
Abstract
Purpose: Substantial cancer burden may be prevented through lifestyle modifications. The purpose of this study was to determine the preliminary effectiveness of health coaching for the improvement of health, fitness, and overall well-being of cancer survivors in a community setting. Methods: Participants were recruited from Cancer Support Community Delaware locations. Health coaching was provided to people diagnosed with cancer anywhere along the survivorship continuum. Coaches provided 6 individual sessions. Surveys were sent pre- and post-intervention on topics including fitness, eating habits, sleep, perceived stress, anxiety, depression, and quality of life. Results were analyzed using multilevel modeling. Results: 48 participants completed an average of 85% of health coaching sessions. Coaching participants noted improvements in weekly physical activity frequency, including moderate–vigorous physical activity. Increases were found in healthy eating behavior. Participants reported improvements in the quality of their sleep, including changes in sleep duration and sleep efficiency. Significant reductions were found in perceived stress, anxiety, and depression. Importantly, participants reported improved quality of life, particularly in areas of physical and emotional well-being, as well as functional and total well-being. Conclusion: Preliminary findings indicate significant behavior change in measured outcomes and suggest health coaching may be an important tool for cancer survivorship.
the more healthy lifestyle behaviors a person engages in, the better their perceived QoL
Background
The prevalence of cancer survivorship in the United States totals close to 17 million people and is estimated to increase to over 22 million by 2030. 1 While cancer is still the second leading cause of death in the United States, from 2001 to 2017, the mortality rates have declined while 5-year survival rates have increased, meaning people are now living longer with the disease. Survivors are often at an increased risk of developing a second cancer or comorbidity, such as diabetes or cardiovascular disease, so finding a way to mitigate these burdens could have a positive effect on quality of life (QoL) and other long-term health outcomes.2-4
Many of the preventable behavioral factors associated with an increased likelihood of developing cancer are similar risk factors associated with an increased probability of developing a chronic disease. 4 According to Medicare data, up to 53% of cancer survivors have at least one other comorbidity. 5 This is problematic as cancer survivors with comorbidities are more likely to have poorer survival, tend to have more postoperative complications, are less likely to complete their course of cancer treatment, and experience poor QoL.6,7 However, evidence suggests a substantial cancer burden may be prevented through the modification of behavioral lifestyle factors. 8
A Healthy Lifestyle
The National Cancer Comprehensive Network (NCCN) has guidelines that recommends several healthy lifestyle habits for survivorship in order to maintain or improve health. 9 They recommend survivors engage in 150–300 minutes of moderate intensity or 75 minutes of vigorous intensity aerobic activity per week along with strength training that involves all muscle groups 2 to 3 times per week. However, it has been found even 30 minutes of moderate to vigorous activity 3 times per week is enough to relieve the burden of cancer-related fatigue, anxiety, and depression while helping to increase physical function and increase health-related quality of life. 10 They also recommend eating a diet high in vegetables, fruit, and whole grains with a reduction in excess sugars, fried foods, and red meat which may impact cancer progression, overall survival, and possibly risk of recurrence, especially when coupled with physical activity and weight maintenance.9,11,12 Additionally, they recommend cancer survivors get an adequate amount of sleep, which may improve physical and emotional functioning and reduce the risk of developing anxiety and depression.9,13,14 Cancer survivors often want information and are willing to make healthy lifestyle changes, but the effects of treatment or the cancer itself can make living a healthy lifestyle challenging.1,15 Because of this, services are often needed to help support life beyond the cancer diagnosis.
Health and Wellness Coaching
Health and wellness coaching (HWC) may be a viable tool for creating lasting, sustainable behavior change for cancer survivors via healthy lifestyle modifications. HWC coaches work with clients utilizing a client-centered approach to address the health topics most important to the individual. 16 Sessions are tailored to the client and utilize techniques such as motivational interviewing, goal setting, and creating accountability within a nonjudgmental environment. 17 HWC has been found to be effective in the general adult population for changing a variety of health behaviors such as increasing physical activity, improving nutrition intake, weight loss, and sleep improvements which subsequently reduces risk factors for several chronic diseases and can improve health outcomes.18,19 Clients often experience a sense of empowerment and increase in self-efficacy toward self-management techniques. 16 However, HWC has not been well studied with cancer survivors, especially within community settings. The HWC interventions that do exist for this population tend to center on pain management.20,21 Very few focus on multiple behavior changes and those that do often focus on just one type of cancer.22,23
Due to the variability of the symptoms experienced by cancer survivors, having an individualized, tailored program suited to their particular health priorities and abilities could help to facilitate adherence to behavioral changes, thereby improving overall health outcomes. By working within an established cancer community support setting, survivors can participate in a comfortable and familiar non-clinical environment with additional resources and programs readily available to them to help support their behavior change.
Due to the limited literature around HWC in this population, we designed a HWC program with the aim to determine the real-world effectiveness of HWC for improving health, fitness, and overall well-being of cancer survivors over a 3-month time period within a cancer community setting. We chose a preliminary effectiveness approach because it allows for the delivery of the program in routine, real-world settings and allows for a heterogeneous sample population as you may expect to see in many community-based organizations or in clinical practices.24,25
Methods
Project Overview
The “Wellness Coaching for Cancer Survivors” program was a program aimed at providing individualized HWC services to cancer survivors anywhere along the cancer continuum from early diagnosis through long-term survivorship throughout a community-based organization, Cancer Support Community Delaware (CSCDE). CSCDE is a statewide non-profit community organization that provides cancer survivors and their caregivers and/or family with counseling support groups, educational workshops, exercise and nutrition groups, and other programs free of charge to help cope with and manage the emotional aspect of cancer. 26 The project was a collaboration between CSCDE, the University of Delaware (UD), and Stockton University, using certified health coaches. 27 Approval was obtained by the Institutional Review Boards at both universities (approval numbers: 1174371 and 2017.132).
Study Design and Participants
A single group pretest–posttest design was utilized for this study. Participants were recruited from CSCDE locations across the state through flyers, email, and an advertisement in the agency’s weekly newsletter. Those who showed interest were contacted by the research coordinator to complete a phone screen to determine eligibility. Participants were considered eligible if they (1) were over the age of 18, (2) had been previously diagnosed with cancer at any time in the past, and (3) were able to read and complete an online questionnaire. There were no exclusion criteria independent of the inclusion criteria; however, the Physical Activity Readiness Questionnaire (PAR-Q) was verbally administered during the phone screen to assess whether a person was physically ready to engage in physical activity or whether they should consult a doctor before beginning an exercise program. 28 In the event someone failed the PAR-Q, they were allowed to be coached but were asked to contact their primary care provider and obtain medical clearance before being allowed to be coached around exercise or physical activity to ensure their physical safety. If eligibility criteria were met, written informed consent was obtained.
Program
Six individual HWC sessions were provided over a 3-month period to cancer survivors. Sessions were led by certified health coaches and followed the standard treatment model used at the health coaching clinic at UD.27,29 The first session was a 90-minute in-person session and held at one of the CSCDE locations of the participant’s choosing. The remaining 5 sessions were approximately 30 minutes in length and conducted either in-person, telephonically, or through a secure video conferencing platform, as designated by participant preference. Sessions were tailored to the individual, allowing them to talk about the most important aspects of their health and what behaviors they were most interested in changing during the next 3 months.
Data Collection
Before meeting with a coach, participants were sent an email with an individualized link to a battery of surveys, collected using REDCap electronic data capture tools hosted at UD. 30 Surveys were completed in the same manner approximately 3 months later, sent immediately following their final HWC session.
Instruments
Demographics and Health Coaching Questionnaire: Demographic information included gender, age, race, ethnicity, marital status, education, and income. Medical information included cancer type, stage, and date of diagnosis, as well as whether the participant had surgery, chemotherapy, or radiation to treat their cancer. The Health Coaching Questionnaire included general physical activity and sleep habits as well as additional information regarding smoking and intake of alcohol.
International Physical Activity Questionnaire – Short Form (IPAQ) 31 : The IPAQ is a seven-question measure assessing the number of bouts of vigorous physical activity, moderate physical activity, and/or walking a person does on average in a 7-day period in their leisure time as well as how many minutes they spend during each bout. The questionnaire also assesses how many minutes per day a person spends sitting. Bouts per week, minutes per week, and MET-minutes of moderate–vigorous and total physical activity were calculated and assessed.
Rapid Eating Assessment for Patients Short Form (REAP-S) 32 : This 16-item questionnaire assesses various eating habits. The higher the score, the healthier a person’s overall eating habits (baseline α .75).
Pittsburg Sleep Quality Index (PSQI) 33 : The PSQI measures various aspects of sleep and sleep patterns in adults. Nine questions determine subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction over the last month. Scores of 5 or above are indicative of poor sleep (baseline α .71).
Perceived Stress Scale (PSS) 34 : The PSS is a 10-item measure used to determine participants’ psychological perception of stress within the last month. Positive questions are reverse scored, and scores are summed for a total perceived stress score. The higher the score, the more stress the participant perceives experiencing (baseline α .87).
Hospital Anxiety and Depression Scale (HADS) 35 : This 14-item scale assesses anxiety and depression separately and categorizes symptoms as “normal,” “borderline abnormal,” or “abnormal”. In this study, this scale was included as a screening tool to help determine if the participant needed to be referred to a mental health professional before beginning the program (baseline α anxiety = .88; depression = .89).
Functional Assessment of Cancer Therapy: General, Version 4 (FACT-G) 36 : The FACT-G is a 27-item questionnaire measuring 4 facets of cancer-related QoL: physical well-being, social and family well-being, emotional well-being, and functional well-being. It provides scores for each individual subscale, as well as a total score. Higher scores indicate higher reported health-related QoL (baseline α physical = .80; social = .86; emotional = .87; functional = .86; total = .91).
Statistical Analysis
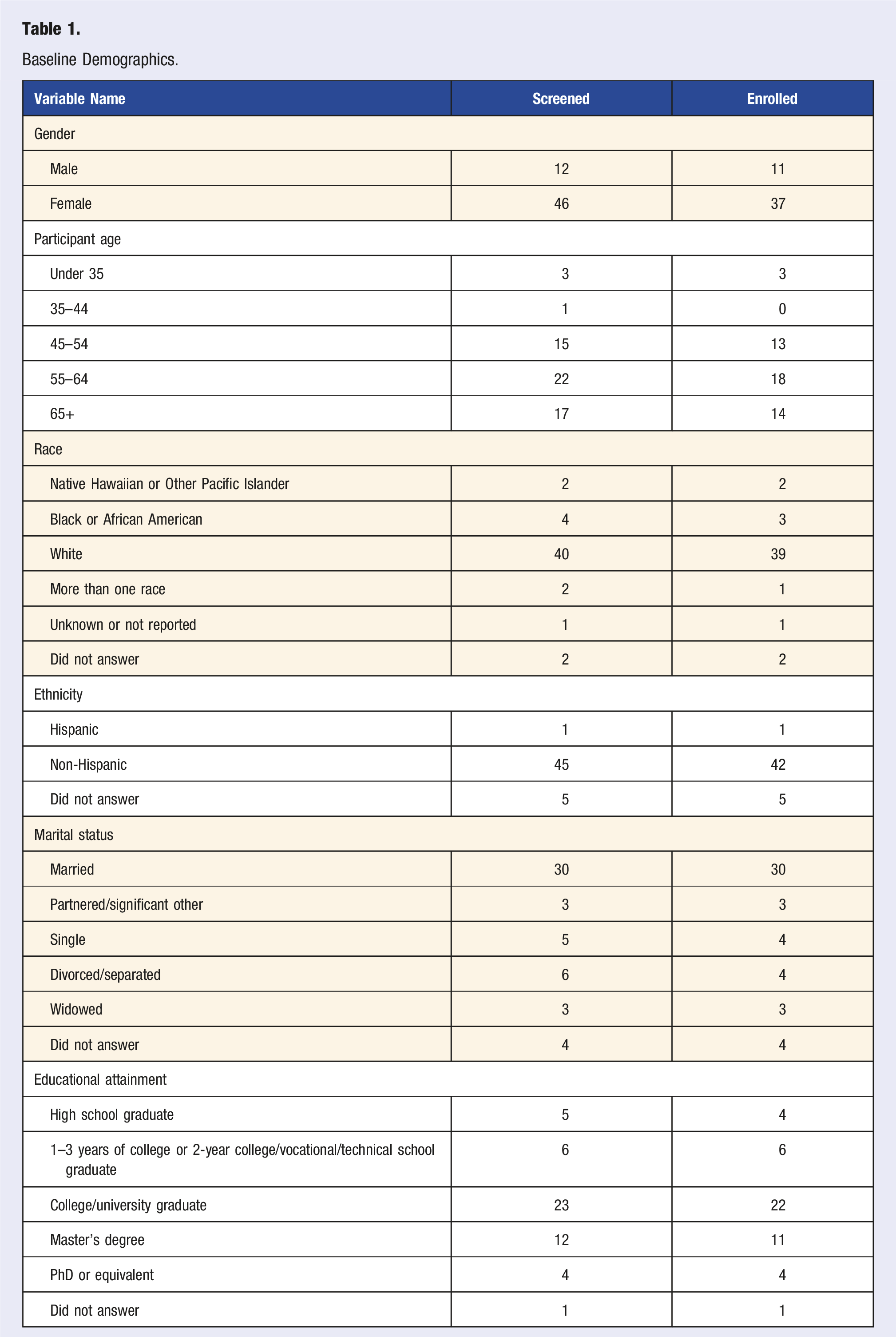
Analyses were conducted on the baseline sample (N = 51) using IBM SPSS version 26. 37 Variable distributions were inspected, and a 5% winsorization technique was applied to preserve out-of-range rank order values in the distribution while limiting their influence. 38 Demographic information was analyzed using means and standard deviations for continuous variables and frequency or percentages for categorical variables. Our analyses examined the overall effects of the program on eliciting change in the various behaviors from baseline to program completion. To do so, estimated marginal means models were computed for each instrument and corresponding sub-scales. Model effects were further decomposed using pairwise comparisons. In addition, Cohen’s d, a distribution-based effect size measure, was calculated for each outcome variable between baseline and program completion. Cohen’s d effect sizes can be interpreted as .20 as a small effect, .50 as a medium effect, and .80 as a large effect. 39
Results
Baseline Demographics.
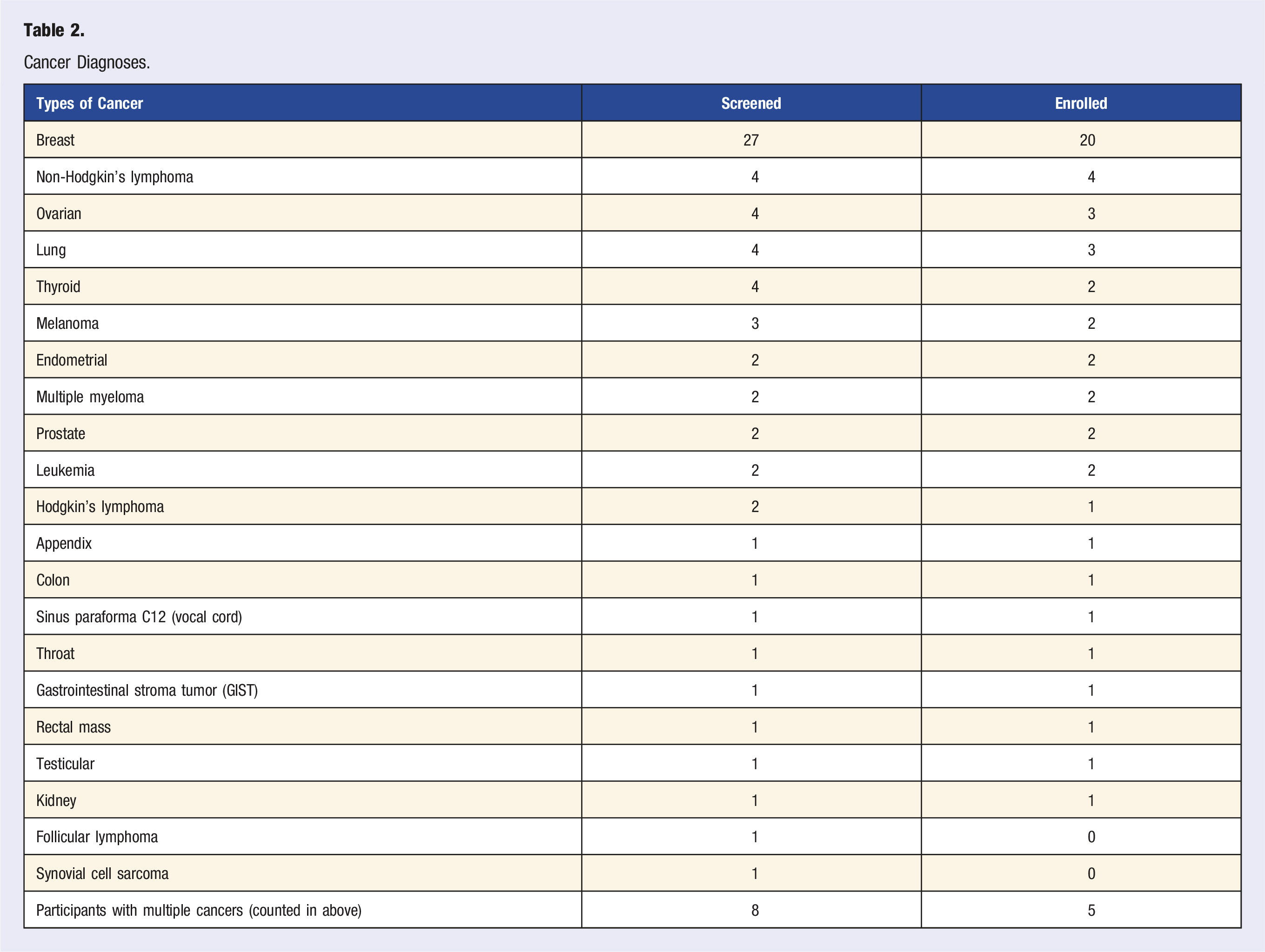
Cancer Diagnoses.
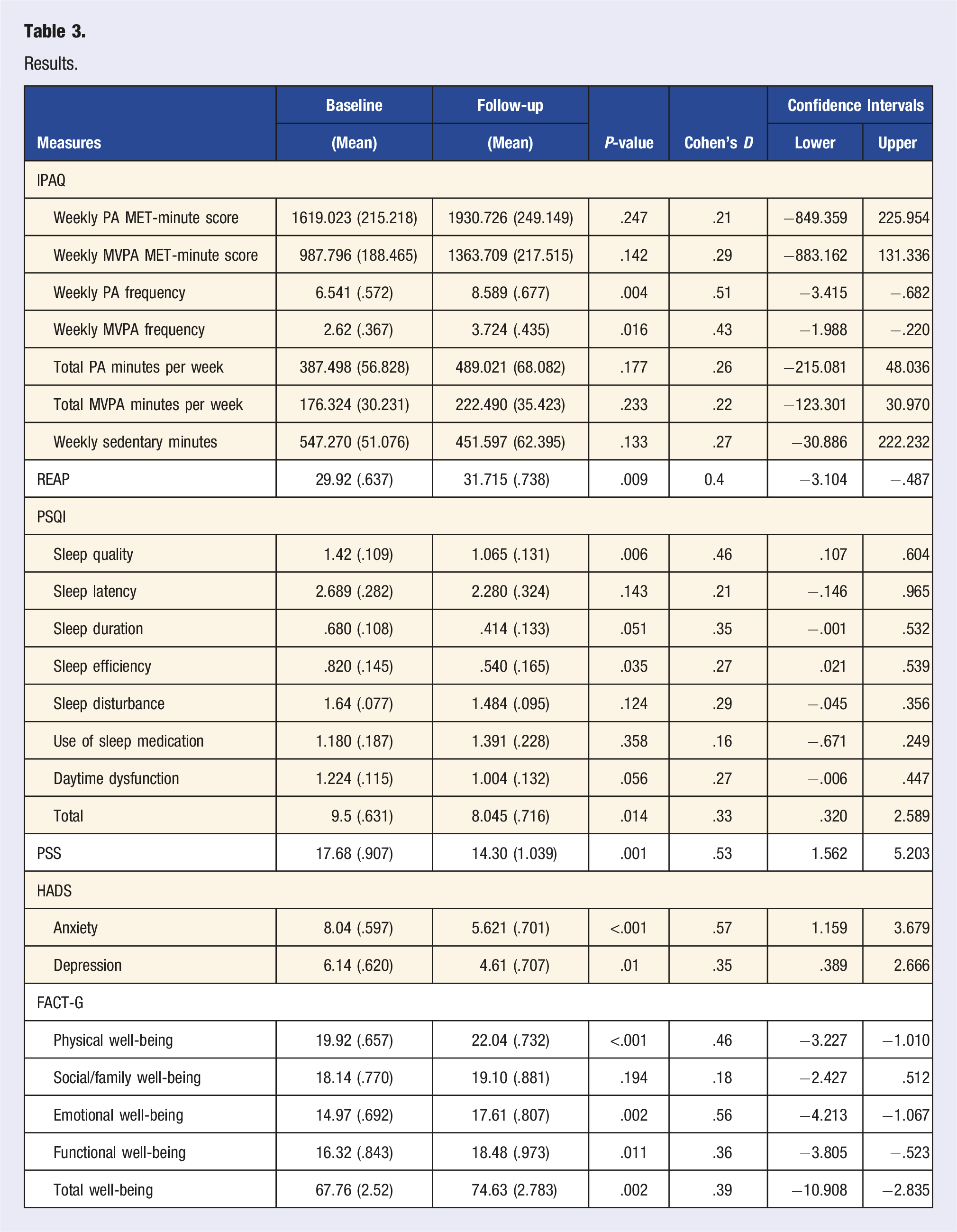
Results.
Discussion
This preliminary effectiveness study aimed to determine the real-world effectiveness of HWC for improvements in health, fitness, and overall well-being of cancer survivors within a community setting. Since survivorship is on the rise, mitigating the burden of cancer and treatment effects through the modification of lifestyle factors is imperative to improving health outcomes. 8 HWC has been shown to have positive effects on many of the outcomes considered in this study in other populations.19,40,41
From baseline to follow-up, participants reported statistically significant and clinically meaningful improvements in overall physical activity frequency and moderate–vigorous physical activity frequency, adding an average of 2 bouts of physical activity per week with 1 bout of moderate–vigorous physical activity each week. This points to participation in leisure activity more often and at a greater intensity. It has been previously noted that physical activity interventions including behavior change techniques such as goal setting, social support, and action planning are more likely to be successful at maintaining long-term results, all of which are inherent in HWC. 42 It was also noted that interventions involving older adults with physical limitations, those involving less contact with participants, and those without a supervised exercise component were more likely to be ineffective. 42 However, 60% of our participants failed the PAR-Q suggesting underlying comorbidity or physical limitation. Almost two-thirds were aged 55 or older and coaching duration was limited across 3 months, yet significant results were found, suggesting HWC may be a viable method to elicit change in a less time intensive manner. While significance was not found for the number of minutes or MET-minutes for overall and moderate–vigorous physical activity, this might be explained by a ceiling effect as our participants reported being fairly active at baseline.
A small, significant improvement was found in healthy eating behaviors. The improvement in overall healthy eating behaviors points toward participants increasing their intake of fruits, vegetables, lean proteins, and/or whole grains while reducing intake of sugar and saturated fats. 32 Prior studies assessing diet in cancer survivors have often used dietary counseling and goal setting as part of their modality, providing a foundation that HWC might elicit similar responses. 43 Coupled with increases in physical activity, this is promising for both cancer prevention and recurrence and predicted cancer outcomes.
Significant improvements in sleep, notably in quality of sleep, duration of sleep, and sleep efficacy were found, suggesting participants were sleeping longer, sleeping better, and falling asleep more quickly. Negative changes to sleep patterns in this population have been associated with more severe fatigue, having less energy and more pain, leading to impairments in performance in daily tasks, and increasing the risk of anxiety and depression.14,44 This in turn affects physical and emotional well-being which may be mitigated when the sleep disturbance is modified. While it is well known that physical activity can reduce stress and anxiety, improving sleep has also been shown to reduce symptoms of anxiety and depression and increase QoL in cancer survivors.9,13
While not directed toward a mental health intervention, coaching participants noted reductions in perceived stress, depression, and anxiety. Stress management has been shown long term to lower the number of depressive symptoms and can create better physical and emotional well-being in cancer survivors. 45 While HWC is not therapy, it is often seen as therapeutic as clients work through the goal setting process and are able to develop mastery of new skills. This increase in mastery can often lead to decreases in perceived stress and non-clinical anxiety as clients feel they are gaining more control over their behaviors and are therefore capable of handling new challenges. 46
Improvements in QoL, particularly in the areas of physical, functional, and emotional well-being, were also noted. QoL has been shown to be interrelated with, and often a byproduct of, other behavioral factors. Being physically active, improving sleep metrics, and stress management have all been shown to independently improve well-being.10,13,45 Evidence also suggests that the more healthy lifestyle behaviors a person engages in, the better their perceived QoL, so improvements in the QoL metrics could be due to independent, or a combination of, the behavior changes seen. 47
Strengths and Limitations
Compared to many other interventions, HWC is less time intensive yet may permit scaffolded behavior change to emerge through specific goal setting. Over the course of 3 months, participants met with coaches less than 5 hours total. HWC is highly individualized, allowing the cancer survivor to work on the issue most important to them while also addressing their own barriers and facilitators toward change. Having this type of flexibility within a program increases the potential for participant adherence and also future sustainability and adoptability of the program within a cancer care setting.
There are also several limitations, most notably the single group study design. Future work should consider the use of a control or comparison group to usual cancer care to increase legitimacy of the results. Participants ranged across the cancer continuum in diagnosis, stage, and various treatment interventions. The impact of coaching may have a different role for various impairments at different times, depending on whether a person is currently undergoing cancer treatment or is post-treatment. Additionally, we did not collect information on whether a client had any prior experience working with a health coach. There can be a learning curve associated with the coaching process and learning to set attainable goals, so a person familiar with health coaching may be able to make more substantial changes in the 3-month timespan, impacting results. Because participants were those who showed interest in health coaching and the data collected was completed by the participant, self-selection and self-report bias should also be considered. While subjective, this method of data collection was chosen due to the community partnership-based nature of this study to reduce participant burden while also keeping in line with other existing programs within CSCDE. While this study provides valuable information about the effectiveness of implementing a HWC intervention for cancer survivors within a community setting, the small sample size and predominately homogenous sample may limit generalizability. Further research should examine intervention effects in various subgroups of cancer survivors, for example, for different diagnostic groups within various stages, alongside duration and sustainability of coaching.
Clinical Implications and Conclusion
While long-term follow-up would be necessary to demonstrate potential survival benefits, based on the literature, it stands to reason that by making improvements in the behaviors studied here, cancer survivors could decrease their risk of developing another cancer, chronic condition, or worsening existing comorbidities, which in turn could reduce the risk of cancer-related death, improve QoL, and increase productivity. Furthermore, leveraging specific time points for regular and ongoing coaching assessments and modification of goals may provide surveillance through the trajectory of cancer survivorship. With less hands-on time needed and more flexibility available to tailor the program to the cancer survivor’s needs, HWC could be a viable way to creating lasting behavior change in this population.
Footnotes
Acknowledgments
We would like to thank the two anonymous reviewers for their constructive comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Longwood Foundation.