
Abstract
Research demonstrates lower school participation in children with sensory disorders. However, the scientific body of evidence supporting existing sensory intervention modalities is difficult to tackle. More specifically, the literature appears poorly organized, with a highly variable terminology, often with nonoverlapping definitions and lack of good keywords classification that would help organize the diversity of approaches. This systematic review organizes the body of evidence for 3 specific approaches (sensory based, sensorimotor, and sensory integration) and questions their efficacy in improving school participation for children with sensory disorders. Two methods were compared: first, a standard systematic review of the literature in 3 databases using appropriate keywords and descriptors, then an original method based on forward and backward citation connections. A total of 28 studies were retrieved, of which only 7 used the standard method for systematic reviews. For sensory-based approaches, the efficacy of weighted-vest varies according to different factors such as the protocol of use. For sensorimotor approaches, the efficacy of therapy balls, air cushions, platform swing, and physical exercise varies according to the child’s sensory characteristics. The efficacy of the sensory integration approach remains mixed across studies.
Keywords
‘It has been shown that children with difficulties in the treatment and integration of sensory information demonstrate lower participation in school activities.’
Introduction
Difficulties in the treatment and integration of sensory information are common for many children with a neurodevelopmental diagnosis, such as autism spectrum disorder (ASD), coordination acquisition disorder and attention-deficit/hyperactivity disorder (ADHD). 1 According to Tomchek and Dunn, 2 90% of children with ASD have hyporeactivity or sensory-seeking behaviors, and 67% have tactile hypersensitivity behaviors. It is also demonstrated that sensory disorders are more often diagnosed for children with ADHD and coordination acquisition disorder in comparison with neurotypical children. 3 However, according to Ben-Sasson et al 4 who affirm that 16.5% of children between 7 and 11 years old have an elevated response to auditory and tactile sensory stimuli, sensory disorders could also be a concern for children without disabilities.
Sensory difficulties are often formally identified in the early school years because these children demonstrate organizational problems in the classroom or delays in the acquisition of fine and global motor skills.1,5,6 An elevated response to sensory stimuli can also be observed at this time because of the increasing demands and stimulation of the learning context combined with the limited control the child has in this particular environment 7 (as quoted in Ben-Sasson et al 4 ). It has been shown that children with difficulties in the treatment and integration of sensory information demonstrate lower participation in school activities. 8 Such children can develop lowered interest in academic activities or even consider school as a place of repetitive failure and develop avoidance, 9 which can compromise their academic success and future socioprofessional integration.
The therapeutic modalities targeting sensory disorders are very diverse and based on different approaches. 10 One of the most common is the sensory integration approach. Its rationale is to remediate sensory disorders by improving the neurological processes that are responsible for the processing, integration, and response to sensory stimuli. 11 It is a traditional approach that has been criticized a lot because it is expensive, intensive, and difficult to integrate into family routines. 12 Other contemporary intervention approaches exist, such as sensory-based and sensorimotor approaches. They focus on adaptation and self-regulation to improve children’s participation. 12 Case-Smith et al 10 explain that the literature regarding all the approaches targeting sensory disorders appears poorly organized, with numerous traditions for naming, often with nonoverlapping definitions and lack of good keywords classification. This situation limits the capacity of practitioners to choose the best practice for sensory disorders and contributes to confuse parents about what they need to prioritize with their children. 10
Because of the high prevalence of sensory disorders in children and their important impact on academic success, it is crucial that practitioners base their clinical reasoning on the best evidence available. Therefore, this systematic review aims at organizing the body of evidence for the 3 specific approaches (sensory-based, sensorimotor, and sensory integration) and examining their efficacy on school participation of children with sensory disorders.
Method
Research Strategies
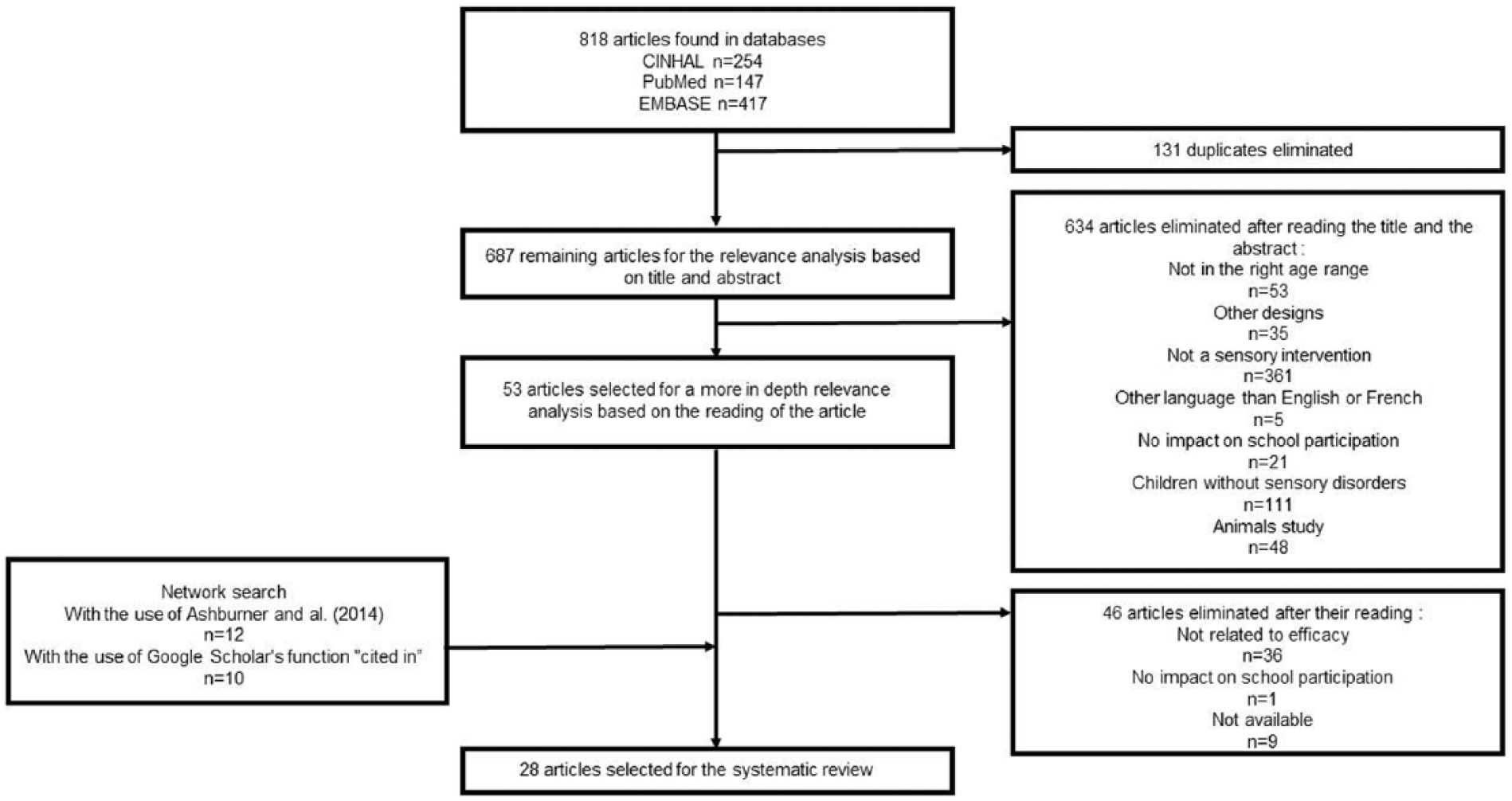
First, a standard database search was performed following PRISMA guidelines from October to December 2016 using 3 databases (PubMed, CINHAL, and EMBASE) and an exhaustive list of keywords and descriptors about children, sensory disorders, school participation, and the 3 sensory approaches used (see Supplemental Tables ST1 and ST2). After the duplicates were eliminated, 687 articles remained and were analyzed with the inclusion and exclusion criteria to determine if they were relevant for this study. The inclusion criteria were the following: (1) the intervention belongs to either sensory integration or sensorimotor or sensory-based approaches (for operational definitions, see the appendix); includes children (2) between 4 and 17 years of age and (3) with sensory disorders; (4) dependent variables should include school participation; (5) the study is experimental or quasi-experimental; and (6) written in French or English. The exclusion criteria were (1) the study could not be accessed neither through the scientific library of Laval University nor by contacting the authors to get them; (2) the modality was not used following the paradigm of 1 of the 3 approaches; (3) results regarding children between 4 and 17 years old could not be separated from that of older or younger children. The selection process was performed by 2 independent evaluators. In the absence of consensus, a third evaluator was used. At the end of the selection process, 28 articles fulfilled the criteria.
This standard strategy resulted in an unsatisfactory grand total of 7 articles. As already noticed by Case-Smith et al, 10 this problem seems to be caused by the subject’s lack of standard keywords that would help finding the relevant articles. We then completed the research using a manual search strategy based on citation links. For this strategy, we started with the clinical reasoning framework of Ashburner et al 12 because it addresses all the sensory approaches studied in this systematic review. We read the title and abstract of each reference cited in their article to find studies responding to the aim of our systematic review. A more thorough reading was performed to eliminate the studies that did not respect our inclusion criteria or that corresponded to our exclusion criteria (same as above). Then, the bibliography of each new study selected was consulted to find other articles. This process of search in the bibliographies was conducted twice (until no new relevant articles were found). Second, the Google Scholar’s “cited in” function was used for each study previously selected to verify that all the studies relevant to the search question had been found. After this process, data saturation was reached because studies found did not contribute new results regarding the 3 sensory intervention approaches. Overall, this research strategy not only retrieved all articles found using the standard approach, but also significantly increased the number of studies included in this systematic review (Figure 1 and Supplemental Figures SF1 and SF2).
Flow diagram
Dependent Measures
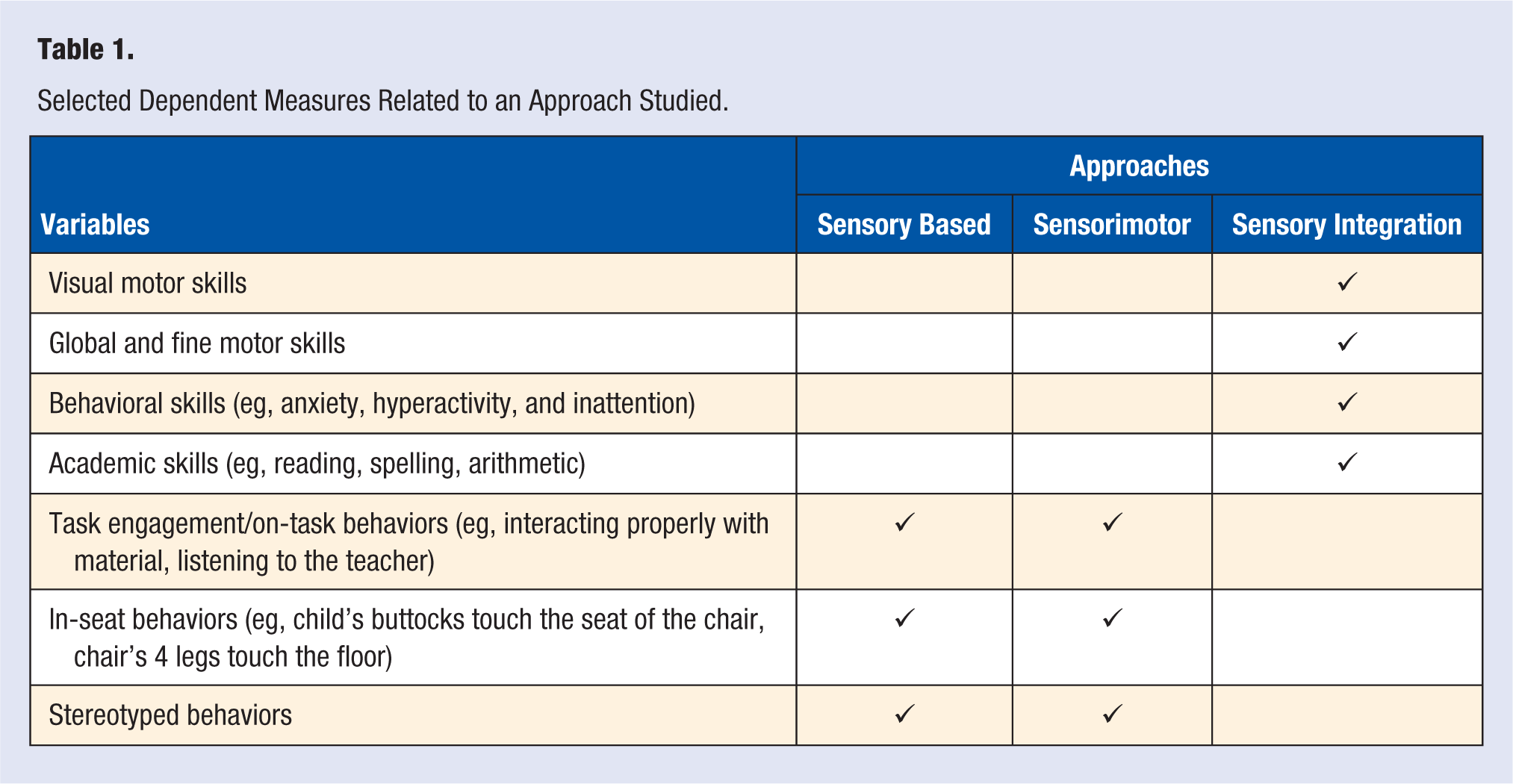
This systematic review included many dependent variables because the authors used many of them to measure the impact of sensory interventions on children’s school participation. Some variables were common to all 3 approaches, whereas others were specific to one (see Table 1). The criteria to select a variable was that it had an impact on school participation. Therefore, skills and behaviors hindering school tasks, disturbing other students, or discouraging the child to engage in school activities were included.
Selected Dependent Measures Related to an Approach Studied.
Data Extraction and Analysis
First, the scientific quality of each included study was determined. Two scientific quality assessment tools were used. The French version of the Letts et al 13 critical review form for quantitative studies, which is a multidesign assessment tool, was used to rate the quasi-experimental studies. Also, the French-Canadian version of the PEDro Scale was used to assess the experimental studies. 14 To rate the quality with these 2 tools, 1 point was given when the study met the criterion. However, some criteria were sometimes rated nonapplicable, such as the one for contamination between groups, because the majority of single-case studies did not have a control group. 13 The sum of the points was calculated and then converted to a percentage. A 4-level quality classification scale was developed to compare the studies (0%-30% = very low quality; 31%-60% = low quality; 61%-80% = moderate quality; 81%-100% = high quality). The quality of each study was assessed by 2 authors. In case of disagreement, a third person was asked to determine the rating of the criterion.
Then, the data relevant to the assessment of efficacy of the 3 approaches were determined by 2 authors using the same process as for the scientific quality assessment. The studies were classified according to their level of scientific quality, from the highest to the lowest (see Supplemental Tables ST3-ST5).
Finally, a combined analysis of the scientific quality and of the data relevant to the assessment of school participation followed by a discussion were conducted by 4 authors (VD, BO, AR, ET) to identify the trends and produce conclusions on the efficacy of sensory modalities. Then, after another discussion, these authors established recommendations for the therapist regarding the use of these modalities in a school context.
Results
As illustrated in Figure 1, the combined searching strategies, carried out from December 2016 to July 2017, resulted in 28 relevant articles. Most of the (n = 22; 78%) studies included were related to sensory-based (n = 9; 32%) and sensorimotor approaches (n = 13; 46%), whereas a few concerned the sensory integration approach (n = 6; 21%). Scientific quality varied between low to high. In the following section, we present the data and analysis for each of the 3 approaches according to the dependent measures and children’s diagnoses.
Sensory-Based Approaches
All the 9 studies related to sensory-based approaches had quasi-experimental designs. All used weighted vest as a sensory intervention modality. The protocol of use of this modality differed between studies, but the vest’s weight, if mentioned, was always between 5% and 15% of the child’s body weight. The majority of the studies (9/11) had a small sample that did not exceed 11 participants, except for 2 studies,15,16 for which samples were of 30 and 110 participants. Most of the time, variables were measured by direct or indirect observations conducted by 1 or 2 observers at a specific time interval (the sequence duration of observation of the child’s behaviors). The scientific quality varied between high (2) moderate (n = 6) to low (n = 3). Most of the studies measured the efficacy of this approach using task engagement/on-task behaviors, in-seat behaviors, and stereotyped behaviors. Results for each dependent measure and submeasure are presented below according to the diagnosis for the children.
Task Engagement/On-Task Behaviors
For children with ASD and developmental delays, one study explained that wearing a weighted vest did not affect their task engagement behavior. 17 Moreover, for children with ASD, 2 studies demonstrated that the difference between the conditions (no vest, weighted-vest, pressure vest, or unweighted vest) was not significant for the attention-to-task behavior.18,19 The scientific quality of all these studies was judged as moderate. For children with ADHD, 3 low-to-moderate quality studies demonstrated a significant improvement in attention to task when wearing the weighted-vest,15,16,20 whereas one moderate-quality study did not show a significant difference between the group of children who wore the weighted vest and the unweighted vest as well as the no-vest group. 21
In-Seat Behaviors
For children with ASD, one study showed that there was no difference when wearing the weighted vest as compared with baseline, 22 whereas for children with ADHD, one study demonstrated a significant improvement when wearing the weighted vest. 15 These 2 studies were of moderate scientific quality.
Stereotyped Behaviors
For ASD children, one study demonstrated that there was no significant difference between the weighted-vest condition and the baseline. 23 However, for ASD and developmentally delayed children, results were variable because stereotyped behaviors decreased during the weighted-vest condition for 1 of the 3 children. 17 These 2 studies were of moderate scientific quality.
Other Variables
A series of variables was less studied. For ASD and developmentally delayed children, one study demonstrated an increase (significant for only 1) in behavioral problems when wearing the weighted vest. 17 For children with ADHD, in one study, positive effects were seen for task completion speed, 16 whereas in one study, no effects were observed for impulse control. 15 The quality of these studies varies from fair to moderate.
Sensorimotor Approaches
Of the 13 studies related to sensorimotor approaches, 11 studies had quasi-experimental designs and 2 had experimental designs. Many different modalities were used, including therapy balls, air cushions, platform swings, and physical activity. Most of the studies had a small sample that did not exceed 15 participants, except for 2 studies24,25 with 30 and 63 participants. For the majority of the studies, variables were measured by direct or indirect observations conducted by 1 or 2 observers at a specific time interval (the sequence duration of observation of the child’s behaviors). Nine studies had a moderate scientific quality, whereas the quality was rated low for the other 4 studies. Per the sensory-based approach, results for the efficacy of the sensorimotor approach were mainly reported on task engagement/on-task behaviors, in-seat behaviors, and stereotyped behaviors. Results for each dependent measure and submeasure are presented below according to the modality used and the diagnosis for the children.
Task Engagement/On-Task Behaviors
Two low-to-moderate quality studies used therapy balls with ASD children. One showed a variable efficacy according to the child’s sensory characteristics, 26 whereas the other showed an improvement of this behavior when using this modality. 27 With the same modality, but in children with ADHD, in their moderate-quality study, Fedewa and Erwin 28 showed an improvement of 70% of the on-task behaviors. Two low-quality studies used air cushions: one was in children with ASD, 29 whereas the other was in children with ADHD. 25 For ASD children, no differences were observed when compared with standard chair, but positive effects were seen for the children with ADHD using this modality. Two moderate-quality studies compared the latter modalities (therapy balls, air cushion, and standard chair) with ASD children.28,29 Therapy balls led to higher improvements, and air cushions were still considered better than standard chairs. One moderate-quality study used platform swing with ASD children and found that there was no significant difference when compared to listening to a movie. 22 Finally, 3 low-to-moderate quality studies used physical exercises with ASD children, and 2 of them showed an improvement,30,31 whereas the other did not demonstrate a significant difference with the baseline measure. 32
In-Seat Behaviors
Two low-to-moderate quality studies used therapy balls with ASD children. One showed a variable efficacy according to the child’s sensory characteristics, 26 whereas the other showed an improvement in in-seat behaviors when using this modality. 33 However, the 2 moderate-quality studies using this modality in children with ADHD demonstrated an improvement of this behavior during the intervention phase.28,33 One moderate-quality study used air cushions with ASD children, and it demonstrated that there was no significant difference between this modality and the standard chair. 29 Moreover, 2 moderate-quality studies investigated the efficacy of the latter 2 modalities (therapy balls and air cushions) for ASD children and showed that they had a better effect compared with the standard chair.30,31 Only 1 moderate-quality study used the platform swing with ASD children and showed that there was no significant difference between this modality and listening to a movie. 24
Stereotyped Behaviors
One moderate-quality study used a platform swing with ASD children and showed no significant difference between this modality and listening to a movie. 24 Results regarding the use of physical exercises with ASD children are contradictory because Neely et al 34 showed a reduction in these behaviors with this modality, whereas Oriel et al 32 demonstrated no significant difference between the phases with or without the intervention. These 3 studies had moderate scientific quality.
Other Variables
A series of variables was less studied. One moderate-quality study used aerobic exercise with ASD children and showed an improvement in the production of correct academic responses. 32 However, with these children, but with the use of a platform swing, results from a moderate-quality study differ regarding the production of correct academic responses. 35 Finally, 2 moderate-quality studies investigated the effect of therapy balls in children with ADHD and showed positive results: one on the Attention-Deficit/Hyperactivity Disorder Test score 28 and the other in writing legibility. 27
Sensory Integration Approach
All the studies on sensory integration had an experimental design and followed the standardized sensory integration protocol of Ayres as cited in Roley et al. 36 The sample sizes varied from 29 to 103 participants. Dependent variables measured were academic skills, visuomotor skills, global and fine motor skills, and behavioral skills. The main method used to measure these variables was standardized assessment tools such as the Bruininks-Oseretsky Test of Motor Proficiency Second Edition (BOT-2) or the Developmental Test of Visual-Motor Integration. The scientific quality was evaluated as low (n = 2) to moderate (n = 4). Results for each dependent measure are presented below according to the diagnosis for the children.
Academic Skills
Regardless of the diagnosis for the children, none of the studies demonstrated significant differences between the use of sensory integration therapy and other interventions, such as tutoring and perceptual-motor training or no intervention.37-41
Visual Motor Skills
For children with learning disabilities and sensory disorders, results differed between studies. In a moderate scientific quality study, Humphries et al 38 showed that sensory integration therapy led to better effects than perceptual-motor training or compared with no treatment for one subtest of the Southern California Sensory Integration Test (SCSIT). In contrast, in another moderate-quality study, for a subtest of the SCSIT, the results revealed that sensory integration therapy was less favorable than perceptual-motor training and not different from no treatment. 39 Moreover, for children presenting with the same diagnosis, a study of low scientific quality demonstrates no significant difference between this modality and no treatment. 37 For children with motor difficulties and sensory disorders, Wilson et al 41 demonstrated no significant difference between this modality and tutoring.
Global and Fine Motor Skills
For children with learning difficulties, Humphries et al 38 found no difference between the use of sensory integration therapy and perceptual-motor treatment, except for the strength component of the BOT-2. In contrast, Humphries et al 39 found that perceptual-motor training leads to better effects. However, specifically for fine motor skills, no significant difference was found between the 2 interventions. These 2 studies were of moderate scientific quality. No significant improvements in global and fine motor skills were reported for children with ADHD or those with learning disabilities, 40 nor for children with sensory disorders40,41 and for children with motor difficulties. 41 One study had low scientific quality, 40 whereas the other was moderate. 41
Behavioral Skills
No significant difference between the experimental and control groups was found for this variable in children with ADHD, or with learning disabilities, 40 sensory disorders,40,41 or motor difficulties. 41 One study had low scientific quality, 40 whereas the other had moderate quality. 41
Other Variables
Regardless of the disorder presented by children, no significant difference was found between the experimental and control groups for 7 less-studied variables: language, praxis and visual functioning, handwriting readiness, attentional skills, ocular control, self-esteem, and reactivity measure.38,39,41 However, for executive function, one study measured significant improvement for children with ADHD. 42 Most of these studies were judged to be of moderate scientific quality (except for one with lower quality).
The variability of the results according to the dependent variables measured and the diagnostic of the children, combined with the variable scientific quality of the studies as illustrated, show that it is not possible to clearly identify which approaches are associated with the highest level of evidence. Also, results between studies of the same approach and presenting a similar level of scientific quality differ. Therefore, recommendations for therapy use are difficult to make.
Discussion
This systematic review organized the body of evidence for 3 specific approaches (sensory-based, sensorimotor, and sensory integration) and examined their efficacy on different variables associated with school participation of children with diverse diagnoses (eg, ADHD). Given the highly variable results and the overall low to moderate scientific quality of the studies, our conclusion at this point is that it is not possible to conclude on the efficacy on school participation for either of these 3 sensory approaches.
Several factors can explain the variability of the results: use of different protocols for the same modalities, medication use of various children in several studies that can influence their behaviors, and sample of children presenting with different diagnoses associated with different levels of disability. In our view, the main factor contributing to the discrepancies in the results is that experimental groups are formed based on the diagnosis for the children. However, for the same diagnosis, we can expect that children will present with many different sensory characteristics. Many studies show that children with ADHD have significantly different sensory modulation characteristics when compared with children with no diagnosis. 43 However, Mangeot et al observed that “considerable variability in sensory processing occurs among children with ADHD.” 44 (p404) The same situation can be identified for children with ASD. For example, Myles et al 19 report significant differences in sensory processing between 2 disorders of the spectrum: autism and Asperger syndrome. Sensory modulation disorders can be categorized according to 3 categories of profiles: (1) overresponsivity, (2) underresponsivity, and (3) seeking, which describes craving of, and interest in, sensory experiences that are prolonged and intense. So it is possible that some particular modalities are more effective for specific sensory profiles. Indeed, the results of our literature review suggest the interesting possibility that children identified as sensory seeking may be the most responsive to sensory-based and sensorimotor approaches.
This hypothesis suggests that the child’s particular sensory characteristics should primarily be taken into consideration to identify which sensory intervention modality and approach fit him or her best. Also, this systematic review revealed that there is another important thing to consider when choosing a sensory approach and establishing its protocol of use: the intervention’s objective. It must be considered because the same modality can be used in several ways to achieve different objectives because they can be used according to several approaches that have different aims. Thus, sensory integration, by working on the underlying skills, is mainly used to improve academic performance and develop the child’s capacity to respond to sensory stimuli in a way that meets the expectations of the environment. Sensory-based and sensorimotor approaches aim to increase the child’s engagement in school activities and to improve behaviors that have impacts on learning. Therefore, because the current level of evidence does not point to a specific approach as best practice, the intervention’s objective can be first used to direct the choice of the approach, which then influences the determination of the modality and the establishment of the interventional protocol.
These conclusions and hypotheses need to be nuanced according to the strength of the evidence. Indeed, none of the studies selected in the review presents a scientific quality higher than moderate. For the 3 types of approaches, the internal validity is limited because of the measuring methods. Assessors were not blinded, and some were directly concerned by the conclusions of the study, so they may not have been completely objective in their rating. Moreover, for many studies on these 2 types of approaches, the external validity was limited by the use of single-case designs. Results from this type of design are difficult to generalize because of the small sample size and variability of sensory characteristics of the participants. All these methodological concerns limit the degree of confidence that can be accorded to the results of this systematic review and the possibility of generalization of its results.
Despite the level of evidence, it is important to note that various pragmatic factors favor the clinical use of sensory-based and sensorimotor approaches rather than sensory integration. Although several practitioners, such as occupational therapists or physiotherapists, already have the expertise to use sensory-based and sensorimotor approaches in their day-to-day practice, the use of sensory integration therapy requires additional specific training. Ashburner et al 12 have even noted that well-trained practitioners in sensory integration often modify the protocol of use in response to the increasing pressure of efficiency and limited resources in their clinical context, which compromises the validity of this standardized approach. Moreover, the sensory-based and sensorimotor approaches are particularly easier to use at school because the child does not have to leave the classroom for a long period, which is the case with sensory integration therapy. On the other hand, although sensory-based and sensorimotor approaches seem favorable to use when compared with sensory integration, their applicability could be influenced by the teacher’s interest in and beliefs regarding these approaches. Indeed, as the modalities are directly implanted in the classroom, teachers need to be involved in the implementation of interventions and need to closely collaborate with the practitioners. Important modifications and adaptations need to be done in the classroom because it was highlighted that lack of adequate training and preparation among teachers was a critical concern. 45 Therefore, whichever approach is used, the practitioner needs to carefully inform the teacher about the protocol and its use with each of the children. They should also monitor closely the use of the modalities to make sure that it responds effectively to the child’s need and is appropriate in the educational context.
In conclusion, sensory intervention modalities related to sensory-based, sensorimotor, and sensory integration approaches are commonly used by therapists, but the results regarding their efficacy in improving school participation are highly variable between studies, and most of them have low to moderate scientific quality. Therefore, in the future, new studies with stronger methodology should be done to better assess the efficacy of sensory intervention approaches to improve school participation in children with sensory disorders. Moreover, the trend observed in the literature suggests that the focus should be on specific sensory characteristics rather than on the diagnosis to conduct further experimental and quasi-experimental research. More specifically, it would be interesting to document if sensory-based approaches are more effective than sensorimotor approaches for sensory-seeking children because these 2 approaches do not reduce children’s time in class and, therefore, avoid the catching up that would be associated with missed learning. Finally, practitioners need to be aware of future evidence related to the use of sensory intervention modalities in the school context. But now, because there is no consensus in the literature, they have to make a critical and conscientious use of the 3 approaches studied and carefully monitor their use with children in the classroom.
Supplemental Material
ST1-5_and_SF_1-2 – Supplemental material for Efficacy of Sensory Interventions on School Participation of Children With Sensory Disorders: A Systematic Review
Supplemental material, ST1-5_and_SF_1-2 for Efficacy of Sensory Interventions on School Participation of Children With Sensory Disorders: A Systematic Review by Béatrice Ouellet, Emmanuelle Carreau, Valérie Dion, Anouk Rouat, Elyse Tremblay and Julien I. A. Voisin in American Journal of Lifestyle Medicine
Footnotes
Appendix
Acknowledgements
We would like to thank Pre Marie-Josée Sirois, Myriam Chrétien-Vincent, and Pre Claude Vincent for their help. Emmanuelle Careau holds a Junior 1 Research Scholars grant from the Fonds de recherche du Québec—santé (FRQS). Julien I. A. Voisin holds a Start-up program for new research professor grant from the Fonds de recherche du Québec—société et culture (FRQSC). The authors declare that there is no conflict of interest.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.