
Abstract
Primary care physicians are well-positioned to integrate lifestyle interventions into the management of patients with unhealthy substance use, who may also have mental and physical chronic health comorbidities. However, the COVID-19 pandemic exacerbated the U.S.’s poor state of health, revealing that its current approach to chronic disease management is neither effective nor sustainable. Today’s full spectrum comprehensive care model requires an expanded toolkit. Lifestyle interventions broaden current treatment approaches and may enhance Addiction Medicine care. Primary care providers have the potential to have the greatest impact on unhealthy substance use care because they are experts in chronic disease management and their frontline accessibility minimizes healthcare barriers. Individuals with unhealthy substance use are at an increased risk of chronic physical conditions. Incorporating lifestyle interventions with unhealthy substance use care at every level of medicine, from medical school through practice, normalizes both as part of the standard care of medicine and will drive evidence-based best practices to support patients through prevention, treatment, and reversal of chronic diseases.
Keywords
Introduction
The United States (U.S.) entered the COVID-19 pandemic with multiple uncontrolled chronic conditions including unhealthy substance use and obesity-related diseases. The COVID-19 pandemic exacerbated the U.S.’s poor state of health, revealing that its current approach to chronic disease management is neither effective nor sustainable.1-6 Today’s full spectrum, comprehensive, chronic disease management care model requires an expanded toolkit. Evidence-based Lifestyle Medicine (LM) and Addiction Medicine (AM), two rapidly growing fields within healthcare, offer great promise to reroute the U.S.’s current trajectory towards a healthier country.
Prior to the COVID-19 pandemic, many clinicians were grappling to support patients with unhealthy substance use behaviors (i.e., alcohol use in excess of National Institute of Drug Abuse recommendations, or any illicit substance use). In 2018, approximately one in thirteen people age 12 or older (7.8%) needed substance use disorder treatment in the prior year and only approximately 17.5% of those needing treatment received it. 7 Since the COVID-19 pandemic, the percentage of the U.S. population with unhealthy substance use increased. By June 2020, 13% of the population started or increased substance use.6-7 The Centers for Disease Control and Prevention reported an increase in drug overdose deaths, including a 55% increase in synthetic opioid fatalities, during the 12 months ending in September 2020. 4 The social and financial stressors related to the COVID-19 global pandemic have widened the treatment gap as the number of individuals with unhealthy substance use increases and new pandemic-related barriers prevent access to care.7-8
Primary care providers (PCPs) practice within the crossroads where untreated substance use and poor lifestyle converge. They are experts in chronic disease management and see how the lack of physical activity, poor nutrition, tobacco use, illicit substance use, and excessive alcohol consumption are contributing to illness, injury, and premature death. Their frontline accessibility minimizes healthcare treatment barriers and they are poised to integrate substance use disorder care and lifestyle interventions to manage a multitude of mental and physical chronic health conditions.9,10 It is critical that clinicians prepare for the inevitable intersection of lifestyle interventions and substance use care (i.e. alcohol, tobacco, or illicit substances) as the need for both grows.
Relationship Between Chronic Physical Diseases and Chronic Mental Diseases
Individuals with either chronic mental illness, untreated substance use disorders, or both are at an increased risk of chronic physical conditions.11-14 In 2021, Richmond-Rakerd et al published a population-based cohort study that used data of 2.3 million New Zealanders aged 10–90 years old from the New Zealand Integrated Data Infrastructure. All individuals born in New Zealand during the 30-year observation period (January 1, 1928, to December 31, 1978) were included in the analysis. When compared to individuals without a mental health disorder, individuals with mental health disorders were more likely to develop physical diseases (31.9% compared to 20.0% without mental health disorders), to develop those physical diseases at a younger age (hazard ratio [HR], 2.33, 95% CI 2.30–2.36), and to die (RR 3.39; CI 3.32–3.47; P < .001). 13 Additionally, the World Mental Health Survey Initiative used cross-sectional data to conduct retrospective surveys of individuals from 28 countries. 15 They reported substance use was associated with poor physical condition outcomes, and that as mental disorder comorbidities increase, physical health outcomes worsen. 15 There is also a high co-occurrence of unhealthy substance use and chronic mental health disease.14,15 Preventing and reversing unhealthy substance use may mitigate chronic physical disease, disability, high healthcare costs, and death. 12
Even before COVID-19, the rocketing opioid use and the rise of metabolic syndrome prompted the Institute of Medicine, in 2001, to convene a special Committee on Crossing the Quality Chasm, resulting in an urgent call for a fundamental change in redesigning the American healthcare system to account for the inherent interactions between the mind and the rest of the body.16,17 Twenty years later, as chasms to care for unhealthy substance use and chronic illness continue to expand, medicine must infuse innovative and evidence-based approaches like lifestyle interventions to bridge this expanding gulf. Recent findings from Rasmussen et al conducted a randomized control study on a Swedish population showing that individuals that improved at least two lifestyle factors in addition to their substance use (tobacco or alcohol) were significantly more likely to achieve sobriety after one year. 18
The Spectrum of Unhealthy Substance Use
Unhealthy substance use is a broad spectrum of conditions ranging from hazardous (i.e., increases the risk of harmful physical or mental health consequences) to the diagnosis of a substance use disorder (SUD) (i.e., use patterns that have already caused harm or dependence)
7
(see Figure 1). When clinicians explore patients’ substance use, it is crucial that they assess their use based on a spectrum rather than categorically if they meet DSM5 criteria for a substance use disorder. If clinicians only intervene when a patient meets substance use disorder diagnostic criteria, they will miss most of the patients that are participating in unhealthy substance use. In 2018, twenty million (7.4%) persons aged 12 or older were diagnosed with a substance use disorder in the past year. However, when asked about the use of alcohol, tobacco or illicit drugs in the past 30 days, 164.8 million (60.2%) people aged 12 or older reported use.6-7 In Rippe’s Lifestyle Medicine, Suzuki et al agree that it is the responsibility of practitioners to identify and treat patients with unhealthy substance use.
19
There is a spectrum of unhealthy substance use that ranges from hazardous, or risky, use to a diagnosed substance use disorder from the DSM5.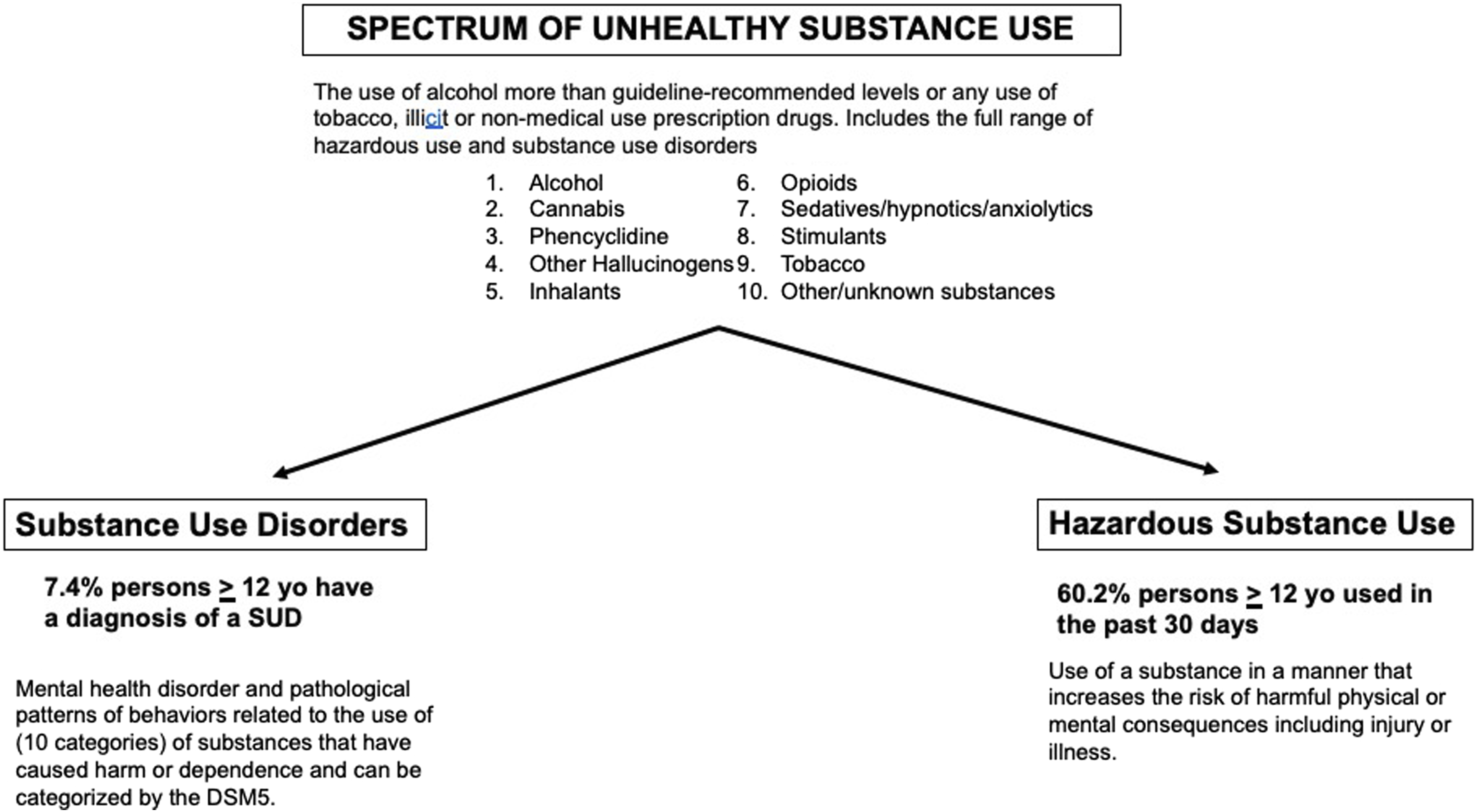
Primary Care Role in Unhealthy Substance Use Care
Alcohol and other substance misuse are common in the U.S. and have risen following the pandemic; yet, the treatment for substance use is still commonly avoided or delegated to addiction specialists for long-term care and emergency rooms for initiation of MAT. Currently, there are not enough specialized substance treatment facilities with addiction specialists to treat the rising number of patients with unhealthy substance use. Without treatment, many individuals with unhealthy substance use are at significant risk of morbidity and mortality. Subsequently, PCPs may be the only financially or geographically feasible healthcare option for many parts of the U.S., especially in rural areas where individuals have more barriers to addiction medicine specialty care, and depend on PCPs to identify and treat patients with unhealthy substance use. 20
Chronic disease management is a common thread sewn into the long-standing relationships PCPs have with their patients. Unhealthy substance use behaviors share many characteristics with the other chronic conditions such as diabetes and heart disease as there are genetic, environmental, and epigenetic etiologies that cause changes in brain structure and function. They can be characterized as uncontrolled during periods of ,or return to use, and maladaptive behaviors, like other chronic diseases including hypertension and diabetes. Management is individualized and like other chronic diseases,or return to use, it can be managed with medications, behavioral support, addressing social determinants of health, and empathy.21,22 As such, patients with unhealthy substance use, like all patients with a chronic disease, need access to continuity care with a PCP. 23
Given the limited availability and accessibility of addiction medicine specialists, one viable solution to address the increasing needs is to continue to broaden unhealthy substance use care to include primary care. PCPs have demonstrated they are well equipped to address unhealthy substance use with their patients. For example, many PCPs are integrating medication assisted treatment (MAT) into their primary care practice. 24 At the time of this publication, the FDA has approved outpatient MAT for the treatment of alcohol use disorders (AUD), nicotine use disorders, and opioid use disorders (OUD). Evidence has shown the PCPs can provide analogous care to addiction medicine specialists. PCPs who practice medication-assisted treatment, such as prescribing buprenorphine for OUD, provide care that is comparable in efficacy and positive patient outcomes, as compared to specialist care.25,26 In some instances, PCPs have demonstrated better outcomes than specialty care. For example, in one randomized control trial, PCPs managing patients with comorbid conditions such as OUD and human immunodeficiency virus in a clinic-based program had better substance use outcomes than those treated in referred treatment programs with specialists. 27 In addition, patients are more likely to access care in a primary care setting. They report unhealthy substance use care in primary care setting supports their recovery because they receive all their services in one place at one time and benefit from the wrap-around services from a multi-disciplinary team.9,28,29 Addiction Medicine care in the primary care setting is also associated with reduced stigma, improve management of other chronic conditions, and increased utilization of preventative health services. 30
Integrating Addiction Medicine and Lifestyle Medicine
Applying lifestyle interventions is an opportunity to not only address chronic health conditions but also positively impact unhealthy substance use. Good sleep quality is considered a protective factor for problematic substance use. 31 Exercise has been shown to increase abstinence rates. 32 Additionally, multiple studies show that mindfulness practices reduce substance misuse by improving cognitive, affective, and psychophysiological processes related to self-regulation and reward processing. 33 Nevertheless, there is overwhelming evidence that most physicians miss these prevention counseling opportunities, do not feel confident in lifestyle intervention counseling, and do not address the root cause of lifestyle-related noncommunicable diseases.34-38 Lifestyle Medicine PCPs are exceptionally positioned to perform a root cause analysis and write a lifestyle intervention prescription in order to prevent or reverse chronic unhealthy substance use, thus reducing the burden of chronic physical diseases. Understanding this connection expands the primary care management approach because many of the patients with chronic physical diseases inevitably have comorbid unhealthy substance use including tobacco, alcohol, and illicit drugs.28,39
In 2017, the American College of Preventive Medicine introduced, and the American Medical Association House of Delegates released Resolution 959 (I-17) to incentivize and/or fund LM education and social determinants of health in undergraduate, graduate, and community medical education. The resolution was passed in response to two realizations: 1) morbidity and mortality related to lifestyle-related, noncommunicable chronic diseases are worsening and 2) physicians recognize the importance of lifestyle intervention counseling but do not feel qualified and/or are not conducting lifestyle intervention counseling to prevent, treat, or reverse of lifestyle-related, noncommunicable chronic diseases.21,35-38,40
Providing integrated care with lifestyle interventions and Addiction Medicine encourages physicians to be trained in both. Insufficient training across the medical education spectrum is a major barrier to identifying and utilizing effective lifestyle interventions for unhealthy substance use prevention and treatment. Many of the current interventions, both educationally and clinically, are conducted in silos. If the fragmented healthcare system continues to silo LM and Addiction Medicine, the next generation of PCPs may not be prepared to practice Addiction Medicine with a lifestyle framework. Integrating lifestyle interventions and Addiction Medicine into undergraduate, medical school, and residency education would normalize them both as part of the standard care of medicine.
Most medical school and residency programs include only a few hours of training in lifestyle interventions. A 2017 systematic review of nutrition in medical education in multiple countries, including the U.S., found that nutrition is insufficiently incorporated into medical education, regardless of country. 41 The American College of Lifestyle Medicine created a Lifestyle Medicine Residency Curriculum (LMRC), which has grown from 4 residency programs in 2018 to 89 programs as of February 2022. Despite this exciting growth, there remains a void in lifestyle training at the residency level with only 3%–6% of internal medicine and family medicine residency programs offering the LMRC.42,43 Limited education leaves trainees ill prepared to counsel or write lifestyle intervention prescriptions for nutrition, stress management, restorative sleep, or exercise. LM in medical school and residency education will shift medicine from disease management to disease prevention and reversal. 19
Additionally, medical trainees do not have standardized or consistent Addiction Medicine education. Often trainees only experience Addiction Medicine in the hospital or emergency department setting rather than the primary care setting where frequent behavioral health change can be supported. In a 2017 CERA study of Family Medicine residency programs, only 28.6% of programs reported a required addiction medicine curricula. 44 A 2021 U.S. survey of internal medicine program directors found that few programs provided training in safe opioid prescribing and treatment of OUD, most did not view the training as very effective, and only .3% of residents completed buprenorphine waiver training. 45
As education and training in both lifestyle interventions and addiction medicine grows, it is important that medical education curricula address both in a desegregated fashion. To create a workforce of primary care doctors who are comfortable and competent to treat unhealthy substance use with lifestyle interventions, training in Addiction Medicine and lifestyle interventions needs to be integrated across all levels of education continuum and in a variety of healthcare settings. This well-trained workforce will also create a pool of lifestyle intervention and Addiction Medicine champions who will perpetuate their knowledge and skills as academic clinicians and/or resources to primary care peers.
Lifestyle interventions are growing in mainstream primary care education and practice. Now is the time to be inclusive of all the chronic health conditions that lifestyle interventions can affect, including unhealthy substance use. Successful Addiction Medicine curriculum in primary care residencies is a starting place for building an integrated lifestyle intervention and Addiction Medicine curriculum. One example of inclusive primary care training is the Yale Primary Care Internal Medicine Residency Program Addiction Recovery Clinic (ARC), developed in 2014. The goal of the ARC was to close the educational gap in Addiction Medicine training while also providing outpatient clinical services to patients with unhealthy substance use and SUDs including OUD and AUD. The ARC is a weekly clinic staffed by internal medicine residents, Addiction Medicine specialists, and a psychologist. Ninety-four percent (n = 29) of patients surveyed reported the ARC probably, or definitely, helped them manage their substance use and 84% (n = 26) were definitely satisfied with the overall treatment received. Learners also rated the rotation highly. They valued faculty members’ role modeling of patient–provider communication skills, learning about treatment options and the opportunity for interactive, real-time, and clinically relevant teaching. 46 This outpatient training model can be applied to both lifestyle interventions and Addiction Medicine in other residency training programs.
Furthering Evidence for Lifestyle Interventions in Addiction Medicine
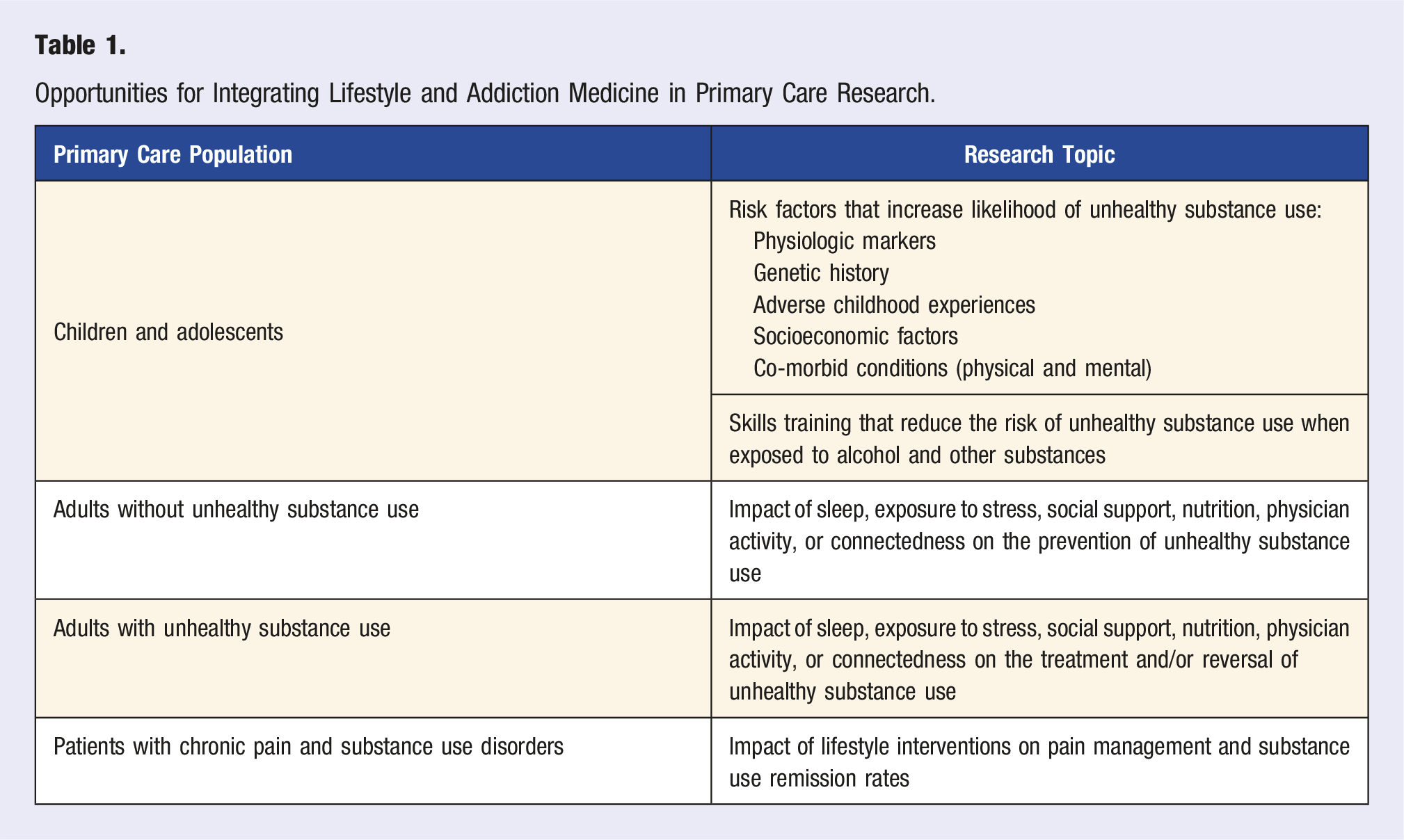
Another way to integrate lifestyle medicine and addiction medicine is through research. The 2019 Lifestyle Medicine Research Summit highlighted the lack of federal research spending for leading causes of death with a paucity of studies evaluating lifestyle interventions to treat and reverse the chronic diseases contributing to premature mortality and morbidity. Increased research will inform evidence-based, best practices in LM so that physicians can support patients through prevention, treatment, and reversal of unhealthy substance use. 21
Opportunities for Integrating Lifestyle and Addiction Medicine in Primary Care Research.
Next Steps: Where to Go from Here?
Many policy and health experts call COVID-19 a “magnifier,” as it has illustrated many social and healthcare disparities within the U.S. and other regions within the world. An end to COVID will not erase these chasms, but hopefully, it will motivate more emphasis to be placed on preventative medicine. Lifestyle Medicine is poised to help bridge this gap and help reverse the harmful effects of chronic illness, especially those effects from unhealthy substance use. To this end, the authors recommend the following: 1. Increase Lifestyle Medicine Exposure
Training for PCPs, Addiction Medicine and Lifestyle Medicine continues to be siloed. Despite the recent publication from The Journal of Family Practice, which centers on the 6 pillars of lifestyle medicine, there needs to be more mainstream integration of lifestyle medicine into all of healthcare training at the undergraduate, medical school, graduate nursing, physician assistant, and residency levels.
48
This may include changing provider level competencies needed prior to graduation. All providers should feel as comfortable writing a lifestyle prescription as they are writing for a pharmaceutical prescription. 2. Increase Lifestyle Medicine Interventions Within Addiction Medicine
The mainstay of treatment for patients with unhealthy substance use has been various forms of therapy, which has not had consensus of effectiveness.
49
Although lifestyle pillars are discussed as ways of improving coping skills, the relative importance has fallen to a lower-level recommended tier compared to that of MAT. Addiction Medicine has advocated that substance use disorders be considered as chronic medical conditions and not those due to poor willpower. Similarly, lifestyle medicine needs to be infused into all levels of provider training within Addiction Medicine training. As such, Addiction Medicine providers need to become as familiar with prescribing lifestyle prescriptions as prescriptions to treat unhealthy substance use. Furthermore, as there is no common criteria as what constitutes appropriate care for addiction residential or outpatient patient models, regulatory boards (i.e., JAHCO) should ensure lifestyle components are a part of program certification. 3. The scientific community should use the “practice near as possible” framework to continue researching the role of diet, exercise, stress reduction, sleep, or social connection, in unhealthy substance use prevention, management, and reversal.
Conclusion
The COVID-19 pandemic highlighted healthcare infrastructure’s weaknesses in chronic disease management as the risk of chronic physical conditions increased for individuals with either chronic mental illness, untreated substance use disorders, or both. To prevent and manage chronic disease, it is imperative that we teach and apply a comprehensive care model in which lifestyle interventions and unhealthy substance use are discussed within the same primary care patient visit. Lifestyle interventions to prevent and reverse unhealthy substance use will lessen chronic physical disease, disability, and death. An impactful intervention for patients will come from primary care physicians, who possess pragmatic experience in chronic disease management and often are one of the first points of contacts for patients struggling with unhealthy substance use. Incorporating lifestyle interventions into chronic disease management, which includes unhealthy substance use care, will enhance primary care physicians’ ability to improve patients’ health in multiple arenas. The American College of Lifestyle Medicine Residency Curriculum has a growing presence in many primary care residencies. Intentionally training medical students and resident physicians in both lifestyle medicine and addiction medicine will arm a new generation of physicians with the knowledge and confidence to apply lifestyle interventions to all chronic diseases, including unhealthy substance use. In addition, supporting research that integrates lifestyle medicine and addiction medicine will establish a new wave of evidence-based, best practices to prevent, treat, and reverse chronic diseases. Lifestyle interventions can mitigate our widening healthcare disparities by reversing the harmful effects of chronic illness, especially unhealthy substance use.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
sj-pdf-1-ajl-10.1177_15598276221111047 – Supplemental material for Primary Care at the Intersection of Lifestyle Interventions and Unhealthy Substance Use
Supplemental material, sj-pdf-1-ajl-10.1177_15598276221111047 for Primary Care at the Intersection of Lifestyle Interventions and Unhealthy Substance Use by Lindsay Nakaishi, Steven G Sugden and Gia Merlo in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.