
Abstract
Lifestyle medicine group sessions present a promising approach to clinical care. Based on decades of work in shared medical appointments and group visits for diabetes and other chronic conditions, a lifestyle medicine group session has the potential to provide a fresh and rewarding way of interacting with patients that fuels the practitioner and feeds patients’ needs to spend time with the lifestyle medicine practitioner, connect with him or her, connect with others, learn the latest recommendations regarding healthy habits, practice these behaviors, and discuss their obstacles, motivations, and strategies for healthy living. The lifestyle medicine group session discussed in this article is a combination of group coaching, education, and group support.
‘Participants may share experiences and advice with one another for the benefit of the group, whereas the practitioner leads the group discussions and provides guidance.’
Group Visits Are of Growing Interest in Lifestyle Medicine
A group visit involves multiple patients seen at once for chronic disease management or follow-up care. These types of visits offer an interactive setting in which patients have improved access to health care providers, more participation in their own medical care, and the advantage of counseling and support. Participants may share experiences and advice with one another for the benefit of the group, whereas the practitioner leads the group discussions and provides guidance. The medical literature supports group visits as an effective method for enhancing patients’ self-care, improving clinical outcomes, providing peer support, and increasing patient satisfaction.
Practitioners are longing for a change because patients are not following instructions and are not changing behavior when they are advised to do so. This creates frustration because practitioners keep repeating key pieces of information to each patient visit after visit, and also, they repeat the same information to one patient as they do to another. A universal complaint among practitioners is that there is not enough time in the day to complete all the paperwork, electronic record keeping, and patient follow-up. Practitioners need more time with patients, but the current system demands that physicians spend more time at the computer. Most practitioners desire to have a solid connection with patients, not their computers. Most patients simply want more time with their doctors.
Practitioners and patients have been longing for a change for many years. One solution that has been tried and studied is the group visit. During group visits, the practitioner spends an hour or two with as many as 12 patients. This gives the practitioner time to share medical information about a specific condition, a risk factor, a symptom or a sign of a disease with 12 patients instead of 1. Thus, the problem of constantly repeating information is partially alleviated. The patients spend an hour or more listening to their practitioner, learning about different medical conditions, and asking questions. Because many patients have the same or similar questions, the practitioner does not need to repeat the answer during different office visits. One answer can work for 12 patients.
Ten years ago, there were enough studies to write a review article. Jaber et al 1 published a qualitative review on the benefits of group visits. This article reported on a variety of patient populations, including those with chronic diseases such as diabetes, coronary artery disease, and headaches. Middle-aged men and women, children, mother-infant pairs, frail elderly, and low-income patients were among the populations included in this review of group visits. As a whole, the results of the group visits were positive for patient and practitioner. The authors reported, “Patients appreciated the physician’s unhurriedness, time spent with the physician, and overall quality of care.”(p283) And, for practitioners, they reported that the group visits were enjoyable, and physicians were “extremely” satisfied with their ability to treat patients in a group setting. In addition, it was noted that with the group format, pediatricians were able to review more material, covering significantly more American Academy of Pediatrics–recommended content in the areas of safety, nutrition, behavior, development, and sleep. Both patients and practitioners reported favorable experiences with group visits. 1
Reviewing studies on group visits from 1974 to 2004, the Jaber et al 1 article reported on several important behavior changes, including better medication compliance. For psychological changes, the patients reported increased self-efficacy and improved quality of life after group visits. In terms of labs, studies report reduced blood pressure and cholesterol, improved control of mean blood glucose, and decreased glycated hemoglobin (HbA1c) levels. Reduced obesity was also reported. Financially, health care costs decreased as a result of fewer emergency and urgent care visits and fewer specialist referrals. Studies also demonstrated increased patient and physician satisfaction as well as improved doctor-patient relations. These benefits are shown in Table 1. However, group visits made no significant difference on scores of depression and functional status. 1
Benefits of Group Visits.
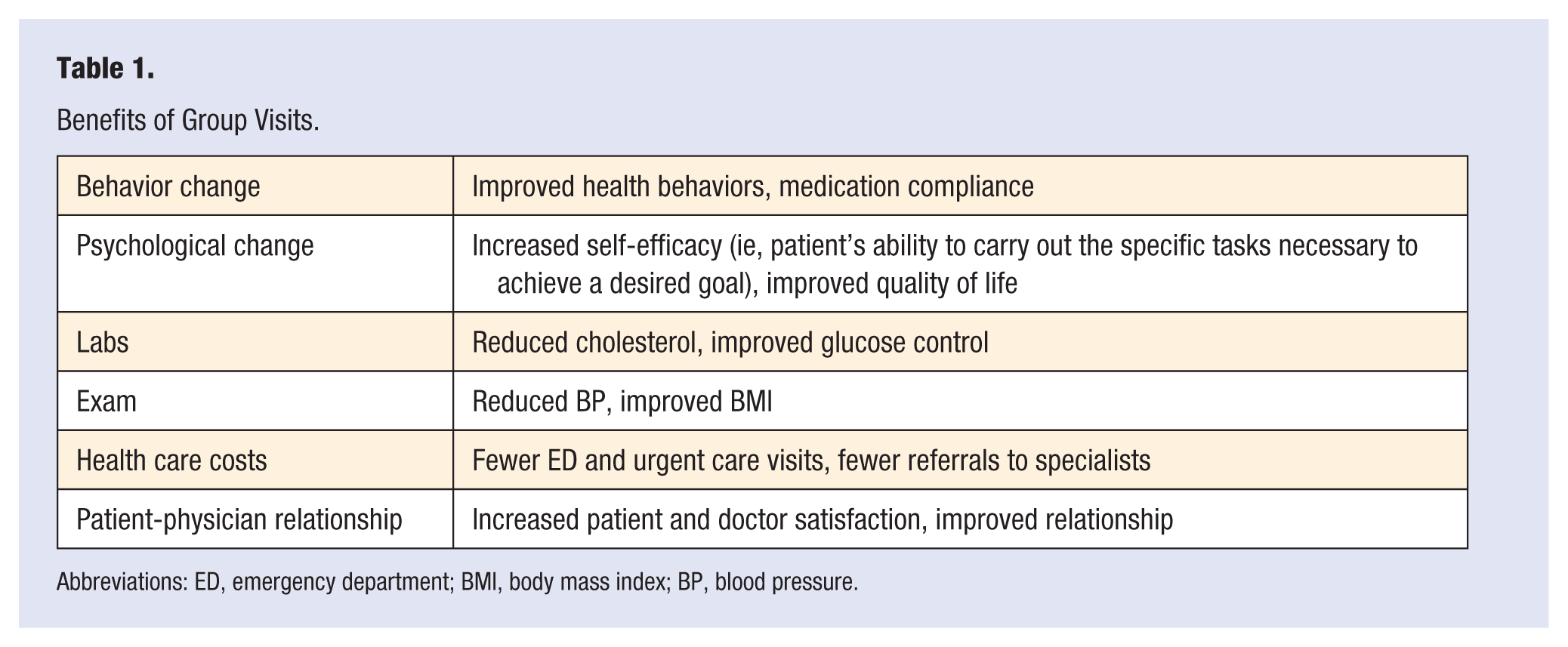
Abbreviations: ED, emergency department; BMI, body mass index; BP, blood pressure.
The Jaber et al 1 review was extensive but had limitations. For example, studies differed in many aspects, including group visit model, educational content, presentation style, patient populations, and length and frequency of sessions. In general, sample sizes were small, varying from 28 to 497 per study. Conditions studied included diabetes, metabolic syndrome, hypertension, arthritis, asthma, Parkinson’s disease, stress, and sleep disorders. This review indicates that group visits can be effective and rewarding for the patient and practitioner, but more studies are needed to fully understand the group visit process.
Diabetes is a disease that lends itself to group visits given its prevalence, the number of instructions the patients need to follow, and the frequency of follow-up required to keep patients on track. A review of only randomized controlled studies with diabetes patients found that group visits provided a significant reduction in HbA1c compared with routine care. 2 In another review focused on diabetic patients, which also only included randomized controlled trials, the authors noted improved clinical, lifestyle, and psychosocial outcomes with group visits compared with usual care. 3 The literature supports the use of group visits for diabetic patients because it improves blood glucose control as well as lifestyle and psychological factors.
Shared medical appointments are a specific type of group visit that resembles a one-on-one visit for blood pressure, weight checks, medication adjustments, and lab tests. If a patient requests privacy, he or she will go to a private space for an exam. The other patients are in the session room and participating in a group discussion, usually with a behavior change expert such as a psychologist or therapist. Many structures and strategies exist for group visits. The systematic review by Edelman et al 4 found that shared medical appointments improve intermediate clinical outcomes for type 2 diabetes. They concluded that these types of visits may be most effective for diseases such as diabetes, where there is a long symptom-free period in which education and self-care are critical components of the treatment.
Use a Systematic Approach to Plan Group Visits
There is no one-size-fits-all approach to group visits. There are different group types, financial models, and formats to consider. Just as local communities and patient populations vary, so will the styles of group visits that best meet the needs of the patients. The size of the group, length and frequency of meeting, and location must also be determined.
The type of group refers to the style or purpose of the group, which may be clinical, educational, or coaching. Table 2 demonstrates information on the type of possible group sessions. Clinical group visits are focused on the management of acute or chronic conditions. The American Association of Family Physicians 5 as well as Mass General Hospital 6 have previously published guides focusing on clinical group visits for chronic conditions. Group visits focused on diabetes or obesity are popular examples of this type of group session. Acute clinical visits called Drop In Group Medical Appointment were pioneered by Edward Noffsinger and are outlined in a number of medical journals. 7 Group visits in lifestyle medicine tend to focus less on acute conditions and more on behavior change.
Types of Group Sessions.
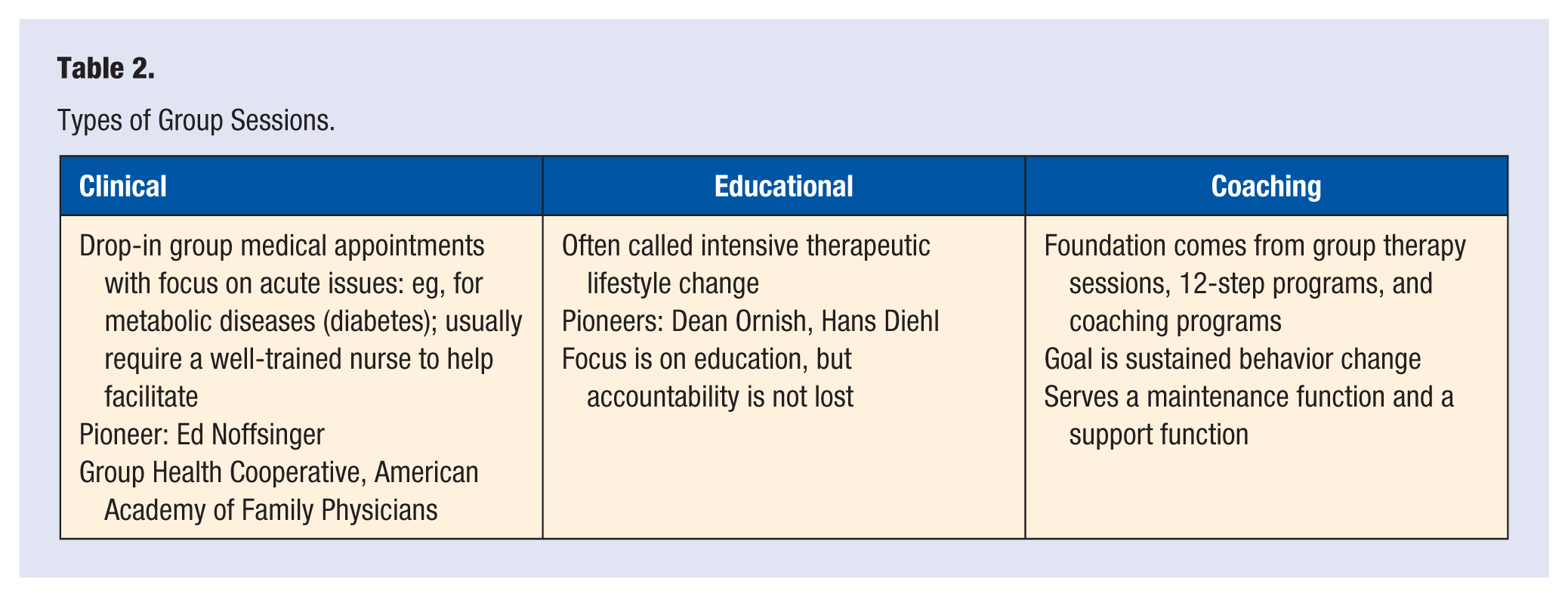
Educational group visits in lifestyle medicine are frequently called intensive therapeutic lifestyle change programs. The focus is on education and presentation, but accountability is not lost. As examples, consider the Ornish Reversal Program by Dean Ornish and Hans Diehl’s Complete Health Improvement Program. These are successful models of group sessions in lifestyle medicine.
Coaching group visits facilitate knowledge sharing among participants rather than directly educating the group. Support groups such as group therapy and 12-step programs rely mostly on the participants themselves to be successful. The group provides a support function and a maintenance function to help members achieve sustained behavior change. The coaching model builds on this foundation of group support. However, in addition, there is a practitioner or leader who is setting the tone for the group and helping to organize the sessions. There is an element of education in these coaching sessions, but the majority of the time is focused on behavior change strategies and empowering patients to take steps toward adopting healthy lifestyles and abandoning unhealthy habits. Armstrong et al 8 provide evidence and examples for coaching group visits.
When planning to start a lifestyle group session, it is important to consider the financial model. Dr Dean Ornish’s program is one of the few programs that is covered by insurance. Other payment models include standard billing and coding, capitation, and self-pay, as described in Table 3. A successful billing method is to submit a 99213 bill for each patient. For this, participants must be established patients with a relevant diagnosis. If the history and medical decision making are documented adequately, a physical exam is not required, though providers often choose to collect vital signs. Public and private insurers are generally supportive as long as the visit frequency is reasonable.
Creating Financial Viability.
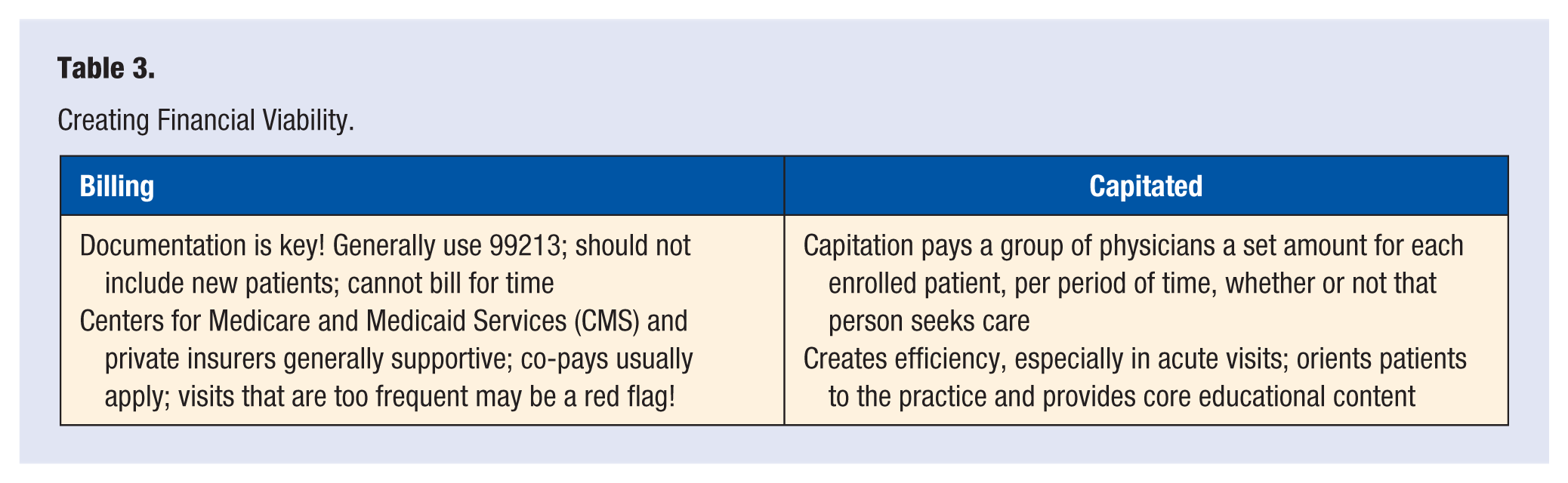
Capitation is a model that pays a group of physicians a set amount per patient enrolled, whether or not a patient seeks care. This promotes efficiency by encouraging providers to utilize time and resources wisely. For example, a provider may choose to save time by holding a group session and educating several patients at once about preparing for a colonoscopy rather than repeating the information at individual visits.
Self-pay models have the advantage of simplicity, but cost often greatly limits participation. Dr Hans Diehl’s Complete Health Improvement Program and the Stroke Wellness Program run by Dr Beth Frates at the Stroke Institute for Research and Recovery, Spaulding Rehabilitation Hospital, a Harvard Medical School affiliate program, are examples of self-pay programs.
The visits may utilize any of a variety of different formats. Didactic lectures or semistructured discussion formats tend to be popular. Videos or other multimedia components may be included. When transportation may be an issue, for example, in underserved areas or for patients seeking specialist care for a rare condition, an online webinar format may be most practical.
Physicians, psychologists, nurses, and nurse practitioners often lead group visits because this simplifies the billing process. Health care professionals such as dieticians, nutritionists, behavioral health experts, physical therapists, occupational therapists, social workers, and others may also be involved. Most clinical group visits require a well-trained nurse or medical assistant to help facilitate.
Marketing is a common challenge because administrators and patients are often unfamiliar with group visits, and they typically do not fit into the regular office visit routine. Health systems tend to focus on individualized care. Practitioners can address these obstacles by leveraging personal connections; targeting specific patients and family members is a good first step to create a group. Working toward building attendance into clinical care for chronic conditions, with systematic referrals from partnering groups or medical practices, is a strategic goal. Keeping a broad focus for the group allows the practitioner to market to a larger audience: for example, focus on metabolic syndrome as an array of diseases rather than focusing on only diabetes. There is an aspect of trial and error and an aspect of filling the need in a specific panel of patients or a particular community.
Use Behavior Change Techniques to Engage Participants
Engaging people in their own behavior change is a process of collaboration and negotiation between the practitioner and the patient. Effective behavior change techniques are essential in group sessions. Some therapeutic benefit stems from patient-to-patient interactions as well as patient-practitioner interactions. Behavior change techniques used in group coaching sessions include motivational interviewing, appreciative inquiry, transtheoretical model of change, social ecological model of change, positive psychology, goal setting theory, adult learning theory, accountability, and tracking.
One of the most important clinical skills to utilize during group sessions is listening. Patients enjoy sharing their stories and listening to others. It is important for the leader to spend more time listening than talking. Evoking change talk by asking powerful questions is a useful skill to hone. The practitioner does educate and share his or her wisdom with the group. This can be accomplished in a “just in time” methodology, where the practitioner gauges the interest and needs of the group and provides information that is relevant and timely for the individuals in the session. Identifying a patient’s readiness for change will aid the practitioner in collaboration. 8
The coach approach fosters collaboration and empowers behavior change in group sessions. This is often more effective than the “expert approach” in group visits. The expert approach is necessary in acute situations such as a myocardial infarction, broken femur, or pulmonary embolism. However, for chronic disease management, the coach approach provides the right mix of education and support to help patients adopt and sustain healthy habits. The basic differences between the 2 approaches are demonstrated in Table 4.
Coaching for Behavior Change: Expert Versus Coach. a
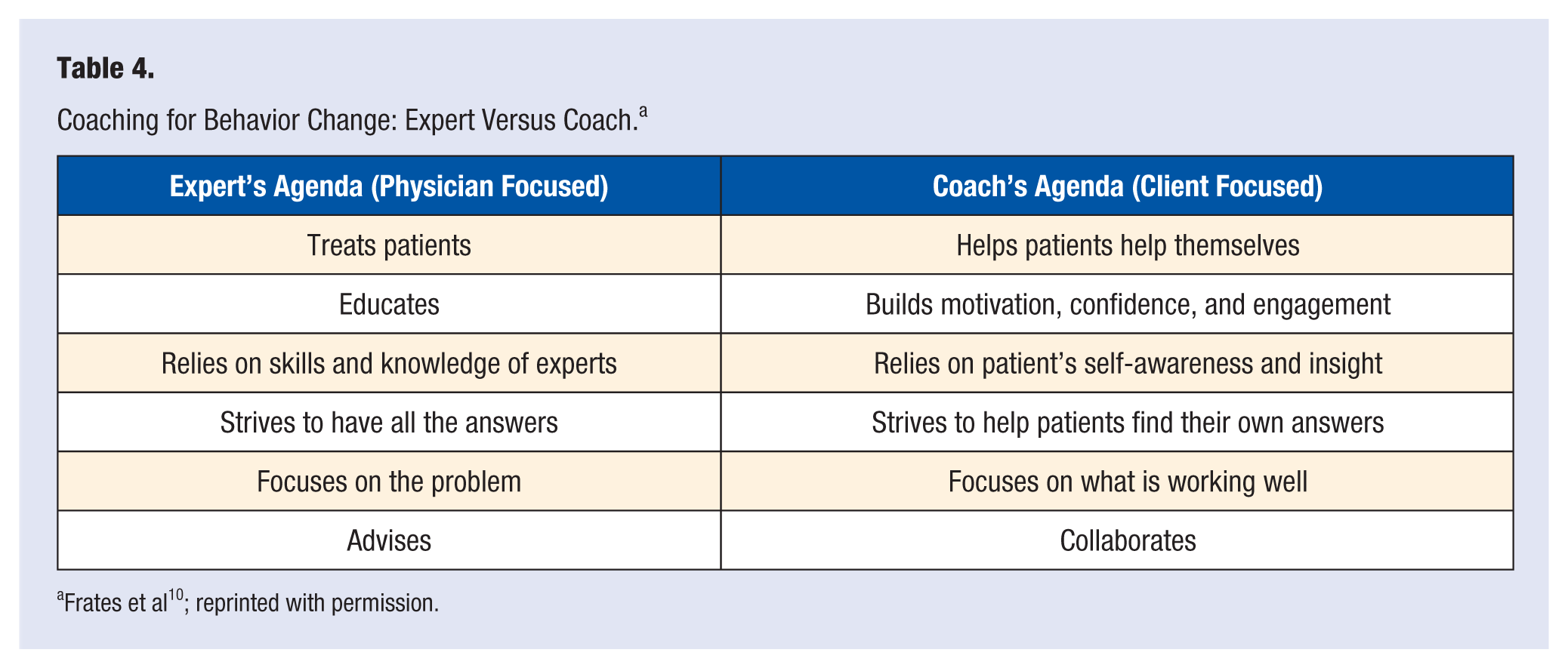
Frates et al 10 ; reprinted with permission.
Health and wellness coaching is a burgeoning area, and randomized controlled studies support its use in chronic conditions.8,11 Health coaching conversations are particularly powerful in group sessions because they empower patients to use their strengths to conquer obstacles and find internal motivators to make lasting change. Focusing on collaborating and negotiating with the patients in the group rather than telling and advising them what to do to tackle behavior change will open up the space patients need to find the solution to their problems that works for them. Patients are the expert of their own life experiences, past failures, recent successes, personal preferences, and family dynamics in their own household. This knowledge is necessary for the patient to craft a behavior change plan that will be successful in the short and long term. These coaching conversations help bring out the wisdom inside the patient and help the patient apply that wisdom to adopting healthy lifestyles. 9
The key to behavior change is to collaborate with the patient. Figure 1 outlines the 5-step cycle that demonstrates the steps to successful collaboration with patients. It provides a system to follow when striving to use the coach approach in one-on-one meetings as well as group sessions. First, the practitioner needs to try to see things from the patient’s perspective and learn about the patient by listening attentively. Then, the practitioner can focus on evoking change talk and helping identify powerful motivators for change that resonate with the patient. With motivators in place, the practitioner can work on helping the patient to use his or her strengths and to remember successful experiences in the past. This will help increase the patient’s confidence. The fourth step is to cocreate SMART goals with the patient. These are specific, measurable, action oriented, realistic, and time sensitive. The patient needs to select the goal that is most meaningful to him or her, and the practitioner can help word it in a way that is SMART. Finally, the practitioner needs to check in on the patient’s goals to hold that patient accountable or put a system of tracking and monitoring in place that works for that particular patient. A spouse, friend, or fellow program participant can serve as an accountability buddy. When the practitioner sees the patient again at the next visit, the cycle starts again with empathy and listening to the patient’s story. If the patient was successful, the practitioner celebrates the glory with the patient. If the patient was unsuccessful, the practitioner works to uncover what happened and how things can be altered to set the patient up for success next time. Trying to understand the experience of failure or success through the words and emotions of the patient is key to being empathetic.
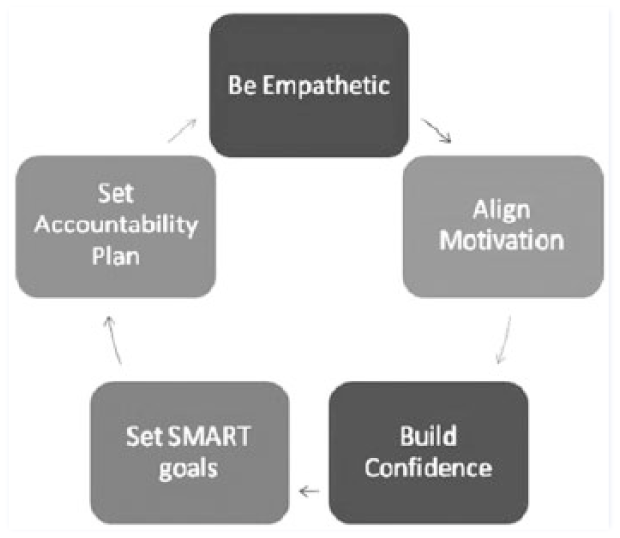
Five-step cycle in the coaching model.a
Foster Cohesion Through Coaching
By listening, expressing empathy, helping identify motivators, highlighting personal strengths, building confidence, creating SMART goals, and holding patients accountable for their goals, the practitioner creates a bond with the patient. They are all on the same team and working to empower the patient to sustain healthy habits. With a group, this bonding can happen between 2 patients and among a group of patients as well.
The key to a successful coaching process is connection. There are 4 important connections to foster when leading a group session: connection with self, connection with patients, connection with the group as a whole and connections among participants.
The first connection, connection with self, might be the most important one. This has to be established in order for the other 3 to happen. Connecting with oneself means to be fully present with one’s emotional and physical state. This requires that a practitioner relax, breath easily, put away electronics, put aside worries, and focus on strengths, purpose, and mindfulness. Practicing self-care, routine exercise, healthy eating, restful sleep, and restorative practices will allow the practitioner the time and space to feel connected to himself or herself.
To connect with patients, the practitioner needs to listen to the patient and get to know him or her and know the personality, the past, the present, the motivators, the goals, the quirks, and the sense of humor of that patient. To connect with the group as a whole, the practitioner needs to be compassionate, authentic, curious, nonjudgmental, open, and honest. It is important to set a positive tone in the sessions. The leader strives to provide energy, hope, consistency, and reliability while showing vulnerability. Sharing one’s own struggles and successes reveals that the leader is human, and this builds connections with patients. Letting down defenses and being authentic is often difficult for practitioners. Being perfect and having all the answers is stressed in medical training. However, vulnerability might just be the key to the bonding process in these group coaching sessions.
Fostering connections among the patients is also critical. One easy way to plant the seeds for these connections is to plan activities in which patients work in pairs. This allows them to listen and learn about each other. Ask the patients to discuss their strengths with each other, or ask the group to help find solutions to problems that one patient might share. The practitioner can ask, “Has anyone else experienced this?” or “ Who remembers what ‘Bill’ said about this last week?” Another strategy to encourage socialization is to allow for extra time to mingle before and after each session. The more connected the patients feel to the leader and to the other participants in the group, the more sessions they will attend and the more they will participate during the sessions.
The overall goals for the group sessions are for participants to feel heard; to feel validated; to learn useful information; to receive practical tips; to share stories, strategies, or suggestions; to create a SMART goal for the next session; and to feel empowered to move forward. For these goals to be achieved, the leader must believe in the wisdom in the room, that each patient comes with their own wisdom, and that when everyone in the group shares wisdom, the group thrives. If the leader listens more than he or she speaks, the wisdom in the group will naturally surface. There is an art and a science to running a group lifestyle medicine session. It takes practice.
Resources
American Academy of Family Physicians Guide to Group Visits for Chronic Conditions Affected by Overweight and Obesity: http://www.aafp.org/dam/AAFP/documents/patient_care/fitness/GroupVisitAIM.pdf
Massachusetts General—Putting Group Visits into Practice: http://www.massgeneral.org/stoecklecenter/assets/pdf/group_visit_guide.pdf
Institute for Healthcare Improvement—The Business Case for Drop in Group Medical Appointments (DIGMAs): http://www.commonwealthfund.org/usr_doc/christianson_bcs_drop-ingroup_611.pdf
Complete Health Improvement Program: https://www.chiphealth.com/
Footnotes
Acknowledgements
This work was presented at Lifestyle Medicine 2016; October 23-26, 2016; Naples, FL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.