
Abstract
Chronic wounds impact 4.5% of the US population, necessitating a comprehensive understanding of their types and underlying mechanisms. Diabetic foot ulcers (DFUs), prevalent in 25% of individuals with diabetes, contribute significantly to lower limb amputations. The pathophysiology involves neuropathy, peripheral arterial disease, impaired immunity, glycemic control, and mechanical stress. Lifestyle medicine emerges as a pivotal aspect of care, offering both prevention and treatment by integrating plant-predominant nutrition, physical activity, stress management, avoidance of harmful substances, restful sleep, and social connectedness. These interventions impact gene interactions, immune function, and tissue regeneration, playing a crucial role in chronic wound management. The standard of care involves a multidisciplinary approach, emphasizing infection and vascular management, pressure offloading, conducive wound healing environments, and lifestyle adjustments. As diabetes prevalence rises, a proactive integration of lifestyle interventions is crucial, offering a promising avenue to alleviate the growing healthcare burden associated with chronic wounds.
“Lifestyle-associated risk factors underscore the importance of integrating local wound care with lifestyle interventions.”
Introduction
Chronic wounds pose a significant burden on the healthcare system, affecting approximately 2.5% of the United States population.1-3 This prevalence underscores the urgent need for a comprehensive understanding of various chronic wound types, their underlying etiologies, and intricate pathophysiological mechanisms. This manuscript focuses on diabetic foot ulcers (DFUs) as a prominent subset of chronic wounds, exploring their unique characteristics and contributing factors.
Diabetic foot ulcers, a common complication in individuals with diabetes, exemplify the intricate interplay of factors leading to chronic wound formation. Diabetes mellitus, affecting over 34 million Americans according to the Centers for Disease Control and Prevention (CDC), is a major predisposing factor for DFUs. 4 Elevated blood glucose levels contribute to peripheral neuropathy and impaired blood circulation, diminishing pain sensation and reducing the body’s ability to initiate an appropriate inflammatory response crucial for wound healing.
Types and Etiologies of Chronic Wounds
Chronic wounds can have mixed etiologies, with the most common types being arterial, venous, neuropathic, and pressure ulcers.
Arterial ulcers may originate from poorly healing trauma due to poor circulation. Venous ulcers often result from ruptured skin or varicose veins, caused by increased venous pressure. Neuropathic ulcers typically develop at pressure points, such as the plantar surface of the foot, due to repetitive micro-traumas. They form on high-pressure areas where continuous pressure diminishes circulation, and increased moisture sets off the ulceration process. Diabetes is the primary cause of neuropathy, and while diabetic ulcers are commonly termed neuropathic ulcers, it’s important to note that not all neuropathic ulcers are associated with diabetes. 5
Chronic wounds, including arterial, venous, and diabetic ulcers, afflict a significant portion of the population. Lifestyle-associated risk factors, such as age, diabetes, peripheral arterial disease (PAD), immobility, poor nutrition, and smoking, highlight the importance of combining local wound care with lifestyle interventions for optimal wound healing and prevention of recurrence. 6
Pathophysiology of Diabetic Foot Ulcers (DFUs)
Twenty-five percent of individuals with diabetes develop DFUs, leading to non-traumatic amputations. DFUs affect 1.5% of the US population, resulting in 73,000 lower limb amputations annually.7-9 The multifactorial pathophysiology includes:
Neuropathy
Diabetic neuropathy affects both sensory and motor nerves. Motor deficit can cause changes in foot structure, leading to foot deformities that can increase the risk of developing ulcers. A patient with a sensory deficit may present a mysterious skin mark on the foot, resulting from a foreign object in the shoe that the patient cannot feel (Figure 1). Diabetic neuropathy. (A). A mysterious skin mark on a patient’s heel. (B). A foreign object inside the patient’s shoe.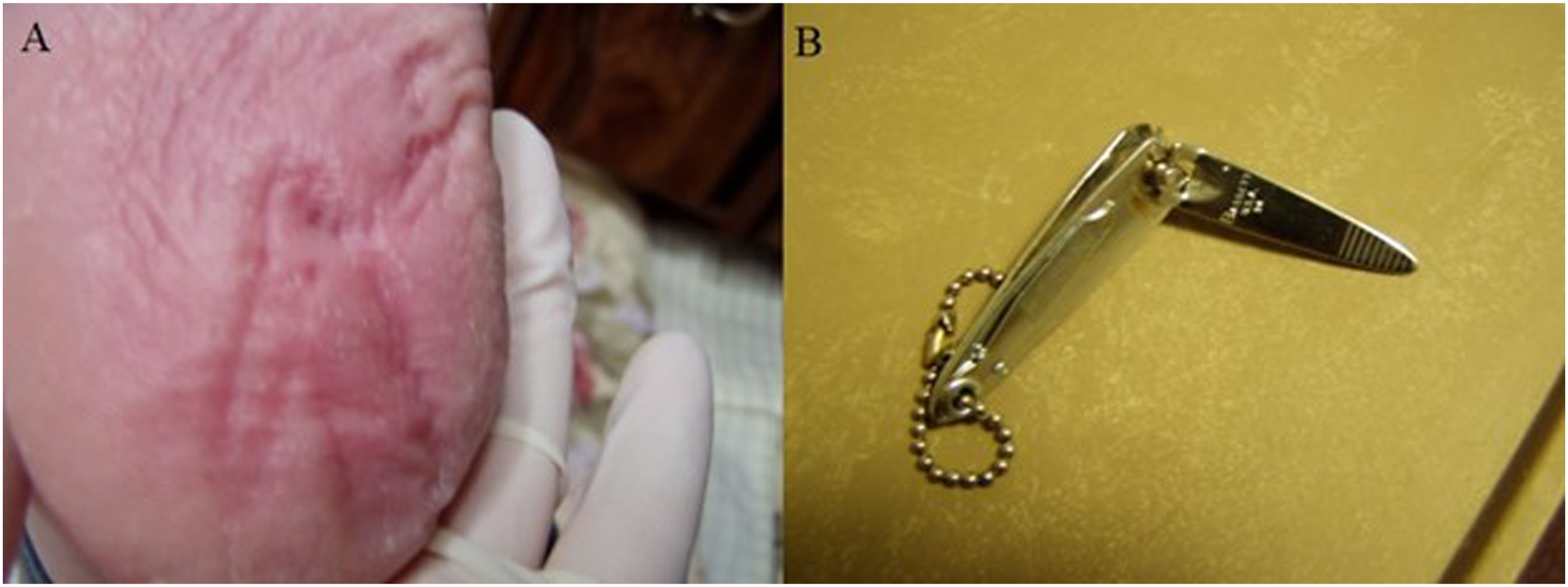
Peripheral Arterial Disease
PAD reduces blood supplies to the lower limbs, impairs wound healing, increases the risk of infection, and reduces wound healing capability.
Impaired Immunity
Diabetes is associated with impaired immunity, which contributes to the development of infection in the ulcerated tissue.
Glycemic control
Poor glycemic control can impair wound healing and increase the risk of infection. High blood glucose levels can also promote the formation of advanced glycation end products (AGEs), which can damage blood vessels and soft tissue and impair wound healing.
Mechanical stress
Repetitive mechanical stress, such as pressure and shear forces, can lead to the breakdown of skin and underlying tissues.
Standard of Care in Wound Management
Managing chronic wounds necessitates a comprehensive approach, including infection and vascular diagnosis and management, pressure offloading, conducive wound healing environment promotion, regular re-evaluation, systemic comorbidity management, and lifestyle adjustments.10,11
Components of an Effective Wound Management Plan
An effective wound management plan integrates local wound care, offloading, and lifestyle interventions. Local wound care includes infection assessment, vascular status evaluation, ulcer debridement, and appropriate wound dressing. Offloading, often associated with DFUs, involves mitigating edema-induced pressure on soft tissue. Lifestyle intervention addresses immunity, circulation, nutrient provision, and systemic comorbidities, integral to holistic wound management.
Lifestyle Medicine in Chronic Wound Healing
Lifestyle interventions play a pivotal role in chronic wound management, with focus on addressing the six pillars of a healthy lifestyle: plant-predominant nutrition, physical activity, stress management, avoidance of harmful substances, restful sleep, and social connectedness. These pillars are assessed and intervened upon to optimize patient outcomes in wound care.
Plant-Predominant Nutrition
The wound healing process involves a cascade of gene interactions. Much research has demonstrated that nutrition can have a broad effect on epigenetics. Fibers in the plant-predominant nutrition benefit the gastroenteric microbiome, which is associated with immunity. Micronutrients, such as vitamin C, zinc and copper, are essential in proper processing of collagen synthesis.12-15
Physical Activity
Physical activity has numerous benefits for overall health, and it can also positively influence the process of wound healing. Most profoundly, physical activities can improve circulation, tissue oxygenation, and tissue regeneration.16-20 Being active can improve other pillars of a healthy lifestyle, such reduced stress and improved sleep quality.21,22
A patient with a diabetic foot ulcer may require activities that do not aggravate the ulceration and the ulcer frequently needs to be offloaded (Figure 2).23-27 Diabetic foot ulcer. (A). A diabetic foot ulcer on the plantar surface of lateral right foot. (B). Simple offloading the ulcer with felt.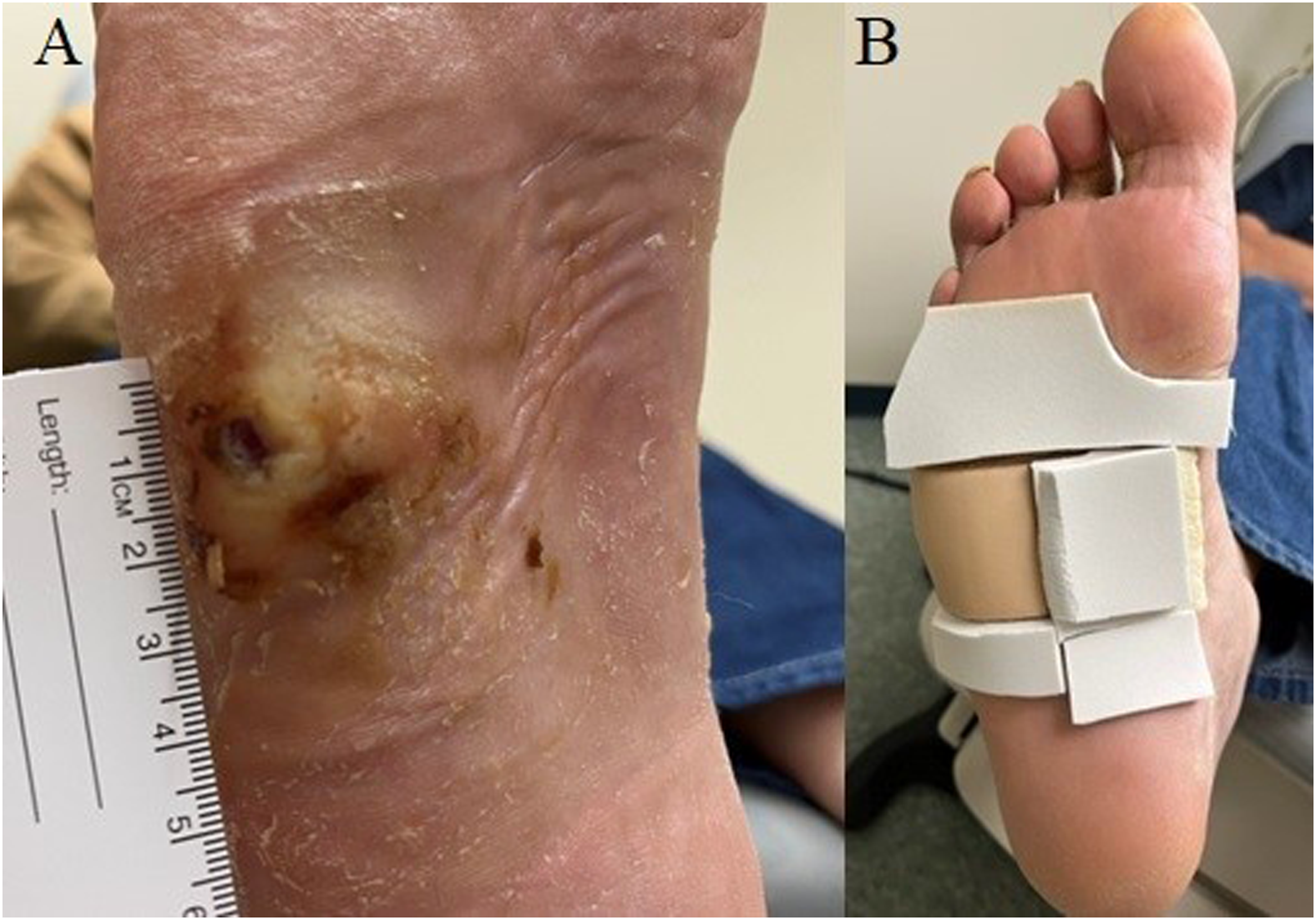
Stress Management
Stress is best associated with an increased level of cortisol that causes hypertension and reduced immunity. Cortisol is also a catabolic steroid that degrades tissues which is counterproductive in wound healing.28-34 Eliminating stress related physiological changes would benefit wound healing with improved immunity, reduced soft tissue degradation, and improved circulation. Stress can be managed with various modalities based on the sources of stress and personal preferences, including meditation, physical activities, and music.
Avoidance of Harmful Substances
Cigarette smoking has been shown to change skin properties, including reduced elasticity, increased thickness of epidermis and dermis, and reduced density of epidermis and dermis. Not surprisingly, smoking increases risks of necrosis, healing delay, surgical site infection, and wound complications. These result from the physiological effects of enhanced extra cellular matrix degradation, increased vasoconstriction and platelet adhesiveness, decreased proliferation of red blood cells, fibroblasts and macrophages, and decreased oxygen transport.35-42
Consumption of alcoholic beverages compromises wound healing by increasing inflammatory mediators, decreasing collagen fibers, and increasing risks of infection. Smoking cessation has been shown to reduce post-operative complications and inflammations.39,43,44
Restful Sleep
The benefits of sleep include improved mental wellness, reduced food craving, and enhanced immunity. Most importantly, tissue regeneration occurs in the deep sleep stages of the sleep cycle, which greatly benefits the wound healing process.45-48
Social Connectedness
Loneliness and social isolation have been associated with development of diabetes and cancer, increased overall mortality, and decreased cardiovascular health and mental health.49,50 Animal studies have shown that animals in isolation healed slower than those not isolated. A possible explanation is that isolation reduces immunity.51-53
Case Study
A 54-year-old white male presented to the office for diabetic foot ulcers. Patient stated that the ulcers occurred about one year ago but had not been taken care of for six months. The last treatment consisted of daily dressing changes without regular debridement. He was provided with arch supports to offload the ulcers. However, the insoles were not supportive to sufficiently offload the ulcers. Lifestyle was not previously assessed as part of his wound management. He just started a job in town. The patient stated that his diabetes was well controlled, and the ulcers persisted simply due to loss of job and health insurance. He denied past medical history except diabetes and did not recall a complete list of medications and dosages.
Lifestyle Inventory
Nutrition
Patient followed a standard American diet with lots of sugar sweetened beverages at work.
Physical Activity
Patient liked to garden, lived on an acreage home, and walked constantly at work.
Sleep
Patient could fall asleep quickly and did not feel tired during daytime.
Social connectedness: Patient had a close family network. He just lost his father-in-law.
Stress
Patient was experiencing grief from losing his father-in-law. He obtained the current job after being laid off for six months. He was the sole financial support at home since his wife stayed home to care for two sons with autism.
Harmful Substances
Patient did not use tobacco products and seldom consumed alcoholic beverages.
Physical Exam
Comprehensive Foot Exam
Dorsalis pedis and posterior tibial pulses were decreased, bilaterally. Mild non-pitting edema was noted on foot and ankle, bilaterally. Skin color was red and temperature was warm. Protective sensation as tested by filament was absent, bilaterally. Sharp-dull discriminatory sensation was absent, bilaterally. Proprioception on hallux was absent, bilaterally. Achilles tendon reflex was absent, bilaterally.
Ulcers
One ulcer was noted on the plantar surface of lateral right midfoot and was classified as Wagner’s grade 2 that is defined as a deep ulcer extended to ligament, tendon, joint capsule, bone, or deep fascia without abscess or osteomyelitis. 8 It was measured 3.0 cm × 3.0 cm × 0.2 cm. The second ulcer was observed on the plantar surface of the left hallux, which was measured 1.0 cm × 1.0 cm × 0.2 cm and was classified as Wagner’s 2.
Treatment and Management
Wound Management
Wound cultures were performed on both ulcers at the initial visit and found to be a mixture of Staphylococcus aureus, Streptococcus agalactiae, Baceteroides spp., Peptostreptococcus anaerobius, and Pseudomonas aeruginosa. The patient was placed on Amoxicillin 875 mg twice daily for 5 days. Ulcers were debrided and covered with hydrofiber and foam. Ulcers were reduced in size immediately. However, the size started to fluctuate after a few visits.
Lifestyle Management
The patient’s BMI was 27.6. He stated that he loved greens and could increase vegetable intake. He would eliminate sugar sweetened beverages at work. He was active at work and would be mindful not to aggravate the ulcers.
Upon further questioning when ulcers failed to respond, the patient revealed that due to his financial responsibility and his regaining employment after being jobless for six months, he was reluctant to ask for job accommodation or adjustments.
After a few months of treatments, the patient transferred his general medical care to our practice. His medications included Aspirin, Amlodipine, Losartan, Atorvastatin, Ozempic, Tresiba, and Novolog. The laboratory tests showed a fasting glucose of 269, HbA1C 7.8, Vitamin D 12.6, BUN 42, creatinine 1.50, eGFR 55, and potassium 5.9. Upon seeing the results, the patient’s first comment was that he really needed to eliminate, not just reduce, those beverages. Additionally, the patient did not know the names and dosages of his medications. What he remembered and brought to the clinic did not match the pharmacy record. This further revealed the status of his diabetes management.
The sizes of the ulcers continue to fluctuate. The patient further disclosed that he had had marital issues. He would focus discussions with his wife on her and the family, instead of him. While being asked whether his wife knew how severe his ulcers or renal functions were, he indicated that she did not.
In the following months, his marital status worsened. The patient had frequent unexpected events that increased walking or pressure on his feet and could not completely follow a plant-predominant diet. Wound sizes continue to fluctuate and wound cultures were taken twice to rule out infection. The 6-month follow up laboratory tests showed a fasting glucose of 118, HbA1c 8.0, Vitamin D 10.7, creatinine 2.02, eGFR 38, and potassium 5.2. The patient’s inability to know what medications he was taking might have partially contributed to the poor diabetes management. The treatment plan focuses more on protecting the ulcers from getting worse while he deals with his family issues. The patient has greatly improved his diet to plant-based nutrition, with limited sugary drinks at special occasions. He started mental health counseling to improve his marriage and stress management. He also received custom molded insole for the left foot and a Charcot Restraint Orthotic Walker (CROW) for the right foot to offload pressure of the ulcers (Figure 3). The patient was grateful that he is able to cope with his personal issue and still has two complete feet. Charcot Restraint Orthotic Walker (CROW). (A). Insole of the CROW. The arrow indicates the offloaded area for the ulcer. (B). CROW is fitted to the patient.
Conclusion
The management of DFUs and other chronic wounds requires a comprehensive, multidisciplinary approach. Understanding chronic wound types and etiologies, particularly DFUs, is crucial for effective interventions. Lifestyle-associated risk factors underscore the importance of integrating local wound care with lifestyle interventions.
The pathophysiology of DFUs involves a multifactorial interplay contributing to their high prevalence and associated risk of lower limb amputations. The standard of care emphasizes infection and vascular management, pressure offloading, conducive wound healing environments, re-evaluation, comorbidity management, and lifestyle adjustments.
Lifestyle medicine emerges as a pivotal aspect of chronic wound management, impacting gene interactions, immune function, tissue regeneration, and overall well-being. Integrating lifestyle medicine principles into conventional wound management can effectively treat and prevent chronic wounds, alleviating the burden on individuals and the healthcare system.
Discussion
As the prevalence of diabetes continues to rise, it becomes increasingly essential to aa0dopt a proactive approach that emphasizes lifestyle-centered wound assessment and treatment plans. Clinicians must remember that their primary focus is on treating the patient, not just the wound. It is crucial for the patient to prepare their body for wound healing, encompassing mental, physical, and physiological readiness. Consequently, a comprehensive, whole-person lifestyle intervention represents the most effective strategy for wound management. Communications play an important role in not only letting patients know the treatment plan but also to gain trust from the patients. This connected sense of trust allows patients to reveal the underlying factors that hinder the healing process.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.