
Abstract
Objective: Identify areas of consensus on integrating lifestyle medicine (LM) into primary care to achieve optimal outcomes. Methods: Experts in both LM and primary care followed an a priori protocol for developing consensus statements. Using an iterative, online process, panel members expressed levels of agreement with statements, resulting in classification as consensus, near consensus, or no consensus. Results: The panel identified 124 candidate statements addressing: (1) Integration into Primary Care, (2) Delivery Models, (3) Provider Education, (4) Evidence-base for LM, (5) Vital Signs, (6) Treatment, (7) Resource Referral and Reimbursement, (8) Patient, Family, and Community Involvement; Shared Decision-Making, (9) Social Determinants of Health and Health Equity, and (10) Barriers to LM. After three iterations of an online Delphi survey, statement revisions, and removal of duplicative statements, 65 statements met criteria for consensus, 24 for near consensus, and 35 for no consensus. Consensus was reached on key topics that included LM being recognized as an essential component of primary care in patients of all ages, including LM as a foundational element of health professional education. Conclusion: The practice of LM in primary care can be strengthened by applying these statements to improve quality of care, inform policy, and identify areas for future research.
Keywords
“Implementing LM in primary care settings benefits providers and patients by identifying the root causes of many chronic diseases that may be prevented, managed, or even reversed using lifestyle interventions coupled with proactive strategies for healthy behavior change.”
Introduction
The United States (US) health care system is performing poorly for patients, clinicians, and the overall economy.1–5 In 2021, the US spent US$12,914 per person in health care costs—approximately 18% of the gross domestic product, which is the highest per capita spending compared to peer nations analyzed by the Organization for Economic Co-operation and Development.1,6 Concurrently, average life expectancy in the US has been decreasing since 2014, long before the COVID-19 pandemic, ranking at the bottom compared to reference countries.1,7 The US also leads in “excess” mortality; with avoidable deaths worsening three years after the COVID-19 pandemic began despite other countries showing lower mortality.1,8,9
Six Pillars of Comprehensive Lifestyle Change. 1
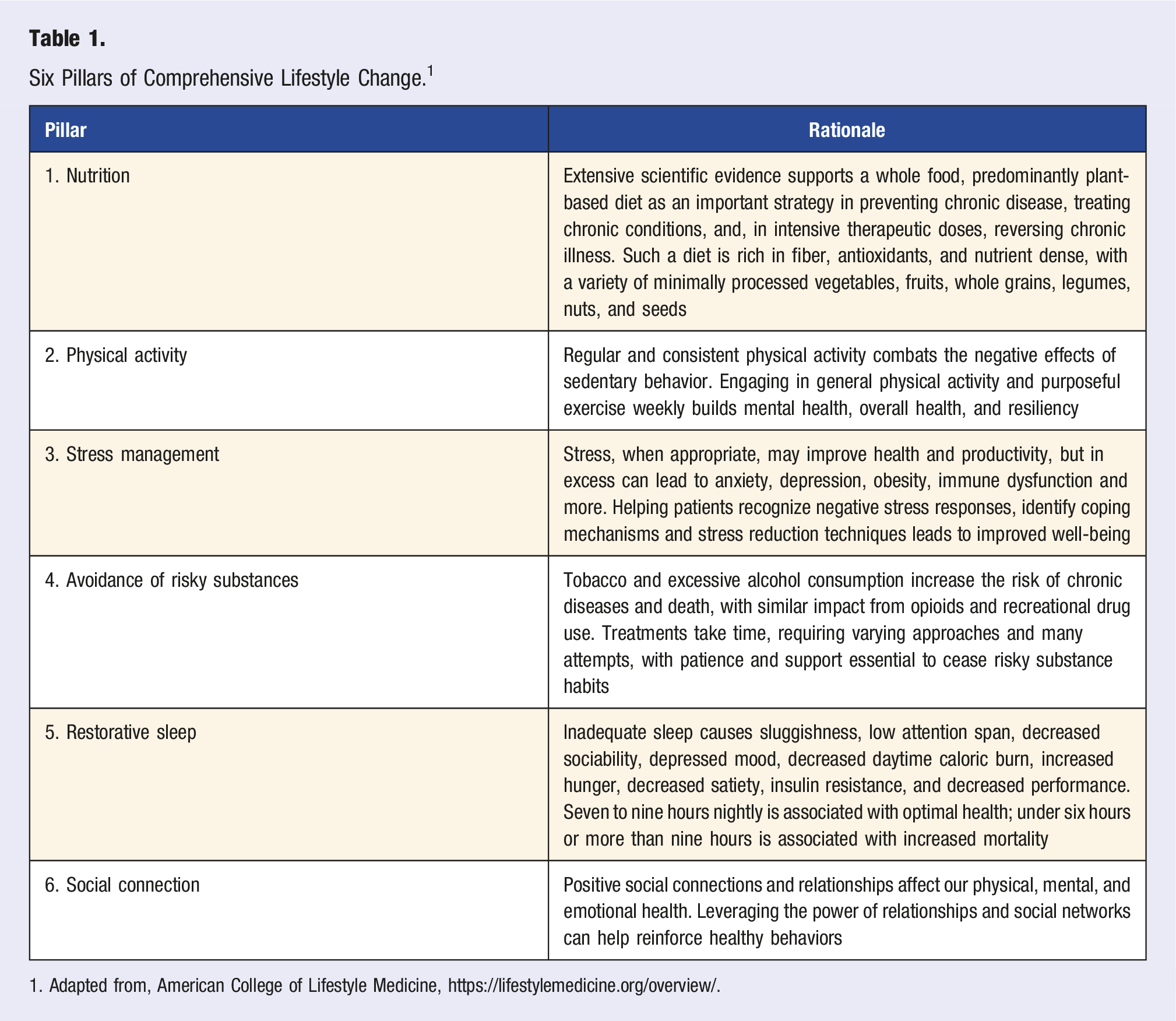
1. Adapted from, American College of Lifestyle Medicine, https://lifestylemedicine.org/overview/.
Ninety percent of health care expenses in the United States are for chronic and mental health conditions. 14 Chronic disease is not only a large part of the US health care problem, constituting approximately 80% of the reasons for medical encounters, but is also rising in prevalence, largely because of lifestyle choices that influence eight of the top ten causes of mortality. 15 For example, cardiovascular disease is the leading cause of mortality in the US, with over 870,000 deaths in 2019 and approximately 125 million Americans living with heart disease or the sequelae of stroke. 16 The prevalence of diabetes is rising, with over 37 million Americans already diagnosed and another 96 million with prediabetes, impacting almost 50% of US adults. 17 About 42% of US adults are obese, almost double the rate in similar nations,1,18 and nearly 74% are overweight or obese, making a healthy lifetime weight uncommon. 19 Adults in the US are also likely to have multiple chronic conditions, with 68% reporting two or more.1,20
Importantly, current clinical practice guidelines for chronic conditions (e.g., hypertension, coronary artery disease, and type 2 diabetes mellitus) often recommend lifestyle changes as first-line or adjuvant treatment to help combat progression and excessive mortality.21–23 Despite these recommendations, health behaviors are not being routinely addressed even in primary care, which is best suited to be highly influential on health behavior change through continuity of care. 24 One reason for this discrepancy is that most clinicians are not adequately trained in lifestyle factors and how to effectively support patients in changing health habits.25,26 Adding to this problem are the time demands inherent in counseling and the lack of reimbursement for evidence-based lifestyle change treatment involving team-based care.
Implementing a LM approach in primary care, where disease risk factors are usually first recognized and chronic disease management is coordinated and continuous, could significantly improve patient outcomes and quality of life. For example, patients could increase life expectancy by up to 13 years by transitioning from a typical “Western Diet,” high in processed foods and animal products, to an “Optimal Diet” with higher intake of whole grains, legumes, fish, fruits, vegetables and nuts, and decreased intake of red and processed meats, sugar-sweetened beverages and refined grains. 27 Similar to dietary changes, adequate physical activity, consisting of only 200 minutes weekly of moderate intensity exercise (e.g., fast walking, easy cycling, hiking, dancing) could decrease mortality risk by 35% in older adults.28–30 Unfortunately, despite robust scientific evidence that beneficial lifestyle choices can prolong the lifespan and health span, relatively few adults are engaged in health-promoting behaviors. 31
To facilitate integrating LM services into primary care, the American College of Lifestyle Medicine (ACLM) convened an expert panel of primary care clinicians from multiple disciplines who also practice lifestyle medicine, including physicians, physician assistants (PAs), nurse practitioners (NPs) and clinical psychologists, to develop consensus statements relevant to LM approaches in a primary care setting. The objective of this expert consensus statement (ECS) was to define best practices for primary care clinicians for integrating LM into the primary care setting to achieve improved outcomes.
Methods
This ECS was developed according to an a priori protocol that has been previously described 32 and used for other ECS publications. 33 Pertinent details of these steps relevant to this ECS are briefly described.
Determination of Lifestyle Medicine Practice Models in Primary Care as the Topic of an ECS and Expert Panel Recruitment and Vetting
The need for an ECS to define essential components of LM practice that could be integrated into primary care and identify current barriers to this integration was based on perceived evidence gaps by ACLM leadership. Despite rapidly growing ACLM membership and board certification in LM by primary care clinicians, there was a clear need for consensus regarding how LM practice could best be integrated into a primary care setting. With this need in mind, the expert panel membership (physicians, NPs, PAs, a clinical psychologist and other professionals who practice LM) was strategically cultivated to ensure appropriate representation of relevant primary care stakeholder groups within ACLM (internal medicine, family medicine, pediatrics, preventive medicine, and behavioral medicine/psychiatry) and in two external groups—The American College of Preventive Medicine and the American Academy of Pediatrics—that accepted and then nominated their representative content experts (KRS and MLB, respectively) to participate.
All expert panel members were in active clinical practice or academic medicine, content experts in implementing LM in patient care, and agreed in advance of the appointment to participate in all verbal discussions (performed via web conference) and votes. Leadership for the ECS included ACLM members serving as chair (MLG), assistant chair (JTS), methodologist (RMR), and primary staff liaison (MCK).
Literature Review and Determination of the Scope of the Consensus Statement
The target audience was primary care providers wanting to integrate LM into their practice. Within this heading, target encounters with patients included both individual and group encounters that focused primarily on lifestyle and those that integrated LM into encounters for other purposes. The target population and setting were all patients encountered in primary care practice. The outcome was to encourage greater uptake of LM practice in primary care by educating clinicians on the unique aspects of LM that can be integrated into primary care to improve clinical results. In defining the scope, the expert panel agreed not to address statements related to using specific assessment tools, intensive therapeutic lifestyle changes, or detailed descriptions of the structure of patient encounters, such as exact duration or frequency of follow-up.
An information specialist helped develop and implement a search strategy to identify all recently published original research related to LM in primary care, including intervention programs, nutrition, or physical activity prescriptions, or shared medical appointments. The search was conducted in four databases: Medline, CINAHL, Embase and Cochrane trials, through September 30, 2022, by two team members (MCK and KS) with oversight from the information specialist. The search was not restricted to human studies, and no language restrictions were applied. Search strategies are presented in Supplementary Tables S1-S4.
After completing all searches, the citations identified, including abstracts, were screened for relevance independently by two team members (MCK and KS) using Rayyan abstract screening software 34 and Endnote. Abstracts were excluded if they were not focused on one of the topics listed (LM, treatment in primary care, including intervention programs, nutrition, or physical activity prescriptions, or shared medical appointments). The expert panel used the results of the literature searches, combined with their experience and perceived stakeholder needs, to propose topics relevant to the goals of the project which were to address controversial clinical issues, reduce variability in care, clarify evidence gaps, or improve quality of care through structured expert consensus. A consolidated list of topic areas was then prioritized by the expert panel used to develop one or more related statements for which consensus would be assessed using the modified Delphi survey method.
Delphi Survey Method Process and Administration
A modified Delphi survey method of three rounds of voting was utilized to assess consensus for the proposed statements, 32 using web-based software (www.QuestionPro.com) to administer confidential surveys to expert panel members. Five virtual meetings in total were conducted, with the third and fourth meetings focusing on deeper discussion of potential statements for revote, including statements of near consensus and selected statements of no consensus that were nonetheless considered important enough to warrant further clarification and consideration. For each Delphi round, the expert panel members rated their agreement, or disagreement, with each of the proposed statements using web-based software and a 9-point Likert scale, ranging from 1 = strongly disagree to 9 = strongly agree.
Criteria for Consensus
The criteria for consensus have been previously defined, and status was numerically calculated for each statement following the Delphi vote as consensus, near consensus, or no consensus. In brief, a statement achieved consensus with a mean score of 7.0 or higher and no more than 1 outlier response, defined as any rating 2 or more points in either direction from the mean score. A near consensus statement had a mean score of 6.5 or higher, with no more than 2 outliers, and a no consensus statement had a mean score below 6.5, more than 2 outliers, or both.
All experts completed all survey items and after each Delphi round the aggregate results were collated and distributed, but individual responses were blinded. The expert panel extensively discussed (via virtual conference) the results of each item after the first Delphi survey. The third iteration of the survey was used to finalize only ten statements which had been determined to merit a revote. The final version of the ECSs were grouped into several specific areas: Integration into Primary Care; Delivery Models; Provider Education; Evidence-Base for Lifestyle Medicine; Diagnosis and Vital Signs; Treatment; Resource Referral and Reimbursement; Patient, Family, and Community Involvement; Shared Decision-Making; Social Determinants of Health and Health Equity; and Barriers to Lifestyle Medicine. Each expert consensus member participated in the drafting and review of the final manuscript.
Results
The formal literature search produced 488 abstracts for screening after removing duplicates. After excluding results without abstracts, 451 results were moved into Rayyan for abstract screening. After abstract screening, 219 articles were identified as potentially relevant, with 28 specifically focused on LM, 72 on shared medical appointments (SMAs), and 68 on physical activity prescriptions. Full-text articles of the 28 specifically focused on LM were provided to the expert panel and included 8 review articles, 6 single-arm or pilot intervention trials, 4 descriptive reports of clinical practice, 4 retrospective studies, 2 case series, 1 randomized controlled trial, 1 cohort study, 1 cross-sectional survey, and 1 qualitative study. Additionally, recommendations or results from manual searching of the most recent, relevant position statements or other guidance documents from the collaborating organizations were reviewed by the panel to inform the process.
The expert panel initially proposed 97 topics as relevant to the ECS, which upon further discussion resulted in 124 statements under the following subtopics: Integration into Primary Care (n = 17); Delivery Models (n = 30); Provider Education(n = 6); Evidence-base for LM (n = 16); Diagnosis and Vital Signs (n = 5); Treatment (n = 21); Resource Referral and Reimbursement (n = 10); Patient, Family, and Community Involvement; Shared Decision-Making (n = 9); Social Determinants of Health and Health Equity (n = 4); and Barriers to Lifestyle Medicine (n = 6).
Integration Into Primary Care: Statements That Reached Consensus.
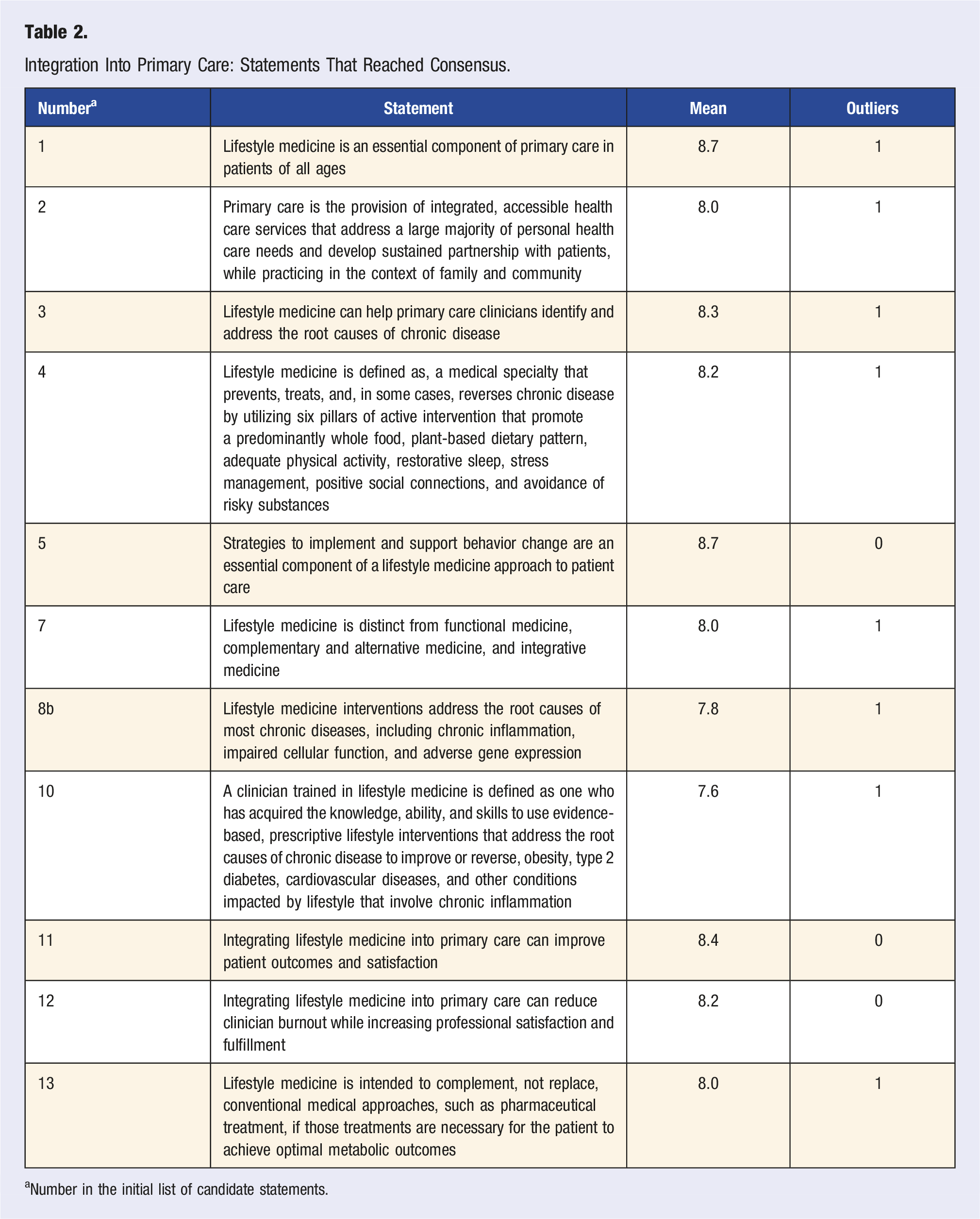
aNumber in the initial list of candidate statements.
Delivery Models: Statements That Reached Consensus.
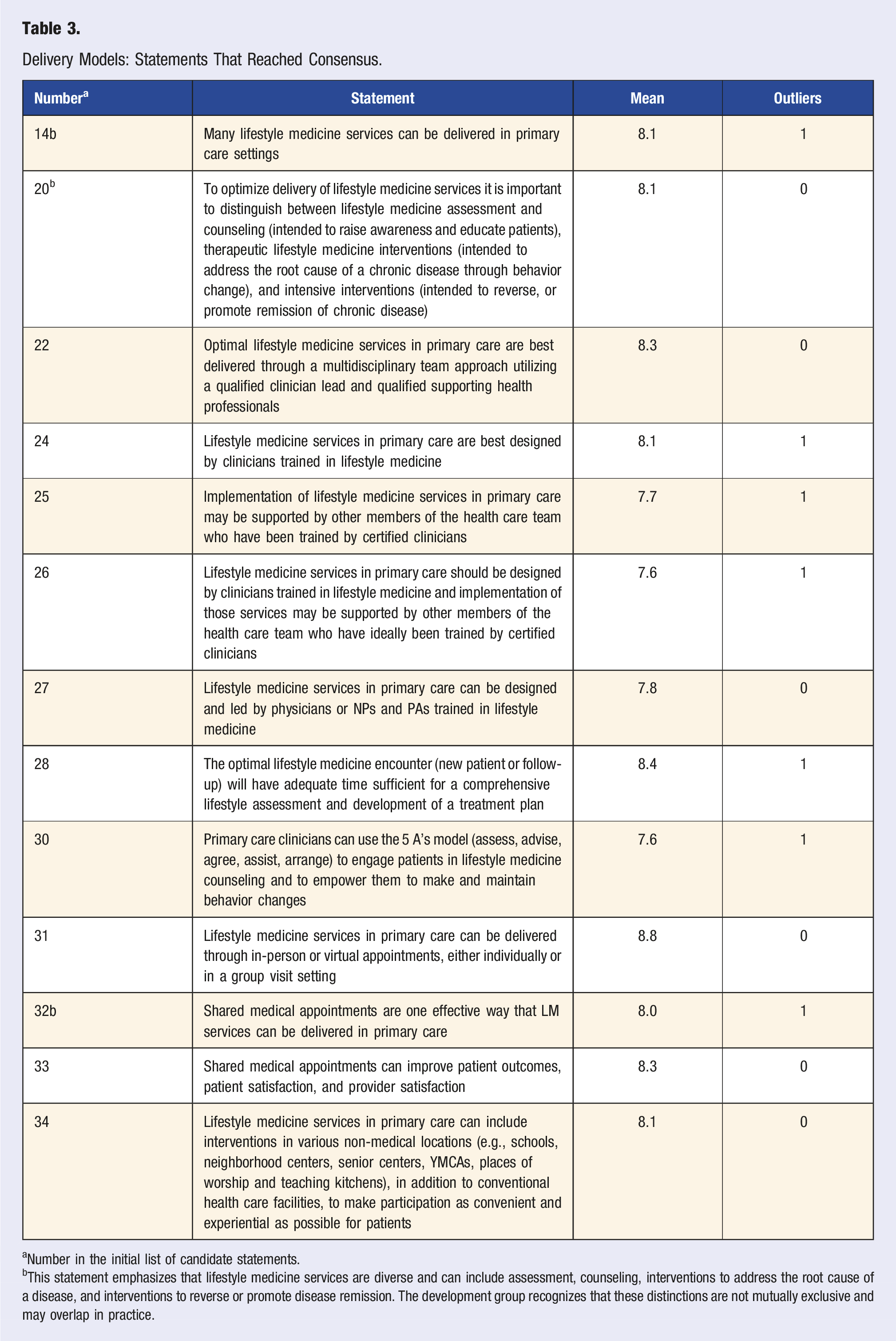
aNumber in the initial list of candidate statements.
bThis statement emphasizes that lifestyle medicine services are diverse and can include assessment, counseling, interventions to address the root cause of a disease, and interventions to reverse or promote disease remission. The development group recognizes that these distinctions are not mutually exclusive and may overlap in practice.
Provider Education: Statements That Reached Consensus.
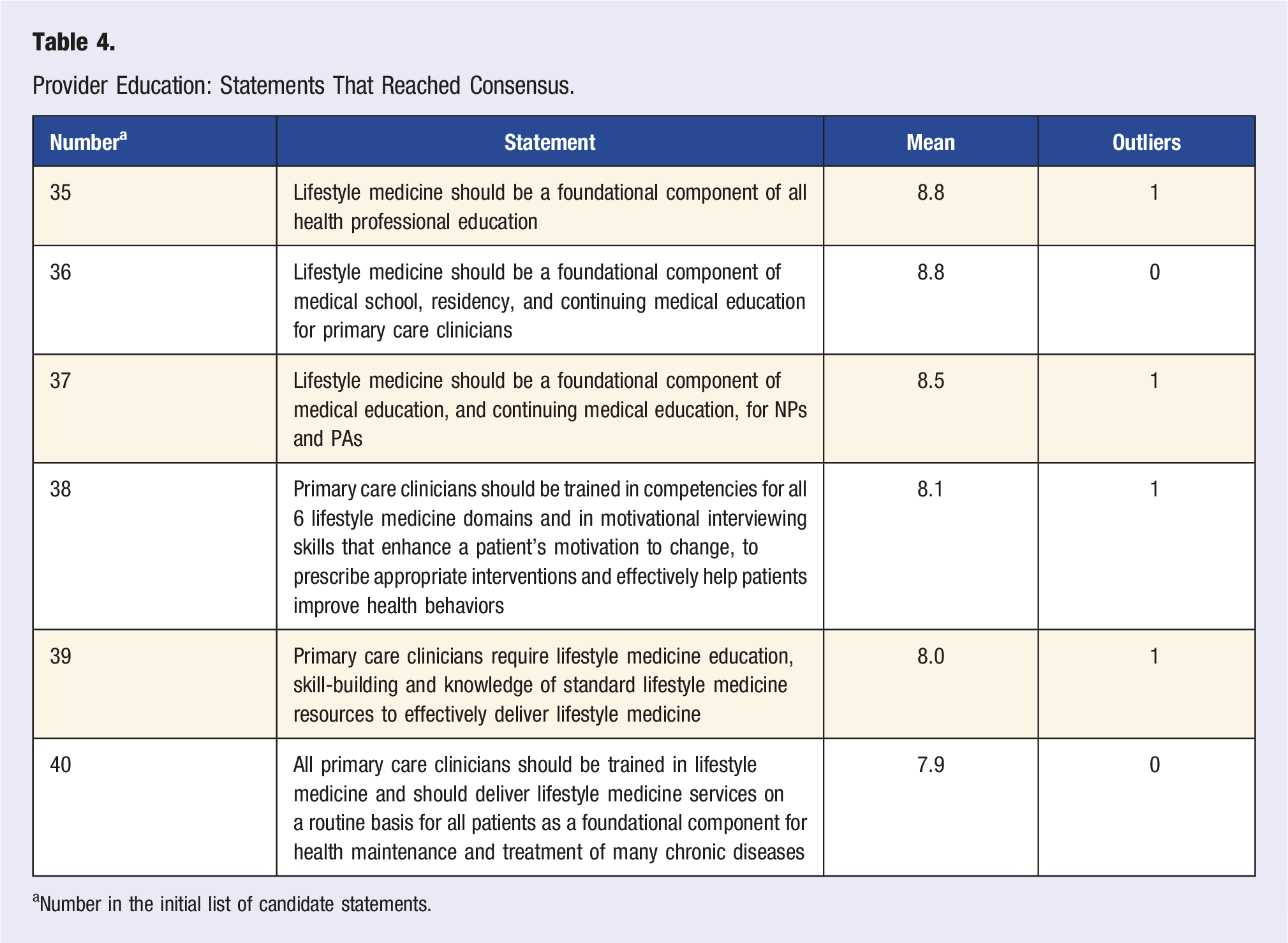
aNumber in the initial list of candidate statements.
Evidence-Base for Lifestyle Medicine: Statements That Reached Consensus.
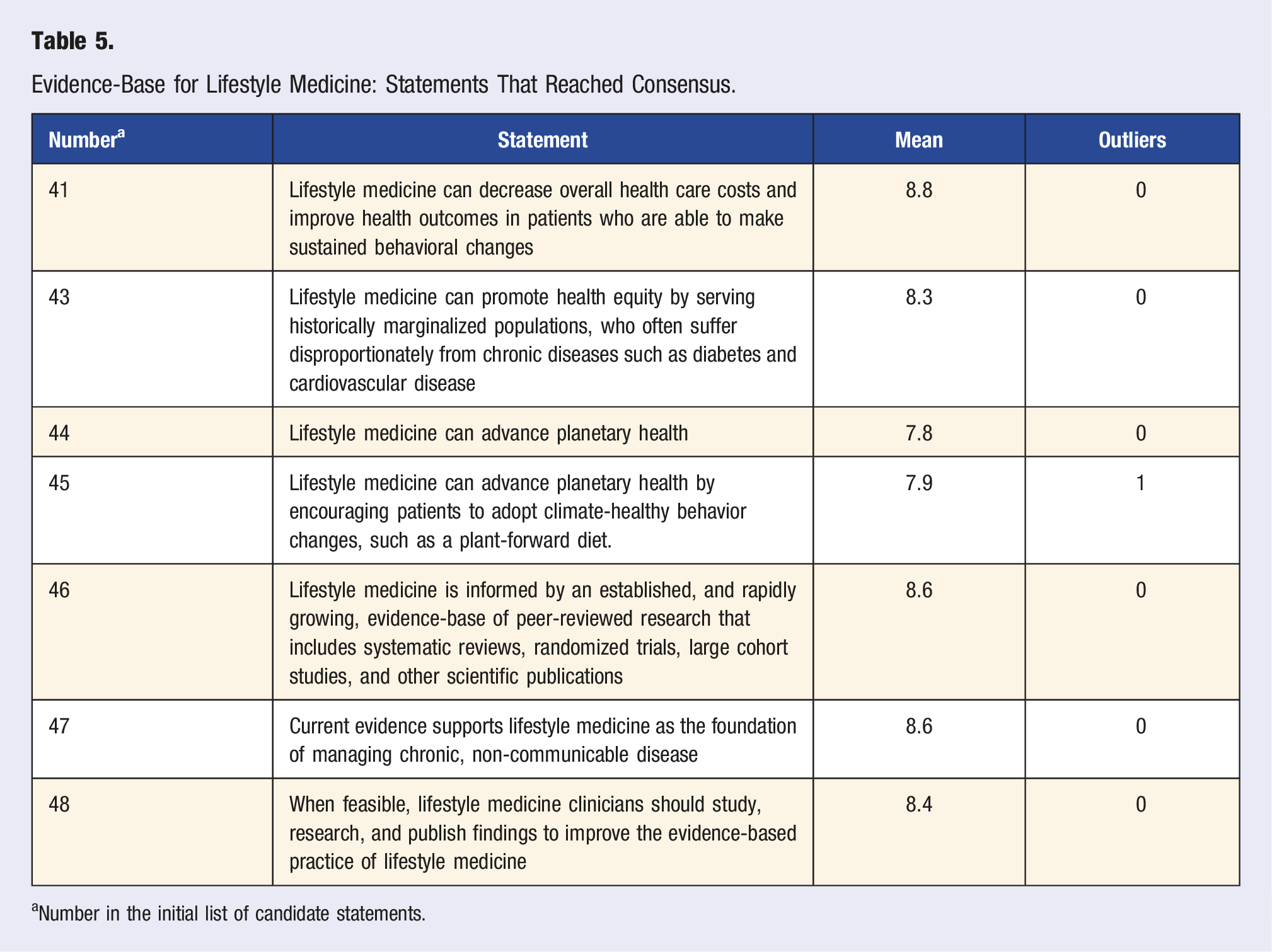
aNumber in the initial list of candidate statements.
Vital Signs: Statements That Reached Consensus.
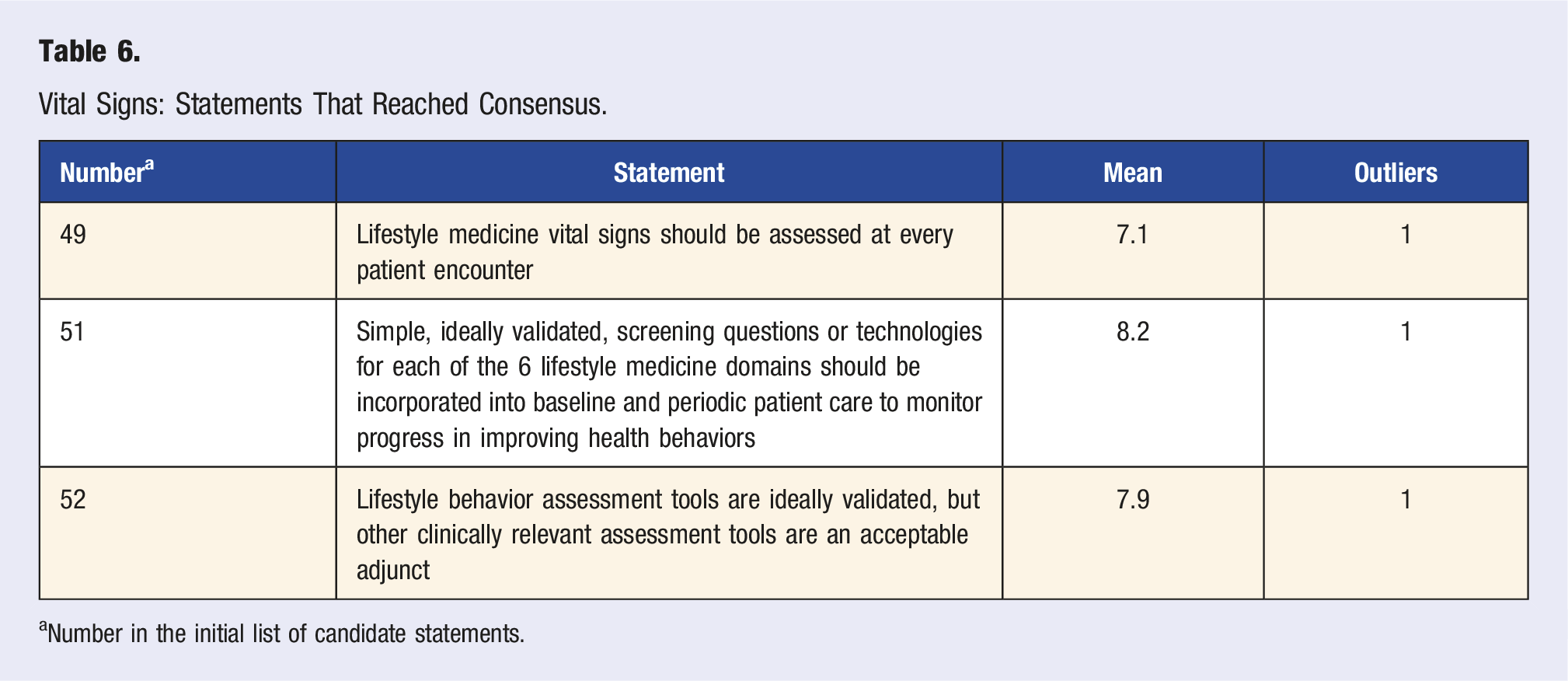
aNumber in the initial list of candidate statements.
Treatment: Statements That Reached Consensus.
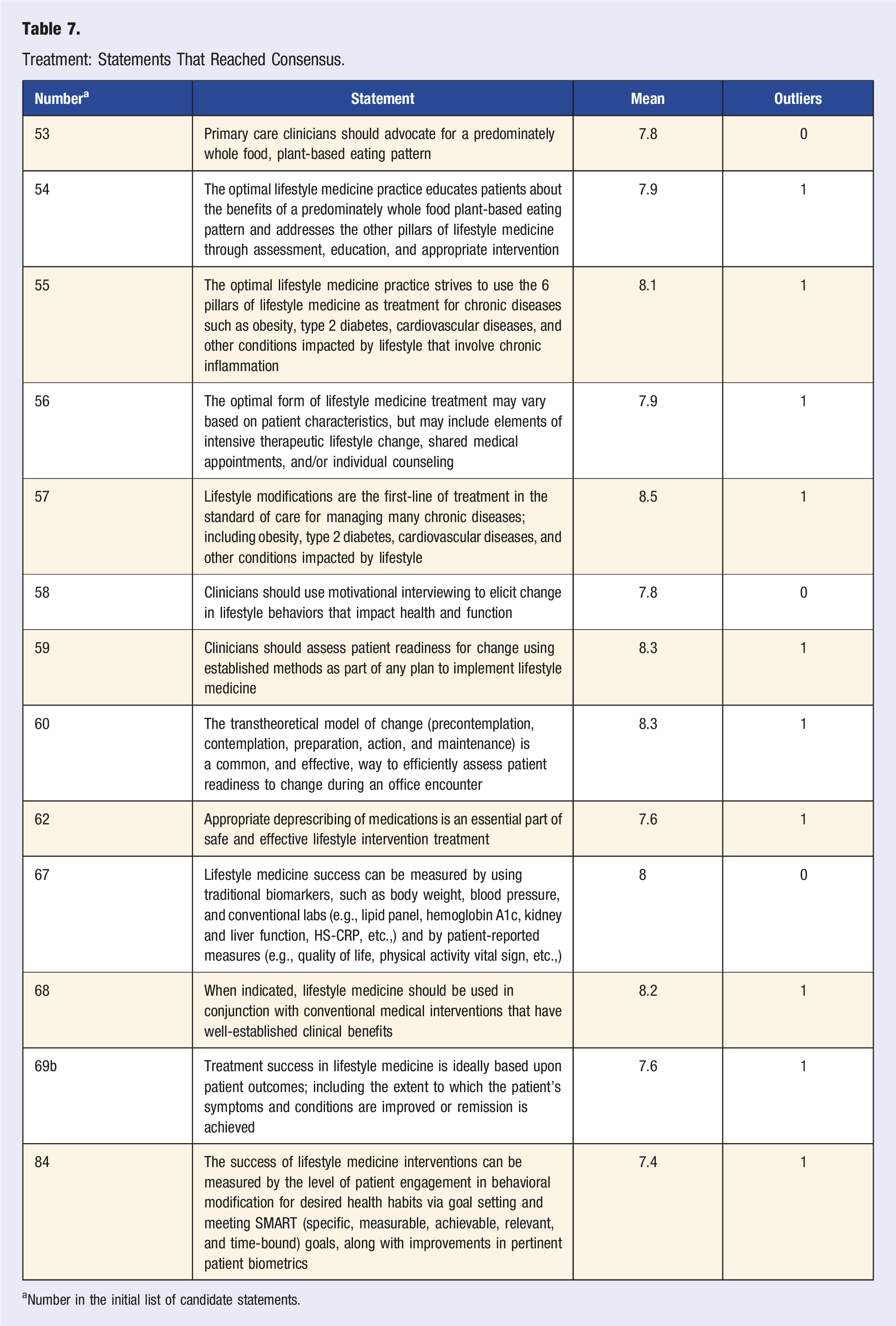
aNumber in the initial list of candidate statements.
Resource Referral and Reimbursement: Statements That Reached Consensus.
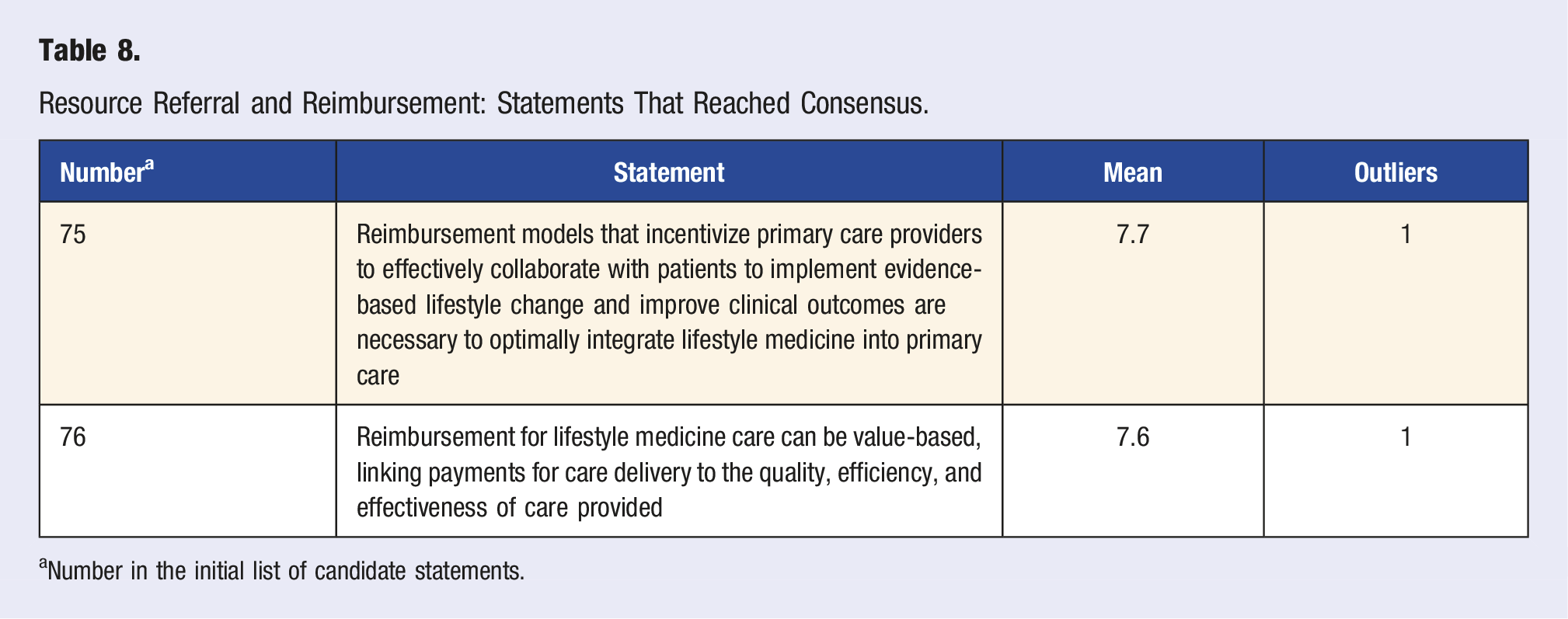
aNumber in the initial list of candidate statements.
Patient, Family and Community Involvement, Shared Decision-Making: Statements That Reached Consensus.
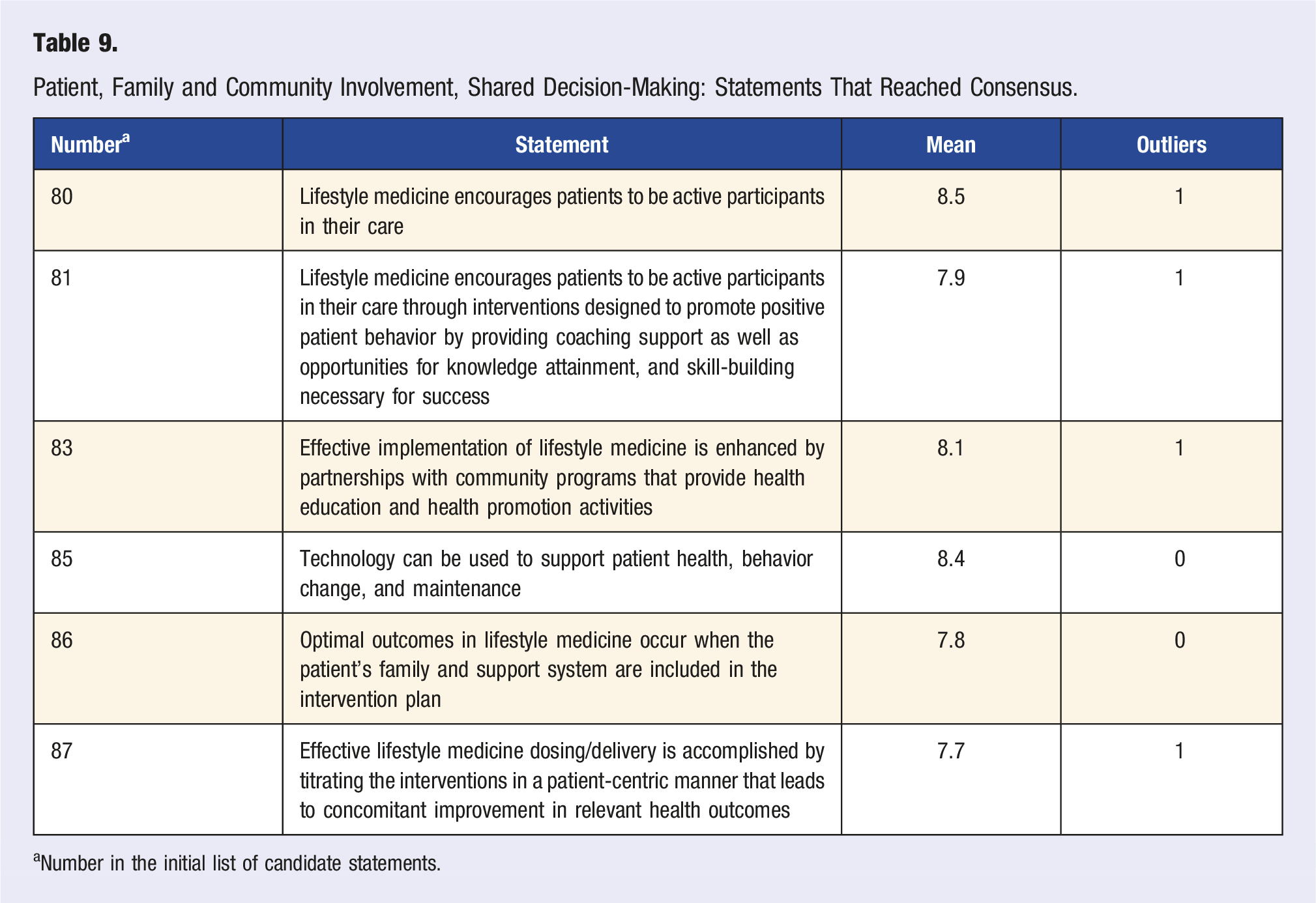
aNumber in the initial list of candidate statements.
Social Determinants of Health and Health Equity: Statements That Reached Consensus.
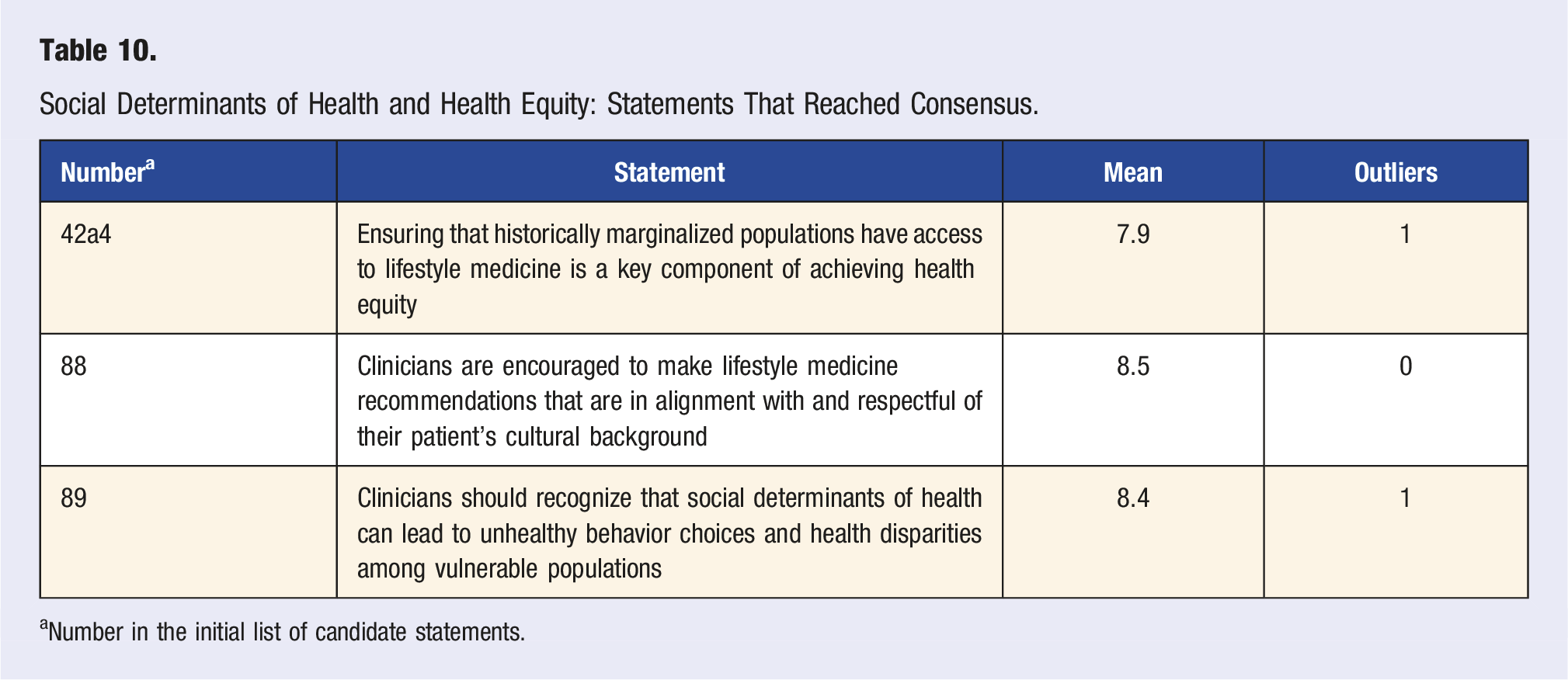
aNumber in the initial list of candidate statements.
Barriers to Lifestyle Medicine: Statement That Reached Consensus.
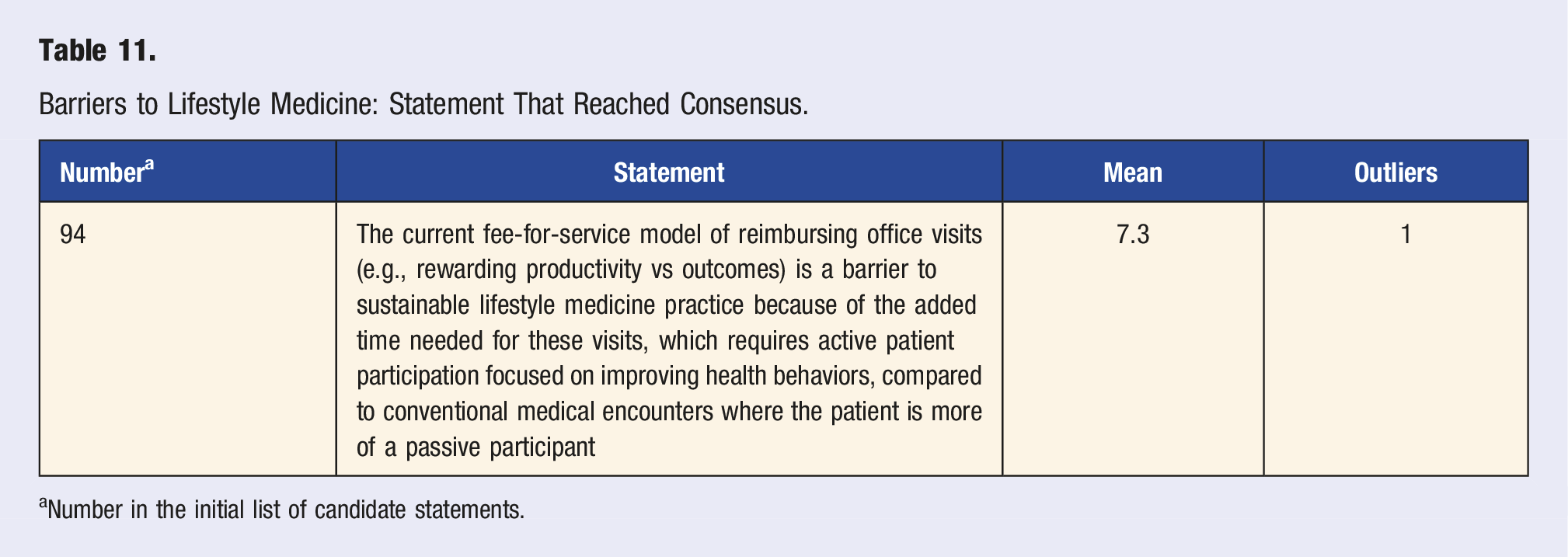
aNumber in the initial list of candidate statements.
Integration of LM into Primary Care
Eleven statements about integrating LM into primary care reached consensus (Table 2). When considered in aggregate, these statements highlight the importance of LM as a medical specialty to primary care clinicians for improving patient outcomes and satisfaction by addressing the root causes of most chronic diseases and implementing strategies to support healthy behavior change. Expert panel members agreed that primary care settings provide vast opportunities to work collaboratively with patients in their communities to promote health care. Additionally, they agreed that by developing knowledge, skills, and abilities through training in LM, primary care clinicians can optimally engage with their patients to prevent, treat, and possibly reverse many chronic diseases and improve satisfaction with care.
Three statements reached near consensus and three statements did not reach consensus (Table S5). Those statements contained themes related to definitions of primary care and LM, and practice considerations related to addressing root causes of chronic diseases, reversing chronic diseases, or both. Expert panel members concluded those statements fell outside its purview, lacked a solid evidence-base, or that other statements that reached consensus better fit within those themes.
Delivery Models
Thirteen statements about LM delivery models in primary care reached consensus (Table 3), nine statements were near consensus, and seven statements did not reach consensus (Table S6). Panel members agreed (Table 3) that many LM services can be delivered in primary care, through individual or group modalities designed and led by LM-trained physicians, NPs, or PAs. Further, the panel reached consensus that the optimal delivery of LM services in primary care includes a multidisciplinary team and adequate encounter time.
The expert panel also agreed on some important aspects of delivering LM services, including a distinction between services intended to raise awareness and educate patients (assessment and counseling), services intended to address the root cause of a chronic disease through behavior change (therapeutic LM intervention), and services provided with sufficient intensity and duration at an appropriate therapeutic dose specifically designed to reverse or promote remission of chronic disease (intensive LM intervention). Appointments for LM services could be in-person or virtual, in an individual or group setting, should empower patients to make and maintain behavior changes, and can include diverse non-medical settings to make participation as convenient and experiential as possible for patients.
Provider Education
All six consensus statements regarding provider education reached consensus (Table 4). The statements focused on the foundational role of LM in health education and training for physicians, PAs, NPs, and other members of the health care team. The consensus on statements related to education was very strong, ranging from 8.5 to 8.8 on a Likert scale with a maximum 9.0 response. Additional consensus noted that this education ideally occurs throughout the learning continuum, including schooling, training, and continuing education. All six domains of LM (Table 1) were agreed upon as being important in this regard, as are motivational interviewing skills for behavior change. There was consensus that optimal provider education teaches LM as the foundation of chronic disease prevention and treatment.
Evidence-Base for Lifestyle Medicine
Seven statements reached consensus regarding the evidence-base for LM (Table 5). Three statements reached near consensus, and five statements did not reach consensus (Table S7). Consensus was reached on LM’s ability to decrease health care costs and improve health care outcomes through patients’ adoption of sustained behavior changes and to improve planetary health with beneficial health behaviors such as plant-forward eating patterns. Consensus was also reached that serving historically marginalized populations who suffer disproportionately from chronic disease can promote health equity, and that ensuring access to LM for these population is a key component of achieving health equity. The expert panel also agreed that current evidence supports LM as the foundation of care for chronic disease, that LM is informed by an established and rapidly growing body of evidence from peer-reviewed research, and that when feasible, LM clinicians should conduct additional research to improve evidence-based practice of LM.
Vital Signs
Three statements about LM “vital signs” and assessments reached consensus (Table 6). In this context, a LM vital sign refers to using a survey, questionnaire, or other measure to determine where a given patient falls on the spectrum of adherence to each of the 6 LM pillars. One statement reached near consensus, and one statement did not reach consensus (Table S8). Expert panel members agreed that lifestyle behavior vital signs should be assessed at every patient encounter, while screening questions or assessments for each of the six LM domains should be included at baseline and repeated periodically to monitor progress over time. Ideally, these tools should be simple and validated; however, other clinically relevant tools were deemed acceptable adjuncts.
Treatment
Thirteen statements about LM treatment reached consensus (Table 7), three statements reached near consensus, and six statements did not reach consensus (Table S9). There was consensus that an optimal LM practice should incorporate the 6 pillars of LM as first-line treatment of chronic conditions that are affected by lifestyle, including advocacy for a predominantly whole food, plant-based eating pattern. There was consensus on the importance of deprescribing medications in successful LM treatment; however, the optimal step-down practices for deprescription only reached near consensus. The expert panel agreed that clinicians should use established methods, such as the transtheoretical model and motivational interviewing, to assess and treat patients in LM practice. Two statements about measuring treatment success of LM interventions reached consensus.
Resource Referral and Reimbursement
Two statements involving reimbursement for LM services in primary care reached consensus (Table 8). Expert panel members agreed that reimbursement issues are currently an obstacle for many clinicians in their quest to integrate LM services into primary care, with lack of sustainable reimbursement a substantial disincentive; and that incentivizing primary care clinicians to effectively collaborate with patients in supporting health-promoting behavior change is critical for optimizing clinical outcomes through a LM approach. Additionally, the panel recognized that a value-based care reimbursement model can support effective delivery of LM interventions in primary care if the evaluation metrics are selected to sustainably compensate clinical outcomes, as opposed to process measures.
Two statements regarding resource referral or reimbursement reached near consensus, and six statements were classified as no consensus (Table S10). Many of these statements contained references to Intensive Therapeutic Lifestyle Change (ITLC) interventions, regarding which the experts had robust discussion on what elements specifically constitute ITLC, what level of training is necessary to provide ITLC services, what clinical parameters suggest a need for referral to an ITLC program, in what setting is ITLC best delivered and whether ITLC interventions could be considered a part of primary care. These concepts represent currently unresolved questions in the field of LM and will be best addressed by future research and expert consensus projects.
The remaining statements that did not reach consensus centered on the perceived scarcity of sustainable reimbursement models for LM services. For example, many panel members were hesitant to agree that SMAs were cost-efficient under the current fee-for-service (FFS) model; despite acknowledging that SMAs are an effective tool for patient education and supporting behavior change. Additionally, statements on whether a capitated reimbursement model could successfully support LM integration into primary care, optimal staffing models for financial viability in a fee-for-service system and whether LM that also necessarily addresses social determinants of health is essential for the financial success of organizations that are transitioning to a value-based care model did not reach consensus.
Patient, Family, and Community Involvement; Shared Decision-Making
Six statements about patient, family and community involvement, and shared decision-making reached consensus (Table 9). Expert panel members agreed that LM encourages patients to be active participants in their care, and that implementing LM can be achieved and enhanced through partnerships with community programs. Furthermore, technology and family support can also facilitate behavior change and maintenance, while patient-centric delivery and dosing in a titrated manner leads to improvement in health outcomes. The remaining two statements addressing patient, family and community involvement, and shared decision-making reached near consensus (Table S11). Expert panel members differed on how shared decision-making is best accomplished.
Social Determinants of Health and Health Equity
Three statements regarding social determinants of health and health equity reached consensus (Table 10), one reached near consensus, and one did not achieve consensus (Table S12). Of the three statements that reached consensus, one was unanimous and the other two had only one outlier. The expert panel agreed that LM can improve health equity by ensuring that access includes historically marginalized populations who suffer disproportionately from chronic disease. In addition, consensus was reached on the importance of clinicians recognizing that social determinants of health can be a factor in disparate access to care and resources which can hinder healthy behaviors and may in turn lead to further increases in health disparities. The expert panel also agreed that LM recommendations should be respectful of and in alignment with the patient’s cultural background.
Barriers to Lifestyle Medicine
Only one statement about barriers to LM practice reached consensus (Table 11). All other statements within this category (n = 6) did not achieve consensus (Table S13). Expert panel members agreed that the current FFS model was a barrier to practicing sustainable LM. They noted that having longer visits to engage patients in health behavior change was financially disincentivized in the FFS model.
Discussion
This ECS is the first publication to identify best practices for integrating LM into primary care, drawing from experience of multidisciplinary experts using a validated and well-established process for assessing consensus, near consensus, and no consensus on key issues. Despite the diverse backgrounds and clinical settings of the expert panel, we achieved consensus for 65 statements reflecting the core belief that LM is the foundation of health care education, training, and practice. Moreover, implementing LM in primary care settings benefits providers and patients by identifying the root causes of many chronic diseases that may be prevented, managed, or even reversed using lifestyle interventions coupled with proactive strategies for healthy behavior change. In the remainder of this section, we add nuance to the consensus statements by discussing their relevance to everyday clinical care and their pragmatic implementation into practice settings.
Integration of LM into Primary Care
Through sustained partnerships with patients, families, and communities, primary care clinicians are well-positioned within an integrated health care setting to treat chronic disease by incorporating LM into everyday care. LM may have added relevance to diseases involving chronic inflammation, impaired cellular function, and adverse gene expression. LM should complement, not replace, conventional medicine; and is distinct from functional medicine, integrative medicine, and alternative medicine. By developing the knowledge, ability, and skills to identify root causes of chronic disease (i.e., unhealthy eating, physical inactivity, inadequate sleep, unmanaged stress, lack of social connection, and use of risky substances), primary care clinicians trained in LM are best positioned to apply evidence-based interventions that engage, empower, and support patients of all ages. In doing so, they can prevent, treat, and potentially reverse chronic disease to improve patient outcomes and satisfaction.
Primary care clinicians and patients are receptive towards addressing behaviors associated with health such as nutrition, physical activity, and unhealthy substance use, and patients benefit from prescriptive support; however, clinicians often lack the specific knowledge or time to provide this care. 35 Advancing LM within primary care may require innovative thinking about how and by whom health care is delivered, clinician competencies, patient engagement, the time and structure of patient visits, and models for reimbursement.36,37
Delivery Models
Despite multiple studies showing that many LM services can be implemented successfully in primary care settings,38–41 the expert panel members could not agree on a specific delivery model for implementing LM routinely in everyday primary care settings. This lack of consensus was partly driven by the current lack of high-quality studies available to guide evidence-based implementation. 42 Further, expert panel members discussed that, despite having the requisite clinical skills, effective delivery of LM interventions in the primary care setting is disadvantaged by the lack of administrative support, time constraints during patient visits, and inadequate financial reimbursement. These limitations are intimately related to the current financial structure of the US health care system that incentivizes “sick care” rather than health care, including performance measures that would disincentivize disease reversal.43,44 Accountable care organizations, direct primary care, chronic care management, and medical homes are existing delivery and payment models that better align with the principles of value-based care, which support the necessary infrastructure to deliver valuable primary care that is enhanced by LM.
Although health care reform may be imperative to improve patient outcomes, the expert panel did not agree that enhancing primary care support with additional resources is required to begin integrating LM into routine patient care. Primary care clinicians could, for example, collaborate with patients to develop individualized nutrition prescriptions or create a self-management plan using the 5 A’s model (Assess, Advise, Agree, Assist, Arrange). 45 LM services in primary care can be delivered through individual or group appointments via in-person visits, virtual platforms, or at non-medical locations such as schools, community centers, work sites or teaching kitchens. SMAs are also a clinically effective model for delivery of LM services in primary care, based on their ability to improve outcomes for obesity, cardiovascular risk factors, type 2 diabetes mellitus, heart failure, and chronic pain.38,46–50 SMAs can improve outcomes and reduce cost in specific populations, but data are limited in primary care settings and further research is required to confidently generalize results these settings.46,51,52
The expert panel members agreed that LM interventions in primary care are best designed and led by physicians, NPs, or PAs trained in LM. Certification through the American Board of Lifestyle Medicine (ABLM) or ACLM is beneficial for clinicians who wish to provide LM services. LM services are optimally delivered through a multidisciplinary team approach 39 and by selecting an appropriate intervention intensity (i.e., dose) for each patient. The intensity of the prescribed intervention can be determined by assessing patient disease severity and factors that affect the patient’s ability to implement lifestyle change such as readiness to change, biopsychosocial factors, and social determinants of health, among others. 53 The expert panel was unable to reach consensus regarding whether high-dose (i.e., intensive) LM interventions can be effectively delivered in the primary care setting or if patients should be referred to a specialty LM setting instead.
Provider Education
The consensus statements regarding LM as a foundation of all health care suggest a need to incorporate LM into all health care professionals’ training and continuing education. There is encouraging momentum to implement LM into medical training, but much more is needed for the practice of LM to become mainstream. 54 At least four medical schools have incorporated LM-specific training at the undergraduate level. 54 Undergraduate medical education competencies for LM were developed and published in 2021. 55
Some of the challenges of including LM in medical school education include a “lack of awareness of the efficacy of LM, lack of time to implement, and lack of standardized curriculum.” 54 At the post graduate level, among residencies, the Public Health and General Preventive Medicine specialty incorporated an Accreditation Council for Graduate Medical Education (ACGME) milestone on LM in July 2022, meaning all residents in this specialty will be evaluated on this competency. 56 The Lifestyle Medicine Residency Curriculum (LMRC) is a joint effort by Loma Linda University Health and the ACLM to fill LM gaps in any specialty’s residency training. Most of the residency programs that have adopted the LMRC are primary care specialties, but LM applies to most, if not all, non-primary care specialties as well.
Next steps could include incorporating LM knowledge on NBME board examinations for medical students and residents. Another option would be to include LM education as part of the core competencies for residency accreditation by the ACGME. Educating current and future primary care providers in LM is of vital importance for reducing the rising prevalence of chronic disease and for optimizing patient health outcomes.
Evidence-Base for Lifestyle Medicine
In addition to the rapid growth of LM as a medical specialty and a concurrent interest in provider certification, the evidence-base that underpins the value and efficacy of LM is growing rapidly. 57 In March 2023, 951 results containing the term “lifestyle medicine” were found in PubMed, as compared to only 296 results by the end of 2017. Of these 951, over 80 are original research, such as intervention trials or randomized controlled trials, observational cohort studies, case series, or meta-analyses. The rapid growth in basic science and clinical research relating to LM led to the Lifestyle Medicine Research Summit in 2019, 58 which advanced our understanding of how the six domains of LM affect epigenetics, microbiome, neuroplasticity, cellular dysbiosis, and the core pathogenetic process of inflammatory-related chronic diseases, thereby providing compelling evidence that LM can prevent, treat, and reverse chronic diseases. 58 LM domain-specific research priorities defined focus areas for LM practitioners to study and publish to further advance healthy behaviors and supportive environments as the foundation of care. 58
Individuals who sustain healthy behavior change(s) improve clinical and health care cost outcomes.59–64 Unhealthy behaviors and the environments that reinforce them are disproportionately observed in historically marginalized populations. As such, LM can address these needs when approaches are culturally tailored and inclusive of social determinants of health.59,65,66
Evidence is also emerging that highlights improved adherence and better outcomes when coaching is prescribed by clinicians. In one integrated coaching model with prescriptions embedded in the electronic medical record at a large health system in the northeast US, a nearly a 10-fold greater engagement and completion of behavior change programs were observed when prescribed by provider vs traditional outreach from the health plan. 67 These improvements in adherence, health outcomes, and cost of care can also extend to planetary health. As one of the six domains of LM is the use of a whole food, predominantly plant-based diet, the expert panel discussed improving planetary health through the reduction of greenhouse gasses, which is associated with less consumption of red meat and ultra-processed foods. 68
Vital Signs
The crux of successful LM treatment is sustained patient health behavior change. Having methods to measure and track patient progress over time is critical for facilitating this process. Vital signs are measured at every visit, as they are considered essential to the care of a patient. The concept of LM vital signs was introduced to emphasize the importance of evaluating lifestyle factors. The ideal duration and frequency of administration is not known for many of the currently available tools, though they should be performed when clinically relevant (i.e., at baseline and monitored periodically as needed to track progress over time).
LM vital signs have been discussed for many years, though universal agreement has not been achieved on what these metrics contain. The only broadly recognized LM-specific vital sign is the Physical Activity Vital Sign, 69 a validated, three question tool that can quickly assess a patient’s weekly minutes of physical activity and number of resistance training sessions. Capturing these data 1) emphasizes the importance of physical activity to the health care team and the patient, 2) allows for a comparison to current physical activity guidelines, 3) creates an opportunity to discuss physical activity and its impact on health, and 4) can serve as the basis to co-create a SMART (specific, measurable, achievable, relevant, and time-based) goal that improves this health metric.
Validated short and long questionnaires/screening tools exist for all pillars of LM (i.e., Nutrition-Starting the Conversation, Physical Activity-International Physical Activity Questionnaire, Sleep-Single Item Sleep Questionnaire, Stress-Perceived Stress Scale, Social Support-A Brief Measure of Social Support, Substance Use-NIDA Quick Screen).70–74 Validated tools are preferred, as they typically have been studied and confirmed to be accurate reflections of the information they are gathering and may also relate to a health outcome of interest. However, there was recognition amongst the expert panel members that current validated tools are not necessarily LM-specific and may not provide the sensitivity or responsiveness necessary for engaging in effective conversations regarding behavior change prescriptions. For this reason, it was felt that other clinical tools, such as the Lifestyle Medicine Assessment, could be acceptable adjuncts to assessing lifestyle behaviors. 75
Regardless of the questionnaires or assessments utilized, having consistent ways to measure and track patient lifestyle behavior change over time is critical to ensure that the patient is receiving optimal LM dosing that can achieve the desired health outcomes. Further research focused on validation of LM-specific assessments and screening tools will be a beneficial adjunct to the currently available options for LM clinicians.
Treatment
Most clinical experts recommend lifestyle changes as first-line or adjuvant interventions when approaching chronic conditions such as cardiovascular disease, 76 obesity, 77 or other chronic disease. 78 Our expert panel agreed that LM provides a structured approach in treating lifestyle-related chronic disease with an emphasis on its 6 pillars (Table 1), with special emphasis on recommending a predominantly whole food plant-based eating pattern. Motivational interviewing techniques and assessing readiness for change were highlighted as efficient and effective tools that provide a framework for clinicians to follow the guidelines and positively impact their patients’ lives. 79 The expert panel further agreed that these changes can be achieved through SMAs, intensive lifestyle change interventions, or individual counseling. The approach should be individualized; and while some of these options may not be conventional, they have been shown to be effective in achieving improved patient outcomes.80,81
Expert panel members discussed the importance of pharmaceutical deprescribing, when appropriate, within optimal LM practice given the pervasive challenge of polypharmacy and the frequently rapid improvement in biometric parameters such as blood pressure and blood sugar when transitioning to beneficial lifestyle behaviors. However, this responsibility may be shared by other medical disciplines. Further study is required to determine the ideal approach to medication de-escalation or deprescription for many chronic conditions; as such, panelists were not able to come to consensus about best deprescription practices, but were agreed that deprescribing is essential when lifestyle changes result in overmedication of a patient.
Behavior change is one of the most important aspects of LM. There was substantial discussion and agreement that assessing patient readiness for change and using tools such as motivational interviewing are important strategies to promote health behavior change. 82 Patient-focused collaborative approaches to behavior change that recognize patients’ goals have been shown to be a powerful strategy for increasing the effectiveness of a clinician’s interventions. 83
While patient engagement and improvement are impactful, disease remission is one of the most powerful outcomes. Clinical trials have been published on disease reversal through lifestyle modification; however, more research is needed in this area.13,84,85 The topic of ITLC generated substantial discussion. Although consensus was not reached regarding various aspects of ITLC, panel members generally felt that intensive LM interventions can reverse some chronic conditions.
Resource Referral and Reimbursement
LM interventions for chronic disease treatment and reversal are effective in diverse settings, often out-performing results delivered by standard of care approaches.86–89 In contrast, sustainable reimbursement for LM services has been challenging to achieve. A 2018 survey of members of the ACLM revealed that 57% of respondents were not compensated for LM services in clinical care. In addition, for the 42% who were being compensated for the LM services the majority reported direct cash payment as a fundamental component of their reimbursement strategy. 90 A more extensive cross-sectional survey in 2021 found similar results, with 55% of respondents reporting being unable to obtain reimbursement for their LM services. This survey identified reimbursement challenges, including those related to spending more time with patients and payment for the extended care team, as primary obstacles to providing LM services. 91
Our expert panel members agreed that reimbursement issues pertaining to LM services are one of the principal challenges impeding the implementation of this approach. There was strong consensus supporting the need for reimbursement models that incentivize effective collaboration with patients to implement evidence-based lifestyle change as a necessary step for successfully integrating LM into primary care. The expert panel also agreed that a value-based care model could be an effective path for reimbursement of LM services, if the metrics selected for evaluation of value calculation emphasize patient outcomes over process measures. The remaining statements pertaining to reimbursement did not reach consensus, highlighting the lack of agreement among the panel regarding what reimbursement models are effective for sustaining a LM approach in clinical practice. The current FFS model was identified as being specifically challenging to navigate.
The expert panel was unable to come to consensus regarding the cost-effectiveness of SMAs under a FFS model, despite agreement that SMAs are an efficient and effective approach for providing patient education, group support and facilitating behavior change. This assessment aligns with survey results of LM practitioners demonstrating that 59% of respondents reported difficulty achieving sufficient reimbursement from SMAs due to the unpredictability of adequately filling the group visit during normal operating hours of operation and the challenge of obtaining compensation for services provided in non-healthcare community settings, which despite being more convenient for patients lack an NPI number for reimbursement. 91 Some clinicians successfully provide LM services in the FFS model using standard evaluation and management billing codes (99202-99215), chronic care management (CCM) and remote patient monitoring (RPM) codes and a multidisciplinary care team utilizing several billable provider types (physician, NP, PA, RDN, PT/OT, licensed behavioral counselor), including SMAs.90,92 However, alternative payment models that adequately reimburse the time-intensive, comprehensive approach to supporting health behavior change that is necessary to achieve an optimal therapeutic dose leading to improve clinical outcomes are desperately needed to accelerate the integration of LM into primary care.
Regarding referral resources, LM is most effective when implemented as a team-based approach. 93 The team may include physicians, NPs, PAs, registered dieticians, physical and occupational therapists, licensed behavioral counselors, fitness professionals, pharmacists and health coaches. Team members may all practice in the same location or they may be part of a referral network to provide all the services inherent in a LM approach to patient care.
A topic of considerable discussion and debate amongst the expert panel members was the appropriate use of ITLC interventions; specifically, regarding what elements constitute ITLC, what level of training is necessary to provide ITLC services, under what clinical circumstances a referral to an ITLC program is warranted, in what setting is ITLC best delivered and whether ITLC interventions could be considered a part of primary care. ITLC programs have been previously defined in the literature as an evidence-based, multi-modal intervention that includes multiple sessions (usually 8 to 20) for at least 60 minutes per session and a duration of 10 days or longer. 94 However, as the field of LM has continued to advance, including the addition of board certification through the ABLM for physicians, a specialty certification for Lifestyle Medicine Intensivists and an educational pathway for ABLM board-eligibility for US medical residents, the optimal definition of an ITLC intervention and who is qualified to provide it have been targeted for further clarification. The expert panel members were unable to agree regarding these currently unresolved concepts in the field of LM but remain confident that they will be addressed by future research and expert consensus projects.
Patient, Family, and Community Involvement; Shared Decision-Making
Health behavior change, which is integral to preventing and treating most chronic diseases, is best achieved and most effective for patients when their family, community and support systems are involved.36,95,96 Furthermore, community-based programs have the potential to tailor interventions, so they are relevant and effective for an individual community. 97 Digital health technologies have also been used to promote knowledge and build skills necessary for successful patient health outcomes and can be incorporated across diverse populations. 98
LM in primary care is uniquely equipped to address patient needs through collaboratively working with patients, families, and local communities. Primary care clinicians have opportunities to engage patients in their care and continuously support them as they develop the knowledge and skills to improve their health. Consensus was reached that LM encourages patient-centered care, and optimal models to achieve this in primary care involve the patient, family, community partnerships, and digital resources. The expert panel members acknowledged that determining the ideal shared decision-making approach to integrate patients, families, and local communities is best achieved through individual clinician expertise that considers the specific patient population being served.
Social Determinants of Health and Health Equity
The Center for Disease Control and Prevention defines health equity as “when everyone has the opportunity to ‘attain their full health potential’ and no one is ‘disadvantaged from achieving this potential because of their social position or other socially determined circumstance’.” 99 Health equity has also been defined as “the absence of systematic disparities in health (or in the major social determinants of health) between groups with different levels of underlying social advantage/disadvantage—that is, wealth, power, or prestige.” 100 Social determinants of health are underlying societal constructs or factors that contribute to health inequities. Examples include racism, poverty, poor access to health care, lack of education and low health literacy. There is a growing recognition that health outcomes are more impacted by zip code than genetic code. 101 Other factors that portend greater obstacles to health include religion, sexual orientation, gender identity, mental health, and physical ability. These factors lead to preventable differences in health status due to discrimination or exclusion. 102
There was expert panel consensus on the importance of addressing social determinants of health, and ensuring that lifestyle medicine recommendations are in alignment with and respectful of the patient’s cultural background. The need for policy interventions to address upstream factors is supported by a growing body of research. 103 The majority of the expert panel agreed that advocacy for addressing social determinants of health should be considered a part of LM, but also felt strongly that advocacy efforts are a responsibility of all medical specialties and all components of health care, not specific to LM alone.
The National Cancer Institute’s guide for health promotion practice reviews the ecological model of health. The ecological model of health looks at multiple factors that influence healthy behavior. LM strives to address the factors that influence health behavior in a personalized fashion; however, consensus was not reached regarding including the ecological model of health. 104
Combined primary care and community-based programs that are in alignment with and respectful of patient’s cultural backgrounds can improve health by increasing health literacy and access to resources such as healthy food.105,106 As such, clinicians are encouraged to work closely with their patients to make lifestyle recommendations that are individualized and in alignment with the patient’s goals and cultural background. This personalized approach to medicine is based on open communication, respect, and recognition of the strengths and resources in all individuals and communities.
Barriers to Lifestyle Medicine
Achieving equitable reimbursement for the value LM practice provides has been challenging in the FFS model. LM services focus on partnering with patients to engage, empower, and facilitate health behavior change. However, the FFS model incentivizes patient volume (number of visits and procedures) over value (improved clinical outcomes at lower cost). This misalignment in patient, provider, and payer preferences has likely hindered both the adoption, delivery, and effectiveness of LM services within primary care.
One study of ACLM members found that 25% do not provide LM services. Over half of the members who reported providing LM services said they did so without receiving compensation for that care. 90 This reality has led to LM physicians, NPs and PAs seeking alternative reimbursement models, such as direct primary care, concierge medicine, or cash practices that better align incentives for all parties. Presumably, as payments shift toward value-based driven care, LM stands to become increasingly utilized as a foundational component of treatment. Until then, financial constraints will likely limit its uptake within primary care; though the panel agreed that brief LM counseling interventions can be integrated into current clinic workflows and that SMAs are an option for leveraging more time for patient education and group support.
Strengths and Limitations
Our research is unique in providing the first expert consensus statements on the inherent relevance of LM to primary care and the essential components of LM practice that can be integrated into primary care practice to help achieve optimal outcomes. We also raise awareness of current barriers to integration of LM into primary care to help inform health care transformation efforts.
A key strength of our research process is the explicit and trustworthy methodology 32 that has been previously tested and validated by the American Academy of Otolaryngology—Head and Neck Surgery in developing multiple consensus documents. Trustworthy methodology is especially important when assessing expert consensus, to limit bias and distortions that may be introduced by expert panel members, particularly when conclusive research evidence is lacking. Highlights of our ECS process include a priori methodology to identify and prioritize key issues, translate the issues into statements for consensus, categorize consensus based on mean rankings and outliers, and refine statements using the iterative Delphi process.
Another key strength is the diversity and breadth of the expert panel members, which comprised clinicians from both academic and community health system settings with representatives from a variety of professional disciplines, including members of the American College of Preventive Medicine and the American Academy of Pediatrics selected by their respective organizations. Some of the panel members currently practice both LM and primary care, and some members were prior primary care providers now providing specialty LM services in collaboration with primary care and/or community health. Review of the available scientific evidence combined with the experience of our panel informed 124 consensus statements on topics relevant to LM practice as it relates to primary care. Strong consensus was achieved on 65 statements that can be used as a starting point for future improvements to the primary care model and highlighted areas that should be prioritized for further study.
Limitations include that despite collecting expert a priori evidence with explicit data forms we cannot exclude bias, recall, or reporting errors as potential sources of distortion. Our efforts were also limited by gaps and uncertainties in the relevant literature. Many of the studies were based on providing specific interventions (SMAs, stress management, lifestyle education, health coaching, physical activity) to subsets of patients in primary care (cancer survivors, patients with obesity, metabolic syndrome, CVD risk factors, depression, minor neurocognitive disorder). Some were LM specialty centers vs primary care practices. Despite the strong consensus on the need to regularly measure LM vital signs, there is no agreement on the optimal, pragmatic way to accomplish this in practice, nor on which specific tools or measures are best suited for this purpose. A final limitation of our research relates to the nature of an ECS, in general, which cannot make recommendations for practice or policy (as could a clinical practice guideline), but instead identifies areas of consensus for others to use in accomplishing this goal.
Conclusions
Diverse experts with experience in both LM and primary care agreed on the integral role of LM as a foundation of all health care and upon key aspects of LM practice that can be integrated into primary care to achieve optimal outcomes. The goal of this ECS was to raise awareness of the benefits and educate on the unique aspects of LM care to encourage integration into primary care. The benefits of LM care identified by the expert panel include addressing the root causes of most common chronic diseases, decreasing health-related costs, improving clinical outcomes, enhancing patient and clinician satisfaction, beneficial effects for the planet, and supporting health equity for historically marginalized populations.
Implications of Expert Consensus Statements on Lifestyle Medicine for Primary Care Clinicians.
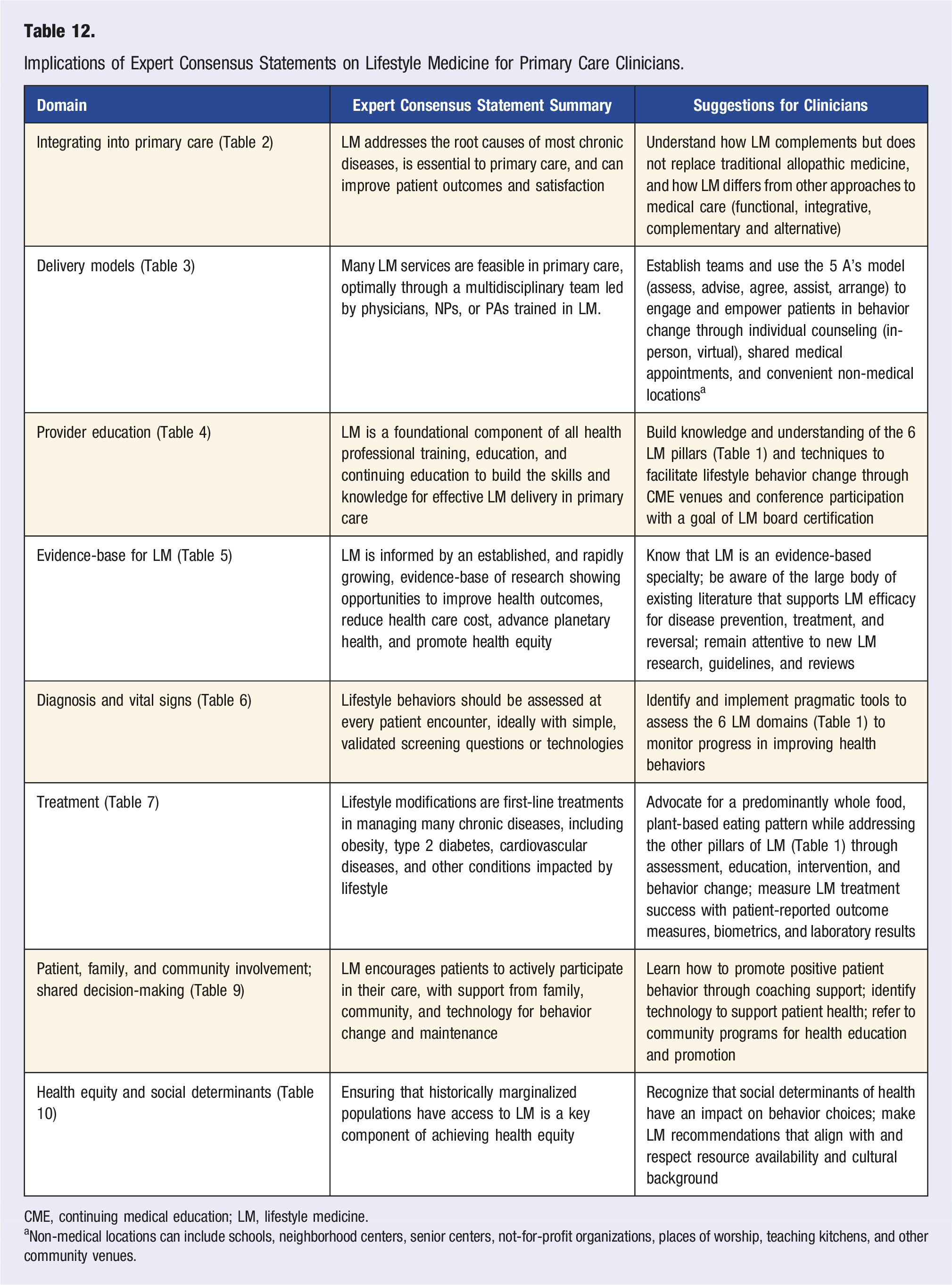
CME, continuing medical education; LM, lifestyle medicine.
aNon-medical locations can include schools, neighborhood centers, senior centers, not-for-profit organizations, places of worship, teaching kitchens, and other community venues.
Future research is necessary to study reimbursement models that make LM integration into primary care more universally feasible. Also, research is necessary to better define ITLC and test its effectiveness for chronic disease treatment, to identify when patients should be referred to ITLC programs, and to define the role of LM in addressing the social determinants of health and health equity. Additional study of examples of LM integration into primary care practice will allow us to eventually define an optimal clinic model that can be standardized and embedded in practices nationwide.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Disclaimer
Expert consensus statements are based on the opinions of carefully chosen content experts and provide for informational and educational purposes only. The purpose of the development group is to synthesize information, along with possible conflicting interpretations of the data, into clear and accurate answers to the question of interest. Expert consensus statements may reflect uncertainties, gaps in knowledge, opinions, or minority viewpoints, but through a consensus development process, many of the uncertainties are overcome, a consensual opinion is reached, and statements are formed. Expert consensus statements are not clinical practice guidelines and do not follow the same procedures as clinical practice guidelines. Expert consensus statements do not purport to be a legal standard of care. The responsible clinician, in light of all the circumstances presented by the individual patient, must determine the appropriate treatment, diagnosis, and management. Consideration of expert consensus statements will not ensure successful patient outcomes in every situation. The ACLM emphasizes that these clinical consensus statements should not be deemed to include all proper diagnosis/management/treatment decisions or methods of care or to exclude other treatment decisions or methods of care reasonably directed to obtaining the same results.
Supplemental Material
Supplemental Material - American College of Lifestyle Medicine Expert Consensus Statement: Lifestyle Medicine for Optimal Outcomes in Primary Care
Supplemental Material for American College of Lifestyle Medicine Expert Consensus Statement: Lifestyle Medicine for Optimal Outcomes in Primary Care by Meagan L. Grega, Jennifer T. Shalz, Richard M. Rosenfeld, Josie H. Bidwell, Jonathan P. Bonnet, David Bowman, Melanie L. Brown, Mollie E. Dwivedi, Ngozi M. Ezinwa, John H. Kelly, Amy R. Mechley, Lawrence A. Miller, Rajiv K. Misquitta, Michael D. Parkinson, Dipak Patel, Padmaja M. Patel, Karen R. Studer, and Micaela Karlsen
Supplemental Material
Supplemental Material - American College of Lifestyle Medicine Expert Consensus Statement: Lifestyle Medicine for Optimal Outcomes in Primary Care
Supplemental Material for American College of Lifestyle Medicine Expert Consensus Statement: Lifestyle Medicine for Optimal Outcomes in Primary Care by Meagan L. Grega, Jennifer T. Shalz, Richard M. Rosenfeld, Josie H. Bidwell, Jonathan P. Bonnet, David Bowman, Melanie L. Brown, Mollie E. Dwivedi, Ngozi M. Ezinwa, John H. Kelly, Amy R. Mechley, Lawrence A. Miller, Rajiv K. Misquitta, Michael D. Parkinson, Dipak Patel, Padmaja M. Patel, Karen R. Studer, and Micaela Karlsen
Footnotes
Acknowledgments
ACLM thanks Lorraine C. Nnacheta, DrPH, MPH, for assistance with project management, methodology, meeting facilitation, and manuscript preparation; Kara L. Staffier, MPH for assistance with the Delphi Survey preparation and analysis; and Kelly Cara, MPH for assistance with search strategies and literature reviews. ACLM thanks the Ardmore Institute of Health for funding support.
Author Contributions
Meagan L. Grega (Kellyn Foundation, St. Luke's University Health Network): writer, chair; Jennifer T. Shalz (St. Luke's Health System): writer, assistant chair; Richard M. Rosenfeld (SUNY Downstate Health Science University): writer, methodologist; Josie H. Bidwell (University of Mississippi Medical Center): writer, expert panel member; Jonathan P. Bonnet (VA Palo Alto Health Care, Stanford University School of Medicine): writer, expert panel member; David Bowman (Howard University College of Medicine): writer, expert panel member; Melanie L. Brown (Johns Hopkins School of Medicine): writer, expert panel member; Mollie E. Dwivedi (Washington University Living Well Center): writer, expert panel member; Ngozi M. Ezinwa (Loma Linda University Healthcare): writer, expert panel member; John H. Kelly (Loma Linda University, Lifestyle Health Education Inc.): writer, expert panel member; Amy R. Mechley (University of Cincinnati College of Medicine): writer, expert panel member; Lawrence A. Miller (Medical College of Wisconsin): writer, expert panel member; Rajiv K. Misquitta (The Permanente Medical Group): writer, expert panel member; Michael D. Parkinson (P3 Health (Prevention, Performance, Productivity)): writer, expert panel member; Dipak Patel (Community Health Center, Inc., Connecticut Lifestyle Medicine): Writer, expert panel member; Padmaja M. Patel (Midland Health): writer, expert panel member; Karen R. Studer (Loma Linda University Health), writer, expert panel member; Micaela C. Karlsen, writer, ACLM staff liaison.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Richard M. Rosenfeld, MD, MPH, MBA, DipABLM (Methodologist): Director of Guidelines and Quality, ACLM; prior Chief Medical Officer, ABLM. Jonathan P. Bonnet, MD, MPH, FAAFP, FACLM, CAQSM, DipABOM, DipABLM (Panel Member): Consultant to AAFP's Lifestyle Medicine Tool Kit (Ardmore Institute of Health Grant)—Consultant to Emory Lifestyle Medicine and Wellness for Teaching Kitchen (Ardmore Institute of Health Grant)—Co-chair of ACLM Board Review Course—Advisory Board of Forfend Health—ABLM Board Member—Co-author of Lifestyle Medicine Handbook: The Power of Healthy Habits—AJLM CME Question Writer. David Bowman, MD, DipABLM (Panel Member): Board of Directors for ACLM. Amy R. Mechley, MD, FAAFP, FACCLM, Dip ABLM, DipABFM (Panel Member): Investor in Poplar Health-ABLM Board member and ABLM Chair-elect. Rajiv K. Misquitta, MD, FACP, Dipl. ABLM (Panel Member): Co-author of a book on plant-based eating called “Healthy Heart healthy Planet.” Michael D. Parkinson, MD, MPH, FACPM (Panel Member) Advisor to employers, health care organizations, numerous startups and Pivio (formerly CHIP - Complete Health Improvement Program). Padmaja M. Patel, MD, FACLM, DipABLM (Panel Member): Investor in Poplar Health and Nudj Health. Advisory board of member of Nudj Health. Karen R. Studer, MD, MBA, MPH, FACPM, DipABOM, DipABLM, Lifestyle Medicine Intensivist (Panel Member):10% FTE for Lifestyle Medicine Residency Curriculum (LMRC) work, a joint product by (LLUH) and ACLM.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ardmore Institute of Health. The funder had no role in topic selection or any aspect of the project. The expert panel members received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.