
Abstract
Lifestyle risk factors, including tobacco and alcohol use, poor nutrition, and inactivity, comprise the leading actual causes of death and disproportionately affect diverse, lower-income and vulnerable populations. Fundamentally influenced by social determinants of health (including poverty, social linkages, food access, and built environment), these “unhealthy lifestyle” exposures perpetuate and sustain disparities in health outcomes, stealing years of healthy and productive life for minority, vulnerable groups. The authors call for implementation of a health equity framework within lifestyle medicine (LM). Community-engaged lifestyle medicine (CELM) is an evidence-based, participatory framework capable of addressing health disparities through LM, targeting health equity in addition to better health. CELM was developed in 2015 by the University of Texas Rio Grande Valley (UTRGV) Preventive Medicine Residency program to address lifestyle-related health disparities within marginalized border communities. The framework includes the following evidence-based principles: community engagement, cultural competency, and application of multilevel and intersectoral approaches. The rationale for each of these components and the growth of CELM within the American College of Lifestyle Medicine is described. Finally, illustrative examples are provided for how CELM can be instituted at micro and macro levels by LM practitioners.
‘Despite overall improvements in life expectancy and quality of health care in the United States, health disparities between certain groups have actually widened.’
Background
Lifestyle is the most fundamental and modifiable influence on risk of disease. Lifestyle risk factors, including tobacco and alcohol use, poor nutrition, and inactivity, comprise the leading actual causes of death. 1 Today, 65% of the world’s population lives in a country where overweight and obesity kill more people than underweight and malnutrition. 2 The 6 leading global risks for mortality, common to low-, middle-, and high-income countries, include high blood pressure, tobacco use, high blood glucose, inadequate physical activity, overweight, and obesity 2 . 70% to 90% of the most common and deadly chronic diseases, including diabetes, coronary artery disease, stroke, and cancer, could be prevented via tobacco cessation, avoidance of overweight, moderate physical activity, and a healthy diet. 3
The Need for Health Equity–Oriented Lifestyle Medicine
Worldwide, lifestyle risk factors disproportionately affect diverse, lower-income, and vulnerable populations. 2 These adverse lifestyle exposures—fundamentally influenced by social determinants of health such as poverty, built environment, education, and food access—systematically perpetuate and sustain pervasive disparities in health outcomes, stealing years of healthy and productive life for minority, vulnerable groups. 4
Based on preventable and “unnatural” causes, lifestyle-related health disparities are unjust.5,6 The United States has some of the largest health inequities in the developed world, occurring by ethnicity, geography, and socioeconomic status.7,8 On average, black men and women die 6.3 and 4.5 years earlier than their white counterparts. 9 One 2006 study illustrated that men and women in the best-off groups in the United States lived almost a decade and half longer (15.4 and 12.8 years, respectively) than worst-off groups; the persistent race-based gap in life expectancy had not narrowed significantly since 1987. 10 Despite overall improvements in life expectancy and quality of health care in the United States, health disparities between certain groups have actually widened. 11 Mortality rates for Native Americans are almost 50% higher than that for Caucasians; Native Americans are twice as likely to have diabetes, are twice as likely to have posttraumatic stress disorder, and are more likely to die from diabetes and heart disease. 12 Compared with Caucasians, Hispanic Americans are 63% more likely to have diabetes and 30% more likely to die from the disease.13,14 Preventable and modifiable risk factors for cardiovascular disease, diabetes, and blood pressure drive these differences in health. Indeed, researchers calculated that if levels of blood pressure, blood sugar, body fat, and smoking were controlled to optimal levels in vulnerable subgroups, disparities in cardiovascular disease deaths would be eliminated by 80%. 9 Preventable health disparities are a threat to economic sustainability and affect the well-being of all residents; one estimate suggests that US health disparities cost more than $1.24 trillion. 15
Although proven to treat, prevent, and reverse lifestyle-related chronic disease and its precursors, narrow lifestyle medicine (LM) prevention efforts could inadvertently widen health disparities, especially if least-accessible populations (those at highest risk of disease) are missed.16,17 This phenomenon occurred with cardiovascular disease prevention efforts in the United States: over the past several decades, mean serum cholesterol and prevalence of tobacco use dropped most in high-income groups, whereas prevalence of certain chronic diseases and lifestyle risk factors actually increased in lower-income groups.18,19
Community-Engaged Lifestyle Medicine (CELM) as a Health Equity Pathway
Health equity is defined as the “principle underlying a commitment to reduce—and ultimately, eliminate disparities in health and in its determinants, including social determinants.” 20 Building health equity is a goal that is within scope, reach, and mission of LM health care reform and can be achieved through momentum of an organized and collective, rather than ad hoc and individual, approach. Evidence suggests that organized, multilevel and tailored disease prevention efforts targeting health equity are feasible on local, national, and global levels and can successfully narrow disparities in diverse groups around the world.13,14
CELM is defined as the practice of preventing chronic disease and promoting healthy lifestyle behaviors via collaborative, multistakeholder, and community-engaged delivery of LM in diverse, low-income populations. 21 Originally developed at the University of Texas Rio Grande Valley (UTRGV, Edinburg, Texas) in 2016, under the primary author’s leadership of the Preventive Medicine Residency Program and collaboration with public, private, and community stakeholders, CELM is an evidence-based framework for promoting health equity in low-resource settings. In the Rio Grande Valley, CELM informed a community-driven effort for lifestyle improvement that engaged some of the most historically marginalized, impoverished border communities in the United States. 21 In this region of approximately 1.3 million, 35% of the population lives in poverty, compared with 17% at the national level; more than one-third are ineligible for health insurance.22-25 Nearly half the population (45%) is obese, and more than a quarter (22%) have diabetes. 23 The specific CELM objectives (grouped into the themes of Engagement, Evaluation, and Education) and the collaborative development and evaluation process for the CELM framework are described in detail elsewhere. 21
Evidence-based pathways to health equity feature 2 broad themes. The first, capacity-building partnerships, is a form of community activism that can ameliorate social determinants of poverty, food deserts, and community safety over time, through tenacious intersectoral partnerships operating at local, state, and federal levels and including representatives of vulnerable groups. The second theme engages health care providers to broaden health care impact by building health outside the hospital: engaging and empowering historically marginalized groups to reduce and eliminate lifestyle risk factors for common chronic diseases through culturally tailored LM outreach in clinical and community settings. Addressing the first theme comprehensively is often outside the scope of work for many LM practitioners. Indeed, one of the limitations of CELM is its inability to target the deeper societal power dynamics and structural discrimination that instigate and sustain pervasive disparities. Nonetheless, the CELM approach can help LM practitioners begin building the long-term health equity partnership infrastructure and momentum needed to address deeper social inequities, via engagement of diverse populations and expanding the reach of LM beyond the clinic walls. 21
The specific principles of CELM have evidence-based associations with health equity and include community engagement (CE), multilevel and intersectoral approaches, and cultural responsiveness. CE refers to partnership and involvement of marginalized community members and stakeholders along all stages of health interventions (identifying priorities and needs, designing and delivering the intervention, and analysis and dissemination of results). By partnering respectfully with the community of interest, CE supports the creation of culturally tailored programs and can add meaningful value in furthering desired health outcomes.26,27 Multilevel approaches to changing lifestyle address the interconnected influences of levels of individual, peer/family group, health care team, neighborhood resources, and cultural context and, therefore, increase the likelihood that patients can sustain behavior changes outside the health care setting.28,29 Intersectoral partnerships, which refers to the coordination of clinical services with participation and resources drawn from the social, political, environmental, and economic sectors, build sustainability, momentum, and capacity for community-driven LM. 30 Finally, cultural responsiveness is a crucial element of provider training and philosophy, enabling the delivery of tailored services that are “respectful of and responsive to the health beliefs, practices, and cultural needs of diverse patients.” 31 Table 1 summarizes these principles, along with examples of general LM applications and those within the UTRGV Preventive Medicine residency program.
Health Equity Principles of Community-Engaged Lifestyle Medicine and Associated Practice Applications Within LM and the UTRGV Preventive Medicine Residency.
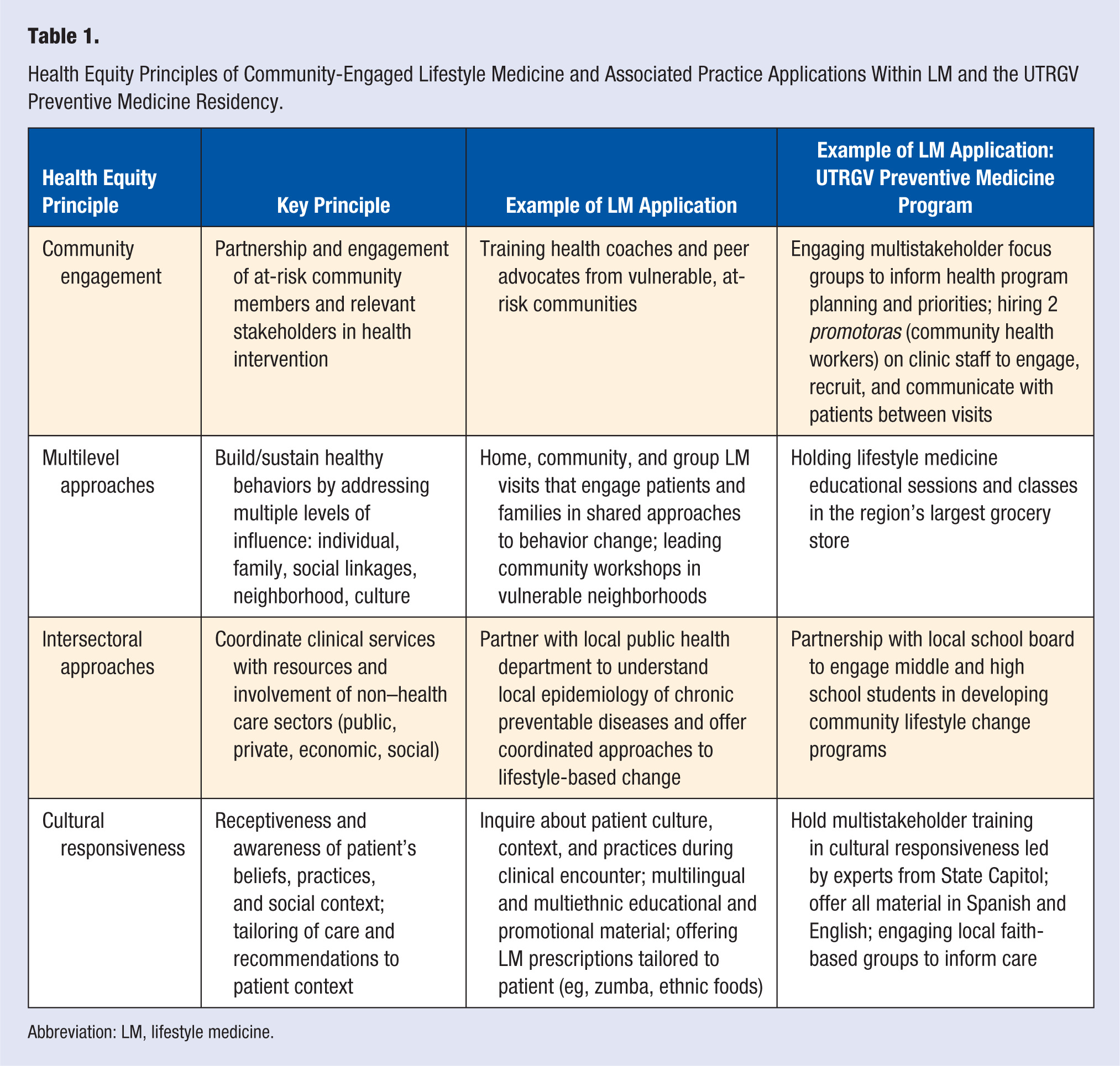
Abbreviation: LM, lifestyle medicine.
Figure 1 illustrates the CELM logic model, highlighting the role of coordinated, community-clinic linkages and the emphasis on quality improvement and continuous evaluation.
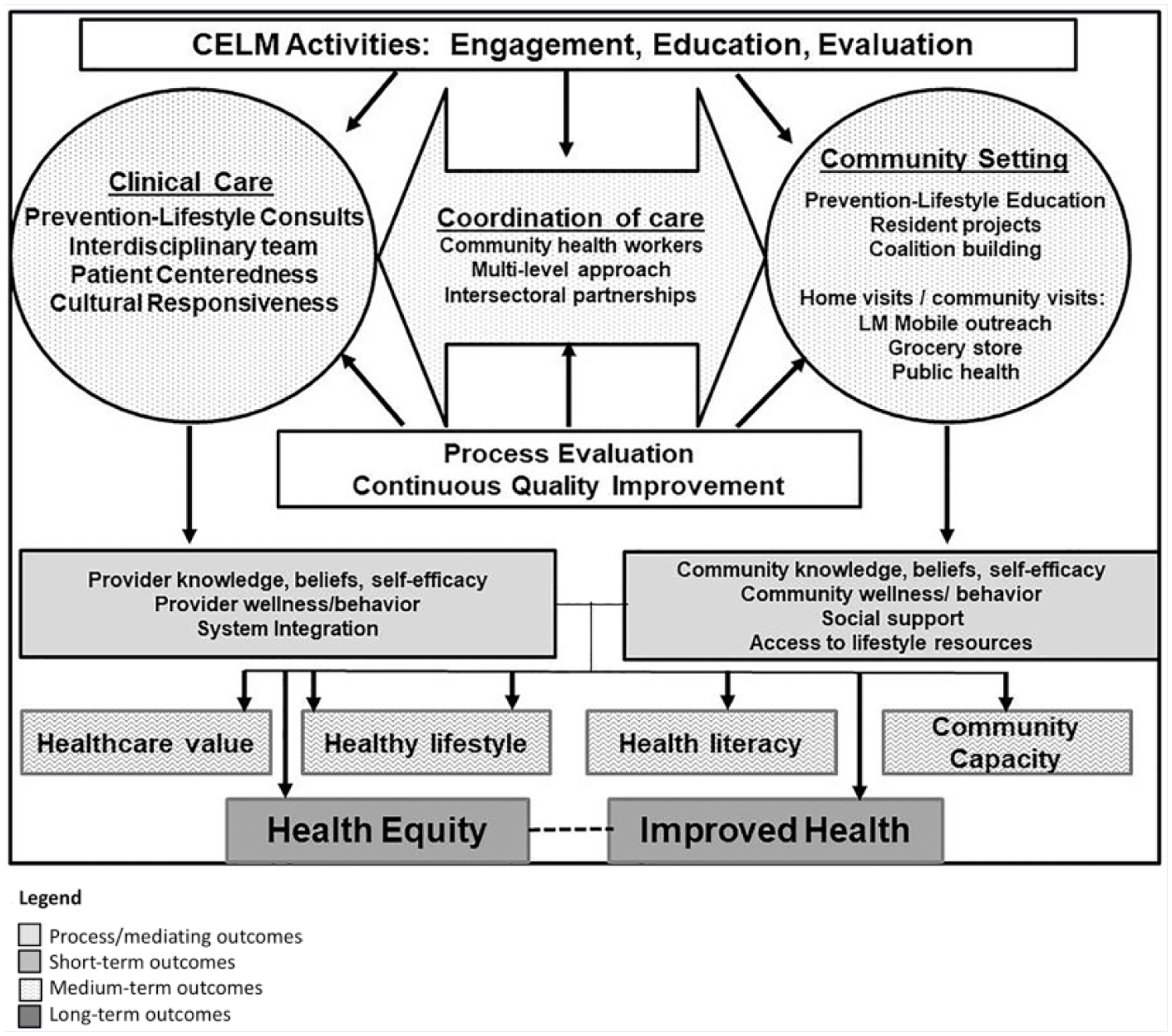
Logic model for CELMa (reprinted with permission from the author).
CELM Efforts Within the American College of Lifestyle Medicine
When a small group of ACLM members were approached in 2017 with the idea of starting a new committee focused on bringing lifestyle medicine to the underserved, the response was overwhelmingly supportive. The leadership and expertise of the initial members along with the enthusiasm of new members has helped this committee grow. The CELM committee is dedicated to highlighting the extraordinary work that many ACLM members are already doing within underserved populations, providing a space to learn from each other’s challenges and triumphs and holding educational workshops to provide ACLM members with the evidence-based tools necessary to enterprise lifestyle medicine–rooted initiatives within those disadvantaged communities.
This young committee was invited to hold a workshop focusing on CELM for the 2018 ACLM national conference. A portion of the workshop focused on highlighting innovative speakers who were implementing successful CELM-based work both across the country and internationally. An important goal of the workshop was to provide those who attended with a practical step-by-step framework as presented by the Centers for Disease Control, which they could use to guide their very own CELM-focused projects. Session attendees were also given the opportunity to ask questions and collaborate with each other during small group sessions while the expert speakers served as a resource to answer questions and share constructive advice. CELM activities presented by the committee during the inaugural workshop are summarized in Table 2.
CELM Inaugural Workshop at American College of Lifestyle Medicine 2018: Presenters and Activities.
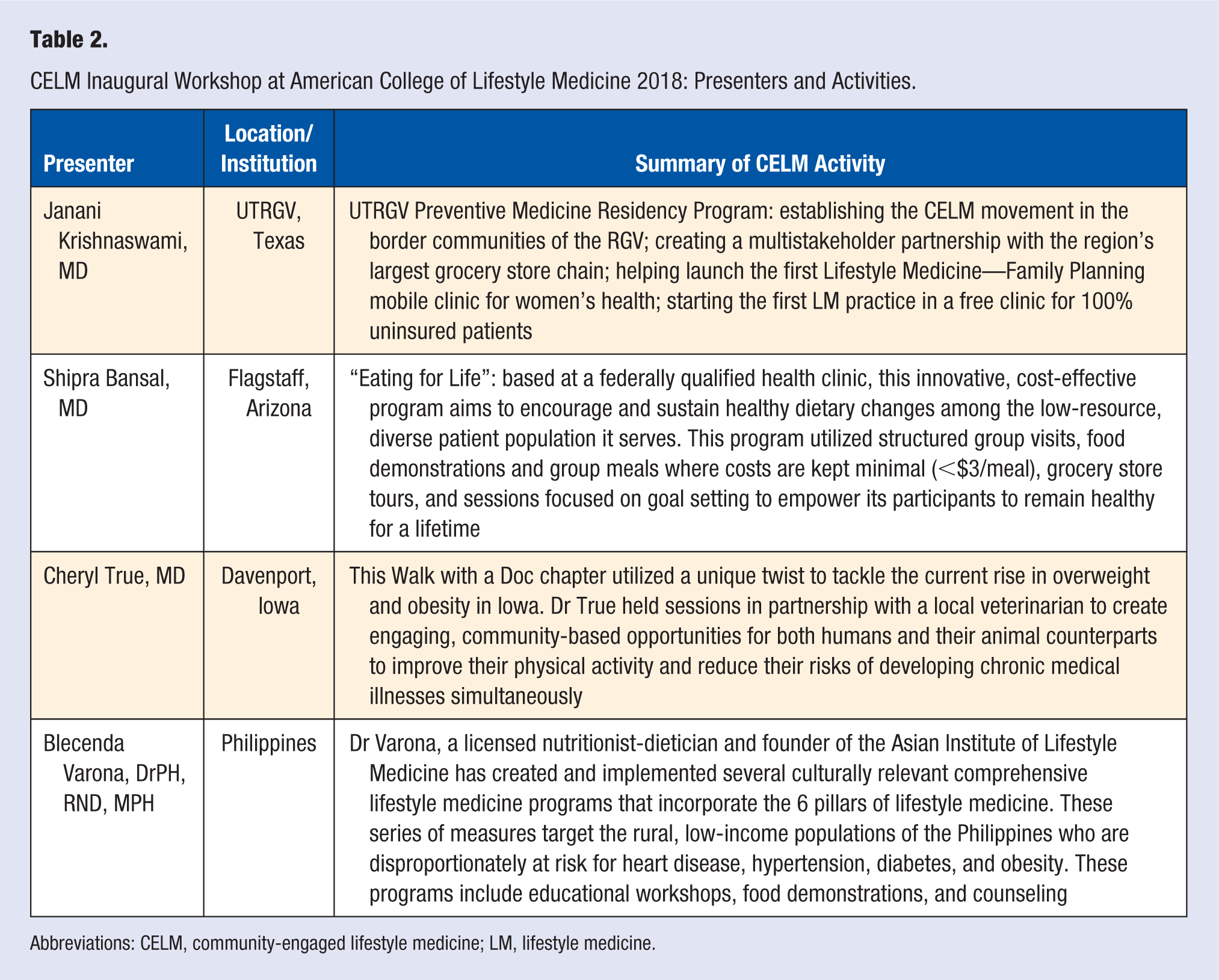
Abbreviations: CELM, community-engaged lifestyle medicine; LM, lifestyle medicine.
Prescriptions for Lifestyle Medicine Practitioners: What to Do Today
Although originally developed as a health equity framework for the border communities of the Rio Grande Valley in Texas, CELM can be translated by clinical providers around the world for the betterment and welfare of diverse, vulnerable, and unhealthy communities. Examples of how to build CELM into existing practices in the short- and long-term levels are presented in Table 3.
CELM Prescriptions for Lifestyle Medicine Practitioners Based on Short-, Medium-, and Long-Term Outcomes.
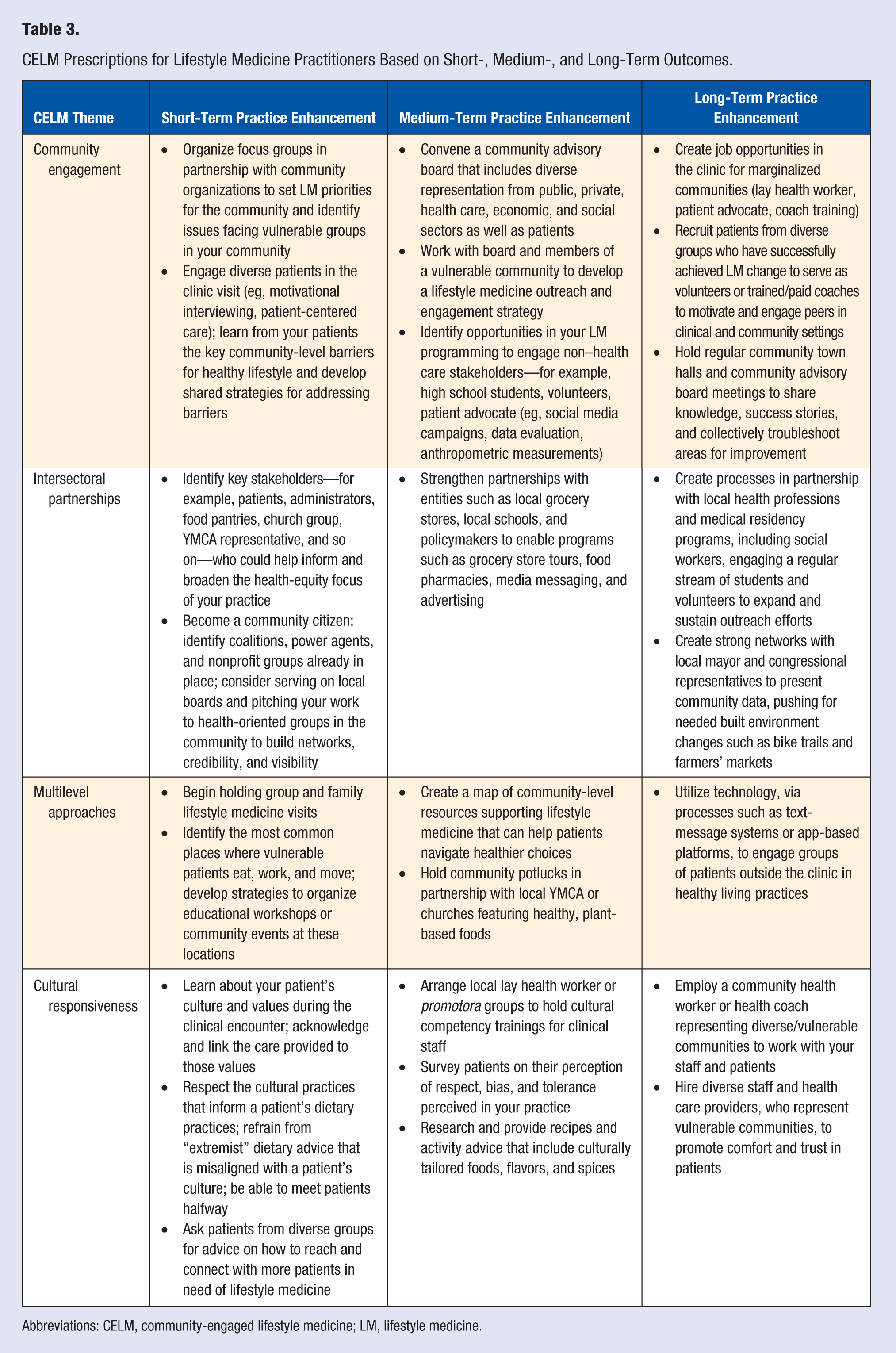
Abbreviations: CELM, community-engaged lifestyle medicine; LM, lifestyle medicine.
In line with CE principles, achieving outcomes of health equity must ultimately extend beyond a single clinic’s efforts. Sustainable partnerships boosting capacity of lifestyle medicine practitioners and community-based organizations at the national, regional, and local levels are needed, engaging stakeholders to address upstream causes of poverty and increasing grassroots community momentum and ownership of health-building programs. Nevertheless, systemic transformation can begin via innovation at the ground level: translating theoretically effective CELM mechanisms to build equitable and efficacious pathways for health.
Footnotes
Authors’ Note
This article is based on a workshop given at the Annual Meeting of the American College of Lifestyle Medicine 2018 in Indiana, IN. Janani Krishnaswami, MD, MPH, lead author of “Community Engaged Lifestyle Medicine: Building Health Equity Through Preventive Medicine Residency Training,” gives permission for the publication of ![]() , originally published in the American Journal of Preventive Medicine (2018). Janani Krishnaswami is currently affiliated with UWorld LLC, Irving TX.
, originally published in the American Journal of Preventive Medicine (2018). Janani Krishnaswami is currently affiliated with UWorld LLC, Irving TX.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.