
Abstract
Lifestyle factors such as diet and exercise have been described as predictors of preventable disease such as Type 2 diabetes. Black/African American (AA) women disproportionately develop and are at greater risk, compared to Whites. The purpose of this study was to examine the association of exercise and adherence to MyPlate diet in this population. The health belief model was the theoretical foundation for this study. Research questions were designed to examine the extent to which lifestyle predicts diabetes. In this quantitative cross-sectional study, data from the 2015-2016 NHANES data sets were analyzed. Using SPSS, a series of binary logistic regressions were conducted. After controlling for age, there was no significant association between MyPlate diet adherence and diabetes (OR = .706, 95% CI [.292, 1.707], P > .005). Similarly, no significant association between exercise and diabetes was observed among this population (OR = 1.032, 95% CI [.721, 1.504], P > .005).
“A variety of studies have been conducted to analyze individual contributing food groups and not the MyPlate plan as a whole.”
Background
Health behaviors such as diet and physical activity, have been described as significant predictors of preventable diseases in the United States, including obesity and diabetes mellitus. 1 According to the Centers for Disease Control and Prevention (CDC), 2 more than 29 million Americans now live with Type 2 diabetes, and another estimated 86 million with prediabetes. The American Diabetes Association (ADA) 1 estimates 4 million annual incidences of diabetes, with millions still undiagnosed. Complications of diabetes can lead to heart disease, stroke, and kidney problems (ADA). 3 Estimated prevalence of diagnosed diabetes by race has shown rates to be highest among American Indians/Alaska Natives Hispanics, and non-Hispanic Blacks/African Americans (CDC). 4 Although significant evidence supports the relationship among Type 2 diabetes, nutrition, and physical activity, there is still a paucity of research in African American women. Overall, making lifestyle changes can dramatically help reduce disease risk and lower chances of developing Type 2 diabetes.5,6
Educational tools, such as Choose MyPlate, provide guidelines for diet and physical activity. Additionally, physical activity guidelines for Americans were published by the U.S. Department of Health and Human Services (USDHHS). These guidelines include the types and amounts of physical activities recommended to offer substantial health benefits (CDC). These tools can be used to promote lifestyle and behavioral changes. More research into the process of behavioral change can reveal opportunities for risk reduction, effective interventions, and improved outcomes. 4 In multiple studies, researchers have found that health behaviors can significantly influence Type 2 diabetes risks. 7 Determining why certain behavioral patterns are more frequently adopted than others can give additional insight into how to address disease prevention efforts. Finally, improving knowledge of health risks can work to reduce disease prevalence and health complications in the future. 7
Purpose
The purpose of this quantitative study was to examine predictors of Type 2 diabetes, including lifestyle factors (diet and exercise), in African American women over the age of 18 in the United States. The goal of this study was to fill a gap in the literature regarding the association between the MyPlate diet and physical activity and diabetes among African American women over the age of 18 in the United States. Current U.S. statistics show a disproportionately higher burden of chronic diseases among certain racial and ethnic groups, with increasing complex influences due to unique lifestyle and behavioral factors. 8 Prior researchers have found that, compared with Caucasian Americans, racial minority groups are at greater risk for both Type 2 diabetes and obesity. 7
Methods
Ethical Considerations
Walden University Institutional Review Board (IRB) confirms that this doctoral capstone meets Walden University’s ethical standards. IRB approval number 10-20-20-0082439. Due to utilization of secondary data analysis this study did not need ethical approval or informed consent. Office of Research Ethics and Compliance Walden University 100 Washington Avenue South, Suite 1210 Minneapolis, MN 55401 Email:
Priority Population and Procedures
The priority population included a representative sample comprised of African American women ages 18 and over in the United States. Existing secondary data analysis was used from NHANES to carry out this quantitative study. A cross-sectional design tested the association between independent variables nutrition (MyPlate) and physical activity (150 minutes per week) and dependent variable Type 2 diabetes. A sample size of 395 was calculated using a G* Power Analysis to determine the probability of diabetes among African American women who have been physically active and who have tried the MyPlate diet. As this is a current representation, the entire sample size was used.
Instruments
NHANES 2015-2016 used a sample person questionnaire instrument to collect individual-level information on participants related to diet behavior and nutrition and diabetes. For example, the use and awareness of MyPlate are assessed in the Dietary Behavior and Nutrition questionnaire. The three pertinent questions were: Have you heard of MyPlate? Have you looked up MyPlate on the Internet? And have you tried to follow the recommendations in MyPlate? Data were obtained and collected through personal household interviews. Variables are measured or manipulated by a three-part questionnaire, as previously mentioned. For each of these questions, participants have the option of choosing yes, no, don’t know, or they can refuse to respond to the question.
Physical activity is described as moderate intense exercise at least 150 minutes a week. For significant health benefits, the 2015 Physical Activity Guidelines for Americans recommends that adults engage in at least 150 minutes of moderate intensity physical activity per week. Fewer than 150 minutes of physical activity per week was considered not meeting Physical Activity Guidelines for Americans. Physical activity was assessed by participants’ self-reported and actual time spent engaging in physical activity. Participants’ response to whether they engage in moderate intense physical activity was used to categorize those who engaged in physical activity.
Type 2 diabetes, MyPlate, and physical activity are considered both categorical and nominal for this study. Age is a continuous variable because it is numeric and can include an infinite number of values. Type 2 diabetes is the dependent variable, as its outcomes can be dependent upon the manipulation or alteration of the independent variables, MyPlate and physical activity. Age is a confounder as it influences both the dependent and independent variable, while also being used to examine potential cause and effect of the relationship between the variables.
Data Analysis Plan
IBM’s SPSS Version 25 was used to import NHANES data for management and analysis. First, the data set was fragmented to include only African American women ages 18 and above. G*Power 3.1 statistical software was used to run a power analysis and compute the required sample size for this study. Software used for this analysis came from Faul et al. (2007). 9 G*Power 3 is a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. The research questions are reiterated below, and the specific analytical strategy explained after.
Descriptive statistics were used to describe the sample characteristics. Frequencies and percentages were reported for categorical data (i.e., age, socioeconomic status, diabetes, MyPlate diet, and physical activity). Means and standard deviations were reported for interval variables. Statistical methods may be used to control confounders related to the primary relationships between exposure and outcomes. Both unadjusted and adjusted odds ratios are reported.
Results
A series of binary logistic regressions were conducted with the dependent variable Type 2 diabetes and MyPlate and physical activity as the independent variables. SPSS sample procedures were used for performance analysis.
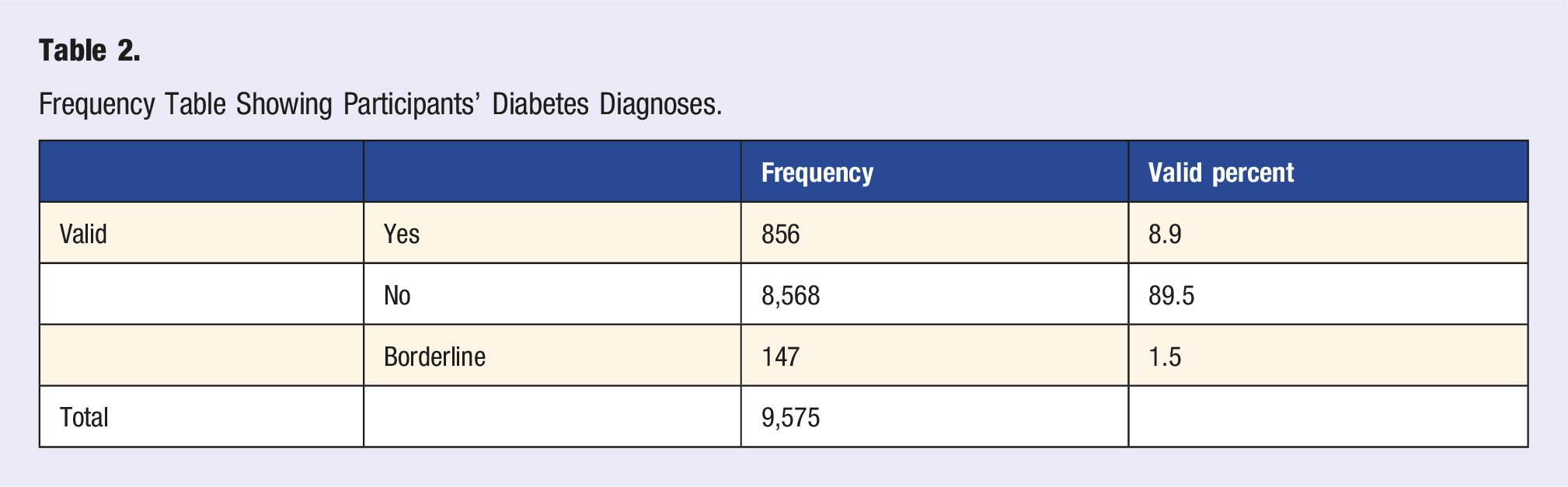
To answer RQ1, a set of uniquely qualified participant identification numbers were used, and the NHANES interview data files were merged to include only those observations with specific criteria. A valid sample of approximately 9571 participants responded yes, no, or borderline that they had been told by a doctor they have diabetes. According to the American Diabetes Association, approximately 11.7% of African Americans/non-Hispanic Blacks are diagnosed with diabetes, compared to 10.4% found in this sample. Borderline results were not included. Without including borderline diabetics, this sample had a lower prevalence of diabetes than the general population. When borderline was included, the percentage was comparable to the general population. Table 1 shows the number of participants who received a diagnosis or were told by a doctor they had diabetes. Additionally, Table 1 represents the frequency and number of individuals who were told yes, they had diabetes, no, they did not have diabetes, or they were borderline, meaning prediabetic. (Brandi Jones, Association of MyPlate Diet and Exercise with Diabetes in African American Women, 2022)
Final (Adjusted) Logistic Regression for MyPlate, Physical Activity, and Diabetes.
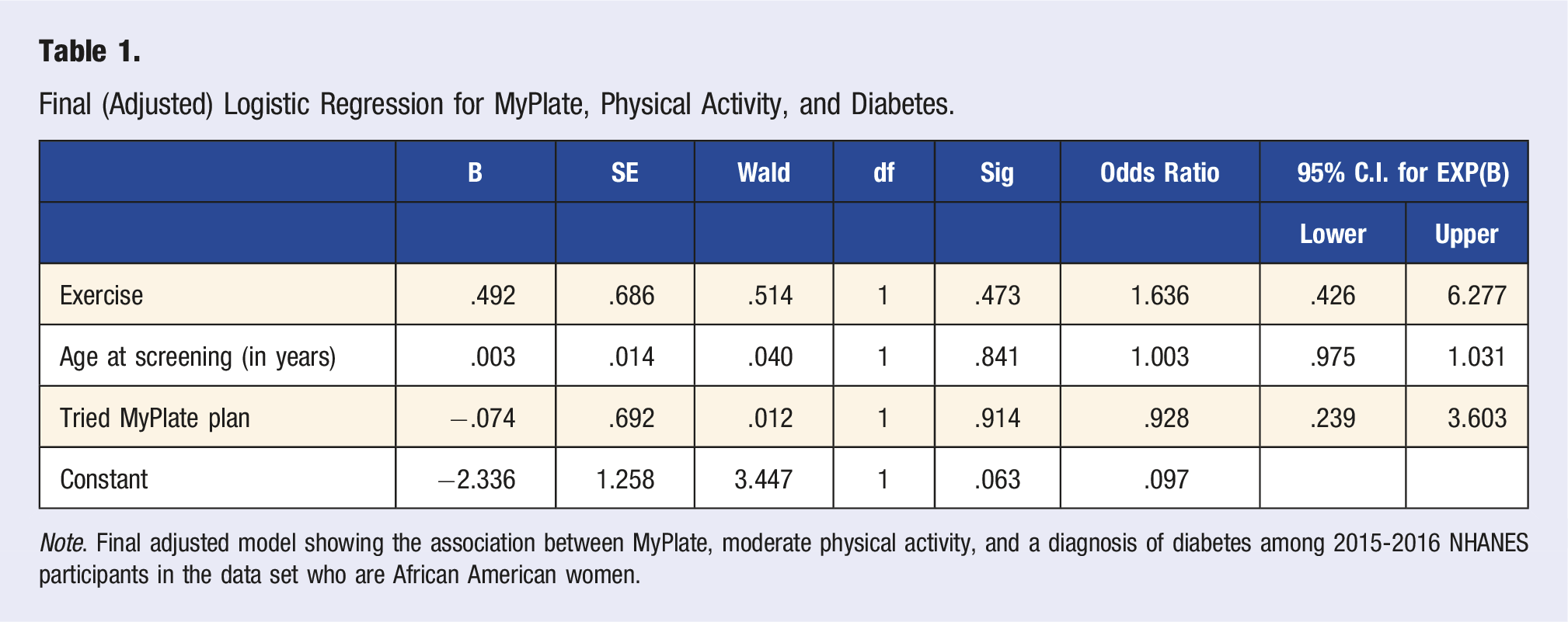
Note. Final adjusted model showing the association between MyPlate, moderate physical activity, and a diagnosis of diabetes among 2015-2016 NHANES participants in the data set who are African American women.
To answer RQ2, a binary nominal logistic regression was conducted. The dependent variable was Type 2 diabetes, and the independent variable was the MyPlate diet. A total sample of 1245 participants responded to whether they had tried the MyPlate plan. A bivariate logistic regression analysis was conducted to determine if trying MyPlate is a predictor of Type 2 diabetes. This statistical analysis was conducted to examine the relationship between the dependent and independent variables and to estimate the likelihood of diabetes as an outcome. There was a significant amount of missing data; those values were not included in this analysis. After running the logistic regression, the outcomes were within the same range of the odds ratio and comparable to the general population. Table 2 displays a binary logistic regression showing the association between MyPlate and a diagnosis of diabetes among NHANES 2015-2016 study participants who are African American women. Out of a total of 446 African American women participants who tried the MyPlate diet, the unadjusted odds ratio is .705. The result of this analysis was not statistically significant, at P > .05, and there is no association. (Brandi Jones, Association of MyPlate Diet and Exercise with Diabetes in African American Women, 2022)
To answer RQ3, a binary logistic regression was conducted. The dependent variable was Type 2 Diabetes, and the independent variable was physical activity. A valid sample of 6963 participants responded to the question of participated in moderate physical activities as “yes,” “no,” or “don’t know.” Table 3 contingency table reveals those who exercise and have Diabetes vs those who exercise and don’t have Diabetes. This table also displays data regarding those who did not exercise and have Diabetes, as opposed to those who did not exercise and don’t have Diabetes. The data was recoded data to include only 1 - yes, and 2 - no, and “don’t know” was excluded. All other values were defined as system missing. Table 3 displays a contingency table showing frequency of participants who participated in moderate physical activity and who had a diagnosis of Diabetes. Out of a total of 751 participants, 60 were diabetic, and 691 were not. In the same manner, 417 were physically active, while 334 were not. The result of this analysis was not statistically significant, since P > .05, and there is no association. (Brandi Jones, Association of MyPlate Diet and Exercise with Diabetes in African American Women, 2022) Table 3 displays a binary logistic regression showing the association between moderate physical activity and a diagnosis of diabetes among the entire population of participants in the 2015-2016 NHANES data set, who are African American women. Out of a total of 1,265, the unadjusted odds ratio is 1.041. The result of this analysis was not statistically significant, since P > .05, and there is no association. (Brandi Jones, Association of MyPlate Diet and Exercise with Diabetes in African American Women, 2022) The binary logistic regression analysis showing the association between moderate physical activity and a diagnosis of diabetes among 2015-2016 NHANES participants in the data set who are African American Women, was similarly significant at 1.041. Therefore, there is no association between Type 2 diabetes and physical activity in African American women in the United States Table 4 displays the Final Adjusted model showing the association between MyPlate, moderate physical activity and a diagnosis of diabetes among 2015-2016 NHANES participants in the data set who are African American Women. The result of this analysis was not statistically significant, since P > .05 and there is no association. Therefore, there is no association between Type 2 diabetes and physical activity in African American women in the United States (Brandi Jones, Association of MyPlate Diet and Exercise with Diabetes in African American Women, 2022)
Summary
From the results of the data analysis, with a 95% confidence interval and P < .05, it is noted that there is no association between the MyPlate diet and Type 2 diabetes in African American women. In the same manner, the results of the next data analysis showed there is no association between physical activity and Type 2 diabetes in this particular population. Age was initially included as it was considered to be an important variable; however, the overall analysis showed that the odds ratio did not change significantly when adjusted for age; therefore, age would not be considered a significant confounder.
Overall, there was insufficient evidence to indicate whether there was a statistical significance or not between these variables, and to determine if the prevalence is comparable to that of the national average.
Frequency Table Showing Participants’ Diabetes Diagnoses.
MyPlate and Diabetes Contingency.
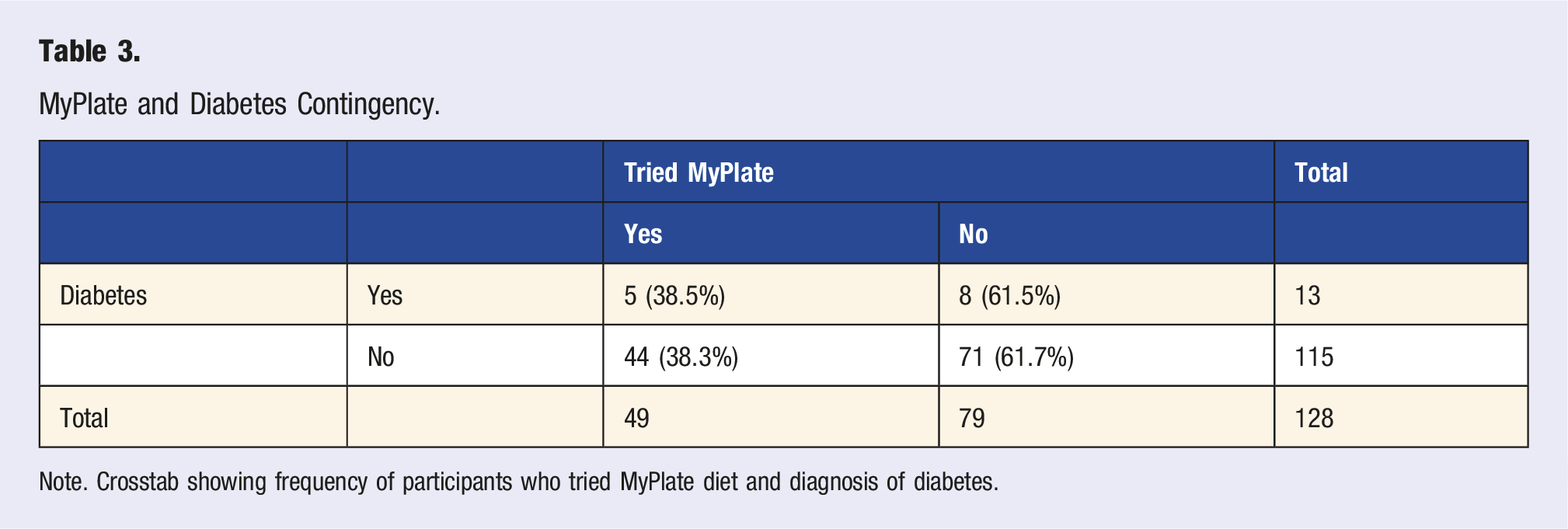
Note. Crosstab showing frequency of participants who tried MyPlate diet and diagnosis of diabetes.
Binary Logistic Regression (Unadjusted) for MyPlate and Diabetes.
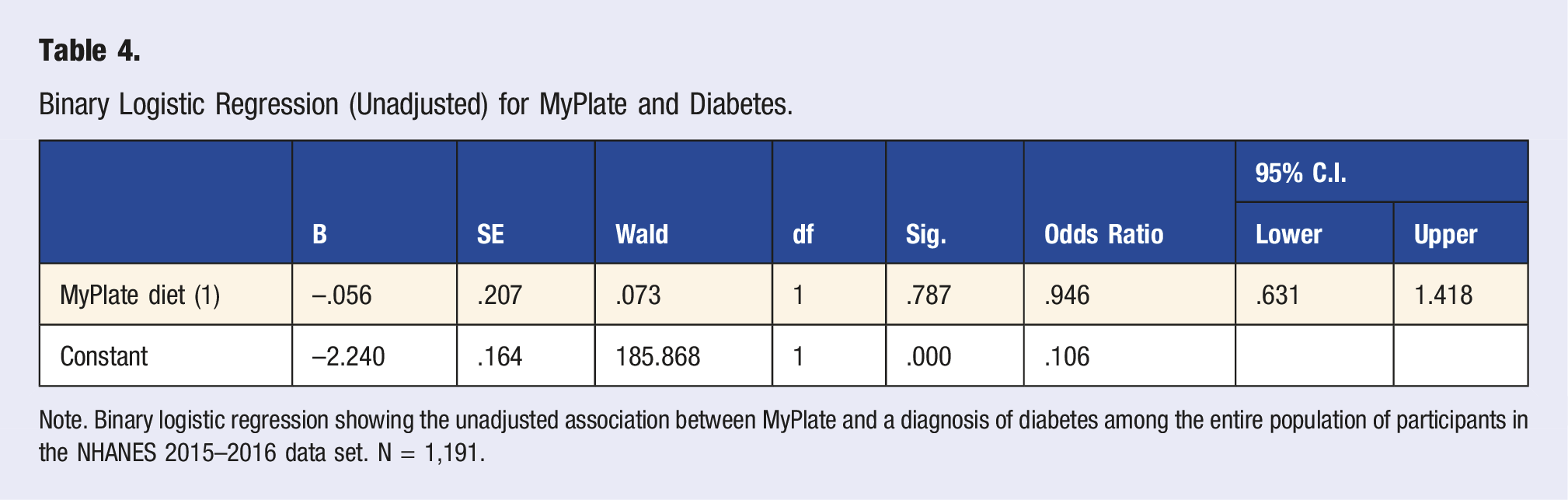
Note. Binary logistic regression showing the unadjusted association between MyPlate and a diagnosis of diabetes among the entire population of participants in the NHANES 2015–2016 data set. N = 1,191.
Discussion
As a significant number of African American women are borderline, prediabetic, or undiagnosed, a major predictor of health outcomes has been health education status. Knowledge of one’s individual health status, in theory, leads to better health outcomes. Individuals’ attitudes and beliefs can have a strong effect on behavioral patterns in general and from a nutritional perspective, such how or if they use the MyPlate diet. Although there is limited information on the MyPlate diet, some studies have shown that consuming food groups represented in MyPlate is key to improving health disparities. 10 However, some researchers have also described how dietary guidelines can be culturally challenging.
As the MyPlate plan is a guideline intended for Americans to eat and be heathier, this study shows no association between African American women and the plan. This leads to further exploration of the design and study of the MyPlate plan, including what populations it intends to target. After numerous studies have been fulfilled, a persisting concern that may still arise would be if this plan was intended for all Americans or just a particular group or population. Determining if the MyPlate plan works is difficult because there are so many different nutrients involved. In general, a variety of studies have been conducted to analyze individual contributing food groups and not the MyPlate plan as a whole.
As the CDC recommends at least 30 minutes of weekly physical activity, studies have shown that not only African Americans, but the American population in general falls below the recommend guidelines for exercise. More than 15% of the American population is physically inactive. The CDC states a lack of physical activity as one of the leading preventable risk factors for Type 2 diabetes. From a cultural perspective, one major contributor to lack of physical activity is time. Busy work, family, and personal schedules have been the basis of limited exercise in various populations, including the African American community. Another reason African Americans lack proper exercise is the environment. Many Americans live in communities that are not designed for physical activity, including lack of sidewalks, parks, and walking trails, which in turn, contributes to limited activity.
Although physical activity guidelines are intended for Americans to be healthy, this study is showing no association between physical activity and Type 2 diabetes in African American women. In comparison to much of the research that has been conducted, the likelihood of a positive association between physical activity and type 2 diabetes in African American women, is evident, but limited data, including the amount of African American study participants, may have affected the results. Various studies continue to show that exercise can help increase energy, reduce stress, and ultimately help reduce risk of health complications.
Limitations of the Study
There were a few limitations of this study including the use of self-reported data, and the nature of the cross-sectional study. The data for this current study was obtained from NHANES 2015-2016. NHANES utilizes a multistage group of cross-sectional studies that help monitor and evaluate the health and nutrition status of both children and adults in the United States. The main challenge with this self-reported data is the information may not be completely accurate. Subjects knowledge may be limited by what the MyPlate diet is and what it entails. This may have affected their responses of “yes” or “no” to “Have you tried the MyPlate diet.”
Another limitation of this cross-sectional study is difficulty drawing predictive conclusions. Because exposure and outcomes are typically assessed simultaneously, there is generally little to no evidence of a temporal relationship between the two. This makes it difficult to establish a true cause and effect relationship. 11
Implications for Professional Practice
Professional practice and social change implications of this study include furthering research and expanding experimental designs that may introduce new food guides and nutrition plans. The results of this study may contribute to positive social change by encouraging not only Black women to make behavior changes, but also health practitioners to promote wellness and preventive health services in their practices. While Type 2 diabetes has been studied by scholars for years, health disparities have persisted, and scholars have struggled to remedy this chronic disease among non-Hispanic Black women (Journal of the American Medical Association, 2005).
More exploration into the process of behavioral change can reveal opportunities for improvement and effective interventions (Hartley, 2014). According to Tija (2008), little emphasis has been placed on soliciting behavioral change as it relates to diabetes education, and possible costs associated with these concerns. From a medical standpoint, research shows that less than 44% of physicians indicated that they routinely provide educational material(s) to patients (Tran, Walker, Wassersug, Matthew, and McLeod, 2017).
Further research is warranted from a culturally diverse perspective. As studies continue to show, minority populations are at higher risk of health complications from chronic diseases such as type 2 diabetes. 7 Greater knowledge and information can improve decision-making opportunities among this population. Presuming inclusivity in education is more of a perplexity than access, minority groups need to see themselves as part of a plan of action and solution, which can help reduce disease burden and improve health status.
Many health plans, programs, guidelines, and recommendations limit inclusivity when it comes to culturally diverse groups of people. Furthermore, they do not take into account food and nutrition practices, physical activities, or behavioral practices these groups typically participate in. Implementing more culturally diverse strategies can increase participation and utilization.
Overall, diet, exercise, and managing weight are lifestyle factors that can help manage diabetes).12,13 A determination of why certain behavioral patterns are more frequently adopted than others can give additional insight on how to address disease prevention efforts. Finally, improving knowledge of health risks can work to reduce disease prevalence, as well as health complication in the future. 7
Footnotes
Acknowledgments
I would like to express my profound appreciation to my academic advisors Dr Heba Tawfik, Dr Gwendolyn Francavillo, and Dr Namgyal Kyulo, for their guidance, which allowed me to complete this research. I truly appreciate your time, expertise, and generous contributions to increase my knowledge of this subject matter. I am also grateful to my family and friends for their love, inspiration, motivation, and commitment throughout this journey. They have persistently helped me keep focus in pursuit of the most important things in life. Thank you for supporting me in diverse ways to make this achievement a reality.
Dr Brandi Jones
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.