
Abstract
The purpose of this study to assess the effects of different protocols of physical exercise on the domains of the quality of life (QoL), sexual function, anxiety, and depression scores in women with polycystic ovary syndrome (PCOS). Data of 112 women with PCOS were extracted from 2 trials with different protocols of physical exercise: continuous aerobic training (ContinuousAT, n = 23), intermittent aerobic training (IntermittentAT, n = 22), and progressive resistance training (ResistanceT, n = 43) alongside a control group (CG, n = 24). Volunteers who completed self-report questionnaires—Female Sexual Function Index (FSFI), the Hospital Anxiety and Depression Scale (HADS), and the MOS 36-Item Short-Form Health Survey (SF-36) for QoL—preprotocol and postprotocol of physical exercise were included. Within groups, from baseline to week 16, all ContinuousAT, IntermittentAT, and ResistanceT protocols promoted improvements in multiple FSFI domains and HADS scores. However, ResistanceT did not improve the QoL aspects. Between groups, from other physical training protocols, the IntermittentAT was most effective for QoL and FSFI domains as well as HADS scores. It is concluded that all interventions were effective and improved indicators of sexual function, anxiety, and depression. When comparing protocols, interval training with high-intensity stimuli and active recovery was more effective.
‘Physical exercise may be an alternative to nonpharmacological treatment for women with PCOS’
Introduction
Polycystic ovary syndrome (PCOS) affects 8% to 18% of women of reproductive age. 1 PCOS has reproductive, psychological, and metabolic features2,3 associated with other systemic conditions such as increased risk of obesity 4 and cardiovascular events. 5 Others symptoms, including growth of body hair, menstrual problems, and infertility, can negatively affect quality of life (QoL) 6 and the feeling of femininity, 7 leading to poor mental health conditions, such as depression and anxiety,8,9 which can interfere with female sexual function.9,10
Physical exercise may be an alternative to nonpharmacological treatment for women with PCOS. Recent studies have shown that physical exercise can prevent depression at all ages 11 and may improve anxiety symptoms and prevent anxiety disorders. 12 Aerobic exercise improves general psychological distress, anxiety, and stress, whereas resistance exercise improves disorder-specific symptoms, such as general psychological distress, anxiety sensitivity, and distress tolerance. 13 Physical exercise can also improve several domains of female sexual function 14 and QoL in people with chronic diseases.15,16 In healthy women, it has been observed that aerobic exercise intensity was able to predict the frequency of sexual arousal, sexual desire, sexual intercourse, and number of orgasms in a single sexual episode, whereas strength training intensity was able to predict orgasms in a single sexual episode. Additionally, frequency in the practice of strength training was able to predict frequency of sexual desire. 17 Furthermore, people with higher levels of physical activity have better physical, psychological, social, and environmental health (ie, better QoL) than those with lower levels of physical activity. 18
In PCOS women, physical exercise is known to improve both physical and psychological health.19-22 The current guidelines include physical exercise as first-line intervention for PCOS according to World Health Organization recommendations: physical exercise at least 150 minutes per week, being 75 minutes of moderate- to high-intensity aerobic activity (60%-90% of maximum heart rate), 23 showed positive effects on the Hospital Anxiety and Depression Scale A (HADS-A) and HADS-D scores The purpose of this study is to assess the effect of various protocols of physical exercise on the domains of QoL and sexual function as well as on anxiety and depression scores in women with PCOS.
Methods
Study Patients
This is a secondary analysis of 4 parallel groups, approved by the Institutional Review Board of the University Hospital of Ribeirao Preto Medical School, University of Sao Paulo (Protocol Number No. 031802/2018). The investigation included data from 2 studies: a nonrandomized, therapeutic, open, and single-arm clinical trial (study 1) and a randomized clinical trial (study 2). The trials were designed to evaluate the effect of distinct supervised physical exercise protocols on the phenotypic characteristics of PCOS, and to investigate QoL, sexual function, and the risk of depression and anxiety, in PCOS patients. Study 1 was registered with the Brazilian Clinical Trials Registry (ReBec RBR-7p23c3), and study 2 was registered with the International Controlled Randomized Controlled Trial Registry (ISRCT-10416750). All participants provided written informed consent.
For study 1, volunteers were recruited between February 2010, and December 2013. In this case-control study, the volunteers (PCOS group and non-PCOS control group) performed progressive resistance training (ResistanceT) for muscle strengthening and hypertrophy in 1-hour sessions, 3 times a week, for 16 weeks. The program included the following exercises: bench press, leg extension, front latissimus dorsi pull down, leg curl, lateral raise, leg press (45°), triceps pulley, calf leg press, arm curl, and abdominal exercise. The program was executed in alternating segments. A linear periodization training approach was used, with decreasing volume of repetitions and increasing intensity throughout the training period (Supplementary Material 1, Tables S1 and S2). In total, 45 PCOS women completed the study.
For study 2, volunteers with PCOS were recruited between November 2014 and April 2016. This study was designed as a 3-armed randomized controlled clinical trial. The sample of this study was randomly allocated. The allocation group was placed inside opaque, sealed envelopes, grouped in blocks of 15 and consecutively picked depending on the body mass index (BMI) of the participant at the time of study inclusion. After the run-in period, 110 volunteers were randomly assigned in a 1:1:1 fashion to 1 of 3 groups: continuous aerobic training (ContinuousAT), intermittent aerobic training (IntermittentAT), or a control group (CG). Random allocation was conducted by the principal investigator and participants were enrolled and assigned to the intervention groups by research assistants. The intervention groups trained with continuous aerobic physical training (ContinuousAT) and intermittent aerobic physical training (IntermittentAT) for 16 weeks, 3 times per week, lasting equally and progressively per session, from 30 minutes in the first week, to 50 minutes in the last week. The target intensity training areas followed the American College of Sports Medicine recommendations. Light (50%-64% maximum heart rate [HRmax]), moderate (64%-77% HRmax), and vigorous (77%-94% HRmax) intensities were considered to calculate the progression of the protocols in order to be applied in the context of the clinical profile of participants. The duration of each weekly session remained the same for both protocols. However, IntermittentAT consisted of 2 minutes running at an upper intensity followed by a 3-minute resting period at recovery intensity and CAT was characterized by uninterrupted running of moderate intensity (Supplementary Material 1, Tables S1 and S2). The CG was instructed to maintain regular activity.
In both studies, PCOS was diagnosed according to the consensus criteria—that is, the presence at least 2 of the following features: chronic anovulation, hyperandrogenism (clinical or biochemical), and polycystic ovaries, based on an ultrasound. Women with congenital nonclassical adrenal hyperplasia, thyroid dysfunction, hyperprolactinemia, or Cushing syndrome were excluded (Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group, 2004). 24 Participants provided blood samples at baseline and at 16 weeks. Detailed information on these studies and physical training protocols have previously been published.21,22
For this study, the convenience sample consisted of women diagnosed with PCOS, aged between 18 and 40 years, with a BMI between 18 and 39.9 kg/m2, who completed the QoL, Female Sexual Function Index (FSFI), and HADS questionnaires and completed the proposed physical training protocols for studies 1 and 2. In total, 45 volunteers in the ResistanceT group, 28 in the ContinuousAT group, 29 in the IntermittentAT group, and 30 in the CG completed the study (see Supplementary Material 2).
Instruments and Materials
QoL was assessed by the validated Portuguese version of the self-reported MOS 36-Item Short-Form Health Survey (SF-36). The SF-36 is a multidimensional questionnaire and includes the aspects of functional capacity, physical limitations, pain, general health, vitality, and social, emotional and mental health. Scores range from zero (lowest QoL) to 100 (highest QoL) for each domain. 25 The risk of anxiety and depression was evaluated using the HADS, which consists of a 14-item self-report questionnaire: 7 to evaluate the risk of anxiety and 7 to evaluate the risk of depression. The overall score for each subscale ranges from zero to 21. Scores of ≥8 and ≥9 were established as cutoff points for the risks of anxiety and depression. 26 Sexual function was assessed using the validated FSFI,27,28 which includes 6 subscales for the assessment of desire, arousal, lubrication, orgasm, satisfaction, and dyspareunia. The subscale scores have been corrected and summed, with final scores ranging from 2 to 36, and scores ≤26.55 indicating that the patient is at risk for sexual dysfunction. For sexual function, all women were asked to state whether they were sexually active (ie, whether they had engaged in sexual activity in the past 6 months), at baseline, and again after 16 weeks.
Statistical Analysis
Exploratory data analysis was performed using central position and dispersion measures. Data are presented as the means, SDs, and estimations of variance (95% CI for difference). Qualitative variables are expressed as absolute and relative frequencies, and the comparison between the 4 groups was performed using analysis of variance. A linear regression model of mixed effects was performed to see which factors were related to the characteristics of the results. The variables group, time, Time × Group interaction, BMI, testosterone levels, and age, were considered as covariables. Model adjustments were checked by residual analysis. Statistical significance was set at the level of P < .05. Analyses were performed using SAS 9.3 software (SAS Institute Inc, University of North Carolina, NC).
Results
A total of 112 women with PCOS participated in this study. Two volunteers were excluded after screening for eligibility criteria, leaving a total of 43 women participating in study 1. In study 2, 69 women who had been sexually active over the previous 6 months were eligible: 23 in the ContinuousAT group, 22 in the IntermittentAT group, and 24 in the CG (see Supplementary Material 2). Table 1 shows the descriptive characteristics of the study sample. There were no significant variations in variables for age, weight, and BMI between the 4 groups. However, the ContinuousAT group had a higher baseline testosterone level.
Descriptive Characteristics.
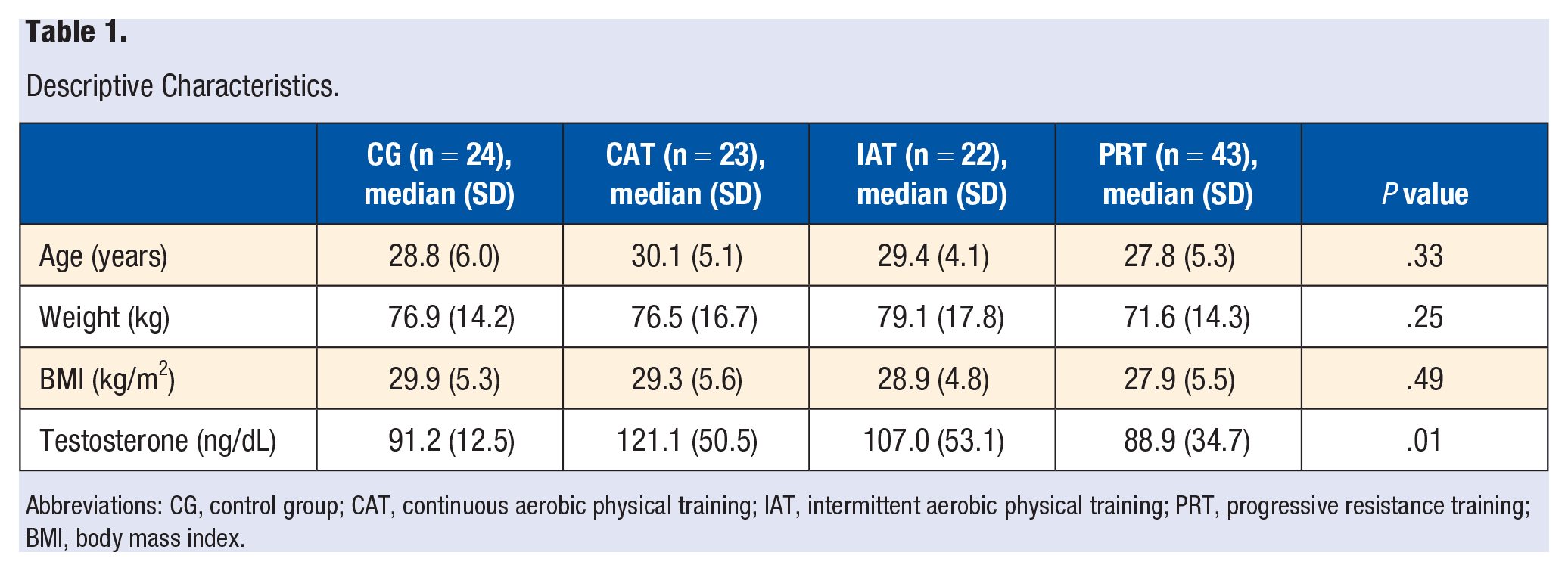
Abbreviations: CG, control group; CAT, continuous aerobic physical training; IAT, intermittent aerobic physical training; PRT, progressive resistance training; BMI, body mass index.
Intragroup Analyses
In Table 2, the FSFI, SF-36, and HADS measurements, before and after the ContinuousAT, IntermittentAT, ResistanceT, and nontraining period, are reported in within-group comparisons. Analysis of the FSFI domains showed that at week 16, the ContinuousAT group had improved its total FSFI score (P < .01) and the scores for arousal, desire, and pain (P < .05). The IntermittentAT group had improved its total FSFI score (P < .01) and the scores for desire, lubrication, and orgasm (P < .01). In the ResistanceT group, improvements were seen in the total FSFI score (P < .0001) and desire, arousal, lubrication (P < .0001, all), pain (P < .01), and satisfaction (P < .05). No differences were observed in the CG after the intervention.
Measurements of FSFI, SF-36, and HADS Preintervention and Postintervention for CG, CAT, IAT, and PRT Within Groups. a
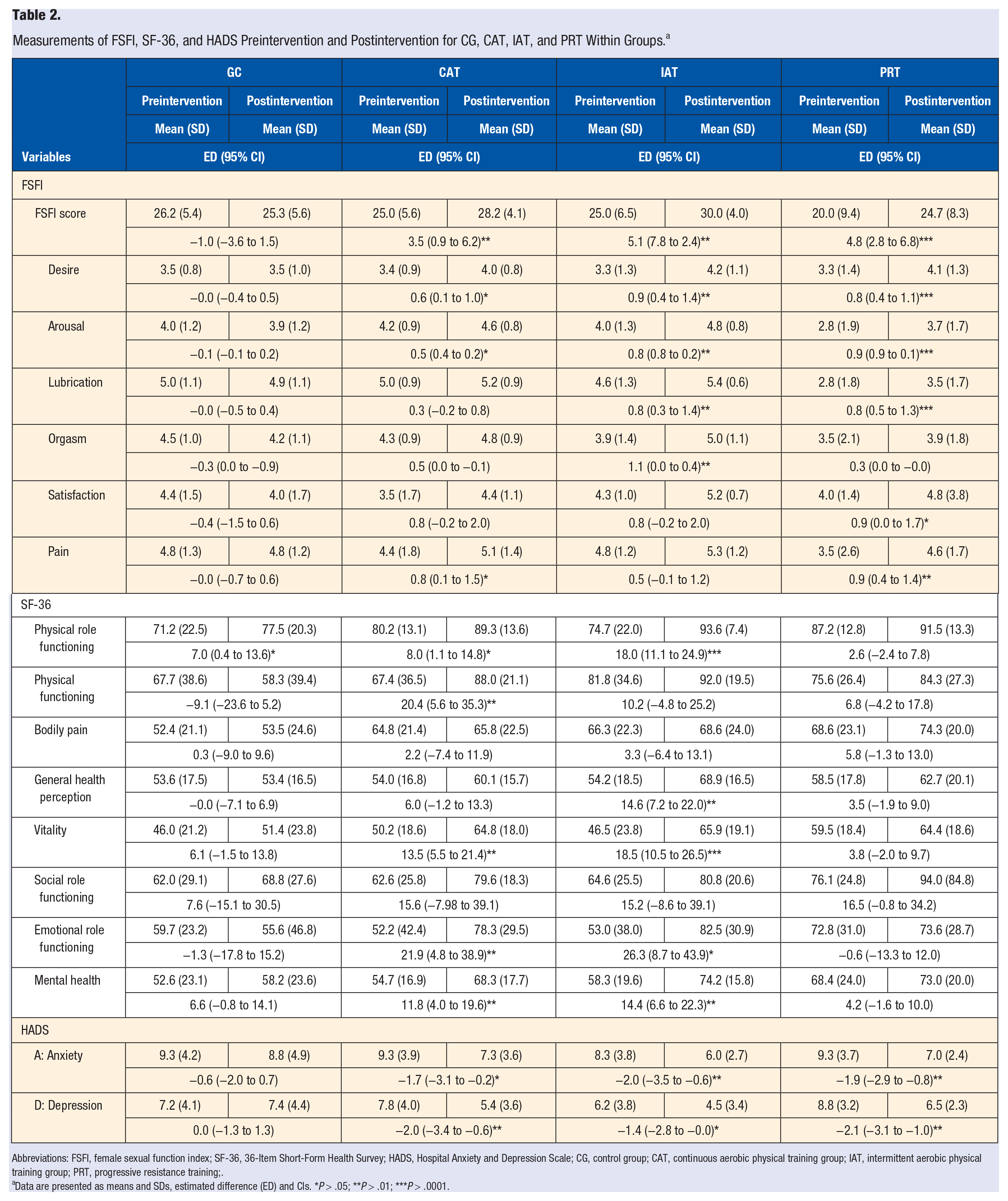
Abbreviations: FSFI, female sexual function index; SF-36, 36-Item Short-Form Health Survey; HADS, Hospital Anxiety and Depression Scale; CG, control group; CAT, continuous aerobic physical training group; IAT, intermittent aerobic physical training group; PRT, progressive resistance training;.
Data are presented as means and SDs, estimated difference (ED) and CIs. *P > .05; **P > .01; ***P > .0001.
Analysis of the SF-36 questionnaire showed that, from baseline to week 16, the ContinuousAT group’s scores improved for physical role function (P < .05), vitality, mental health, physical functioning, and emotional role functioning (P < .01). The IntermittentAT group’s scores improved for physical role functioning, vitality (P < .0001), general health perception, mental health (P < .01), and emotional role functioning (P < .05). The CG showed significantly improved scores for physical role functioning (P < .05). For the ResistanceT group, there were no significant changes in the SF-36 questionnaire scores.
Analysis of the HADS showed that from baseline to week 16, the groups with interventions had improved their HADS-A (CAT, P < .05; IntermittentAT and ResistanceT, P < .01) and HADS-D scores (IntermittentAT, P < .05; ContinuousAT and ResistanceT, P < .01).
Intergroup Analyses
The comparison of FSFI measurements between the groups at baseline and after 16 weeks are presented in Figure 1. At baseline, when compared to the CG and ContinuousAT and IntermittentAT groups, the ResistanceT group showed a significant difference in total FSFI score for the domains of arousal, lubrication, orgasm, and pain. There were no differences in comparison between the ContinuousAT and IntermittentAT groups. At week 16, compared to the CG, the IntermittentAT group showed an improved total FSFI score and desire domain score (P < .05). Compared to the ResistanceT group, the IntermittentAT group showed an improved total FSFI score (P < .05) as well as improvements in the domains of arousal (P < .01), lubrication (P < .0001), and orgasm (P < .05). The ContinuousAT group showed improvement in the FSFI domains of arousal (P < .05) and lubrication (P < .0001).
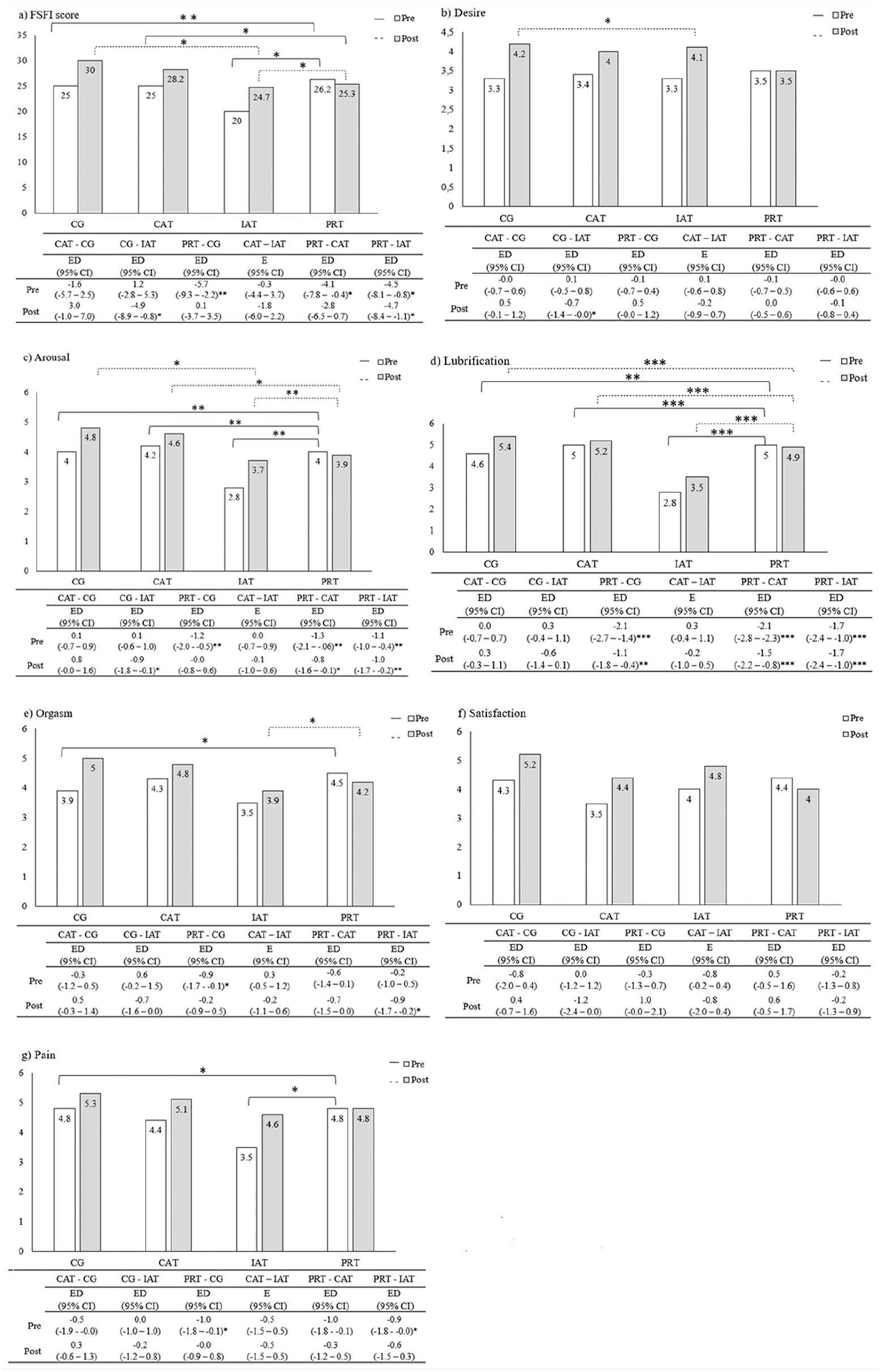
FSFI measurements at baseline and week 16 between groups: Data are presented as means, estimated difference (EDs), and CIs.a
Table 3 shows the SF-36 score measurements between groups at baseline and at week 16. At baseline, compared to the CG, the ResistanceT group showed different scores for mental health, vitality, and physical role functioning; the ContinuousAT group showed significant differences for physical role functioning. At baseline, compared to the IntermittentAT group, the ResistanceT group showed different scores for vitality and physical role functioning. At week 16, compared to the CG, the ContinuousAT group showed improvements in physical role functioning, physical functioning, vitality, and emotional role functioning (P < .05l). The IntermittentAT group showed improved scores for physical role functioning, physical functioning, bodily pain, general health perception, vitality, emotional role functioning, and mental health (P < .05, all). The ResistanceT group showed improved scores for physical role functioning, physical functioning, body pain, and mental health (P > .05). Comparisons between the ResistanceT and ContinuousAT groups, as well as comparisons between ContinuousAT and IntermittentAT, showed no differences at baseline or at week 16.
SF-36 Scores Measurements at Baseline and Week 16 Between Groups. a
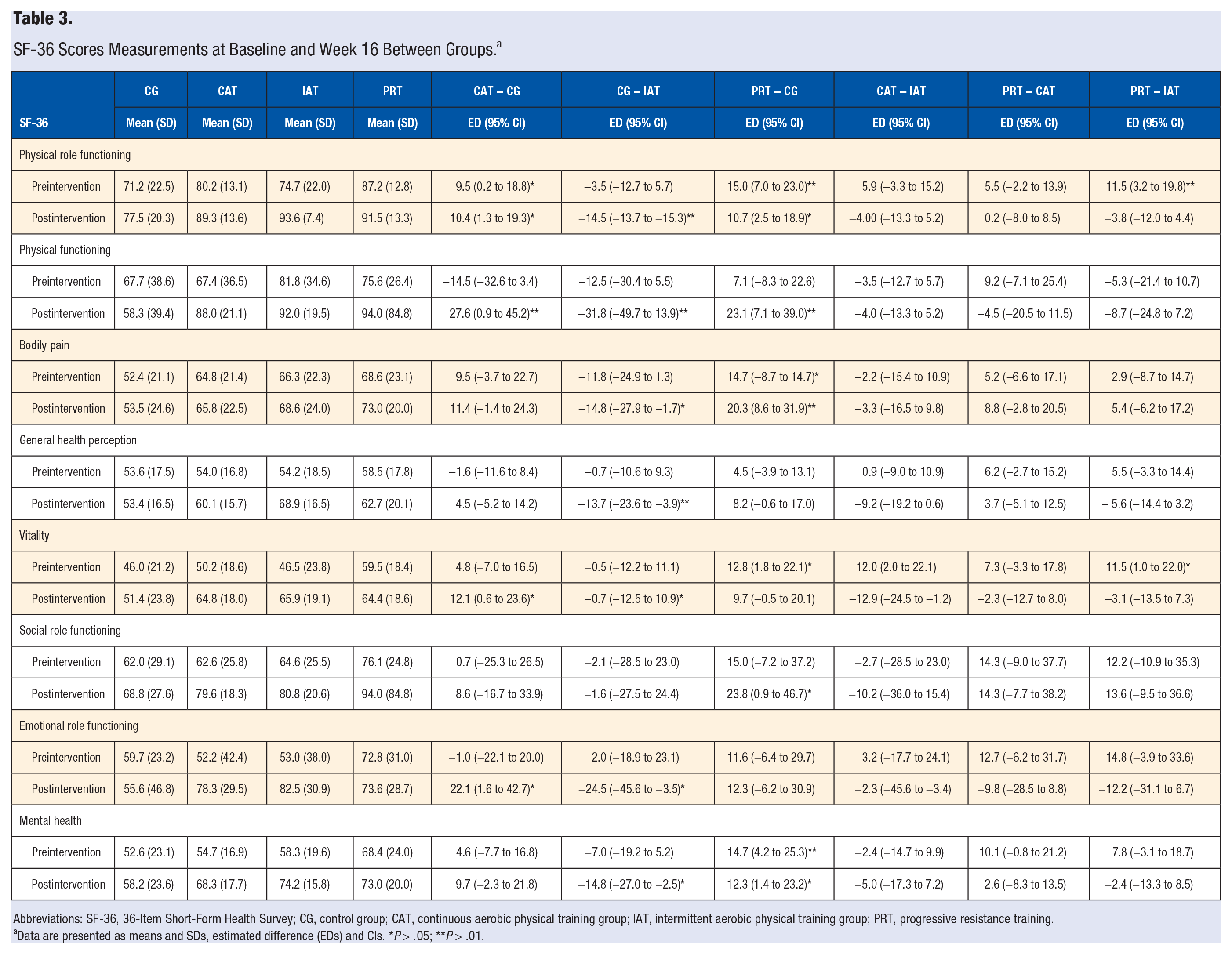
Abbreviations: SF-36, 36-Item Short-Form Health Survey; CG, control group; CAT, continuous aerobic physical training group; IAT, intermittent aerobic physical training group; PRT, progressive resistance training.
Data are presented as means and SDs, estimated difference (EDs) and CIs. *P > .05; **P > .01.
The HADS measurements between the groups at baseline and after 16 weeks are presented in Figure 2. In the HADS-A, there were no differences between groups at baseline. At week 16, compared to the ContinuousAT group, only the IntermittentAT group showed improvement (P < .05). In the HAD-D, at baseline, the ResistanceT group showed different scores to the CG (P = .05) and the IntermittentAT group (P > .01). In depression, only the IntermittentAT group showed improvement, compared to the CG and the ResistanceT group (P < .05).
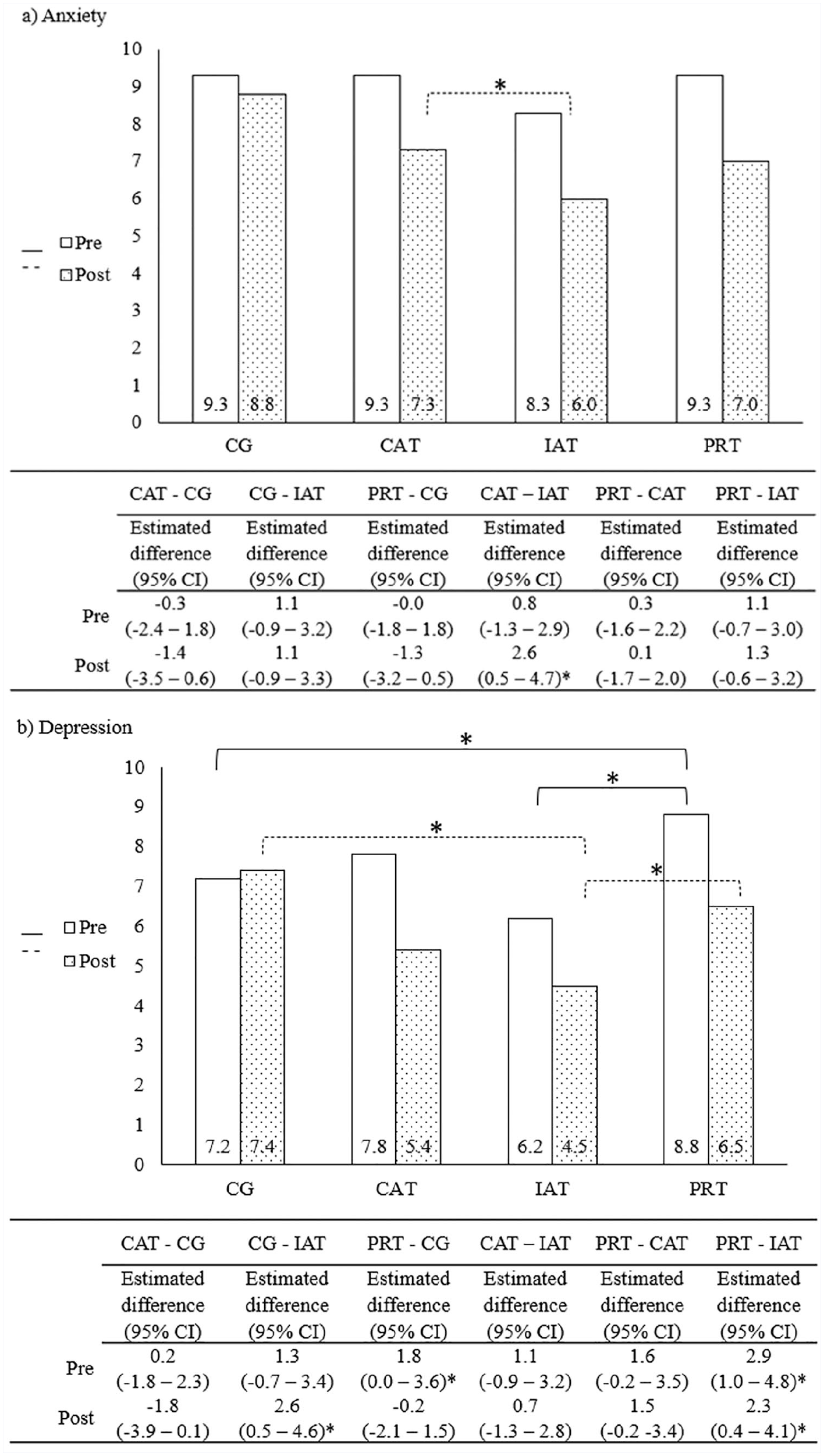
HADS measurements at baseline and week 16 between groups. Data are presented as means, estimated difference (EDs) and CIs.a
Discussion
The aim of this study was to investigate whether different physical exercise protocols can affect well-being in women with PCOS. Our results indicate that, regardless of the protocol, physical exercise improves scores for anxiety and depression. However, the results from all 3 experiments suggest that, compared to other protocols, IntermittentAT has the greatest positive influence on total FSFI score for the domains of desire, arousal, lubrication, and orgasm. Compared to the CG, all exercises performed (ContinuousAT, IntermittentAT, and ResistanceT) also had the greatest positive influence on the HADS-A and HADS-D scores. In terms of QoL, compared to the CG, the 3 protocols showed positive effects in several domains. At baseline, testosterone levels were significantly different between groups. However, this difference was controlled in the linear mixed-effects regression model and the variables BMI, age, group, time, and Time × Group interaction.
It is worth highlighting that this is the first study that compares the effects of aerobic and strength training protocols on QoL, sexual function, and anxiety and depression in women with PCOS. Previously, our research team observed that, compared with healthy women, 16 weeks of ResistanceT helped improve scores for the FSFI, for the domains of desire, excitement, lubrication, and pain in women with PCOS. 29 It was also observed, that 16 weeks of intermittent aerobic exercise improved the FSFI domain scores for desire, arousal, lubrication, orgasm, and satisfaction in women with PCOS. 30 In this analysis controlled by covariates, comparisons within groups show that the 16-week ResistanceT protocol for strength and hypertrophy was more effective when compared to ContinuousAT and IntermittentAT protocols or to the CG in improving a larger number of FSFI domains: desire, arousal, lubrication, pain, and satisfaction. However, an intergroup comparison shows that the IntermittentAT 16-week exercise protocol with high-intensity stimuli and active recovery was more effective. Little is known about the true role of physical exercise in the sexual function of women with PCOS. In obese and infertile women, including PCOS patients, it was observed that a 6-month lifestyle intervention with moderate physical exercise—approximately 10 000 steps per day—and reduced daily caloric intake can have beneficial long-term effects on sexual health, with more vaginal lubrication and a better overall sexual function. Moreover, these authors noted that the effect of the intervention on sexual function can be partially mediated by the change in physical activity. 31
In middle-aged women, physical exercise has a positive impact on sexual function. A recent study showed that, compared with moderately active and sedentary women, very physically active women scored higher in all FSFI domains (desire, arousal, lubrication, orgasm, satisfaction, and pain). 32 There are reports that arousal can be predicted by cardiovascular endurance, total self‑concept may be related to both orgasm and desire, and muscular strength may be related to the number of sexual partners. 33 However, the sexual arousal has physiological and subjective arousal associated with positive mental engagement. 34 Therefore, an improvement in physiological sexual arousal can occur immediately after an exercise session or acute exercise. It may be a result of increased sympathetic nervous system activity and endocrine factors. Additionally, chronic exercise may indirectly enhance women’s sexual response, via positive effects on cardiovascular health, mood, and body image. 14 However, the actual effect of physical exercise on the domains of sexual function in women with PCOS has not yet been established as well as the possible relationships and mechanisms between mood disorders, self-image distortions, metabolic parameters, and sexual function in this group of women.
The benefits of physical exercise on QoL are subjective and depend on the individual and the circumstances. 35 A pioneering study in PCOS patients has shown that 16 weeks of aerobic exercise, without direct supervision and monitoring, improves only the physical functioning domain. 36 Recently, a study that included progressive overload and aerobic exercise session supervision observed that health-related QoL improved in the SF-36 physical functioning, general health, and mental health domains in women with this condition. 20 Our research team has shown that 16 weeks of continuous and intermittent aerobic exercise improves several domains of the SF-36 in women with PCOS. 37 In a previous analysis, only the functional capacity domain showed a modest improvement after a period of 16 weeks of performing supervised resistance training. 38 In this controlled analysis, only the aerobic training protocols ContinuousAT and IntermittentAT improved several domains of the SF-36 questionnaire. From the control group, specific exercise intensities were related to different parameters of QoL. However, IntermittentAT protocol, with high-intensity stimuli and active recovery, was more effective at improving multiple SF-36 domains than other protocols: physical role functioning, physical functioning, bodily pain, general health perception, vitality, emotional role functioning, and mental health.
Although robust IntermittentAT programs are designed to improve various clinical aspects, 39 the influence of the intensity in this protocol has never been tested on the QoL of women with PCOS. In previous studies, both high-intensity interval training (HIIT) and ContinuousAT, by 12 weeks, were effective in improving only the domains of physical function that showed the greatest benefit from the intervention (HIIT or ContinuousAT). 40 In healthy adults, HIIT, performed 2 or 3 times per week, for 8 weeks, improves elements of QoL related to physical health. Performed 3 times per week, for 3 weeks, HIIT promotes benefits related to mental health. 41 In adults diagnosed with moderate to high cardiovascular risk, the protocol of HIIT and resistance exercise improves the social functioning and physical role functioning domains as well as the total FSFI SF-36 score. The same duration of ContinuousAT and resistance exercise only improved the general health domain. 42
Supervised exercise interventions have antidepressant effects in people with depression 11 and anxiety disorders. 12 However, few studies have shown the use of physical activity to treat these disorders in PCOS women. We have previously shown that resistance exercise and distinct aerobic exercise protocols reduce the risk of anxiety and depression in women with PCOS.29,30 This current analysis adjusted for confounding variables as in Kogure et al 43 and found that although all physical training protocols were effective in reducing anxiety and depression scores, the IntermittentAT protocol with progressive intensity stimuli and active recovery was the most effective. Earlier meta-analyses have shown that moderate- and vigorous-intensity exercise is more effective than light- to moderate-intensity exercise in treating major depressive disorders. 11 In healthy women, although 2 distinct protocols of HIIT improved depressive symptoms, they did not improve anxiety symptoms. 44 On examining exercise types, only aerobic exercise significantly influenced depression and not the mixed interventions. 45 These findings warrant further investigation because there have been no randomized controlled trials that investigate the effects of resistance exercise in samples of major depression. 11
Recently, Tonello et al 46 noted that depressive symptoms in sedentary women are related to cardiorespiratory fitness and body fat levels. In this sense, the IntermittentAT with vigorous intensity may be of interest to different populations because of its beneficial effect on cardiorespiratory fitness and other health-related parameters.47,48 A previous systematic review noted that aerobic exercise was effective in the treatment of patients with clinical anxiety and that high-intensity exercise may be more effective than low-intensity exercise 49 and resistance training 50 These beneficial effects may be a result of multiple mechanisms by which several biomarkers and parameters are altered. Exercise increases the availability of neurotransmitters, neurotrophins, and neurogenesis; reduces the serum levels of proinflammatory cytokines; contributes to the modulation of the hypothalamic-pituitary-adrenal axis; increases the plasma levels of endocannabinoids; and increases positive growth factors. 51
This study has some limitations. A convenience sample for the ResistanceT group was analyzed along with randomized samples for the ContinuousAT and IntermittentAT interventions. This may primarily be a bias in the pooled analysis of the entire sample’s baseline characteristics. However, in the statistical analysis, all variables that could interfere with the actual impact of the protocols on the domains of sexual function, QoL, and anxiety and depression scores were controlled. In addition, another limitation of this study was that sociodemographic characteristics were not analyzed. Finally, we did not assess stressful life events and the cognitive, behavioral, and physiological aspects of the response to stress. We concluded that after 16 weeks, all interventions were effective in improvement of indicators of sexual function, and anxiety and depression, with the exception of strength training for QoL aspects. When comparing protocols, the IntermittentAT with high-intensity stimuli and active recovery was the most effective. Our findings, combined with the benefits of exercise for physical health and well-being, reinforce exercise as an important treatment option for PCOS women. However, the comparative efficacy of aerobic and resistance exercise, the ideal frequency, duration, and intensity of the exercise, and mechanisms and pathways require further investigation.
Supplemental Material
sj-docx-1-ajl-10.1177_15598276211001330 – Supplemental material for Distinct Protocols of Physical Exercise May Improve Different Aspects of Well-being in Women With Polycystic Ovary Syndrome
Supplemental material, sj-docx-1-ajl-10.1177_15598276211001330 for Distinct Protocols of Physical Exercise May Improve Different Aspects of Well-being in Women With Polycystic Ovary Syndrome by Gislaine Satyko Kogure, Lúcia Alves da Silva Lara, Victor Barbosa Ribeiro, Iris Palma Lopes, Maria Célia Mendes, Sérgio Kodato, Rui Alberto Ferriani, Cristiana Libardi Miranda Furtado and Rosana Maria dos Reis in American Journal of Lifestyle Medicine
Supplemental Material
sj-docx-2-ajl-10.1177_15598276211001330 – Supplemental material for Distinct Protocols of Physical Exercise May Improve Different Aspects of Well-being in Women With Polycystic Ovary Syndrome
Supplemental material, sj-docx-2-ajl-10.1177_15598276211001330 for Distinct Protocols of Physical Exercise May Improve Different Aspects of Well-being in Women With Polycystic Ovary Syndrome by Gislaine Satyko Kogure, Lúcia Alves da Silva Lara, Victor Barbosa Ribeiro, Iris Palma Lopes, Maria Célia Mendes, Sérgio Kodato, Rui Alberto Ferriani, Cristiana Libardi Miranda Furtado and Rosana Maria dos Reis in American Journal of Lifestyle Medicine
Footnotes
Acknowledgements
We would like to thank all the participants who volunteered for this study. Authors also thank Henrique Reis Moura for technical support with the English review.
Authors’ Note
All authors made substantial, direct, and intellectual contributions to the work and approved it for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the National Council for Scientific and Technological Development (CNPq, Finance Code 001), the Coordination for the Improvement of Higher Education Personnel (CAPES, Finance Code 001), and Sao Paulo Research Foundation (FAPESP), with the Grants 2010/08800-8 and 2015/14031-0 (RMdR) and fellowship 2012/11069-9 (CLMF).
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.