
Abstract
Physical activity during pregnancy is an important health behavior. However, many pregnant individuals are provided with little-to-no guidance to adequately engage in physical activity. The purpose of this quantitative and quasi-qualitative study of currently or previously pregnant women was to examine physical activity behaviors in pregnancy and understand barriers and facilitators to achieving physical activity recommendations. Overall, 431 women (18+ years), White/Caucasian (84.5%), married (84.9%), and currently pregnant (66.6%), completed an online survey study. Most women (69.4%) reported engaging in cardio-based physical activity and willing to engage in physical activity to meet guidelines between 2 and 5 days per week (77.4 –88.8%). The most frequently reported barriers were feeling too tired (72.8%) or uncomfortable (71.8%) and childcare needs (57.8%). Being able to choose time of day (96.0%), accessing home workouts (92.9%), and having a personalized prescription (95.6%) were the most reported facilitators. Open comment feedback resulted in additional barriers, such as ensuring proper energy intake, while motivation and support from other pregnant individuals were fundamental facilitators. Individualized physical activity prescription is lacking in routine prenatal care. To support pregnant individuals to achieve physical activity recommendations, developing a prescription with suitable modalities, at-home options, and consideration for physical activity timing are required.
Introduction
Increasing or maintaining physical activity throughout life is important for the maintenance of overall health. 1 This is especially true during pregnancy, which is a critical moment for enhancing health of pregnant individuals, 2 and their offspring. 3 Health benefits of physical activity in pregnancy include reducing maternal risk for excess gestational weight gain,4,5 gestational diabetes mellitus, 6 and hypertension disorders, 7 and reducing risk of macrosomia and excess adiposity for offspring.8,9
The United States (U.S.) Department of Health and Human Services, 10 American College of Sports Medicine (ACSM), 11 and the Canadian guidelines for physical activity 12 recommend at least 150 minutes of moderate-intensity physical activity accrued over a minimum of 3 days per week during pregnancy. Although these guidelines clearly prescribe physical activity based on the frequency, intensity, time, and type (FITT) principle, they provide a one-size-fits-most approach. Yet, clinical groups now acknowledge that the prescription of a plan to meet recommended levels of physical activity are needed and such prescription may be more effective when individually tailored by appropriate specialist or trained clinicians. 13 In non-pregnant adults, adherence to a 12-month physical activity intervention was enhanced by exercise specialist supervision compared to a home-based approach even though both intervention programs were prescribed 60 minutes of moderate-intensity physical activity per day over 6 days per week. 14
Prenatal programs promoting physical activity, such as lifestyle interventions or in-person physical activity interventions, have been evaluated in systematic reviews and meta-analyses of randomized controlled trials.15,16 These studies provide robust evidence that physical activity, including aerobic, resistance training, or a combined approach improve pregnancy, birth, and offspring outcomes.17-19 Despite these benefits, only 20 to 45% of pregnant individuals meet physical activity recommendations per self-report.20,21 As such, we speculate that optimizing adherence to the physical activity guidelines through individual prescription may be the most effective means at engaging a large majority of pregnant women to meeting these recommendations.
Pregnant individuals fail to meet and adhere to physical activity recommendations owing to several barriers that, unless addressed, may never be overcome. These include misinformation as to physical activity benefits or harms, an inability to self-prescribe physical activity,22,23 pregnancy-related symptoms and restrictions, and concerns for the safety of the maternal-fetal unit.24-26
ACSM’s Exercise is Medicine® initiative strives for physical activity assessment and prescription to be standard practice in clinical care. This effort is actively working towards connecting providers and patients with evidence-based physical activity resources for people of all abilities, including pregnant individuals.27,28 Although pregnancy is a teachable moment with a finite window of opportunity, 29 healthcare providers are encouraged to institute more proactive, creative, and individualized approaches, in-line with the goals of Exercise is Medicine® initiative, to identify opportunities to prescribe physical activity.
Prior research does not describe factors which may aid pregnant individuals to become physically active, maintain levels of physical activity, or adhere to prevailing physical activity guidelines throughout pregnancy. Therefore, the primary aims of this informative research study were to (1) evaluate physical activity habits in pregnancy, (2) determine willingness to engage in recommended physical activity guidelines according to the basics of the FITT principle: frequency (1–7 days per week), intensity (moderate), time (150 minutes per week), and type (aerobic), and (3) assess barriers and facilitators of physical activity engagement.
Methods
Study Design
This was a cross-sectional quantitative and quasi-qualitative research study that was approved to capture responses of up to 1000 women residing in the U.S. ≥18 years of age who were currently pregnant or gave birth within the past two years. 1000 women was set as an upper-limit of responses to ensure capturing of various opinions on dietary behaviors and physical activity during pregnancy without oversaturating responses by race/ethnicity, body weight status, or current pregnancy status. The study was comprised of an electronic survey developed, piloted, and refined by research staff within the Reproductive Endocrinology and Women’s Health Laboratory. The survey was developed to be completed in 15 minutes, and the constructs within the survey were based on previously reported priorities for pregnancy-related research participation.30-32 This study was approved and monitored by the Pennington Biomedical Research Center Institutional Review Board and informed consent was received prior to participation.
Participant Recruitment
Study advertisements were shared on social media platforms, including Facebook, Instagram, and Twitter, or via email listservs for potential research participants, and the survey was available for completion between December 2020 and March 2021. Advertisements indicated that the study was seeking to understand women’s perceptions of types of eating patterns and physical activity habits during pregnancy. Willing participants were provided a hyperlink to the electronic survey hosted on Research Electronic Data Capture (REDCap®), a secure web-based application at Pennington Biomedical Research Center. 33 Before initiating the survey, participants were provided a description of the study purpose, disclosure of the estimated length of completion, and were asked to provide electronic informed consent to participate. Women who met the inclusion criteria were admitted into the survey. Responses were anonymous and no protected health information was obtained. Participants were offered an opportunity to enter a drawing for one of ten gift cards for completion of the survey by providing their email address, if desired.
Survey Characteristics
The survey was designed to capture responses surrounding the perceptions of physical activity habits and modern eating patterns during pregnancy. The instrument was structured according to the following domains: (1) physical activity habits during pregnancy, (2) willingness to engage in physical activity during pregnancy, (3) barriers and facilitators to physical activity, (4) respondent demographics, pregnancy status, and anthropometrics, as well as domains outside the scope of the present manuscript, but published elsewhere, (5) eating patterns during pregnancy, and (6) willingness to engage in eating plans during pregnancy.34,35 Each of the physical activity domains fell in-line with the basics of the FITT principle and highlighted each individual component of frequency, intensity, time, and type.
To assess physical activity habits, women were asked, “When pregnant, do you perform the following physical activity?” Responses included “Yes” or “No” to performing the pre-determined modes of physical activity, including: (1) Cardio—“Cardio” exercises increase your heart rate and breathing rate and make it difficult to hold conversation while working out. Examples of “cardio” based physical activity include: walking briskly, running or jogging, using the elliptical machine, dance, or Zumba classes, (2) Yoga-includes prenatal yoga, (3) Weightlifting or resistance training, (4) Pilates, and (5) HIIT (High Intensity Interval Training) Classes. If women responded “Yes” to performing “Cardio,” they were asked “How many days per week do you perform cardio-based physical activity during pregnancy?” Responses included 1-7 days per week and only one option could be selected.
To assess willingness to participate in physical activity, women were then provided the following text: Pregnant women are recommended to perform physical activity for at least 150 minutes per week, spread throughout the week (e.g., 30 minutes a day for 5 days) and asked: “How many days per week would you be willing to perform physical activity to meet 150 minutes per week during your second or third trimester of pregnancy?” Responses included 1–7 days per week and “women were” allowed to respond to any number of days per week as “not at all willing,” “not very willing,” “somewhat willing,” “very willing,” or “I don’t know.”
To assess barriers to physical activity, women were asked, “What concerns would you have about performing physical activity for 150 minutes per week during your second or third trimester of pregnancy?” Women were provided with nine concerns and allowed to respond to any concern as “not at all concerned,” “not very concerned,” “somewhat concerned,” “very concerned,” or “I don’t know.” Concerns included were (1) I would not enjoy the physical activity, (2) The physical activity would be too hard, (3) I would be too tired, (4) I would be too uncomfortable, (5) It would not be safe for my health, (6) It would not be safe for my baby’s health, (7) It would not work for my busy schedule, (8) I would not have childcare for my other children, (9) It would take away time from my social life.
To assess facilitators of physical activity, women were asked, “If you could work with a professional exercise specialist (free of charge) in a secure, private, and sanitized environment to follow a workout plan during your second or third trimester of pregnancy, would you find these things helpful?” Women were provided with eight helpful tools and allowed to respond to any tool as “not at all helpful,” “not very helpful,” “somewhat helpful,” “very helpful,” or “I don’t know.” Facilitators included were (1) Being able to choose the time of day for my workouts, (2) Being able to do some of the workout sessions at home, (3) Being able to do some of the workout session at home while video chatting with my exercise specialist, (4) Working out on weekdays only, (5) Working out on weekends only, (6) Having the workout sessions catered to my personal fitness level, (7) Checking in with my doctor more often to make sure my baby is healthy, (8) Providing childcare for my other children while I workout.
Statistical Analysis
Upon closure of the study, data were exported from REDCap® into a SAS database (SAS version 9.4, Cary, NC) for analyses. Descriptive statistics and proportional analyses were performed to evaluate physical activity engagement, perceived concerns, which were established as barriers, and proposed helpful tools, which were established as facilitators. Data summarized in figures are presented as proportion (expressed as percentage) of respondents, while data in tables are expressed as number and proportion of respondents for categorical variables or Mean ± SD for continuous variables. The multi-level responses of “not at all willing/concerned/helpful” and “not very willing/concerned/helpful” were combined to create dichotomous responses of “not willing/concerned/helpful” while “somewhat willing/concerned/helpful” and “very willing/concerned/helpful” were combined to create dichotomous responses of “willing/concerned/helpful.” “I don’t know” responses were excluded. Pregnancy engagement in cardio-based physical activity, willingness of frequency to engage in physical activity, and number of barriers to engagement in physical activity were further explored. Additional proportional analyses based on pregnancy status and parity was also performed. Pregnancy status was pre-determined based on the survey item: “Choose what best describes your pregnancy status,” in which women had the option to select 1) I am pregnant now AND have given birth in the past two years, 2) I am pregnant now but have NOT given birth in the past two years, 3) I am NOT pregnant now but HAVE given birth in the past two years, or 4) am NOT pregnant now and have NOT given birth in the past two years. Women who responded I am NOT pregnant now and have NOT given birth in the past two years were ineligible to continue the survey and therefore not included for analysis. In those who reported being currently pregnant, they were then asked for their current weeks gestation, and categorized into trimester 1 (<14 weeks), trimester 2 (14–26 weeks), and trimester 3 (≥27 weeks). Parity was a continuous variable and, based on the distribution of data, was categorized as no other children, one other child, and two or more other children. Other exploratory analyses that may affect physical activity habits and barriers and facilitators to physical activity were performed for demographics characteristics: age, body mass index (BMI), and education. General linear model and X2 analyses were performed for continuous and categorical variables, respectively. A p value < .05 was considered significant. Reponses to the free-text open comment feedback were reviewed by three separate reviewers (J.R.S., E.W.F., and M.K.). Exemplar quotes pertaining to physical activity during pregnancy are highlighted in the results.
Results
Study Participants
Respondent demographics.
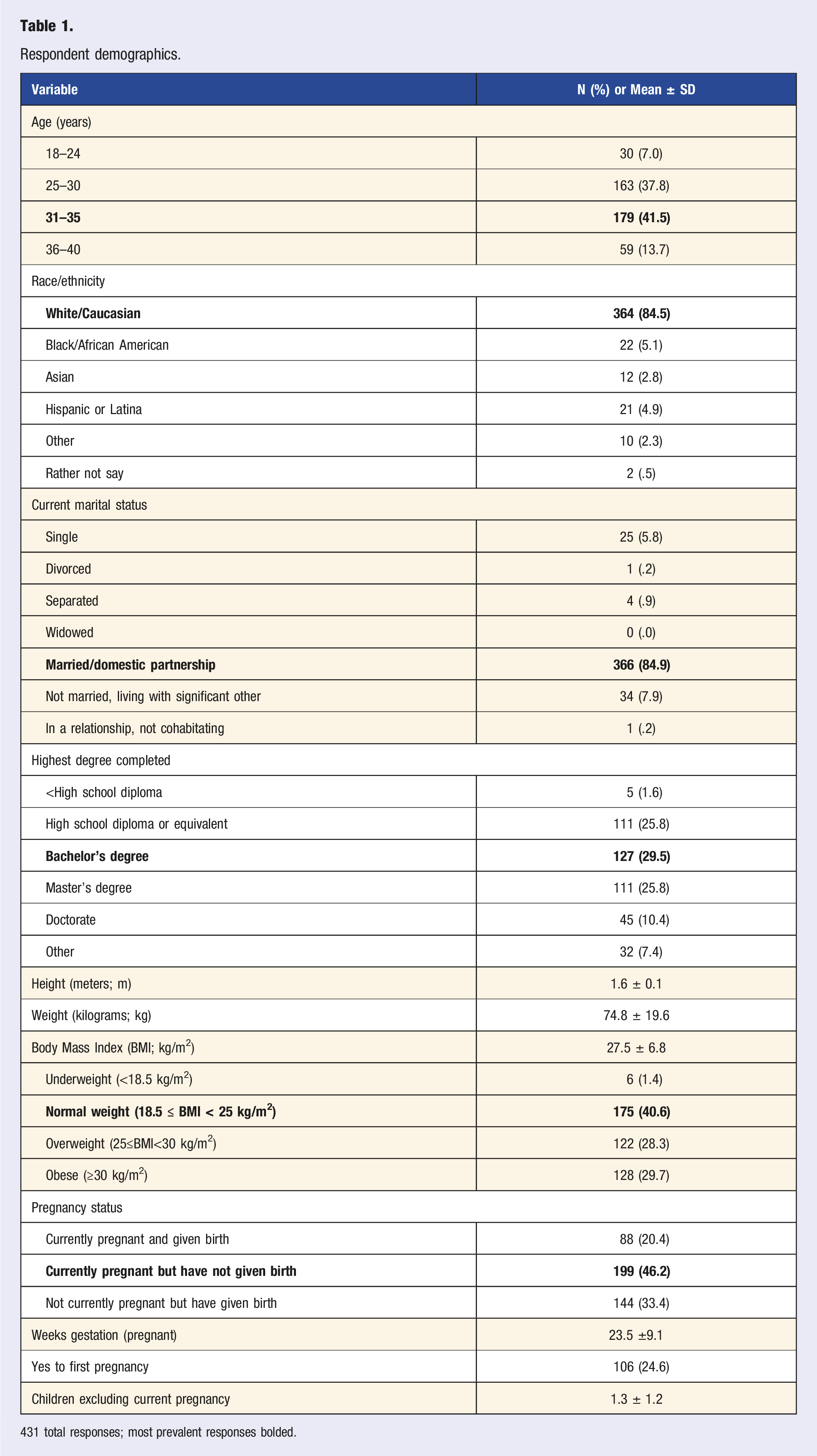
431 total responses; most prevalent responses bolded.
Physical Activity Habits during Pregnancy
Most women reported participating in cardio-based physical activity during pregnancy (69.4%; 299/431; Figure 1A). Of those, the majority reported performing cardio-based activities 2–5 days per week (87.6%; 262/299) with few responding to 1, 6, or 7 days per week (2.0%; 6/299; 4.0%; 12/299; 10.4%; 31/299; respectively). Other reported activities were yoga (44.1%; 190/431), weightlifting (33.9%; 146/431), HIIT (13.5%; 58/431), and Pilates (12.1%; 54/431) (Figure 1A). Percentage of respondents who reported their pregnancy engagement in physical activity (1A), days per week willing to engage in physical activity to meet 150 minutes per week (1B), and barriers (1C) and facilitators (1D) to physical activity engagement. For Figures 1C and 1D, the barriers and facilitators were shortened for graphical representation. Figure 1C: Tired = I would be too tired, Uncomfortable = I would be too uncomfortable, No Childcare = I would not have childcare for my other children, Hard = The exercise would be too hard, Busy = It would not work with my busy schedule, Enjoy = I would not enjoy the exercise, Baby’s Health = It would not be safe for my baby’s health, Personal Health = It would not be safe for my health, Social Life = It would take away time from my social life. Figure 1D: Personalized = Having the workout sessions catered to my personal fitness level, Choose Time = Being able to choose the time of day for my workouts, Home Workouts = Being able to do some of the workout sessions at home, Doctor’s Check-Ins = Checking in with my doctor more often to make sure my baby is healthy, Virtual Coaching = Being able to do some of the workout sessions at home while video chatting with my exercise specialist, Weekdays Only = Working out on weekdays only, Childcare = Providing childcare for my other children while I workout, Weekends Only = Working out on weekends only.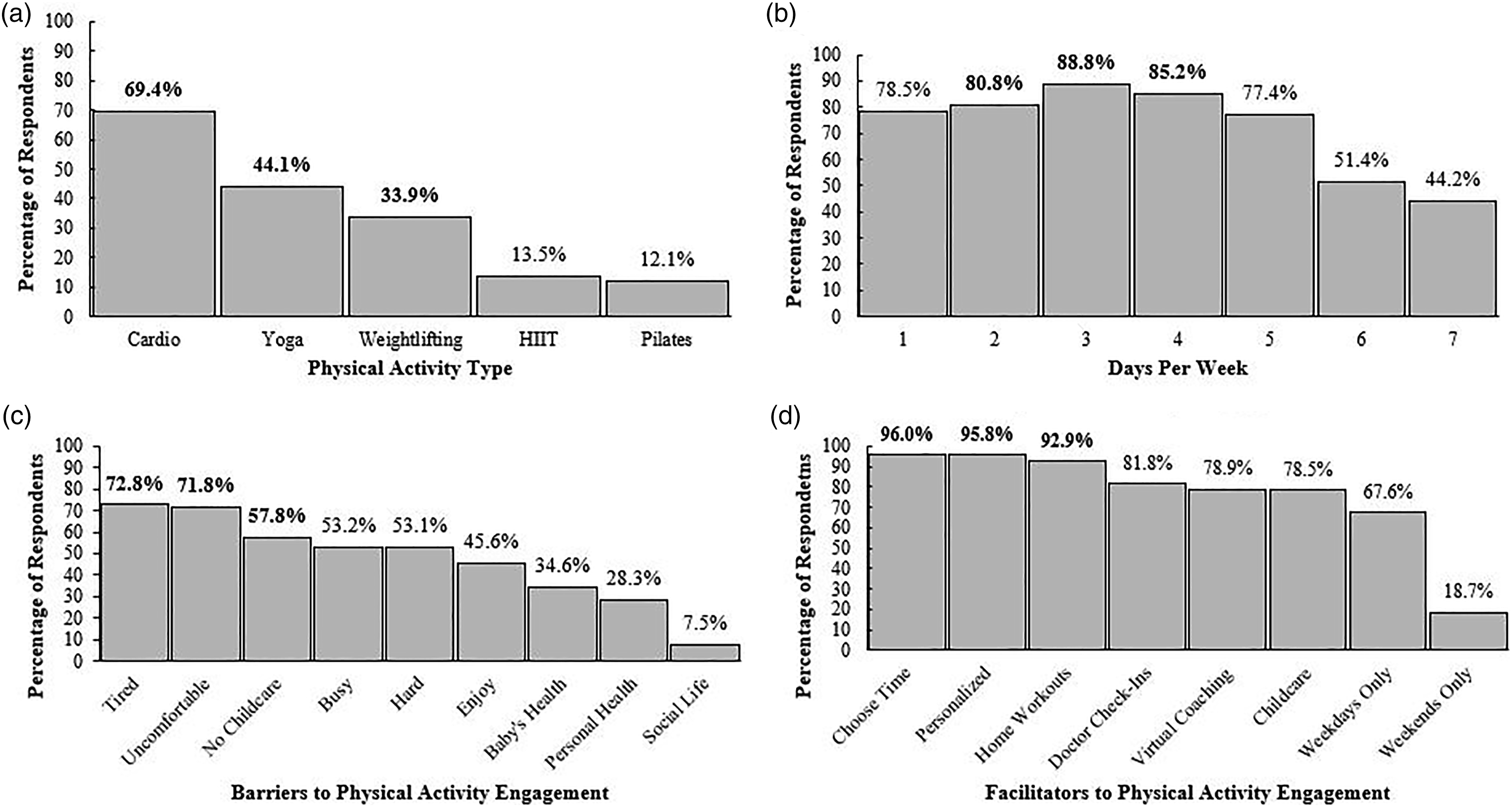
Willingness to Perform Physical Activity during Pregnancy
In ranked order, women were most willing to perform physical activity 3 days (87.9%; 379/431), 4 days (84.0%; 362/431), or 2 days (80.0%; 345/431) per week (Figure 1B). Of note, 77.7% and 76.1% reported willingness to engage in 1 or 5 days of physical activity per week, respectively. Only 43.2–50.1% (186-216/431) reported willingness to engage in 6–7 days of physical activity per week. The high willingness to engage in physical activity during pregnancy may likely be due to the understanding of physical activity for overall health. This was exemplified by participant quotes such as,
“I think exercise and following a healthy diet are important when pregnant,”
“I think exercise and eating healthy is important,” and
“It's important to maintain physical fitness and to gain weight slowly [during pregnancy].”
Barriers to Physical Activity
On average women reported 4.1 ± 2.5 barriers to prenatal cardio-based physical activity. In ranked order, the top three reported barriers (Figure 1C) were I would be too tired (72.8%; 314/431) or I would be too uncomfortable (71.8%; 309/431), and I would not have childcare for my other children (57.8%; 249/431). Compared to the overall sample, the total number of reported barriers did not differ across number of days per week women were willing to perform physical activity; 2 days (4.1 ± 2.5), 3 days (4.0 ± 2.1), and 4 days (3.8 ± 2.4) (p> .05 for trend); nor did the order of the most frequent barriers reported. However, other barriers such as safety concerns emerged from quasi-qualitative findings. Although a smaller proportion of the participants thought that exercising would not be safe for my baby’s health (34.3%; 148/431), it is important to note that this concern does resonate with some individuals. For example, one participant reported,
“I’m scared to exercise too hard during pregnancy for fear that I will harm the baby.”
One unforeseen barrier was fear of maintaining an appropriate energy balance. One participant stated,
“My main concern is maintaining any calorically sufficient diet and exercise plan if I experience the same level of nausea as I did during my first pregnancy. I also lacked the energy to workout during the first trimester and half of the second trimester and again was hit with the fatigue during my third trimester” and another,
“I am concerned about dieting and exercising as I barely am gaining [weight].”
Facilitators to Physical Activity
The average number of facilitators reported was 6.0 ± 1.6. Women preferred flexibility and tailored approaches to physical activity when asked If you could work with a professional exercise specialist (free of charge) in a secure, private, and sanitized environment to follow a workout plan during your second or third trimester of pregnancy, would you find these things helpful? (Figure 1D). Women preferred to be able to choose the time of day for my workouts (96.0%; 408/425). In addition to flexible timing, women also preferred having the workout sessions catered to my personal fitness level (95.8%; 409/427), and desired to being able to do some of the workout sessions at home (92.9%; 395/425). This was exemplified in one response,
“I want more options. My Dr. doesn’t say much but walk. But where am I to walk during winter? I want exercises to do at home or to know how to do them and how much and what’s safe.”
Compared to the total sample, the number of facilitators reported did not differ across days per week willing to perform physical activity; willingness to perform physical activity on 2, 3, and 4 days reported 6.1 ± 1.6, 6.1 ± 1.5, and 6.1 ± 1.5 facilitators, respectively (p > .05 for trend).
Impact of Number of Barriers on Physical Activity Habits, Willingness to Engage in Physical Activity, and Facilitators to Physical Activity
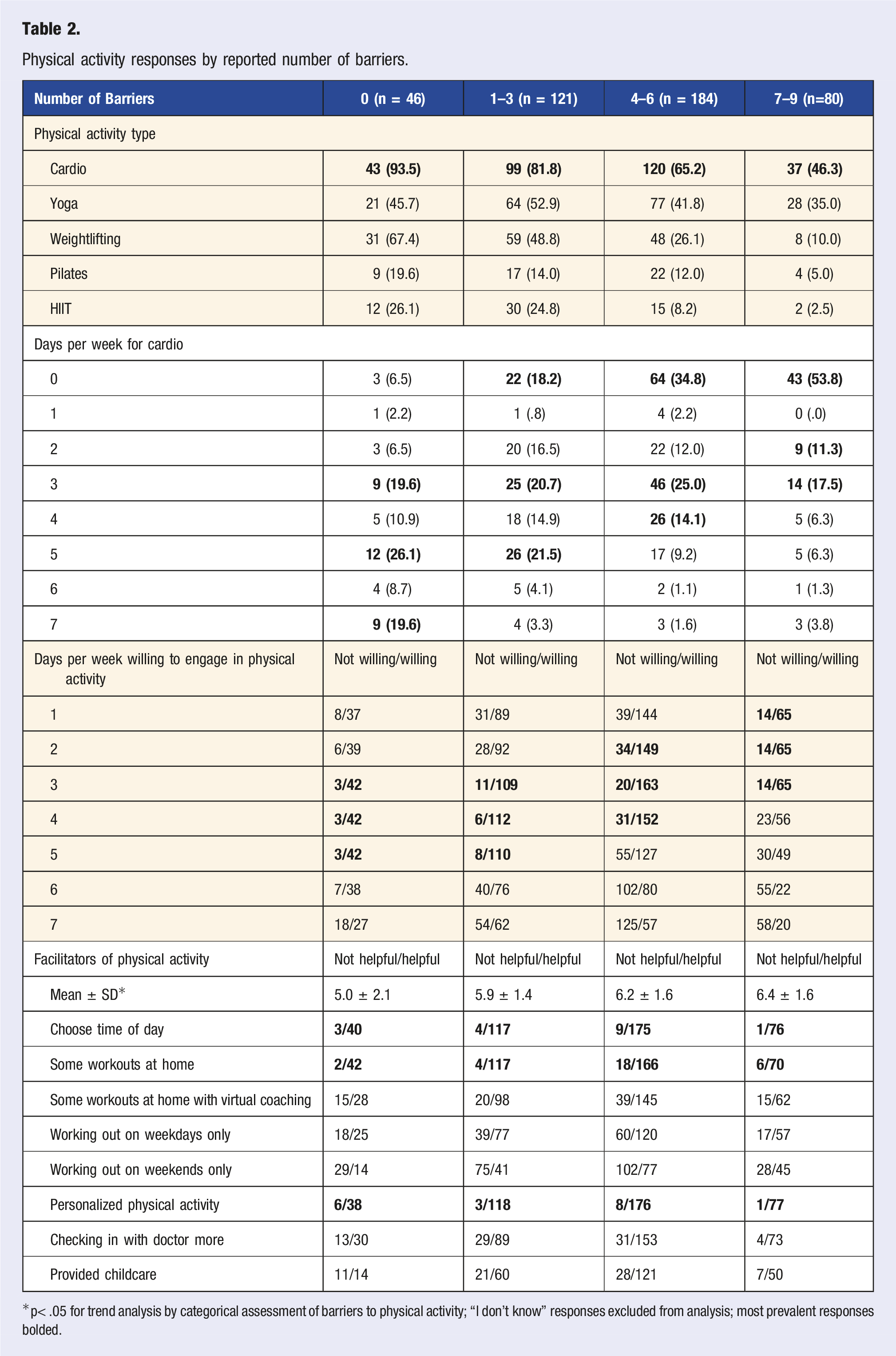
The number of reported barriers were inversely related to the proportion of women who responded to currently engaging in cardio-based physical activity; 0 barriers (93.5%; 43/46; reported as participating in cardio-based physical activity), 1–3 barriers (81.8%; 99/121; reported as participating in cardio-based physical activity), 4–6 barriers (65.2%; 120/184; reported as participating in cardio-based physical activity), and 7–9 barriers (46.3%; 37/80; reported as participating in cardio-based physical activity) (p< .05 for trend) (Figure 2). Respondents with fewer barriers were more willing to engage in 2–5 days per week of physical activity compared to those with more barriers; 0 barriers (38–42/46; 84.8–91.3%), 1–3 barriers (92–112/121; 76.0–92.6%), 4–6 barriers (120/184; 69.0–88.6%), and 7–9 barriers (49–65/80; 61.3–81.3%) (p< .05 for trend). As the number of barriers increased, the number of facilitators increased; 0 barriers (5.0 ± 2.1), 1-3 barriers (5.9 ± 1.4), 4–6 barriers (6.2 ± 1.6), and 7-9 barriers (6.4 ± 1.6) (p< .05 for trend) (Table 2). Even in the presence of these differences, the prominent facilitators remained in the same ranked order as having the workout sessions catered to my personal fitness level (56.8–70.7%; 38-176/44–184), being able to choose the time of day for my workouts (56.4–70.1%; 40–175/43–184), and being able to do some of the workout sessions at home (54.0–66.8%; 42–166/44–184). One additional support mechanism highlighted by women is to increase internal motivation. This was exemplified by one participant’s response,
“Motivation is probably my biggest issue during pregnancy. I get tired and lazy easily, if I had the support, that is probably all I would need.”
Pregnancy engagement in cardio-based physical activity by reported number of barriers. Respondents were categorized into reporting 0 (n = 43/46), 1–3 (n = 99/121), 4–6 (n = 120/184), and 7–9 (n = 37/80) barriers to physical activity. Physical activity responses by reported number of barriers. *p< .05 for trend analysis by categorical assessment of barriers to physical activity; “I don’t know” responses excluded from analysis; most prevalent responses bolded.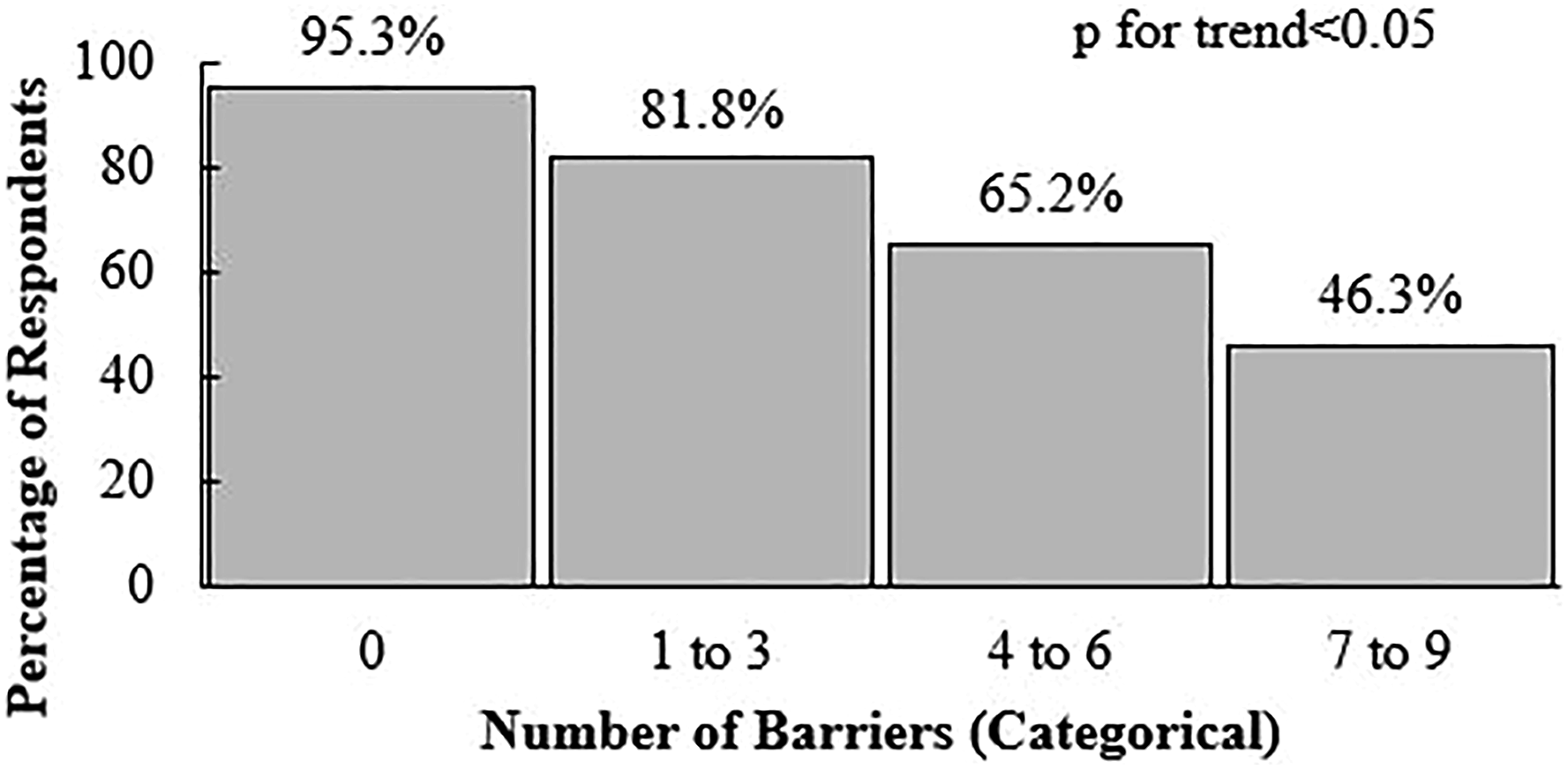
While another participant suggested that social support may help to boost motivation stating,
“I would like to exercise with other women.”
Influence of Pregnancy Status and Parity on Barriers and Facilitators to Physical Activity
The number of barriers reported were significantly different by pregnancy status defined as those currently pregnant and have given birth within the previous two years (n = 88) = 3.6 ± 2.3 to those currently pregnant and have not given birth within the previous two years (n=199) = 3.9±2.6, and those not currently pregnant, but have given birth within the previous two years (n = 144) = 4.6 ± 2.3 (p< .05 for trend). The three most prominent barriers remained the same as in the overall sample, except for those not currently pregnant, but have given birth within the previous two years expressed it would not work with my busy schedule (62.2%; 90/144) (Figure 3). The number of facilitators reported were not different between pregnancy statuses (p> .05 for trend), while the most prominent facilitators reported were the same as in the overall sample (Figure 3). In those who were currently pregnant (n = 287), there were no differences by trimester for the number of reported barriers: trimester 1 (n = 39) = 3.9 ± 2.4, trimester 2 (n = 133) = 3.8 ± 2.6, or trimester 3 (n = 115) = 3.9 ± 2.5 (p> .05 for trend), or facilitators: trimester 1 = 6.1 ± 1.8, trimester 2 = 5.8 ± 1.7, or trimester 3 = 5.8 ± 1.7 (p> .05 for trend). Additionally, the three most prominent barriers and facilitators reported remained the same as in the overall sample. Top three most prevalent barriers and facilitators to physical activity engagement by reported pregnancy status at time of survey completion. (A) Currently pregnant and have given birth in the previous two years (n = 88), (B) currently pregnant and have not given birth in the previous two years (n = 199), and (C) not currently pregnant but have given birth in the previous two years (n = 144). For Figure 2A–C, the barriers and facilitators were shortened for graphical representation. Tired = I would be too tired, Uncomfortable = I would be too uncomfortable, No Childcare = I would not have childcare for my other children, Busy = It would not work with my busy schedule, Choose Time = Being able to choose the time of day for my workouts, Personalized = Having the workout sessions catered to my personal fitness level, Home Workouts = Being able to do some of the workout sessions at home.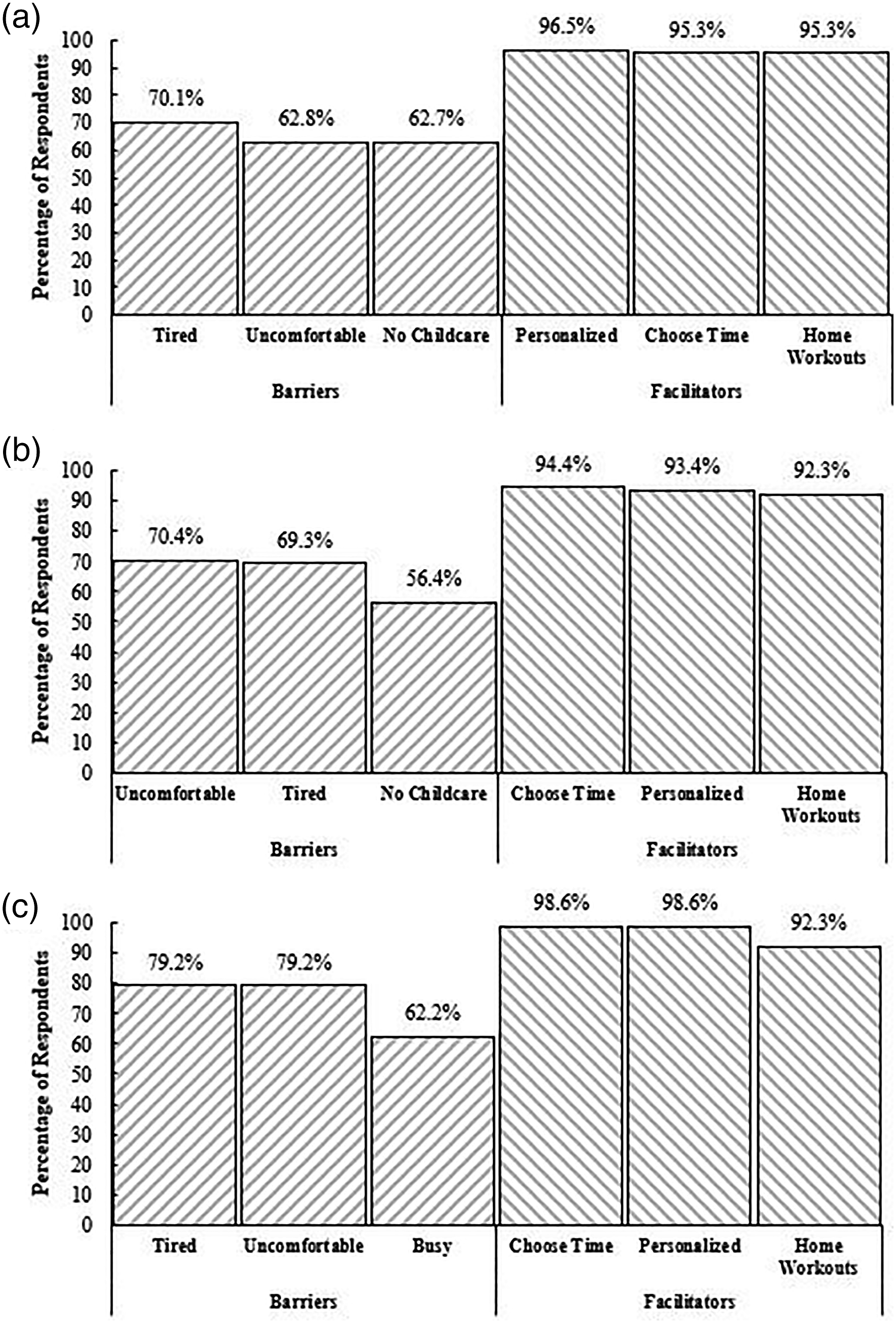
Parity associated with significant differences for the number of reported barriers to physical activity engagement whereby as number of other children increased, excluding current pregnancy, so did the number of barriers; no other children (n = 108) = 3.4 ± 2.5, one other child (n = 169) = 4.1 ± 2.3, and two or more other children (n = 154) = 4.4 ± 2.5 (p< .05 for trend). Parity also influenced the number of reported facilitators to physical activity engagement in the same manner as barriers; no other children (n = 108) = 5.6 ± 1.5, one other child (n = 169) = 6.0 ± 1.6, and two or more other children (n = 154) = 6.3 ± 1.7 (p< .05 for trend). The two most frequently reported barriers and three most frequently reported facilitators remained consistent as in the overall sample (Figure 4). However, women who reported no other children or one other child expressed it would not work with my busy schedule (47.7–58.4%; 52–99/108–169) as the third most prominent barrier to physical activity engagement. Our findings were similar regardless of examination by participant characteristics, including age, BMI, marital status, and education. Top three most prevalent barriers and facilitators to physical activity engagement by number of other children (excluding current pregnancy) at time of survey completion. (A) No other children (n = 108), (B) one other child (n = 169), and (C) two or more other children (n= 154). For Figure 3A–C, the barriers and facilitators were shortened for graphical representation. Tired = I would be too tired, Uncomfortable = I would be too uncomfortable, No Childcare = I would not have childcare for my other children, Busy = It would not work with my busy schedule, Choose Time = Being able to choose the time of day for my workouts, Personalized = Having the workout sessions catered to my personal fitness level, Home Workouts = Being able to do some of the workout sessions at home.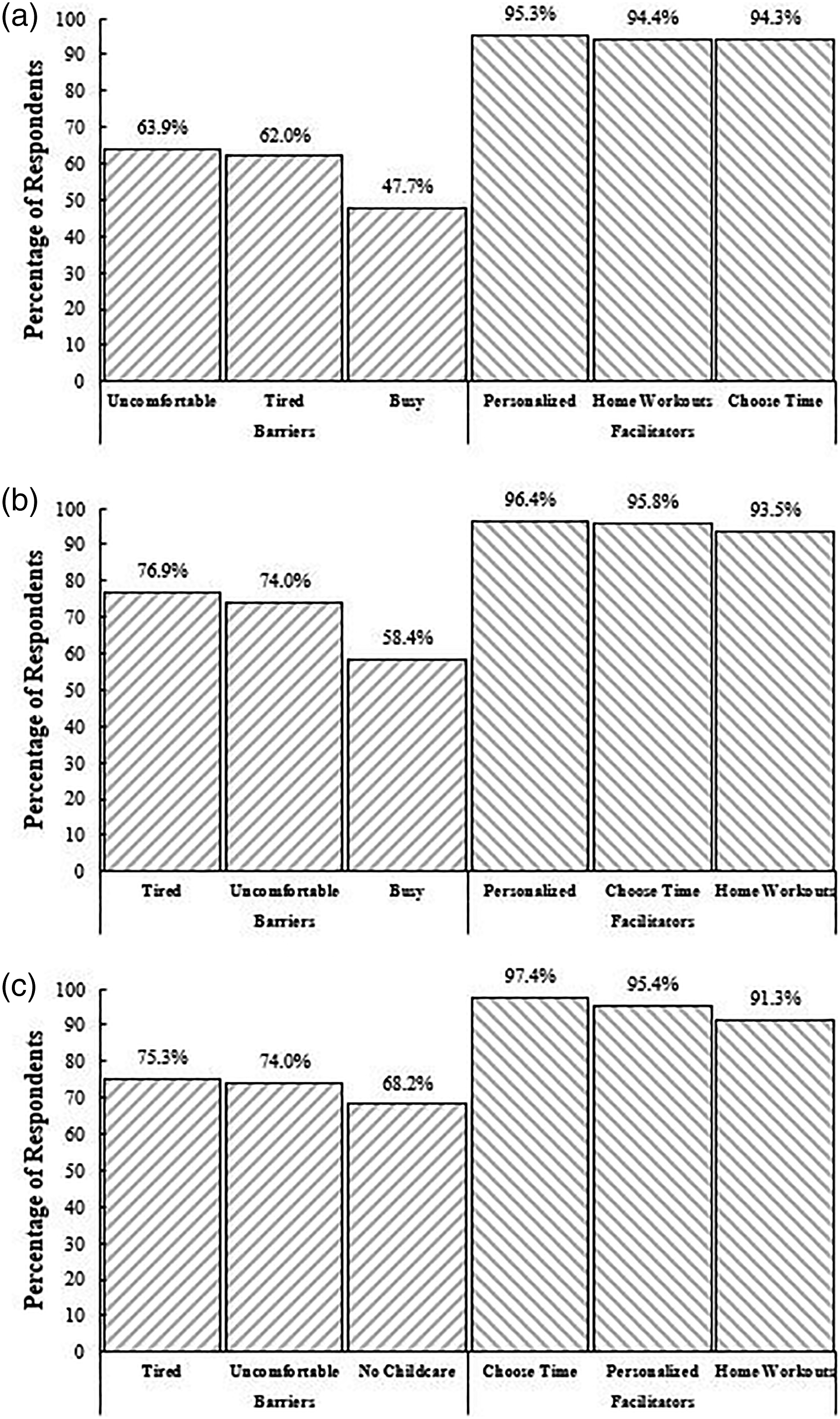
Discussion
Although this is not the first study to examine barriers and facilitators to physical activity during pregnancy, this is the first to capture non-theoretical constructs in relation to how to improve and enhance physical activity habits of pregnant women. Prior literature has considered theoretical frameworks or models and did not consider the interaction between barriers and facilitators to physical activity engagement during pregnancy.36-38 In this sample of 431 pregnant or recently pregnant women, most were willing to meet current physical activity guidelines. They reported that a tailored physical activity prescription with flexible times and locations, and the support of an exercise specialist would help optimize physical activity participation during pregnancy. These findings suggest personalized and prescriptive physical activity may be an advantageous approach to effectively support pregnant individuals to meet and maintain current physical activity recommendations.
Participants largely reported that physical activity during pregnancy would make them feel too tired, too uncomfortable, or that physical activity would be too hard, and that they would not have childcare for their other children. These barriers are consistent with previous research.39-43 Other previously reported barriers included concerns for mother-child safety, lack of advice/information, and lack of social support. 44 It has been proposed that the inability to adequately address barriers to prenatal physical activity may be due, in part, to the lack of healthcare providers prescribing and educating pregnant women about physical activity in pregnancy. 22 This was highlighted open comment feedback recorded in our study, which found that pregnancy-related physical limitations, maternal-fetus safety, knowledge/information, and misconceptions surrounding or lack of prescription for energy balance may influence physical activity decision-making during pregnancy. Leveraging these missed opportunities for healthcare providers to educate their patients regarding safe physical activity practices during pregnancy could alleviate concerns and/or barriers to physical activity engagement.
Multiple organizations recommend physical activity during pregnancy. Recent systematic reviews and meta-analyses have highlighted that most prenatal physical activity interventions are based on the recommendations of national and international organizations.15,16,45-47 Although this structured, one-size-fits-most approach is consistent within clinical trials, it is not pragmatic for most people and settings, and healthcare providers must look beyond such recommendations. Programs that target specific barriers to physical activity need to be developed and tested based on recommendations of the most critical stakeholders of a pregnancy, the pregnant individual, to consider their needs and desires of a prenatal intervention. To overcome this gap in execution of effectively engaging pregnant individuals in physical activity, experts have highlighted the need for enhanced patient education25,44,48-50 and use of motivational techniques.51-54
To our knowledge, prior research has not considered facilitators of physical activity as intervention targets, including time, location, and developing individual exercise prescriptions to foster physical activity engagement. Although interventions are successful at increasing physical activity, individually-centered prescriptions often result in long-term maintenance of, and avoid lapses in, physical activity engagement in non-pregnant populations. 55 If clinicians can individually tailor physical activity prescriptions based on factors such as current fitness level and individual time allocation, they may enhance continual engagement in physical activity by designing the program with the patient at the center. With the advent of technologies (i.e., pedometers and accelerometers) and mobile applications (e.g., MyFitnessPal), real-time physical activity feedback may be provided to the pregnant individual, while adaptive feedback may be provided through clinician engagement to individually enhance opportunities to be physical activity. Additionally, self-monitoring of health behaviors, including physical activity, have previously been shown to foster physical activity adherence and recommended gestational weight gain. 56 Collectively, leveraging the expertise of health professionals, including exercise specialists, in conjunction with self-monitoring tools and additional real-time and adaptive feedback to pregnant individuals, allows for greater personalized prescription of physical activity. This approach also accounts for reported barriers, such as time and location to allow for physical activity engagement of pregnant individuals.
There is a continual shift to empower and enable individuals to feel comfortable and safe with engaging in behavioral and lifestyle changes during pregnancy. The U.S. Preventive Services Task Force recently recommended that providers offer pregnant individuals effective behavioral counseling, including physical activity. 57 Rapid advancement in maternal healthcare has allowed for pregnancy and birth outcomes to be the focal point of prenatal care.58,59 Evidence-based practices, including prenatal education around safe practices during pregnancy from midwives or doula care, as well as nutritional counseling from registered dietitians, have shown that expanding the prenatal care beyond traditional maternal care improves outcomes.60-62 However, incorporation of providers from multiple disciplines is underutilized due to their associated cost and lack of health insurance coverage. 63 The lack of financial affordability has also been an established barrier in the integration of exercise specialists in traditional health care despite its added benefits. 64 The Exercise is Medicine® initiative encourages health care providers, particularly those in primary care, to assess and record physical activity as a vital sign during patient visits.27,28 This includes concluding each visit with an exercise “prescription” and/or referral to a certified health fitness professional or allied health professional for further counseling and support.27,28 Yet, to adequately prescribe physical activity during pregnancy, trained providers need to be incorporated, such as exercise specialists, which necessitates policy-level change to ensure financial compensation for services delivered. Until such policy-level changes can be enacted, organizations, such as ACSM, offer continuing education credits for healthcare providers, 65 as well as provide the opportunity to obtain an Exercise is Medicine® credential to intertwine the healthcare community with physical activity.28,66 These building blocks have begun to lay the groundwork for potential insurance incentives for pregnant individuals engaging in healthful physical activity habits, as well as healthcare providers having access to billing codes for physical activity monitoring to help in their personalized prescription.
It should be acknowledged that while the sample size is large, our recruitment efforts yielded a homogenous sample comprised primarily of women who identified as White/Caucasian, married, normal weight, and engaging in at least one mode of physical activity. These findings may not be generalizable to other groups including underrepresented races, single mothers or those not engaged in a domestic partnership, or gender identity in addition to biological sex, and to those who are physically inactive. Considering the increased risk of adverse maternal and birth outcomes for populations not well sampled within this study, efforts should be made to gather this information. Additional limitations were the online study design to capture survey responses and potential desirability bias, not considering contraindications to physical activity during pregnancy, including risk level, as well as type of prenatal care received or location of respondents within the U.S.
Conclusions
This study of over 400 women showed that women are willing to engage in physical activity in pregnancy at a minimum of 3 days per week to meet 150 minutes of moderate-intensity physical activity each week, which falls in-line with current recommendations. However, based on prior literature, most pregnant individuals do not meet these recommended physical activity guidelines. To better support all pregnant individuals to meet physical activity recommendations, our study provides evidence that personalized prescription for physical activity based on fitness level, versatility for home workouts, and at varying times of the day could enhance engagement. These observations were universal, regardless of current engagement in cardio-based physical activity, days per week willing to engage in physical activity, and demographic information, such as age, BMI, highest degree completed, current pregnancy status, and parity. Although previous randomized controlled trials have provided evidence to support the health benefits of physical activity during pregnancy, their rigidity in structure and one-size-fits-most approach drastically limits their ability to inform the design of a program which offers flexibility in physical activity prescription. Therefore, the need for precision medicine, specifically precision prescription of physical activity, is greater than ever before and warrants appropriate focus and consideration.
Supplemental Material
Supplemental Material - Understanding Barriers and Facilitators to Physical Activity Engagement to Inform a Precision Prescription Approach during Pregnancy
Supplementary Material for Understanding Barriers and Facilitators to Physical Activity Engagement to Inform a Precision Prescription Approach during Pregnancy by Joshua R. Sparks, Emily W. Flanagan, Maryam Kebbe, and Leanne M. Redman in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
The authors would like to acknowledge the members of the Reproductive Endocrinology and Women’s Health Laboratory at Pennington Biomedical Research Center who helped refine the survey from the initial iterations to its final version. The authors would also like to acknowledge the survey respondents. Without them, these results would not be possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by National Institutes of Health (NIH) R01 NR017644 and R01 DK124806.
Data Availability
Data may be made available upon reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.