
Abstract
‘Although the etiology of this syndrome is still not well recognized, it seems that a series of genetic, metabolic, and environmental factors, such as diet, play an important role in its incidence.’
Introduction
Metabolic syndrome (MetS) is a cluster of disorders that includes central obesity, dyslipidemia, hypertension, and glucose intolerance. This syndrome increases the risk of cardiovascular diseases and diabetes. 1 The present evidence shows that the prevalence of MetS among adults, in the majority of countries, is from 20% to 30%. 2 Although the etiology of this syndrome is still not well recognized, it seems that a series of genetic, metabolic, and environmental factors, such as diet, play an important role in its incidence.3,4 Diet is considered as a key factor in the prevention and treatment of MetS.5,6
It has been shown that diets with high saturated and trans fatty acids, cholesterol, salt, processed red meat, fried foods, refined grains, and simple carbohydrates are substantial contributors to pathogenesis of MetS. In contrast, diets rich in fruits and vegetables, whole grains, and fiber can be useful in the prevention of this disease.7-9 However, adoption of these healthy behaviors can be affected by health education and behavioral change programs, so many studies have proposed the application of theories and behavioral change models for designation of any nutrition education intervention. 10
One of the most successful theories used to evaluate behavioral change is the theory of reasoned action (TRA), designed by Ajzen and Fishbein. According to this theory, intention is considered as the first and the strongest component of behavior, which is predicted by attitude and subjective norm. 11 Attitude is a positive or negative evaluation about doing a behavior, which is made up of behavioral beliefs and evaluation of behavior outcomes. Subjective norms or social pressure are impressed on the individual by other people, including father, mother, spouse, and religious leaders, and is made up of normative beliefs and motivation-to-comply variables. 12
The TRA is the most commonly used theory in food choice behavior. 13 Recent studies have evaluated the application of this theory in nutrition-related behavior.14-16 Knowing that MetS is the key pathological condition involved in the development of many metabolic, cardiovascular, and endocrine disorders and keeping in mind the positive role of healthy nutritional behaviors in the clinical management of these diseases, we aimed to identify factors affecting behavioral intentions and nutritional behaviors of MetS patients based on the TRA.
Methods
This cross-sectional study was done on 322 individuals suffering from MetS, diagnosed according to the International Diabetes Federation (IDF) criteria. 17 The patients were selected using a convenience sampling method from individuals attending to outpatient departments in Mahabad district hospital in northwestern Iran, from April to June 2013. The sample size was achieved using a level of significance of 95%, error 5%, and prevalence of MetS of 30%. Inclusion criteria were as follows: ages between 20 and 50 years and diagnosis of MetS based on the IDF criteria that included having a waist circumference ≥94 cm for men and ≥80 cm for women in addition to having at least 2 of the following characteristics: fasting blood glucose ≥100 mg/dL or previously diagnosed type 2 diabetes; systolic blood pressure ≥130 mm Hg and diastolic blood pressure ≥85 mm Hg or treatment for previously diagnosed hypertension; triglyceride ≥150 mg/dL or specific treatment for this lipid abnormality; high-density lipoprotein cholesterol <40 mg/dL for men and <50 mg/dL for women or specific treatment for this lipid abnormality. Exclusion criteria were mental illness, cancer, stroke, pregnancy, and lactation.
The instrument used for data gathering was a questionnaire that included demographic information and basic information of MetS components. This questionnaire was constructed by text reviews and focus group discussions with people who were suffering from MetS. The content validity of the tool was approved by personal interviews with 15 experts of nutrition and health education professionals. The final confirmed questions of the questionnaires included the demographic and basic information of MetS components (16 questions), nutritional attitude (17 questions), subjective norms (13 questions), and nutritional behavior (15 questions). The questions of nutritional attitude, subjective norm, and behavioral intention were evaluated by a Likert scale that ranged from “strongly disagree” to “strongly agree”; also, questions of nutritional behavior ranged from “never” to “always.” 18 The participants who were eligible to be included in the study were asked to sign an informed consent. All participants had the right to withdraw from the study at any time; confidentiality of the participants was respected, and ethical considerations were taken into account. An expert dietician helped the participants fill out the questionnaire.
Data Analysis
The data were analyzed using SPSS 19 software (SPSS Inc, Chicago, IL). Data are presented as mean (SD) for quantitative variables and frequency (percentage) for qualitative variables. The normality of data was assessed and confirmed by the 1-sample K-S test. The independent t-test was used to compare the means of different variables between groups. A univariate-multivariate hierarchical strategy was applied to investigate the relationship between behavioral intentions as the dependent variable and baseline characteristics as well with other components of TRA. In the univariate analysis, each variable was entered in the regression model individually to assess its relationship with the dependent variable. In the multivariate analysis, a 2-step hierarchical strategy was used, wherein in the first step, the significant baseline variables in the univariate analysis were entered into the model. Second, the main TRA variables—nutritional attitude and subjective norms—were entered. Also, the demographic variables, including level of education and gender of the patients, which became significant, remained in the model.
Another univariate-multivariate hierarchical multiple linear regression model was proposed for nutritional behavior as the dependent variable. In the first model of nutritional behavior, the variables age, gender, and level of education that became significant in the univariate analysis remained in the model. In the next step, significant sociodemographic variables with nutritional attitude, subjective norm, and behavioral intention entered into the regression model. The regression assumptions of residual normality, homogeneity of residual variances, residual independence, and colinearity were assessed and confirmed using a normal probability plot, the residual versus predicted values plot, Durbin-Watson Statistics (values between 1.5 and 2.5 as the acceptable range), and variance inflation factor (<5 as the acceptable values).
Results
As presented in Table 1, the study population was composed of equal number of men and women (n = 161, each) with a mean age of 40.55 ± 5.97 years. Of the participants, 78.6% had children, and 82.3% were residing in urban areas. The education level of 45.3% of the participants was below high school level, 39.2% had completed high school education, and 15.5% had college education or higher. Also, 9% of the participants (mostly men) were smokers.
Demographic Characteristics and Drug Therapy in the Study Population.
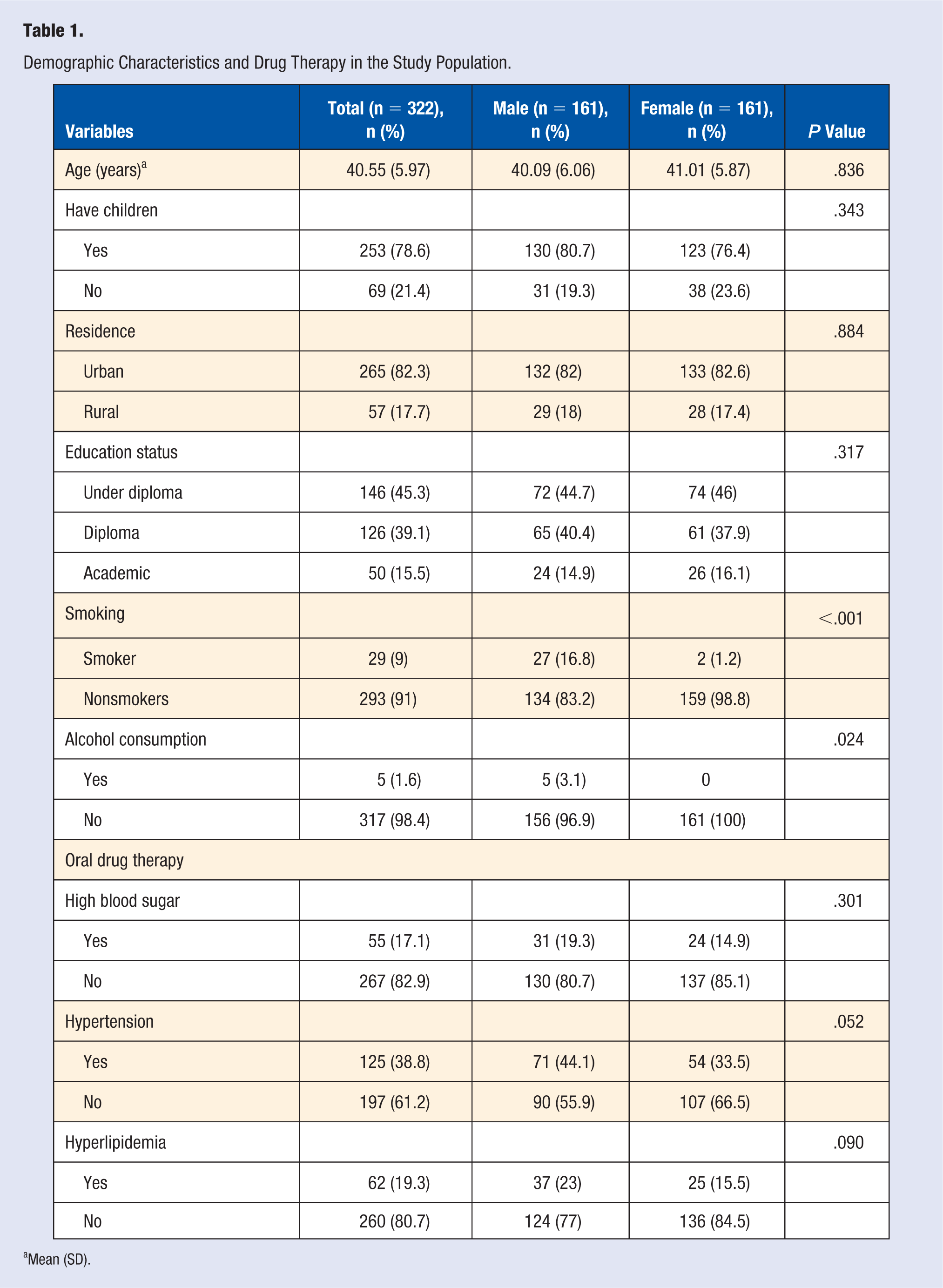
Mean (SD).
As shown in Table 2, average of behavioral intention was significantly higher in women versus men (P = .002), in nonsmokers versus smokers (P = .029), and in people with educational qualifications of higher than school diploma versus diploma and diploma versus lower than school diploma (P < .001). Also, the average of nutritional behavior was significantly higher in women versus men (P < .001), in urban versus rural people (P = .048), and in people with educational qualifications of higher than school diploma versus diploma and diploma versus lower than school diploma (P < .001).
Behavioral Intention and Nutritional Behavior Based on Sociodemographic Characteristics of Study Participants.
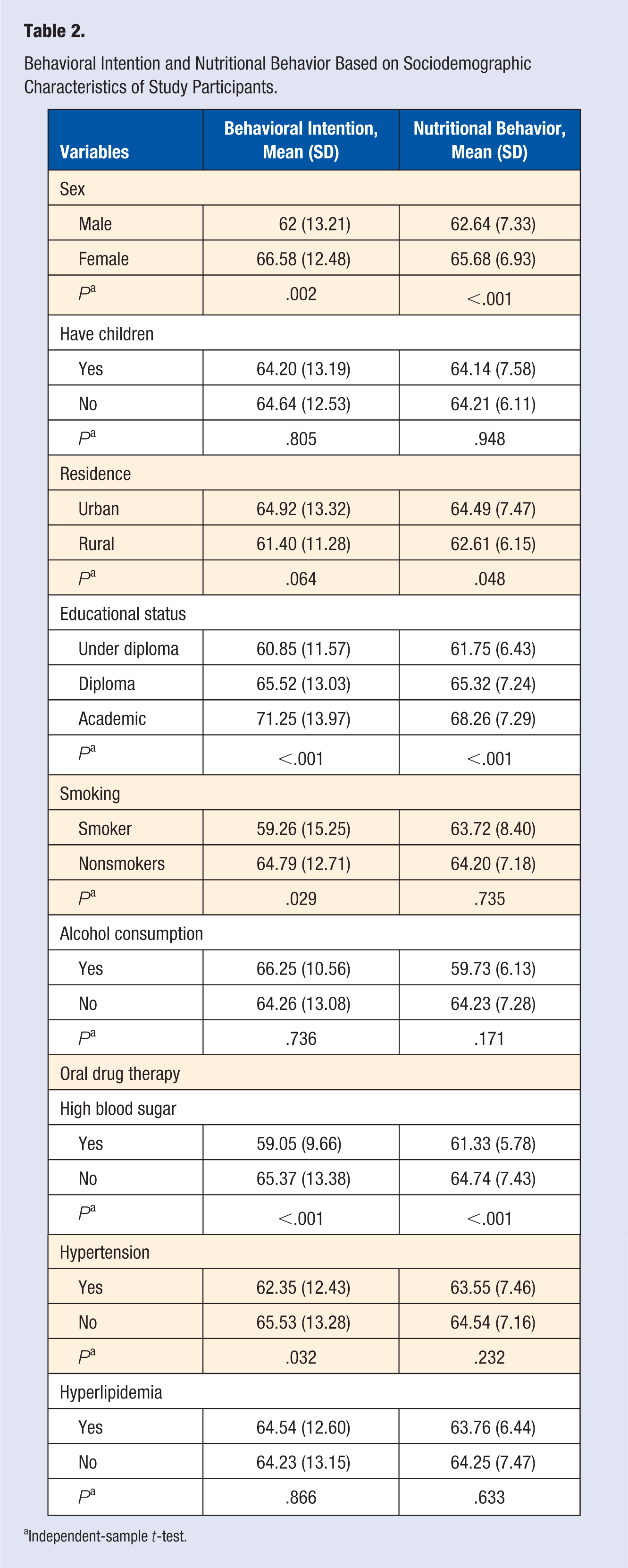
Independent-sample t-test.
Table 3 shows correlations between TRA components. There was a significantly positive relationship between behavioral intention with nutritional attitude (P < .001; r = 0.543) and nutritional behavior with behavioral intention (P < .001; r = 0.619). Also, there was a moderate correlation between nutritional behavior and nutritional attitude (P < .001; r = 0.463). Finally, variables of subjective norm had significant but weak correlations with behavioral intention (P < .001; r = 0.240) and nutritional behavior (P < .001; r = 0.235).
Correlation Matrix for Theory of Reasoned Action Variables. a
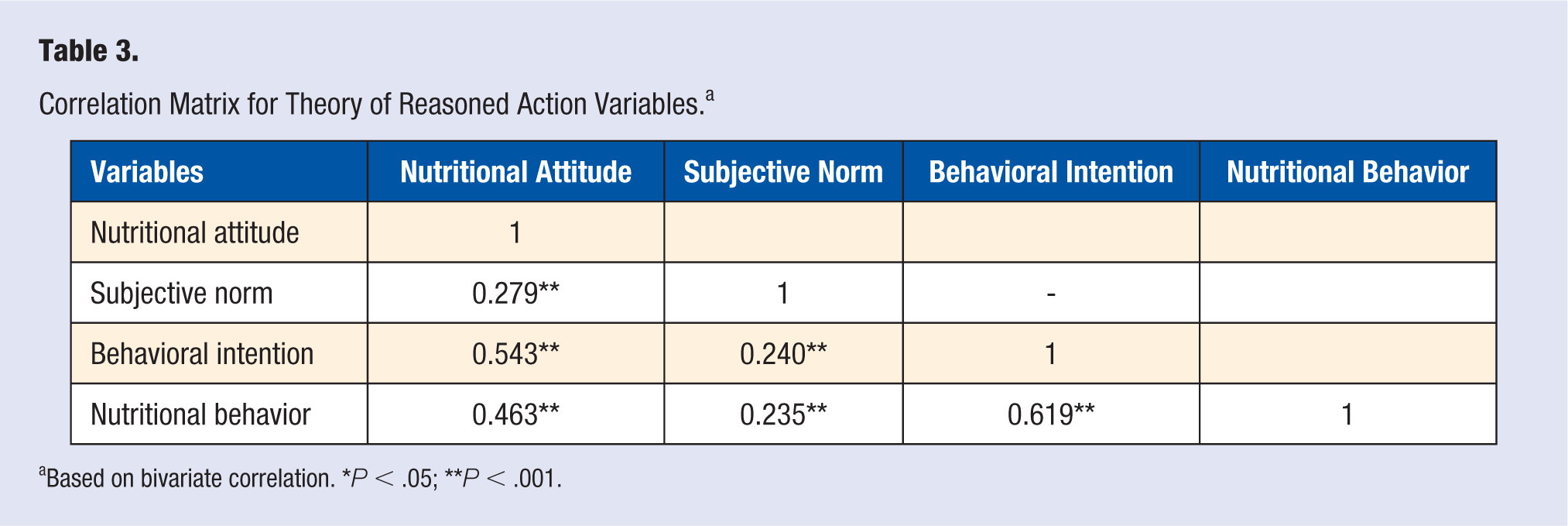
Based on bivariate correlation. *P < .05; **P < .001.
Hierarchical regression of behavioral intention on predictors yielded a final model where gender (β = 0.118; P = .015) and nutritional attitude (β = 0.471; P < .0001) were the significant determinants. Subjective norm was near significance (β = 0.090; P = .068). This final model could predict 32.5% of the variance in behavioral intention. Education level did not reach significance (Table 4).
Multiple Regression Analysis on Behavioral Intention of Study Participants (n = 322). a
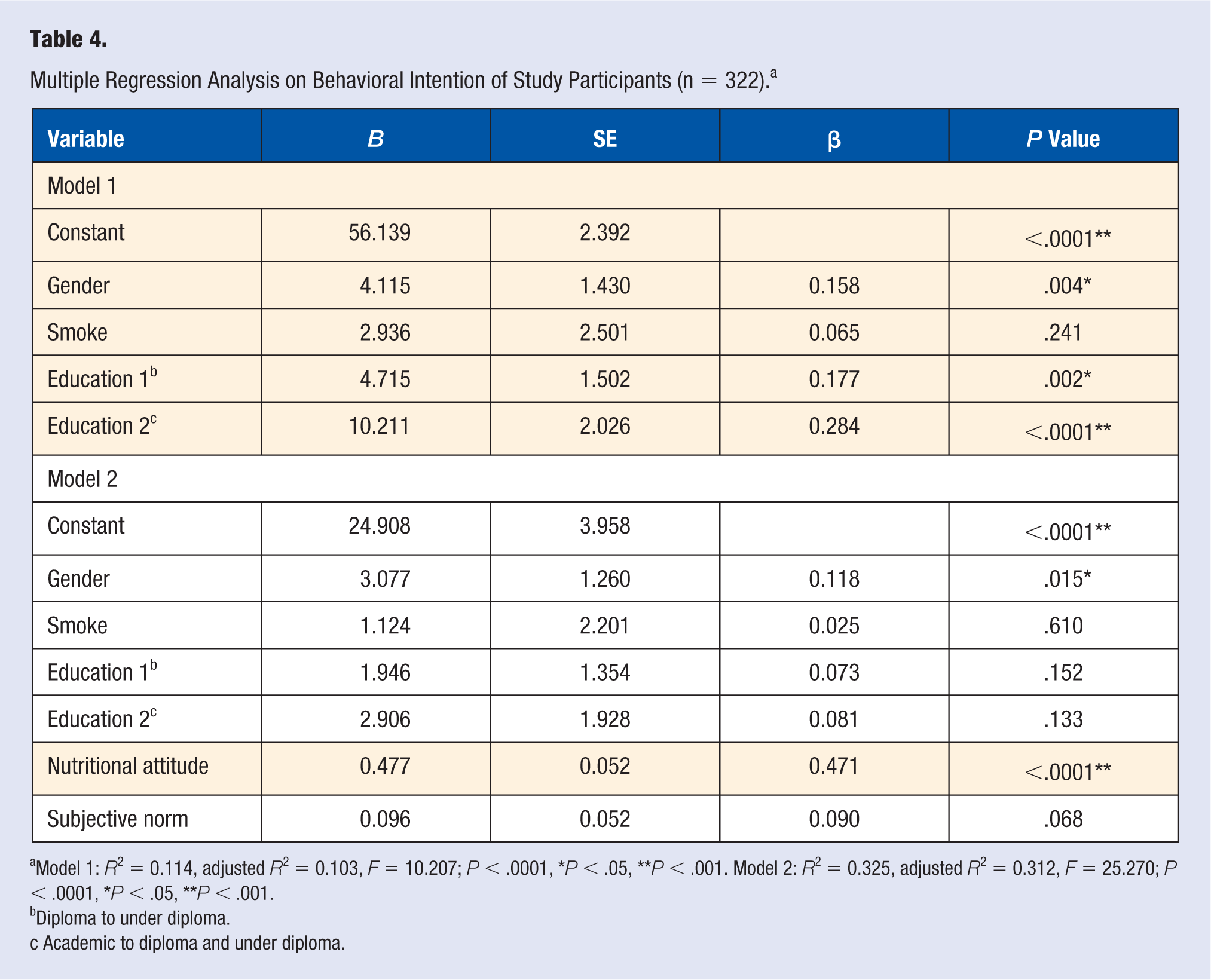
Model 1: R2 = 0.114, adjusted R2 = 0.103, F = 10.207; P < .0001, *P < .05, **P < .001. Model 2: R2 = 0.325, adjusted R2 = 0.312, F = 25.270; P < .0001, *P < .05, **P < .001.
Diploma to under diploma.
Academic to diploma and under diploma.
In the multiple regression analysis on nutritional behavior, predicting effect of age, gender, level of education, nutritional attitude, and behavioral intention on the nutritional behavior was confirmed (P < .05), and this model could predict and explain 44.7% of nutritional behavior variance (Table 5).
Multiple Regression Analysis for Nutritional Behavior. a
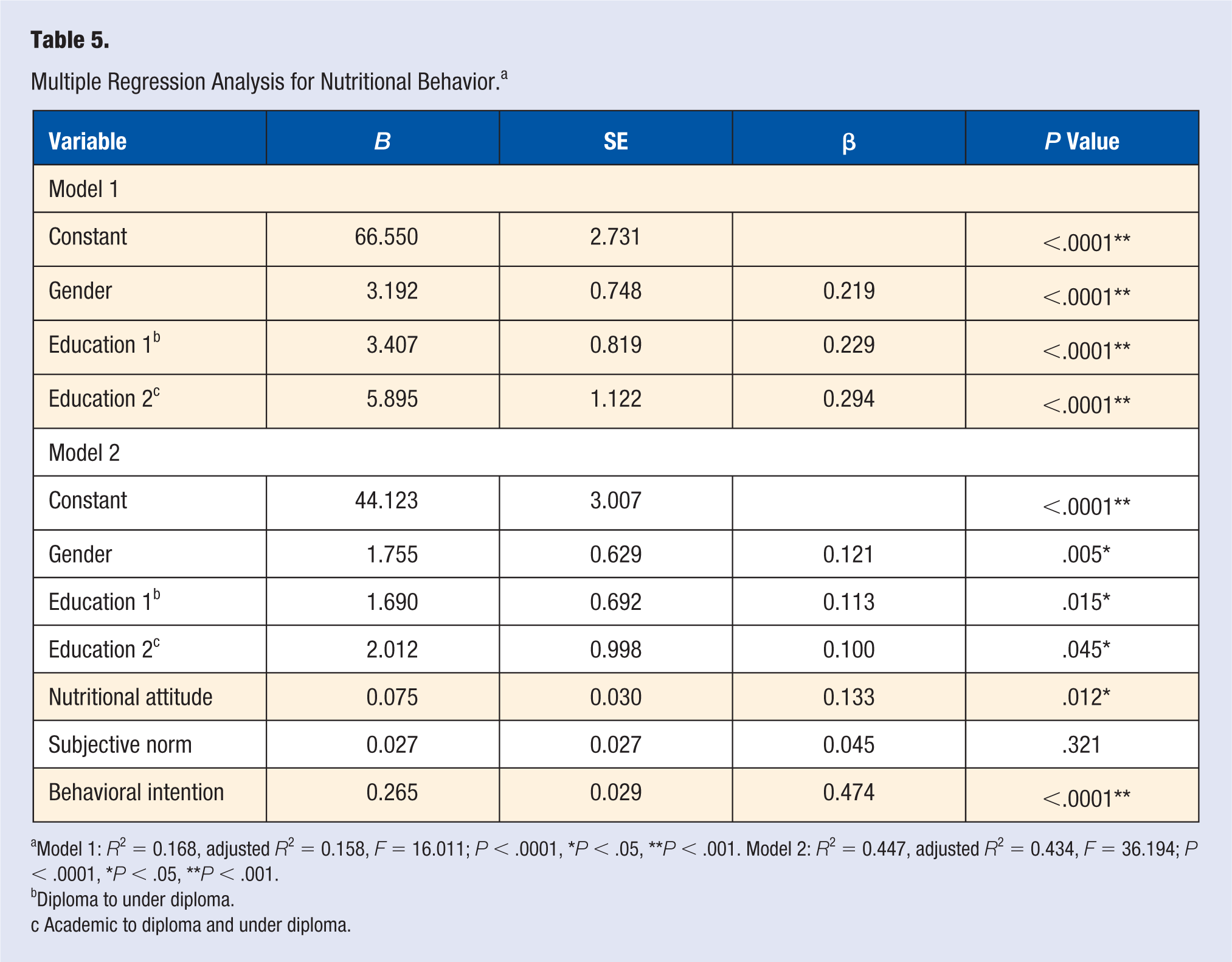
Model 1: R2 = 0.168, adjusted R2 = 0.158, F = 16.011; P < .0001, *P < .05, **P < .001. Model 2: R2 = 0.447, adjusted R2 = 0.434, F = 36.194; P < .0001, *P < .05, **P < .001.
Diploma to under diploma.
Academic to diploma and under diploma.
Discussion
The objective of this study was to identify the determinants of behavioral intention and nutritional behavior of the individuals suffering from MetS based on the TRA. The findings highlighted that nutritional attitude efficiently predicts behavioral intention, followed by gender, as a sociodemographic variable. Also, behavioral intention is the strongest predictor of nutritional behavior, followed by nutritional attitude, gender, and educational levels of participants.
The increasing trend in the prevalence of MetS is one of the most challenging global epidemic concerns. Management of this syndrome, which is a collection of cardiovascular disease and type 2 diabetes risk factors, including high blood pressure, blood lipid abnormalities, abdominal obesity, and increased blood glucose, requires in-depth identification of factors affecting behavioral intention and nutritional behavior of the patients. Thus, characterization of predictors involved in the pathogenesis of MetS is important for adoption of healthy lifestyles, such as physical activity and diets, which are substantial contributors in preventing and treating this syndrome.19,20
Exploring nutritional attitude of MetS patients revealed a positive and strong relationship between nutritional attitude of the patients and their behavioral intention. The findings are in good accordance with a report by Kassem and Lee 20 who found that attitude is the strongest predictor of intention to drink regular soda. 21 Moreover, intention to eat breakfast by adolescents 22 and consumption of sports supplements was predicted by attitude. 14 In another study, no correlation was determined between attitude and intention in consumption of sugar-free products. 13 The findings indicate that enhancing nutritional attitude by nutritional education could affect behavioral intention to choose a healthy diet. Assuming that intention leads to behavior, it could be declared that enhancement of an individual’s attitude indirectly leads to health promotion.
There was also a positive and significant relationship between nutritional attitude and nutritional behavior. Previous studies have also shown similar results.11,23-25 Thus, it could be concluded that in addition to the indirect relationship of attitude with behavior via behavioral intention, there is a direct relationship between attitude and nutritional behavior.
Subjective norm is another component of TRA. It was believed that identification of this variable may be helpful in predicting intention and nutritional behavior. In our study, there were no significant predicting effects between subjective norms of study participants and intention or behavior. One study showed that the subjective norms of the participants had less effect on behavior and attitude. 26 Moreover, eating dairy products was not influenced by subjective norms in another study. 27 Whereas Bartee et al 13 reported that using sports supplements in adults was predicted by subjective norms, it is speculated that this contradiction could be attributed to different behaviors considered by studies and also the variation of cultural, social, and personal characteristics of the individuals. The previous studies showed that the subjective norm has often a weaker power of prediction compared with the other components of TRA and planned behavior theory.21,22
The correlation observed between behavioral intention and nutritional behavior may imply that the more the intention of an individual toward engaging in a behavior, the more will be the performance. Accordingly, previous studies have suggested that intention was a significant determinant of fruit and vegetable consumption,28-34 drinking regular soda, 21 or adolescent breakfast consumption. 22 Other studies found a nonsignificant or weaker effect of intention in performing a behavior.23,31,32,35 This phenomenon could be explained by the fact that frequent performance may lead to a strong habit with a minor consideration of intention.
In addition to the main components of TRA, strong relationships between sociodemographic variables, including gender, smoking, and level of education, with intention and nutritional behavior were also identified. Therefore, these variables were put in the proposed model of predicting behavioral intention and behavior. It was also determined that gender is one of the factors that can indirectly affect behavior via behavioral intentions. The findings were in agreement with the results of Shepherd and Towler. 22 In other studies, women had more positive attitudes and behavior in terms of “healthy eating”36,37 and higher preference for eating low-fat milk products. 38 It seems that women have more interest in healthy nutritional behavior compared with men.
Education level was another demographic factor that had a positive and significant relationship with nutritional behavior. This factor indicated that a higher level of education in patients leads to improved nutritional behavior, which is in accordance with the Mazloomi et al 15 study. The results of this part of the study may reflect the fact that enhancing education level in society could promote healthy behaviors, including nutritional behaviors, which subsequently improve the health status of the society.
Limitations
The main limitation of this study is that our findings are not easily generalizable to MetS patients in other nations because of the diversity in sociodemographic variables. Thus, future research should include diverse populations to identify factors affecting nutritional behavior among these patients.
Conclusions
It is concluded that attitude and intention, but not subjective norms, along with some sociodemographic variables, including gender and educational levels, were able to predict the nutritional behavior of MetS patients. These findings could be used to design effective interventions and programs about nutritional education for health improvement of MetS patients, which could decrease the subsequent side effects of this syndrome, prevent related diseases, and finally promote health aspects in society.
Footnotes
Acknowledgements
We appreciate the patients and all the people who helped us during this study.
Authors’ Note
MA and NE were involved in the conception and design of the study. ATE performed the data analysis and interpretation. MA wrote the manuscript and acted as corresponding author. EF and SK supervised the development of the work and helped in data interpretation and manuscript evaluation. EF helped evaluate and edit the manuscript. The study was ethically approved by an authorized ethics committee at Tabriz University of Medical Sciences, Tabriz, Iran (Reference no. 5/4/3189). Data for the current study were gathered from the clinics in the main general hospital in the Mahabad district in northwestern Iran from April to June 2013.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The article is the result of the sponsorship of Nutrition Research Center of Tabriz University of Medical Sciences, Tabriz, Iran.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.