
Abstract
A lifestyle medicine (LM) practice aims to treat the whole person, with a focus on addressing the root lifestyle causes of disease. Creating a practice in LM comes with an array of challenges. Utilizing different payment systems and practice models, such as cash, traditional insurance, Direct Primary Care model, or concierge systems, allows for the incorporation of more LM services and ensures sustainability in the practice. One must develop a sound business model and aim to keep costs low. Optimizing coding, taking advantage of additional LM services, and expanding service formats to group visits or telemedicine are all creative ways to incorporate and develop LM practices. Anticipation of new challenges and flexibility in practice models and payment systems allows one to be successful in starting or transitioning to an LM practice.
‘With the lifestyle medicine (LM) approach, the emphasis is on treating the root lifestyle causes as the foundation of the treatment pyramid.’
Conventional Medicine Versus Lifestyle Medicine
The current conventional medicine model does tests, prescriptions, and procedures that are paid by third party insurers. The complexity created by having multiple payers with different coverage plans and services covered requires enormous staff, resources, and energy to manage appropriately. These challenges all take time away from providing direct patient care. The systemic inefficiencies, overwhelming paperwork, and depersonalization from lack of provider-patient time produces enormous provider and patient frustration. With the lifestyle medicine (LM) approach, the emphasis is on treating the root lifestyle causes as the foundation of the treatment pyramid (Figure 1), or first-line therapy, for most conditions. This is usually done through extended history taking, patient engagement, education, and counseling. There are challenges to starting or transitioning to an LM practice and reasons that a practice may not succeed. Common challenges include the following:
The lack of standardized guidelines at this time.
The lack of expertise in the components of practice outside of patient care: billing, business, management, marketing, and so on.
The lack of LM practice support systems, services, and resources.
Considering the conventional system and ever-growing time constraints, how does one practice this kind of health care and make it financially sustainable?
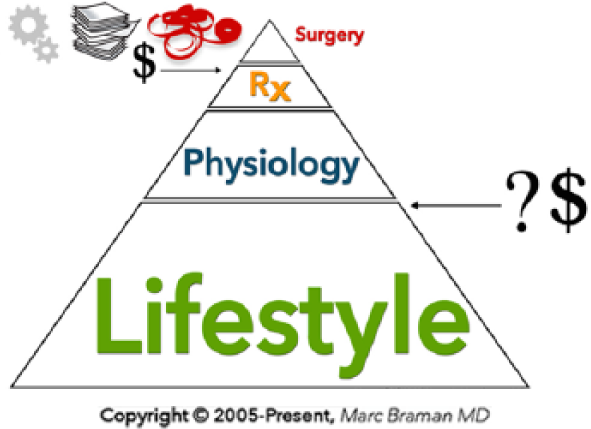
The left represents conventional medicine payment for treatment of symptoms and consequences. The right represents the LM challenge of payment for treating the causes of disease. Copyright © 2005-present, Marc Braman, MD.
The Whole Person Model
At the center of medicine is the patient. One must always remember that he or she is treating people. Treating the patient as a whole person is the core of LM (Figure 2). In health care, focus is primarily placed on the physical aspect of a person. To be most effective, one must consider the patient as more than just “the broken toe in room number three.” The mental, emotional, social, environmental, and spiritual domains of a patient’s life need to be understood. Gathering a complete, whole-person history requires more time than the traditional 15-minute patient encounter. This additional information allows for a more complete understanding and approach to each patient. Furthermore, the number of conditions that can be treated with LM is huge and encompasses the vast majority of diseases that are prevalent today.
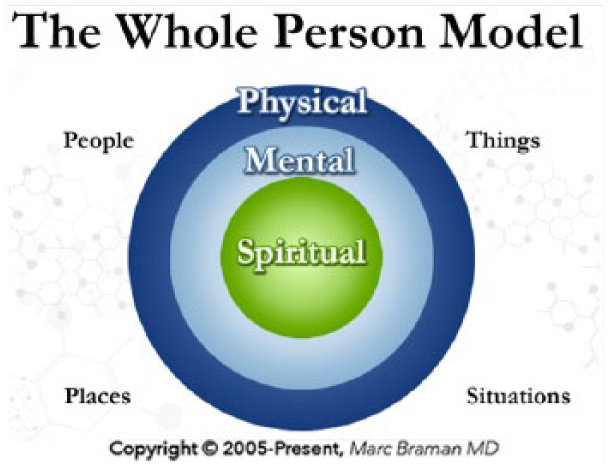
Whole Person Model including the people and context of a person’s life. Copyright © 2005-present, Marc Braman, MD.
Do “Real” Business
The business of health care is “different”; it is not real business. Hospitals are built and equipment is purchased using donations, grants, and other methods. There is not a true marketplace in health care. Pricing and value are typically obscured, the customer is often not paying the bill directly, and other similar dynamics keep normal marketplace forces from working. In this atypical market, attempting to build an LM practice using a typical business model is difficult and can often result in failure. One must approach the business aspects of an LM practice with the same evidence-based approach that is used in clinical medicine. Analogous to consulting a specialist for clinical issues beyond one’s area of expertise, it is important to engage business experts regarding the operations and business components of an LM practice.
The most basic practice management principle is to focus on keeping costs down. It is dangerous to start out with a large amount of financial debt and a lot of overhead. These 2 issues, disproportionate debt relative to cost generation and having too much overhead, are the most common causes for independent LM practices to fail. A practice or provider has a better chance for succeeding if they are able to keep overhead and costs low and are willing to be open to various revenue sources (ie, supplementing revenue from conventional systems or services as needed). Attempting to focus solely on LM services too early can result in insufficient revenue to maintain a practice. Additionally, there are some common misconceptions in health care that need to be recognized. These include the following:
Insurance paying claims does not mean they approve of the services being offered, codes being used, and billing practices. If the insurance company discovers that atypical practices are being conducted they may take their payments back.
If there is a code for a condition or service, it does not mean insurers will necessarily pay for it.
If insurance pays for a code or service, it does not mean it is worth performing. “Covered” services relevant to LM are often paid for at such a low rate that it is a net financial loss to provide and bill for them.
Be cautious of advice. Get expertise. There is a lot of wrong advice being given, often by people speaking outside their areas of expertise. One would not trust a billing person to do neurosurgery. Why would one trust a neurosurgeon to understand all of the complexities of coding and billing?
Payment Systems
In order to understand the role insurance plays in LM, one must recognize that insurance is a financial product. It is not health care. In many ways insurance companies do what they want, when they want. Knowing this, one must not let insurance companies dictate health practices or the medical services that one provides. Listed below are some of the most common business approaches of medical practices, followed by a few examples of LM practices.
The most basic payment method is cash payment. Two major drawbacks to using cash are dealing with patient expectations that insurance should pay for the services and that often patients do not have enough cash readily available for treatment.
Direct primary care (DPC) is another model becoming popular. It requires each patient to pay a set fee every month, which covers defined primary care services.
Traditional practice where insurance reimburses in a fee-for-service manner.
Concierge is similar to direct primary care in that patients pay a fee for access to a provider. However, it generally has higher fees and smaller patient panels. It does allow patients to have increased access to providers, but is considered to be a luxury service that is not accessible to many people.
Direct Primary Care Model
The DPC model is an alternative to current fee-for-service models where the patient pays a retainer—a monthly, quarterly, or annual fee—for all or most primary care services. Patients can use DPC alone or in combination with a high deductible health plan, health savings account, health share, or participating Medicare Advantage plan. (A health share is an Affordable Care Act exempt program [avoids the tax penalty for not having insurance] that is based on the Biblical teachings regarding sharing each other’s burdens.) The typical DPC model covers basic labs and allows for more personalized primary care. It does not cover specialists or hospitalizations. Thus, a combination of coverage can be beneficial.
A DPC model creates more flexibility in treating patients and allows for more communication options (eg, phone, text, email, or telemedicine), rather than only a traditional office visit. Typically, a provider will carry a patient panel of roughly 500 patients. It costs each patient roughly $100/month for the service. A firm understanding of practice management functions (ie, coding/billing, staffing, etc) is still required, and additional skills of retail business, such as marketing, are needed. The DPC model is very amenable to an LM foundation and may foster increased patient contact and engagement.
Traditional Practice
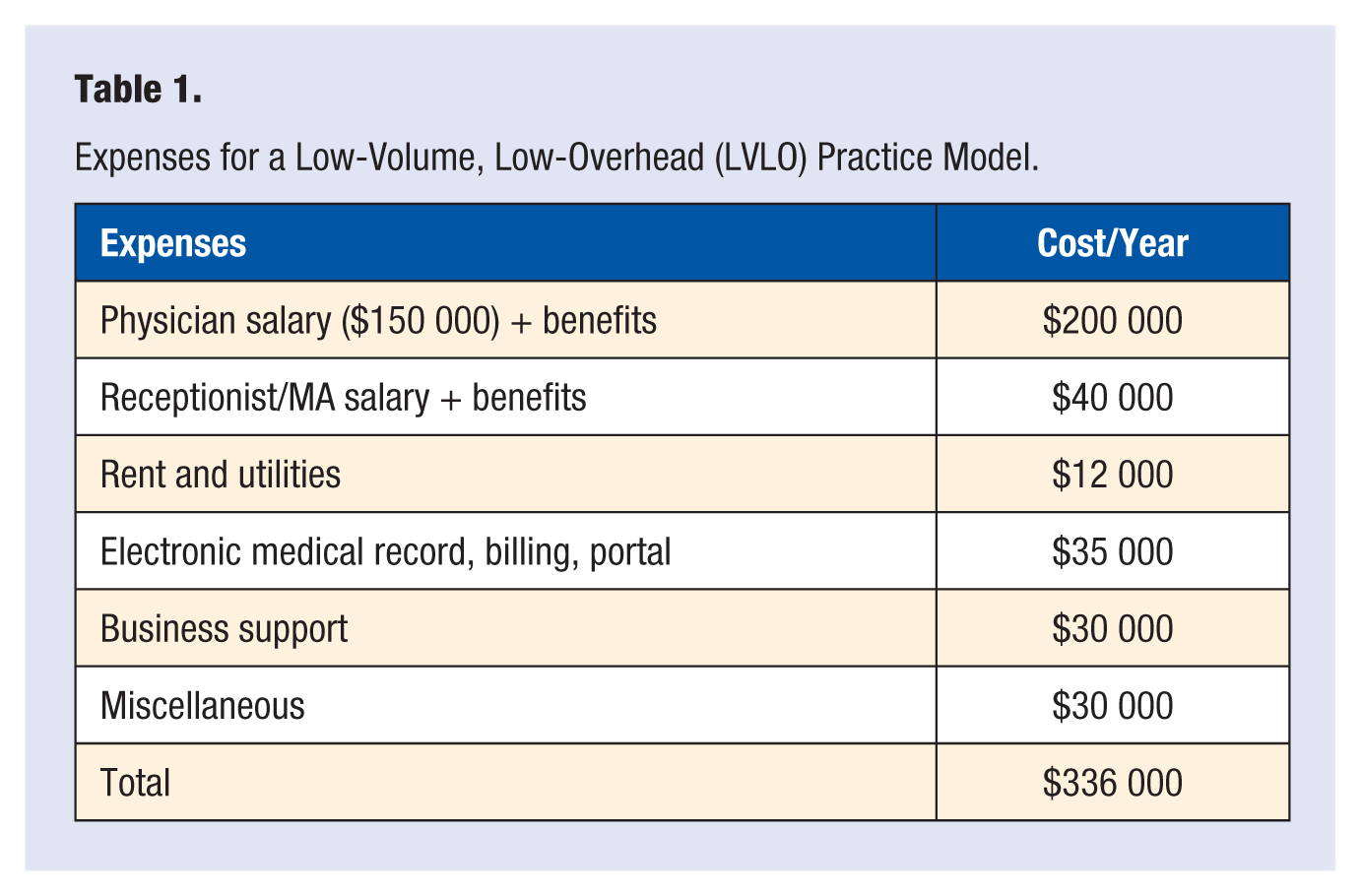
A traditional fee-for-service model may seek to incorporate LM components into the practice. Low-volume, low-overhead (LVLO), and retainer or subscription-based (eg, Direct Primary Care) are 2 other models for LM in a private practice setting. Table 1 provides anticipated expenses in an LVLO model that utilizes insurance reimbursement only. The example scenario is based on a subleased space within a larger clinic and has a limited staff consisting of a physician and receptionist. They use an all-in-one system for their electronic medical record, scheduling, billing, and patient access via a patient portal. They have a reasonable schedule with regular business hours and are closed on holidays. Typical reimbursement rates for the Pacific Northwest are consistently used. Table 2 presents a breakdown of income and profit for this scenario over a 1-year period. Profits are in addition to the base salary of the physician and receptionist.
Expenses for a Low-Volume, Low-Overhead (LVLO) Practice Model.
Profits With Different Payer Mixes.
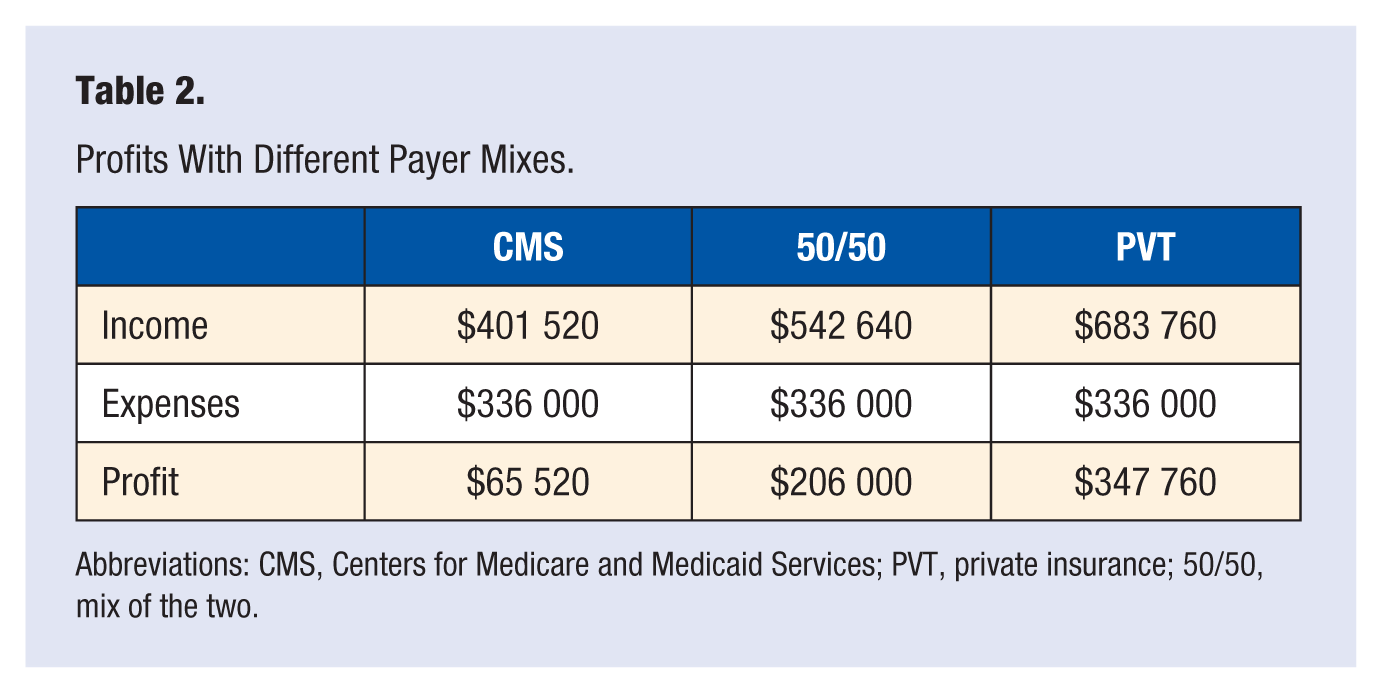
Abbreviations: CMS, Centers for Medicare and Medicaid Services; PVT, private insurance; 50/50, mix of the two.
Coding/Billing
Optimizing coding is key for success in an LM practice. One must understand the basics of coding as a foundation, then add LM-specific coding and time-based billing as appropriate. The most commonly used Current Procedural Terminology (CPT) code is 99213 (Private [PVT] insurance pays $121.00), which is equivalent to a 15-minute encounter. Visits for patients with chronic conditions are typically coded a 99214 (PVT insurance pays $179.01). A 99214 visit is reimbursed nearly 50% more than a 99213 visit. However, in order to code for a 99214 encounter, there must be proper documentation to support the higher level of service. Figure 3 highlights some LM relevant components of a visit that may comprise a 99214 visit. Documenting LM vitals such as sleep, stress, fatigue, nutrition, and so on may be appropriately placed in the Review of Systems (ROS) section. Documentation for LM interventions can be done in the decision-making section where one would normally document disease management treatments or therapies. Descriptions of why medications were not chosen in this section may be helpful. Time-based coding requires documentation of the amount of face-to-face time spent with the patient and that over 50% of that time was spent in counseling or care coordination.
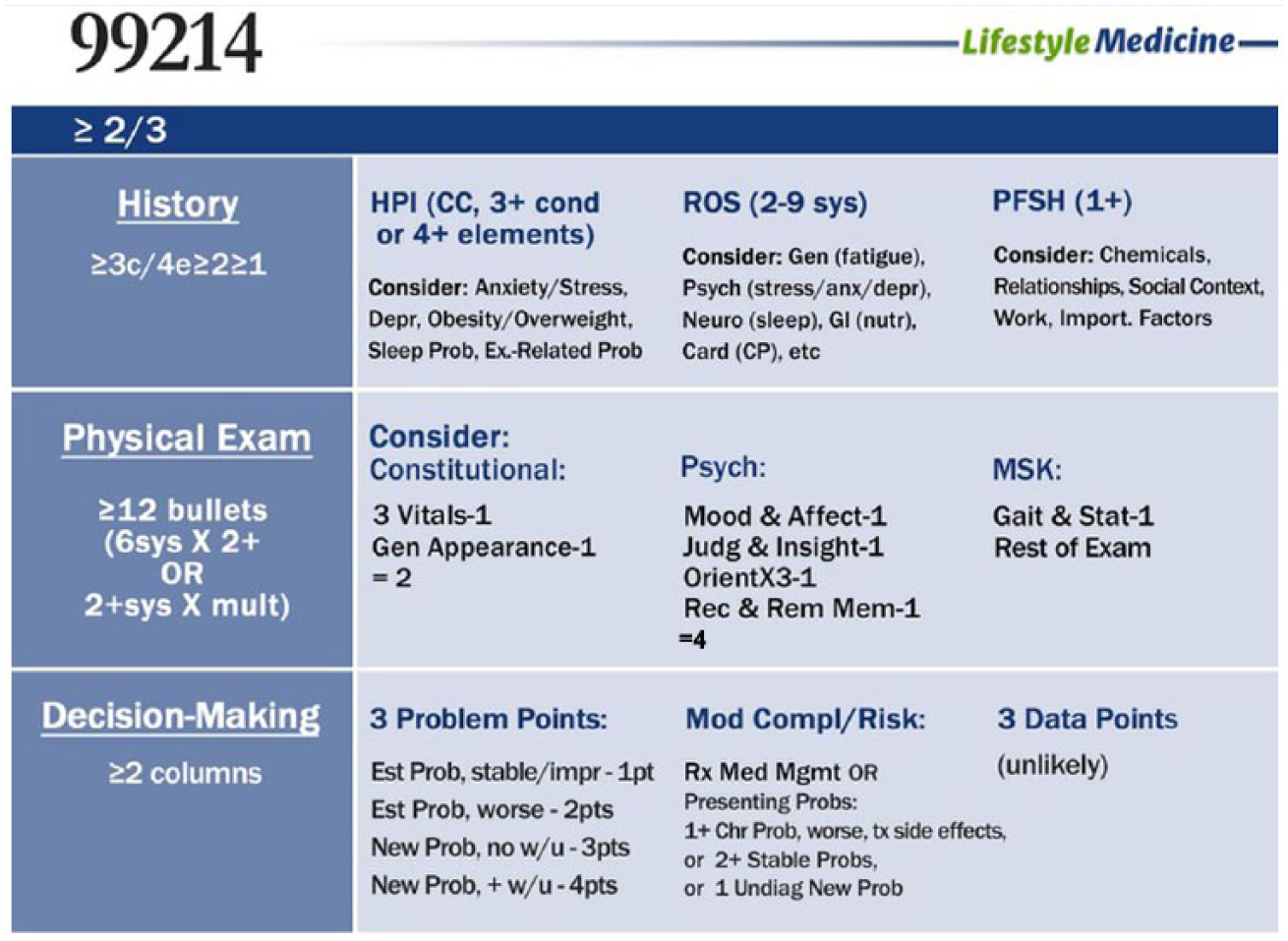
Potential LM relevant components for a CPT 99214 level visit. Copyright © 2016, Marc Braman, MD.
Lifestyle Medicine Services
There are a number of specific services that are worth considering. Medicare and various insurers provide 100% coverage for an annual wellness visit. This visit is a great opportunity to identify all the lifestyle-driven diseases that a patient has and discuss what lifestyle factors are responsible for creating them. Depending on what disease states a patient may have, there may be utility in providing ECGs, counseling, or other LM services. However, one must consider the reimbursement for these services. ECGs are often readily performed with existing equipment, though they do not produce significant additional revenue alone. Unfortunately, obesity and tobacco counseling are typically reimbursed at such a low level that counseling is usually a net loss for a practice. Other services may make sense for cash payment if the perceived value is sufficient relative to expense; however, reasonable evidence and clinical utility should always be considered. Telemedicine is an emerging vehicle that is well suited for LM, as much care does not need to be done in an office.
Group Visits
Billable group visits are another excellent approach to deliver high-quality LM. Advantages of a group visit include improvements in efficacy, patient and provider satisfaction, improved quality measures, and increased revenue when done well. A group visit also fosters community building among patients. Disadvantages of the group visit are the differences in scheduling and staffing, need for patient orientation, and need for additional staffing support. Care is delivered one-by-one in a group context. Documentation is done in the same way as used for individual office visits and standard office visit codes are used. One cannot use time-based billing for group visits or bill for education. This model of conducting and billing group visits should not be confused with educational models or group visit codes that are either reimbursed at unsustainable levels or not reimbursed at all.
The Future of Lifestyle Medicine
Health care will be changing dramatically as patients are increasingly empowered by technology to learn new information and connect with others. LM has become established with the development of professional bodies representing LM such as the American College of Lifestyle Medicine. The next major phase of LM’s development as a field is the increasingly widespread implementation and adoption of sustainable LM business practices and models. “Treating the cause” is the foundation and most important component of any present or future sustainable health care system.
Footnotes
Authors’ Note
This article is based on a keynote presentation delivered at the American College of Lifestyle Medicine 2016 Annual Meeting, October 26, 2016.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marc Braman discloses that he is the founder/owner of Lifestyle Medicine Pro, a practice support network for lifestyle medicine practice implementation.