The 4C Collaborative course also included recordings of exclusive learning sessions and webinars and supplemental links to external resources and modules.
Technical Assistance
Technical assistance refers to the support, information, and resources provided by the Division of Diabetes and Heart Disease Management (Division), SC Office of Rural Health (SCORH), and SC Pharmacy Association (SCPhA) to facilitate learning and develop and implement action plans for policy and systems change. Practice (SCORH) and Clinical (Division) Transformation Consultants supported teams in using PDSA cycles to test, reflect, learn, and refine their change ideas. SCPhA conducted an electronic survey and virtual interviews with key health care personnel to assess each practice’s capacity and readiness to engage with a community-based pharmacist. For each participating team, SCPhA used follow-up interviews and results of the assessment to develop individual action plans outlining the process of integrating a community-based pharmacist into primary care using resources from the Change Package. These plans addressed a range of topics including the medical practices’ motivation, capacity, and readiness to collaborate with a community pharmacist to enhance MTM or engage community pharmacists in non-dispensing roles.
Monitoring and Reporting
The 4C Collaborative was designed to help facilitate the implementation of several strategies with the goal of improving the management of hypertension, hyperlipidemia, and diabetes among participating medical practices. Deliverables varied by each action period, but primarily included submitting documentation of PDSA cycles and bi-annual reports. At the end of the action periods, each team submitted written documentation (e.g., policies, protocols, or workflows) demonstrating the adoption of an evidence-based practice that resulted from the PDSA cycles. For practices that were successful in engaging with a community-based pharmacist, deliverables included the submission of a collaborative practice and/or business agreement.
Recruitment of Medical Practices to Participate in the 4C Collaborative
Two cohorts of medical practices were engaged in the 4C Collaborative between August 2020 and July 2022. Medical practices that opted to participate in the 4C Collaborative formed teams and were engaged during an 11-month duration.
Cohort 1 Recruitment
For Cohort 1, SCORH was responsible for identifying and recruiting potential RHCs to participate, as outlined in their contract with the Division. The identified medical practices were emailed an electronic baseline assessment, which was used to determine their capacity to implement the 4C Collaborative strategies. Utilizing the results of the baseline assessment and building upon SCORH’s knowledge of these medical practices’ capabilities and capacities, SCORH identified practices that were most ready to participate and invited them to join the 4C Collaborative. Upon joining the Collaborative, medical practices were expected to implement all four strategies within an 11-month timeframe.
Cohort 2 Recruitment
Applying lessons learned from Cohort 1, the recruitment of medical practices for participation in Cohort 2 took an alternative approach. To recruit medical practices to participate, the Division promoted the collaborative via partner networks and interviewed interested practices to learn about their current policies, procedures, and/or programs for patients with cardiovascular disease and/or diabetes. Moreover, the Division developed an expectations agreement which outlined the timeline of the collaborative, the deliverables, documentation required, a compensation overview by activity, and program benefits. To participate in the collaborative, interested practices were required to sign the agreement, confirming that they understood the requirements of the collaborative and were committed to doing the work as outlined. Additionally, during Cohort 2, interested practices were able to select which action periods they wanted to participate in to ensure buy-in on strategies that best aligned with their practice goals. Lastly, at the start of Cohort 2, medical practices were provided with implementation plans outlining the strategies and timeline to complete the associated deliverables.
Results
A total of 15 medical practices participated in the 4C Collaborative across the 2 cohorts, with 6 participating in Cohort 1 and 9 participating in Cohort 2. The results below highlight attendance at program events, the PDSA cycles conducted among participating practices, summaries of resulting documented processes submitted for hypertension and diabetes care, and relationships created between participating practices and community-based pharmacists.
Cohort 1
Action Period 1: Implicit Bias as a Lens for Quality Improvement and Identifying Undiagnosed Hypertension
During the first action period, all participating practices attended a learning session entitled “Implicit Bias as a Lens for Quality Improvement and Identifying Undiagnosed Hypertension.” All practices engaged in PDSA cycles during this action period that included designating a chronic disease champion in the practice and implementing policies to measure and address blood pressure at every patient encounter (including during lab-only visits). Implementation of and results from PDSA cycles varied by practice; however, many practices noted conducting outreach to patients recently seen that had an elevated blood pressure but were not diagnosed with hypertension. Patients were offered blood pressure logs and prescriptions for blood pressure monitors. Practices reported not identifying many patients with undiagnosed hypertension and received mixed reviews from patients regarding the additional follow-up calls.
All six practices submitted documented processes (e.g., policy, protocol, or workflow) for identifying undiagnosed hypertension. The practices highlighted the use of a second blood pressure screening during the visit if the first screening was elevated; patient education on lifestyle changes and monitoring their blood pressure at home; follow-up appointments to rescreen and review blood pressure logs; and discussion of medication if hypertension was diagnosed.
Action Period 2: Embracing Team-Based Care and Integrating MTM to Promote Health Equity
During the second action period, five RHCs attended a learning session on promoting health equity through team-based care and MTM. Only one medical practice was successful with integrating a community-based pharmacist into their practice through the development and execution of a collaborative practice agreement. This pharmacist conducted 92 visits with 78 unique patients. Most of patients seen had hypertension or hyperlipidemia (82%), and about 20% had diabetes. The pharmacist conducted visits for chronic care management and was able to solve 59 out of the 65 medication related problems she found during her visits. Moreover, she was able to either administer or schedule 47% of the immunizations patients needed. The pharmacist generated $3732.09 in revenue during the project, which equated to 39% of her expense (hourly rate was set at $62.50; total cost for the pharmacist was $9500.00). At the end of this action period, this RHC hired two full-time pharmacists.
Action Period 3: Adopting Clinical Systems to Improve Diabetic Patient Outcomes
During the third and final action period, three practices attended the learning session on the adoption of clinical systems and care practices to improve diabetic patient outcomes.
Following the learning session, four practices conducted PDSA cycles testing change ideas that included designating a chronic disease champion in the practice to address diabetes care; adopting clinical policies and procedures for diabetes care; and implementing a new registry of patients with and at risk for diabetes using the EHR. Implementation of the change ideas and results of the PDSA cycles varied by practice. Nurses and pharmacists designated as champions were assigned tasks such as collaborating with providers to promote diabetes policies and procedures, providing input and leadership for the monitoring and evaluation of diabetes care, and supporting patients suffering from complications of diabetes.
All six practices submitted a documented process (e.g., policy, protocol, or workflow) for patients with diabetes. Practices updated existing diabetes policies to include initiation of care planning, improve patient education regarding lifestyle modifications and self-management tools, and referrals to accredited Diabetes Self-Management Education and Support (DSMES) programs. Additionally, most practices showed documentation of the use of standard lab orders and procedures for caring for patients with diabetes. Practices noted there would be continuous training for staff regarding diabetes-related quality measures, as well as continued use of huddle tickets and the EHR to identify patients with diabetes.
Cohort 2
Action Period 1: Implicit Bias as Lens for Quality Improvement and Identifying Undiagnosed Hypertension
Seven of the nine practices in this cohort chose to participate in this action period. All seven attended the learning session and submitted a PDSA cycle. Change ideas tested in the PDSA cycles included creating a nurse blood pressure visit; ensuring standardization of blood pressure screenings; creating and distributing a blood pressure questionnaire for patients with elevated blood pressure to determine root causes; piloting a remote patient monitoring program; and establishing clinical criteria to define potential undiagnosed hypertension. Testing of the change ideas were unique to each practice and results included acknowledging missed hypertension diagnoses and standardizing blood pressure screening protocols among free medical clinic volunteers.
Following the PDSA cycles, all seven practices submitted a documented process (e.g., policy, protocol, or workflow) for identifying patients with undiagnosed hypertension. Processes included standards of care for the detection and management of hypertension, defining categories of elevated blood pressure, scheduling follow-up appointments to rescreen blood pressure, and referral to external programs for management of high blood pressure (e.g., YMCA blood pressure self-monitoring program).
Action Period 2: Embracing Team-Based Care and Integrating MTM to Promote Health Equity
Two practices opted to participate in this action period. Of those, both attended the learning session, and one was able to develop a limited scope collaborative practice agreement with a community-based pharmacist, that resulted in the pharmacist working 26 eight-hour days and conducting 89 chronic care management visits. Through their visits with the pharmacist, 22 patients received medication to prevent a fracture and six patients received self-monitoring education for hypertension or diabetes. Additionally, the pharmacist assisted with medication management, including making 15 therapeutic substitutions to lower patient cost, adjusting dosage for six patients to improve efficacy, and conducting 22 medication reconciliations. This practice continued to collaborate with the pharmacist on immunization and remote physiologic monitoring projects after this action period ended.
Action Period 3: Adopting Clinical Systems to Improve Diabetic Patient Outcomes
All nine practices chose to participate in this action period. Eight of the nine practices attended the learning session regarding the adoption of clinical systems and care practices to improve diabetic patient outcomes. Following the learning session, eight practices conducted PDSA cycles testing change ideas that included updating and training staff on diabetes standing orders; implementing a diabetes circuit training (DCT) for diabetic patients; and conducting outreach to patients with an A1c > 9 for chronic care management. Practices highlighted results from PDSA cycles that included updating clinical policies and procedures to include referrals to a DSMES program, increasing to the number of routine diabetic foot exams, extending responsibilities of diabetes management to internal pharmacists through the addition of team-based care protocols, decreasing A1c among patients participating in the DCT, and increasing SDOH screenings among diabetic patients conducted by community health workers.
Following the submission of PDSA cycles, seven practices submitted a documented process (e.g., policy, protocol, or workflow) for diabetes. Many practices provided documentation of the use of diabetic standards of care (e.g., lab orders, procedures). Others submitted protocols related to their test of change. For example, one practice piloted the use of an internal pharmacist to titrate diabetic medication and submitted the workflow developed among the pharmacist, diabetes educator, and medical director outlining specific steps for such titration.
Discussion
Deliverables
During review of the submitted deliverables, it was acknowledged that not all change ideas tested during PDSA cycles were from the Change Package; however, participating practices had autonomy in implementing additional evidence-based strategies that were of interest. During Cohort 1, it was found that there was often a disconnect between the PDSA cycles conducted and the resulting documented processes; however, during Cohort 2, this was found to be less common and improvements in deliverables were observed. Improved quality of the deliverables could be related to a variety of factors, including, but not limited to, the hiring of an internal Clinical Transformation Consultant within the Division to improve communication with practices and SCORH; outlining explicit expectations for each practice; changing the approach to allow practices to choose the action periods they wanted to participate in; and practices becoming less burdened by the COVID-19 pandemic.
Barriers and Facilitators
Barriers identified from the evaluation of the first and second cohorts of the 4C Collaborative included the lack of robust EHR systems, time constraints, staffing shortages, and competing priorities. Throughout the collaborative, archaic EHR systems, or the lack an EHR, led to many barriers related to retrieving data from the practices to support their quality improvement work. A few practices noted manual extraction of data from paper chart systems as a barrier. During Cohort 1, the COVID-19 pandemic was continuously cited as a practice-level barrier, as many found themselves stretched thin with regard to finding available staff and time to test and implement change ideas. Additionally, many participating practices were involved in hosting COVID-19 vaccination clinics, which pulled time away from implementing the work of the 4C Collaborative. Staff shortages were identified as another barrier, with the pandemic only exacerbating the personnel shortage. Moreover, time between action periods was noted as a barrier, with practices highlighting that the time allotted to conduct the PDSA cycle was too short and that it was difficult to see impact on the patient population over a short period of time.
Although there were many barriers, practices notated benefits to their participation in the collaborative, including support received from the 4C Collaborative team to conduct quality improvement projects and having dedicated time set aside to address specific chronic disease burdens. Moreover, practices that participated in Cohort 2 notated that a facilitator to this work was the incentive payments tied to deliverables that helped with the obligation to keep project performance on task.
Suggestions for Future Implementation
Based on the findings from the evaluation of the 4C Collaborative, suggestions for future iterations of chronic disease learning collaboratives can be provided. For example, when implementing a learning collaborative for medical practices at the state level (e.g., within a state health agency), it is recommended that practitioners investigate which additional departments, programs, or partners are currently working with potential learning collaborative practices to avoid competing priorities and promote synergy. Moreover, there may be advantages to working with a group of practices over a longer period to ensure adequate time for implementing quality improvement projects at the practice level. Chronic disease learning collaboratives should also establish expectations for what addressing health disparities or implicit bias would look like. Health equity audits, which examine how equitably resources are allocated to different racial/ethnic groups based on their health needs, show some promise for establishing baseline measures and tracking progress toward reducing health disparities. 22 Lastly, a learning collaborative would benefit from having a subject-matter expert on the internal team when it comes to engaging medical practices in quality improvement work. A clinical subject-matter expert may be able to assist with shaping reasonable expectations for participating partners and medical practices at the start of the collaborative, which may better clarify what final deliverables should include and improve communication.
Conclusions
The activities within the 4C Collaborative allowed participating medical practices to identify areas of improvement within their practices to better serve their patient populations. Best practices and lessons learned from learning collaborative participants were compiled into storyboards and presented during end of program celebrations. Through the improvement of documented processes for the identification and management of chronic disease, as well as collaboration between members of the health care team, poor health outcomes can be ameliorated, and patients in underserved communities can obtain access to better quality care.
Supplemental Material
Supplemental Material - The Chronic Conditions Care Collaborative (4C Collaborative): A Platform for Improving Diabetes and Heart Disease Outcomes in Rural South Carolina
Supplemental Material for The Chronic Conditions Care Collaborative (4C Collaborative): A Platform for Improving Diabetes and Heart Disease Outcomes in Rural South Carolina by Brittney Grant, MPH, Jennifer Mandelbaum, PhD, MPH, Khristian Curry, MPH, CHES, Kristian Myers, MPH, CHES, Michele James, MSW, Courtney Brightharp, DHSc, MPH, Shauna Hicks, MHS, CHES in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors thank the following organizations for their contribution to the development of the 4C Collaborative: Carolinas & Georgia Chapter American Society of Hypertension, Inc.; J. Renee Consulting LLC; USC/Prisma Family Medicine Department, USC School of Medicine—Columbia Campus; South Carolina Office of Rural Health; South Carolina Pharmacy Association; and South Carolina AHEC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work reported in this publication was supported by the Centers for Disease Control and Prevention (CDC) (DP18-1817).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.