
Abstract
Pediatric overweight and obesity is a complex chronic medical condition with a multitude of contributing factors. Rates are now nearly double what they were before the COVID-19 pandemic and if the current trajectory holds it is anticipated that by 2050 one in every two US children will experience obesity before the age of thirty-five. Pediatric obesity guidelines emphasize referral to intensive health behavior and lifestyle therapy programs, but these are difficult to access. Front line providers caring for children can use a lifestyle medicine approach within the medical home to make lifestyle changes easier. Lifestyle Medicine can promote a family-oriented, weight-neutral approach by (1) Educating and equipping providers to assess readiness to change and providing high-quality motivational interviewing and lifestyle counseling, (2) Equipping patients and their families with tools involving the six lifestyle interventions to optimize health starting an early age, and (3) Offering a longitudinal uniform office approach to effectively prevent, manage and often reverse obesity and related comorbidities through healthy habit change.
“A LM approach to childhood obesity is empowering to both providers and patients.”
Case Study
Rosa is a 15-year-old girl who presents to your primary care office for her annual well child check. Her last visit to the office was three years ago and you learn that she was recently placed in the care of her grandmother. She is well-appearing but has a flat affect. There are healed linear scars on her forearms. In the chart you notice a significant increase in her body mass index (BMI) since age 12. Using the extended BMI growth chart, you see that her BMI increased from the 75%ile 3 years ago to now 120% of the 95th percentile today.
Introduction
Rosa’s story represents a common clinical scenario that pediatric providers are facing across the country as children return to their primary care medical homes after the COVID-19 pandemic. According to the Centers for Disease Control and Prevention, the body mass index (BMI) of children aged two through 19 years old, particularly among Hispanic and non-Hispanic black elementary-aged youth, increased at nearly double the rate of that seen pre-pandemic. 1 While childhood obesity was recognized as one of the most common chronic diseases of childhood prior to the pandemic, healthcare professionals are now calling for childhood obesity to be considered a United States public health emergency. 2 Shockingly, if the current trajectory holds, it is anticipated that by 2050 one in every two US children will experience obesity before the age of thirty-five.3,4
Childhood obesity is a complex medical condition with a myriad of internal and external contributing factors. Children with obesity are 50%–80% more likely to experience obesity as an adult and obesity is a lifelong risk factor for disease of nearly every body system.5,6 A 2015 New England Journal of Medicine study showed that 30%–50% of children with obesity carry at least one cardiometabolic risk factor, and risk factors increase in number with increasing severity of obesity. 5 Diseases such as non-alcoholic fatty liver disease and type 2 diabetes mellitus are particularly concerning since they have a more aggressive phenotype when presenting in childhood.7,8
We are at a critical time in the national dialogue around childhood obesity with the American Academy of Pediatrics (AAP) publication of its first “Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents with Obesity” in early 2023. 9 This clinical practice guideline (CPG) thoroughly reviews the evidence and suggests key action statements while emphasizing that obesity is a chronic, relapsing disease and watchful waiting is no longer an appropriate strategy. The guidelines also reinforce that a person’s health and body size are impacted by far more than lifestyle choices; factors such as economic stability, access to education, living environment, race, genetics, and chronic stress. The CPG also appropriately acknowledge the impact of weight bias that is experienced both in the community as well as, unfortunately, in health care settings.
However, important questions are being raised and debated about the national guidelines. Some of the strongest scrutiny is around the emphasis on surgery and on the glucagon-like peptide-1 receptor agonists (GLP-1) that were recently approved for children starting at just 12 years old.10-12 While the CPG recommends medications and surgery as an adjunct to lifestyle changes, there is growing concern that an approach that includes a stronger emphasis on surgery and medications may contribute to disordered eating and detract from the messaging around healthy habits. Even if there were a population-level decrease in weight from medications, without healthy habits, this generation of adolescents would remain at elevated lifetime risk for cardiovascular disease, cancer, and other chronic conditions.13-15 We know that regardless of weight, healthy habits have a strong and lasting positive effect on both physical and mental health.9,16-21
As with lifestyle change, medications and surgery also require a lifelong commitment. We know, for instance, that stopping anti-obesity medications often leads to rebound weight gain.22,23 It is also well documented that anti-obesity drugs have side effects, and available studies are not able to tell us about the long-term effects of these medications on young, developing bodies.22-25 Additionally, recent reports of suicidal thoughts linked to the use of GLP-1s are drawing increased scrutiny from both European regulators and the FDA. 26
For the primary care provider, the AAP obesity guidelines include a strong emphasis on referring to intensive health behavior and lifestyle therapy (IHBLT) for children who are at least 6 years old and have overweight and obesity. Effective IHBLT programs deliver 26 or more hours of face-to-face, family-based counseling on nutrition and physical activity over at least a 3- to 12-month period. 9 IHBLT programs are difficult to fund, sustain, and currently not easily accessible to most pediatric providers and their patients. 27 Patients who do have access to IHBLT programs may prefer to stay in their medical home for reasons such as transportation barriers or comfort level with providers.28,29
We are excited about the opportunity for lifestyle medicine (LM) to augment the guidelines in three key areas to support providers on the front lines of pediatric obesity: 1. Educate and equip providers to offer high-quality health behavior and lifestyle counseling in a manner that is weight-neutral and considers critical factors like the social drivers of health. 2. Equip patients and families with educational tools involving interventions in the six pillars of a healthy lifestyle which can be incorporated into a family-focused, comprehensive care plan. 3. Offer a consistent and longitudinal office approach in which the number of healthy habit touchpoints is increased within a busy medical home.
There is no easy solution to address the issue of childhood overweight and obesity; however, LM offers a comprehensive, family-oriented, and weight-neutral approach that addresses both physical and mental health and recognizes the impact of the social drivers of health. One of the most pressing unmet challenges for preventing and controlling epidemic obesity is ensuring that historically marginalized populations benefit from relevant public health interventions. 30 The high cost of anti-obesity medications such as GLP-1s is already further increasing health disparities. 31 Both the AAP guidelines and an article by Ludwig DS and colleagues published in JAMA in 2023 deftly highlight the importance of better research into nonpharmacologic treatments in children and across the lifespan.9,31 Childhood obesity is a hot topic sitting right at the crossroads of science and social justice.
The AAP guidelines appropriately emphasize that obesity is a complex chronic disease influenced by just as many, if not more, external factors as internal factors. Our communities are overwhelmed with obesity-promoting influences that often overwhelm individual efforts to control weight in a healthy range. These external factors (represented in Figure 1 by the two outer large arches) require comprehensive and long-term policy, systems, and environmental strategies to shift both the range and balance of behavioral options toward an obesity-protective environment where the healthy choice becomes the easy choice. The lower dark green area in Figure 1 represents biologic and genetic risk factors which some may view as “fixed” and without hope; however, studies in epigenetics demonstrate that our habits and our environment significantly impact gene expression.32,33 In the field of Lifestyle Medicine, we like to emphasize that “our genes don’t have to be our destiny.”
34
Research framework for childhood obesity from the Michael & Susan Dell Center for Healthy Living. Originally published by Perry et al and reprinted with permission by the lead author.
Although many factors impacting obesity are outside individual control, we know that individual health behavior change is a critical piece of the puzzle in our increasingly sedentary, fast-food culture with easy access to ultra-processed foods and sugar-sweetened beverages. Behavioral factors, personal factors, and family/peer factors (represented by the blue arch in Figure 1) are areas where individuals generally have more control over their health than they realize when they are ready and able to make changes. It is in this space of individual health behavior change that most of us work and live every day, and this is where a lifestyle medicine approach can be impactful to both providers and their patients.
Case Study (Continued)
Rosa’s grandmother expresses that she has been very worried about her. Over the past year, Rosa has gradually been spending more time in her room and less time engaging with family and friends. You learn that her mother lost custody of her due to substance use disorder when Rosa was just 13 years old, and her father is not involved in her life. Rosa shares feelings of hopelessness and she has tried cutting. Her PHQ-9 depression screen is elevated today in the “moderately severe” range.
At this point in the case, two very important issues stand out about Rosa’s health: her significant BMI acceleration and her depression. Of course, depression presents potential safety issues and should be immediately prioritized. This case illustrates a young patient with both chronic mental health (depression) and chronic physical health (obesity) conditions, which allows an opportunity to consider the importance of readiness to change. When we reflect on Rosa and her grandmother’s readiness to change with her increasing BMI, it is fair to say they would be in the “precontemplation stage” of the transtheoretical model for change (Figure 2).
35
Precontemplation can imply that a person is not interested in considering change or maybe they are unaware that there is a problem at all. The term precontemplation can also indicate there are much more pressing issues that a patient is currently prioritizing. When we consider readiness to change in terms of her depression, however, her grandmother shows a much higher level of readiness. In fact, it is her primary concern at today’s visit. Transtheoretical model of change originally created by J. Prochasko and C. DiClemente.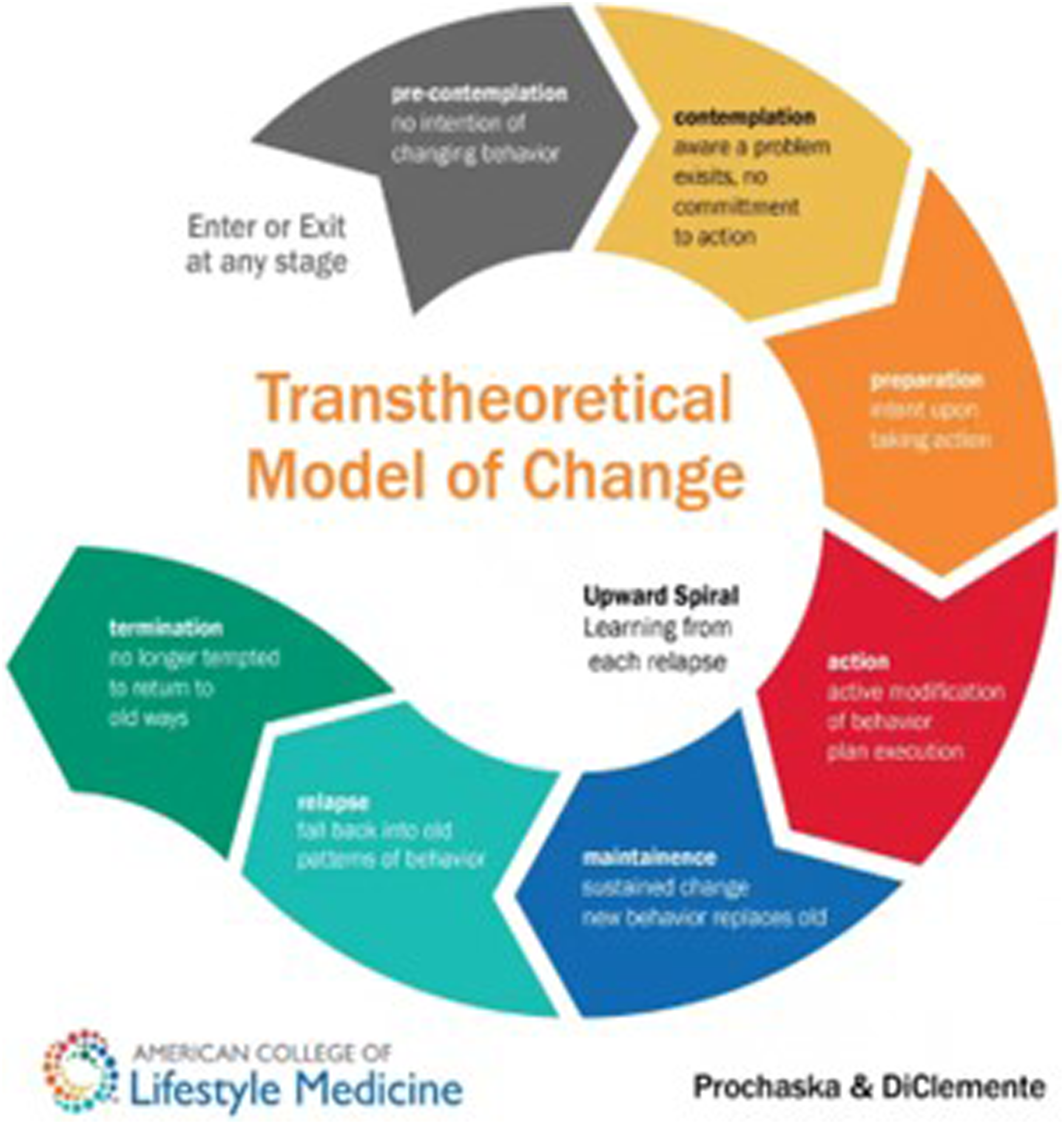
Assessing Readiness to Change
For a multitude of reasons, most patients will not be ready for change the first time clinicians note an increasing BMI, but these early stages are when motivational interviewing is most impactful to help resolve ambivalence and address barriers (Figure 3).36,37 No matter how high the BMI is or how many comorbidities exist, when clinicians give advice or start setting goals when a person is not ready or give advice without understanding their situation, resistance is built rather than rapport. As clinicians, we must pay attention to what our patients are ready to do, not what we are ready to tell them to do. Core motivational interviewing skills. Originally published in ACLM’s Beyond the Numbers: A Lifestyle Medicine Approach to Pediatric Obesity Toolkit. Reprinted with permission of lead authors.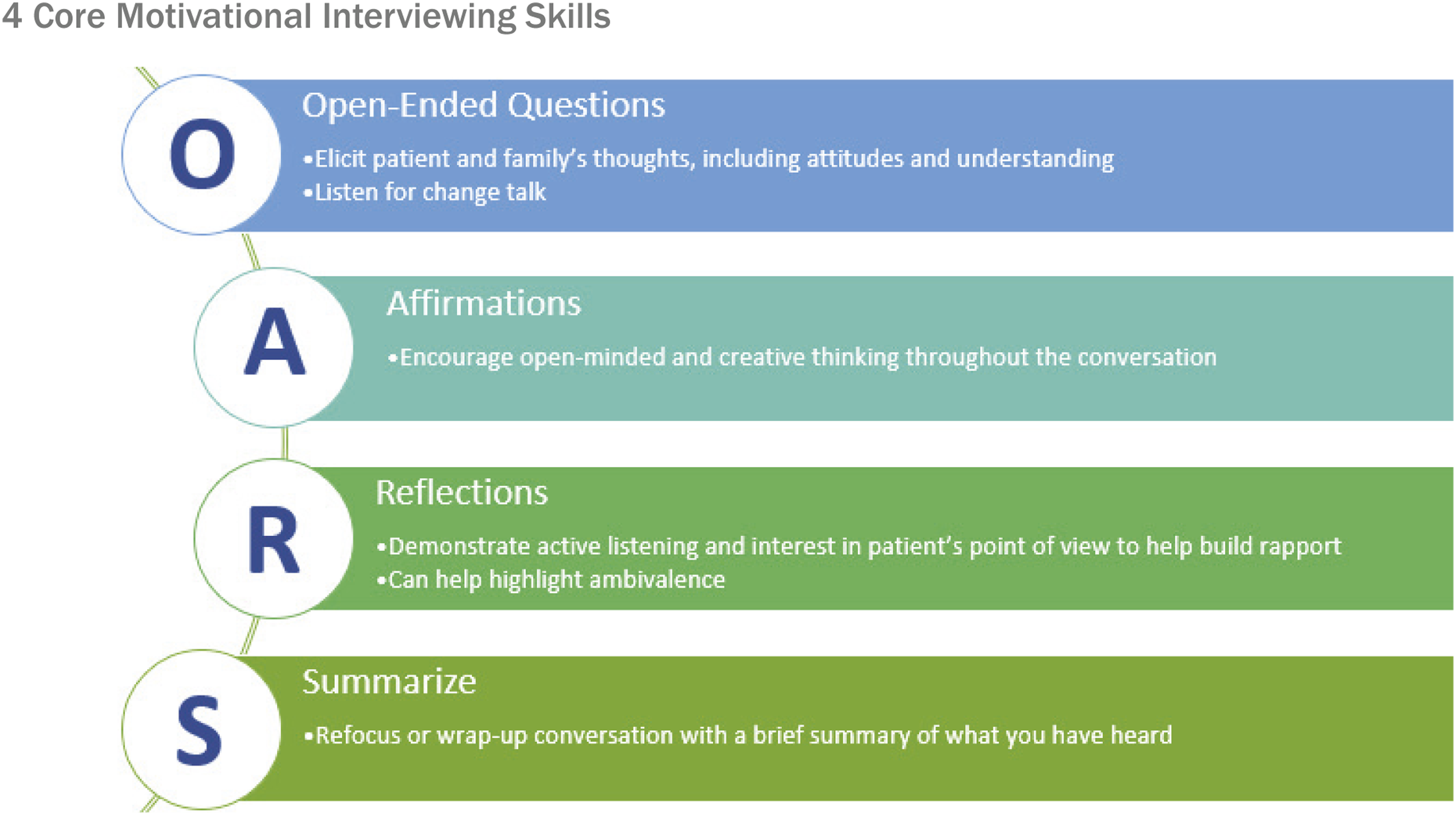
Complex factors are at play, driving both her depression and increasing BMI over the past several years. As the case suggests, Rosa has experienced adverse childhood events. Clinicians must recognize the complicated pathology of toxic stress which disrupts neurobiology and neurodevelopment often leading to chronic illness, including obesity, and can even lead to early death.38-40 In addition to considering the impact of toxic stress, the social drivers of health are a critical part of understanding individual patients in an integrated manner. For instance, where Rosa lives, her primary caregiver’s level of education, their household income, her race, and access to food all play an important role in her risk of obesity and chronic disease.30-32
Case Study (Continued)
You proceed with your standard evaluation for depression and assess her safety. Rosa and her grandmother are open to the idea of trying a medication, but they hope she will not be on it “forever.” They are open to counseling as well. You know that the medication and the counseling will both take about 4-6 weeks, and you ask the family if they would like to work on a healthy habit that is evidence-based for depression in the interim. The family says “yes.”
An LM approach incorporates qualities needed to address both of Rosa’s complex chronic health issues, as all six LM interventions are evidence-based for the prevention, management and even treatment of chronic disease. This comprehensive approach allows for improvement in BMI even while treating other chronic issues, such as depression. This can be freeing and empowering for providers and patients alike. Issues and solutions are not viewed in silos when we practice a more integrated approach to wellness.
There is an exciting synergy among the six pillars in an LM approach. If a patient like Rosa is interested in starting healthy changes, the interventions are likely to benefit both mood and BMI in a dose-response manner. Adopting one new healthy habit is likely to lead to another, and often combining lifestyle interventions is even more impactful. 41 Specifically considering depression, evidence-based lifestyle interventions can be utilized as part of a comprehensive plan that includes medication and therapy independently, for those who would benefit from meds and therapy but are not ready, or independently for patients with mild–moderate depression.42-44
Case Study (Continued)
You offer Rosa and her grandmother a few options of evidence-based lifestyle interventions for depression (listed below).
○ Increasing physical activity. Physical activity has the benefit of reducing symptoms of depression. Research also shows that just decreasing sedentary time reduces depressive scores. Physical activity with a friend or family member has the added benefit of social connection and reducing stress.16,18,42 ○ Improving sleep hygiene. A growing number of studies highlight the benefits of nonpharmacologic sleep interventions for those with mental health issues.42,45 ○ Starting a mindfulness practice. Mindfulness is shown to improve symptoms of depression and anxiety. There are some excellent, free cognitive behavioral therapy-based apps available.42,46
They choose to start walking together and Rosa would like to try a mindfulness app.
A Lifestyle Medicine Approach to Pediatric Overweight/Obesity
Pediatric care providers are now providing care for chronic diseases more than ever before, and most are related to obesity. A standardized longitudinal approach is important, where management is uniform and messages to families are consistent across multiple providers and visits (Figure 4). We recommend that follow-up intervals become more frequent for patients when they are ready for change, which we define here as preparation or action stage of change. This approach optimizes provider time and expertise as well as utilizing clinic resources where they are most needed and can be most effective. The three parts of a Lifestyle Medicine approach to pediatric obesity. Originally published in ACLM Beyond the Numbers: a Lifestyle Medicine Approach to Pediatric Obesity Toolkit. Reprinted with permission of lead authors.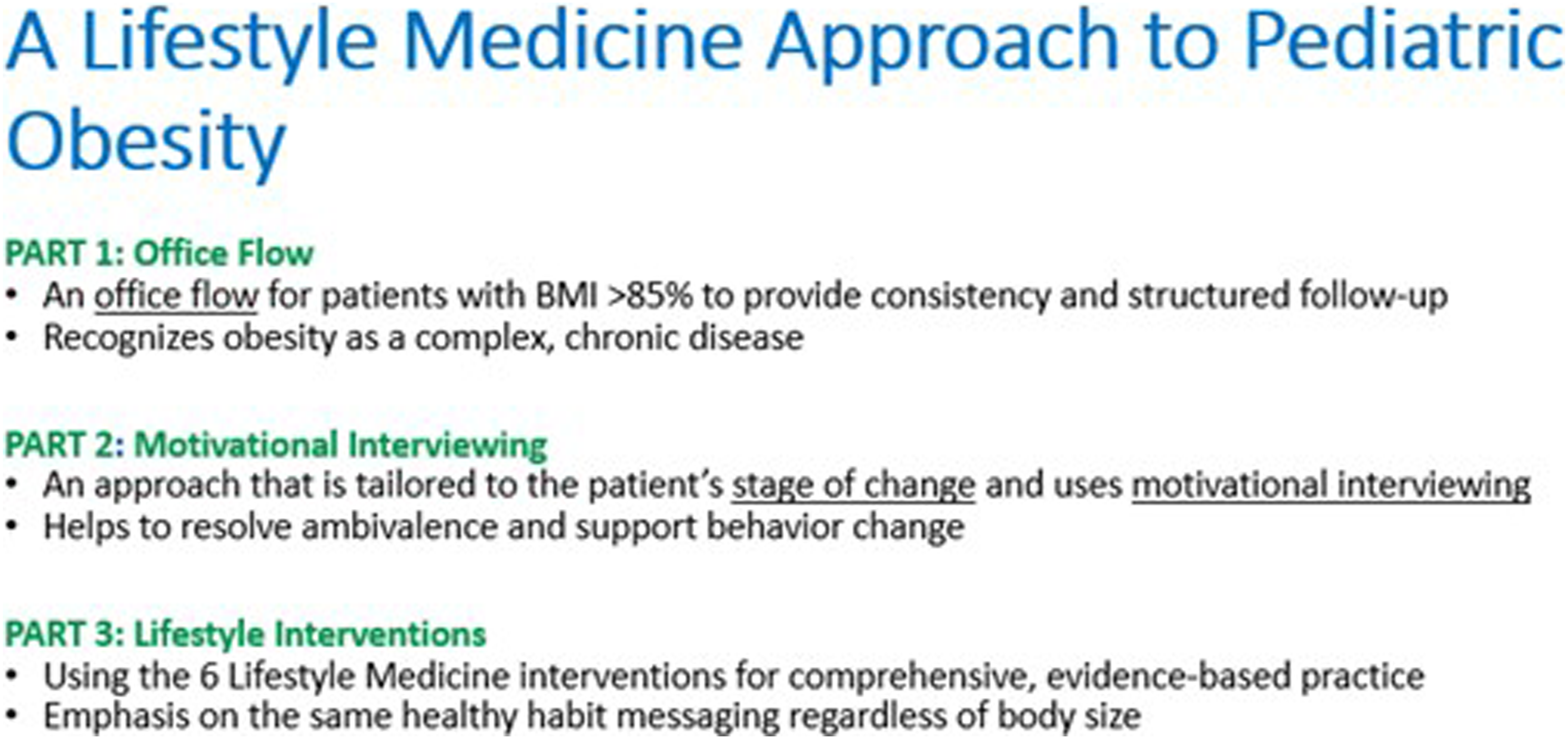
This structure to office flow feels very freeing for providers and patients alike as we respect the patient and family’s stage of change and promote self-efficacy. The 2022 American College of Lifestyle Medicine (ACLM) Pediatric and Adolescent Member Interest Group toolkit entitled “Beyond the Numbers: A Lifestyle Medicine Approach to Pediatric Obesity” offers pediatric providers specific and actionable recommendations for how to implement a comprehensive, family-oriented, and weight-neutral LM approach (Figure 5).
47
ACLM Beyond the Numbers: A Lifestyle Medicine Approach to Pediatric Obesity Toolkit. Access at https://connect.lifestylemedicine.org/viewdocument/beyond-the-numbers-a-lifestyle-med-2.
Case Study (Continued)
Rosa and her grandmother return three weeks later for follow-up. Rosa is taking her medication and says she feels a little better. She and her grandmother have enjoyed quality time after dinner walking the dog together. Rosa likes the free cognitive behavioral therapy-based app you recommended and is using that until her counseling appointment which is in five weeks. Her PHQ-9 has improved to the “moderate” range.
Another four weeks pass, and they return to your office. Rosa is smiling and more engaged with you. Her grandmother is visibly relieved. They are still enjoying the daily walks and have increased their pace. Her grandmother’s health is also improving from the physical activity, social connection, and fresh air.
Since Rosa’s mental health has stabilized, you decide this is an opportunity to try and discuss her growth chart again. (You may recall that Rosa’s BMI had accelerated from the 75th percentile three years ago to the 120th of the 95th percentile at the initial visit). After permission is given, you discuss the BMI acceleration on the growth chart, and you re-assess readiness around this issue.
Adopting a Weight-Neutral Approach
Body Mass Index (BMI) is an indicator with inherent limitations, and not a diagnosis. One BMI calculation on a growth chart is of little use, but a trajectory or pattern over time should prompt further inquiry. When addressing BMI and obesity, providers must first remember to “do no harm.” It is essential to approach this topic in a thoughtful manner to build collaboration, elicit reasons for motivation, and to promote body positivity.
A helpful initial step is to normalize review of the growth chart and first ask permission. Communication is of critical importance in these conversations and providers must practice the use of sensitive language with a keen awareness of their own weight bias, which is very common among healthcare providers. Many patients will have experienced weight- related trauma, such as bullying in the family, the community as well as, unfortunately, in the healthcare setting. 48
If a patient or family doesn’t identify weight as a concern, but a provider feels it is important to discuss, a sensitive statement could look like, “I always review growth charts with my patients. Would it be okay to look at the pattern on your child’s growth chart together?” (Or your growth chart if speaking to an older child.) Terms recognized as non-shaming are “unhealthy weight,” “elevated BMI,” or “excess weight.” 49 Latinx parents also found the phrase “too much weight for health” to be helpful. 50
When discussing growth acceleration, focus on health, longevity, and developing sustainable healthy habits as a family. Try to keep the conversation positive, pointing out the pleasurable aspects of new habits and eliciting reasons to make changes. Acknowledge past efforts to make healthy changes while recognizing that many will need to re-think an unhealthy “dieter’s mentality” to make successful lifelong changes. Recognize that the patient or family may be experiencing a wide variety of thoughts or feelings around this sensitive topic.49,51-53 For example, there may be a history of disordered eating, or other pressing issues affecting their family (such as depression in Rosa’s case). Barriers such as the social drivers of health must also be recognized and appropriately addressed. A family’s heritage, food culture, or issues like food allergies, must also be considered as these factors will often impact how receptive a family is to change.
A skillful clinician will keep a wide differential with growth acceleration as with growth failure. Are these changes in BMI the result of physical or mental health issues? Are there any new stressors in their life or changes in family habits or patterns? Non-judgmental, genuine curiosity, and open-ended questions are much more likely to get to the root of the issue while also building collaboration and positive rapport.
A weight-neutral approach begins at the earliest age. Discussion of the growth chart and lifestyle habits should be included at every visit, presented in a family context, with the same healthy messaging regardless of body size.51,54,55 If lifestyle habits are only discussed when there is a health concern, then habits are not being discussed enough and likely they are being linked more to weight than to health and longevity.
Case Study (Continued)
This most recent visit was scheduled as a mental health follow-up visit and Rosa is doing much better now with her depression. Because you built rapport over the last few visits and they are open to discussing the BMI acceleration today, you assess and find that they are ready to consider other healthy lifestyle changes. This is an opportunity to celebrate their success so far by highlighting the progress they have already made with increased physical activity and stress reduction through the goals that were set to address her depression. You agree on a follow-up visit that can be dedicated to review of healthy habits and addressing her BMI acceleration.
The step-by-step approach in this case illustrates that behavior change is a marathon not a sprint. As providers we must meet patients and families “where they are” and recognize their priorities while aiming to incorporate lifestyle changes whenever possible. In the appendix of “Beyond the Numbers: A Lifestyle Medicine Approach to Pediatric Obesity” there is a sample approach/algorithm used in one large pediatric practice incorporating readiness to change and BMI.
The “Beyond the Numbers” toolkit also contains a sample of a brief family intake survey designed to be filled out at a comprehensive lifestyle intake visit. The survey includes past medical history, family history, an assessment of how the family is doing with all 6 lifestyle interventions and screens for the social drivers of health. To make the visit more efficient, the survey corresponds with a note template that flows directly from these answers. The survey can also be used at subsequent visits to assess changes. For specific talking points and resources on all 6 interventions, refer to “Beyond the Numbers,” where you will find both provider-facing and patient-facing resources.
At the intake visit and each subsequent visit, one or two SMART Goals (Specific, Measurable, Achievable, Relevant, and Time-Bound) can be set if the patient continues to demonstrate readiness. Goals should be driven by the patient and family and re-assessed at each visit. If a patient is struggling with a goal, the follow-up visit is designed to address barriers to the goal or to adjust the goal with shared decision making. If the patient is doing well with the goals, new goals may be set to build on the existing ones.
Incorporating the Whole Family
Comparison of an expert versus a coach approach. Table originally created by Jessica A. Matthews, DBH, MS, NBC-HWC, DipACLM, FACLM; Margaret Moore, MBA; and Cate Collings, MD, MS, FACC, DipABLM for “A Coach Approach to Facilitating Behavior Change.” Supplement to the Journal of Family Practice, 71(1): eS93-eS99 and used with permission of senior author.
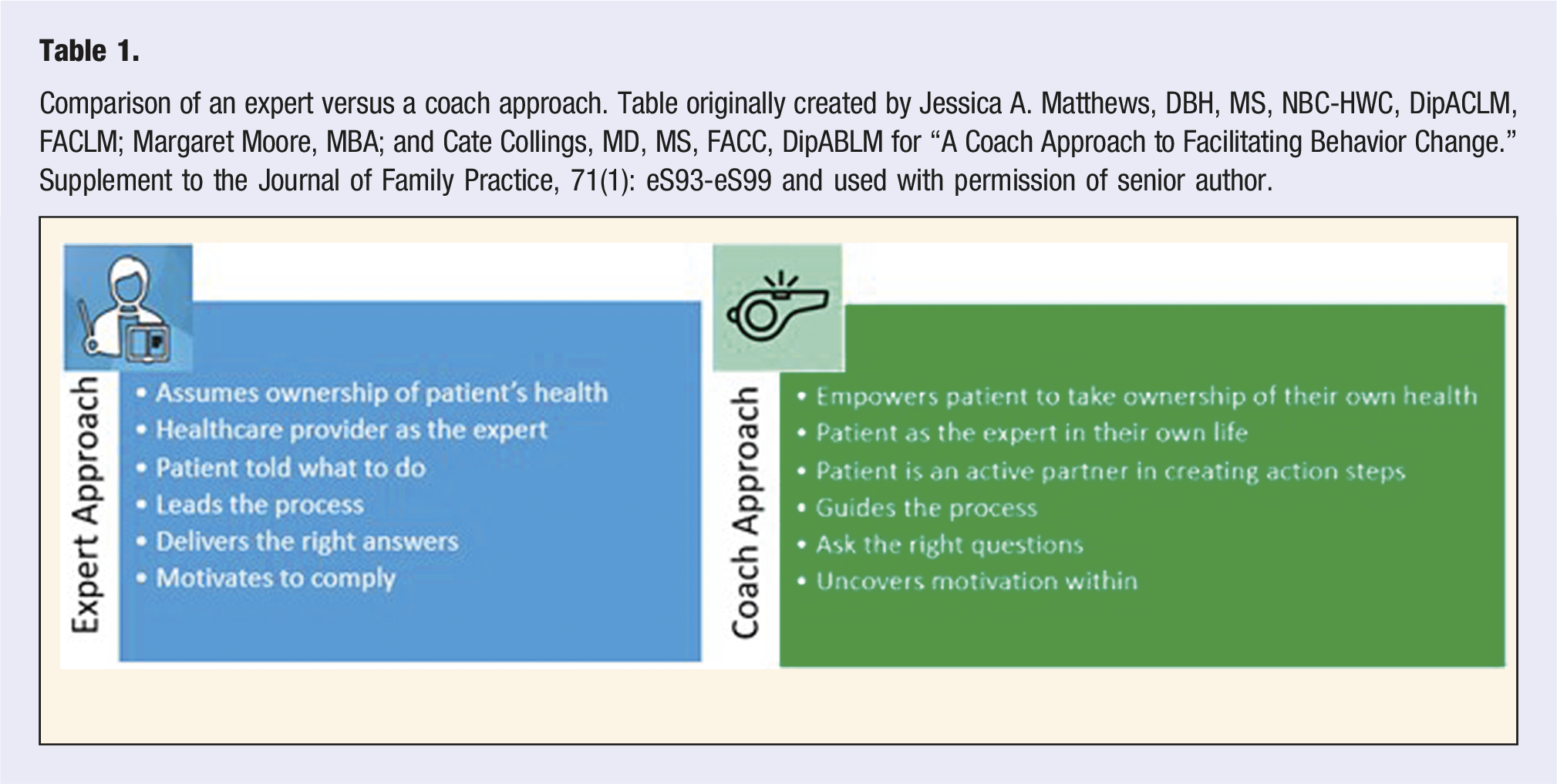
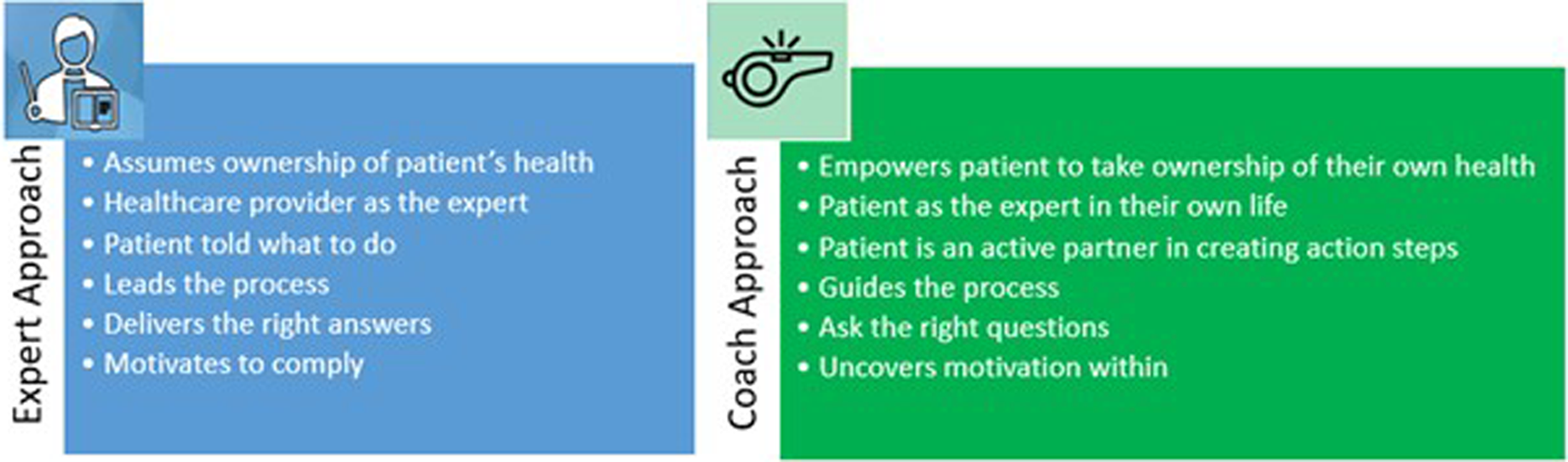
Parents and caregivers play a crucial role in positive behavior change. Parental behaviors most strongly associated with successful change include parental leadership in goal setting, problem solving, social support, role modeling, and restructuring the home environment. 57 “Beyond the Numbers” emphasizes the evidence for and importance of family mealtime to promote connection and role-modeling. 58 Ellen Satter’s “Division of Responsibility in Feeding,” for example, is a useful guide for parents that can be applied at every stage of development. 59 The toolkit addresses many common parental questions on common barriers to healthy eating habits.
Adolescence is an exciting developmental period, but it can present significant challenges to family-based care, particularly when there are mismatched levels of readiness between a teen and his or her family. However, progress can still be made, particularly if a caregiver is motivated to restructure the home environment in a way that is positive and promotes connection. For motivated and interested teens, ACLM offers an excellent resource “The Teen Lifestyle Medicine Handbook: The Power of Healthy Living.” 43
Conclusion
Ideally, an ACLM and an AAP approach should work synergistically as both approaches are weight-neutral and for the entire family. It is the opinion of the authors that ACLM is well positioned to assist the AAP CPG recommendations by equipping providers with high quality behavior-change counseling skills and tools for evidence-based lifestyle interventions. Equipping providers, many of whom have not been adequately trained in these skills and knowledge base, is urgently needed to help address the obesity crisis. Furthermore, an LM approach offers a consistent and longitudinal office approach that increases the number of healthy habit touchpoints in a pediatric practice, improving care for patients who do not have access to, or who are not interested in, an IHBLT program.
A LM approach to childhood obesity is empowering to both providers and patients. Providers are empowered with the knowledge and visit structure to use their time wisely and effectively, meeting patients where they are and coaching them along their path of change. It is also empowering for patients and families who are no longer passive recipients of information but are now “in the driver’s seat” as experts in their own lives, learning to apply lifestyle interventions for the prevention, management, and even treatment of chronic disease. An LM approach guides us to measure success not in terms of weight or numbers, but in terms of health behavior change. We know that even with little change in body weight, positive health behavior change can promote significant improvements in health and longevity for the patient and the family, ultimately changing generational patterns. As cultural anthropologist Margaret Mead offered, “Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it is the only thing that ever has.”
Supplemental Material
Supplemental Material - Empowering Families and Providers With a Lifestyle Medicine Approach to Pediatric Obesity
Supplemental Material for Empowering Families and Providers With a Lifestyle Medicine Approach to Pediatric Obesity by Jane Blakely Amati, MD, FAAP, DipABLM, and Erin L. Brackbill, MD, FAAP, DipABLM in American Journal of Lifestyle Medicine.
Footnotes
Author’s Note
Portions of this information were presented at the Annual Lifestyle Medicine Conference 2023: Denver, Colorado, October 30-November 2, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.