
Abstract

‘What is the best way to approach her [SP] concerns about her cardiovascular risk from a lifestyle standpoint?’
SP is a 54-year-old emergency room physician who presents for an executive health physical for a comprehensive health assessment. She has 2 primary concerns:
She is concerned about cardiovascular risk. Her cholesterol has been as high as 270 mg/dL in the past. Five years previously she was told she had no evidence of coronary plaque by ultrafast computed tomography. Her father is alive at 86 with a history of both cardiovascular disease diagnosed in his 60s and prostate cancer. Her maternal grandfather died in his 50s of unknown causes, and her paternal grandfather died suddenly at the age of 40. She is an only child and there is no other family history of coronary artery disease. She does not want to take medications for her cholesterol.
She has symptoms consistent with restless legs. Although present for several years, they have worsened over the last year and are now interfering with the quality and continuity of her sleep, waking her up as much as 4 to 5 times nightly.
Past medical history: Menarche 14, regular but heavy. G0 P0.
Surgical menopause at age 47: s/p TAH/BSO for cervical cancer. She took oral conjugated equine estrogens for 5 years then stopped 1 year ago with no symptoms.
She is on no medications. She takes a multivitamin and occasional calcium chews.
Social history: she is divorced and works as the medical director of an emergency room. She loves her work, which is mostly administrative from 8:30 to 5:30. Two nights a month she works overnight in the emergency room.
Dietary habits: She does not eat meat or poultry; occasional shellfish.
Breakfast: Oats with honey and flax or pumpkin seeds, vegan “bacon,” tomato juice, and hot tea.
Lunch varies: Vegetable quiche or baked potato with vegetables.
Dinner: If out, sushi or ethnic food. If home (70% of her dinners): pasta with shellfish or vegetables. She does not drink alcohol. She snacks on sweets or ice cream when stressed and drinks 1 to 2 caffeine-free non–diet sodas daily. She reports exercising on a treadmill 30 to 60 minutes 4 times weekly. She also likes to garden.
Other key symptoms include heartburn twice weekly, which is worse with stress and relieved with over-the-counter antacids. She had been feeling more fatigued this last year and that has recently improved. Her weight has slowly crept up over the last few years, and she feels she is about 10 pounds over her ideal weight of 110 pounds.
Key findings on physical exam: height 5′0″, weight 120 pounds, body mass index (BMI) 23.4 (normal). Waist-to-hip ratio is 0.88. Blood pressure is 108/74 mm Hg. Her cardiopulmonary exam is normal. She has mild decrease in vibration at the ankles and reflexes are normal. The remainder of her exam is normal and stool was heme negative. Cardiometabolic stress test shows no symptoms or electrocardiogram changes to a heart rate of 161 (97% predicted maximum). VO2 max is 22.8 mL/kg/min (6.5 METs [metabolic equivalents]).
Initial laboratory testing is notable for the following:
Total cholesterol 287 mg/dL
Triglycerides 600 mg/dL
High-density lipoprotein (HDL) 34 mg/dL
Unable to calculate low-density lipoprotein (LDL)
Cholesterol/HDL ratio 8.44
Fasting glucose 96 mg/dL
Are there any other diagnostics that may be helpful in understanding and addressing her lipid profile? Do those results surprise you?
Additional information:
DEXA body composition: 31.5% fat (32.3% in the trunk) with 83.7 lbs fat-free mass
HgbA1c 5.4
Fasting insulin 11 µIU/mL
Insulin and glucose 1 hour post 75-g glucose challenge: 87 µIU/mL and 212 mg/dL
Insulin and glucose 2 hour post 75-g glucose challenge: 104 µIU/mL and 127 mg/dL
Cardio C-reactive protein (CRP) 0.7 mg/L
25-OH vitamin D 18 ng/mL (20-100)
Thyroid-stimulating hormone (TSH) 6.3 uIU/mL with normal free T4 and free T3; significantly elevated thyroperoxidase and thyroglobulin antibodies
Ferritin 26 ng/mL, transferrin saturation 25%
Helicobacter pylori antibody positive
What is the best way to approach her concerns about her cardiovascular risk from a lifestyle standpoint? Should she be started on lipid-lowering therapy?
Results and Discussion
SP meets criteria for metabolically unhealthy normal weight (MUH-NW), which is defined as a BMI <25 with 2 or more features of metabolic syndrome: blood pressure ≥130/85, fasting triglycerides ≥150 mg/dL, fasting glucose ≥100 mg/dL, and HDL ≤50 mg/dL (<40 mg/dL for men). 1 The prospective San Antonio Heart Study found the odds ratio for the development of diabetes over a mean of 7.4 years of follow-up in MUH-NW was 2.5, while the odds ratio for incident cardiovascular disease was 2.9. 2 Body fat in the upper third (>23.1% for men and >33.3% for women) with a BMI <25 strongly predicted risk of metabolic syndrome. 3 It is likely that improving fitness and improving body composition will yield greater reductions in cardiovascular risk than will weight loss in MUH-NW. 4 Because of SP’s expressed desire not to take medications, the presence of a potentially treatable contributor to her hyperlipidemia (subclinical hypothyroidism with high thyroid antibodies), 5 and her low cardio CRP and normal stress test, the initial approach was focused on normalizing her thyroid status, improving dietary quality, and modifying her exercise program. She met with a dietician with a focus on limiting/avoiding refined carbohydrates and added sugars in addition to increasing dietary fiber in the form of beans and lentils. An exercise physiologist worked with her to increase the number of days doing cardiovascular exercise, adding interval training with target heart ranges based on her cardiometabolic stress test results, increasing her total exercise time, and adding in resistance training twice weekly. She also met with a behavioral medicine specialist to learn relaxation and breathing techniques to address sleep and stress.
She was initially started on 0.025 mg levothyroxine with a plan to increase as tolerated to a target TSH between 1 and 2. She was given a 10-day course of lansoprazole, amoxicillin, and clarithromycin for eradication of H pylori in light of her reflux symptoms. 6 In addition to the dietary recommendations outlined above, she was also encouraged to increase dark leafy greens as an iron source and consider iron supplementation because of her symptoms of restless legs. 7 Vitamin D 50 000 IU weekly for 8 weeks was also given.
Her reflux symptoms resolved following treatment for H pylori, and her symptoms of restless legs were markedly better and no longer disrupting sleep. Over the next year she had gastroenterology follow-up for a further drop in ferritin: celiac testing, EGD (esophagogastroduodenoscopy), and colonoscopy were all normal. At her 1-year follow-up, her weight was down to 110 pounds and her body fat by caliper testing was 24%. Over the next 10 years she has maintained a weight between 110 and 112 pounds.
Table 1 illustrates the trend over time of her labs and her lipids. Although her triglycerides and VLDL-3 responded dramatically to her lifestyle changes and thyroid replacement, her LDL remained significantly elevated with an unfavorable ratio. The presence of an elevated Lp(a) 8 (lipoprotein-a) and LDL pattern B added to her risk. She was eventually started on ezetimibe/simvastatin with subsequent improvement in her lipids. Following an episode of chest pain, she was seen by a cardiologist and underwent repeat computed tomography angiography, which showed slight noncalcified plaque in the right coronary artery and left anterior descending artery. Twice she developed elevated transaminases when attempting to increase her dose of ezetimibe/simvastatin. She was subsequently changed to rosuvastatin and has stayed at a dose of 20 mg daily with excellent lipid results and normal transaminases. Through the years she has periodically reassessed her exercise routine and has continued to engage in aerobic exercise 5 days a week with strength training 2 to 3 days a week. She has experimented with a grain-free diet and adding in more olive oil and nuts9,10 but overall continues eating a whole foods, plant-based diet with some fish and shellfish, but no red meat or poultry. Ten years after her original presentation, her weight is 111 pounds with 26% fat by caliper testing. Her VO2 max is 35.89 mL/min/kg (10.5 METs), a 57% improvement from her original measurement.
Anthropometrics and Lab Results Over Time.
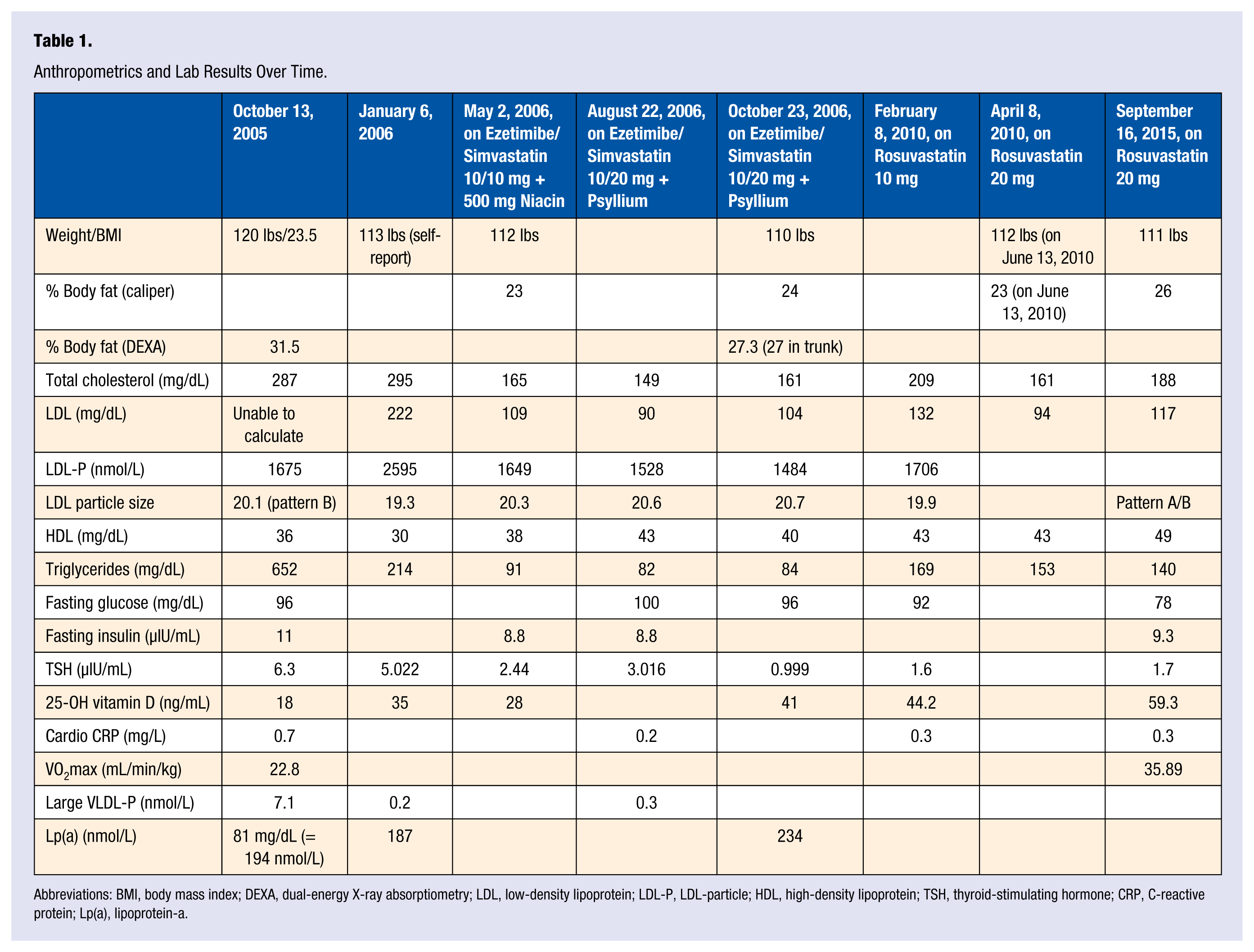
Abbreviations: BMI, body mass index; DEXA, dual-energy X-ray absorptiometry; LDL, low-density lipoprotein; LDL-P, LDL-particle; HDL, high-density lipoprotein; TSH, thyroid-stimulating hormone; CRP, C-reactive protein; Lp(a), lipoprotein-a.
Several meta-analyses have been done evaluating statins for primary prevention of cardiovascular disease in women, 11 including a recent one in this journal in 2015 12 after newer concerns emerged related to statins and risk of new-onset diabetes. 13 The conclusion was that statin use led to a trend toward reduction of cardiovascular morbidity and mortality in women at higher risk for cardiovascular disease, and the slight increased risk of diabetes was outweighed by the greater cardiovascular benefit. Statins combined with lifestyle changes have an additive effect in lowering risk.14-16 Unfortunately, data from NHANES III (National Health and Nutrition Examination Survey III) showed that in 2009 and 2010, statin users consumed an average of 9.6% more calories and 14.4% more fat than 10 years previously. 17 This dietary change was not seen in nonstatin users, suggesting an unintended “behavioral” effect of statins: if lipids are well-controlled with medication there may be less incentive to continue dietary efforts to impact cholesterol. Given the effects of dietary habits on insulin resistance, diabetes risk, inflammation, and endothelial function, it is critical for patients to understand the importance of food choices for cardiovascular risk reduction above and beyond their impact on blood lipids and weight.
The interplay between statin use and decreased exercise is more complicated.18,19 Independent of overt rhabdomyolysis or a behavioral effect as described above with diet, patients may decrease exercise because of myalgias and/or decreased exercise tolerance as a side effect of statins. Correction of vitamin D deficiency, 20 changing statin class, and alternate day dosing may mitigate some of the muscular side effects of statin therapy.21,22 A recent small study using a proprietary nutraceutical supplement containing red yeast rice, berberine, policosanol, folic acid, CoQ10, and astaxanthin in high-risk statin-intolerant patients found that 100% achieved their LDL target goals with minimal to no side effects. 23
Low fitness more than doubles the risk of cardiovascular disease in women and is linked to higher mortality than high fitness in women who have other cardiovascular risk factors (smoking, hypertension, and hyperlipidemia). 24 In men, for each 1 MET improvement in cardiovascular fitness, there was a 20% lower risk of coronary heart disease while controlling for their Framingham Risk Score. 25 Another study found that each MET of fitness achieved lowered risk of all-cause mortality and cardiovascular disease and mortality by 13% and 15%, respectively. 26 Unlike statin therapy, the benefits of exercise extend well beyond reduction in cardiovascular risk (see Figure 1). SJ’s increase of 4 METs in her cardiorespiratory fitness would translate to a 60% reduction in cardiovascular disease and mortality.
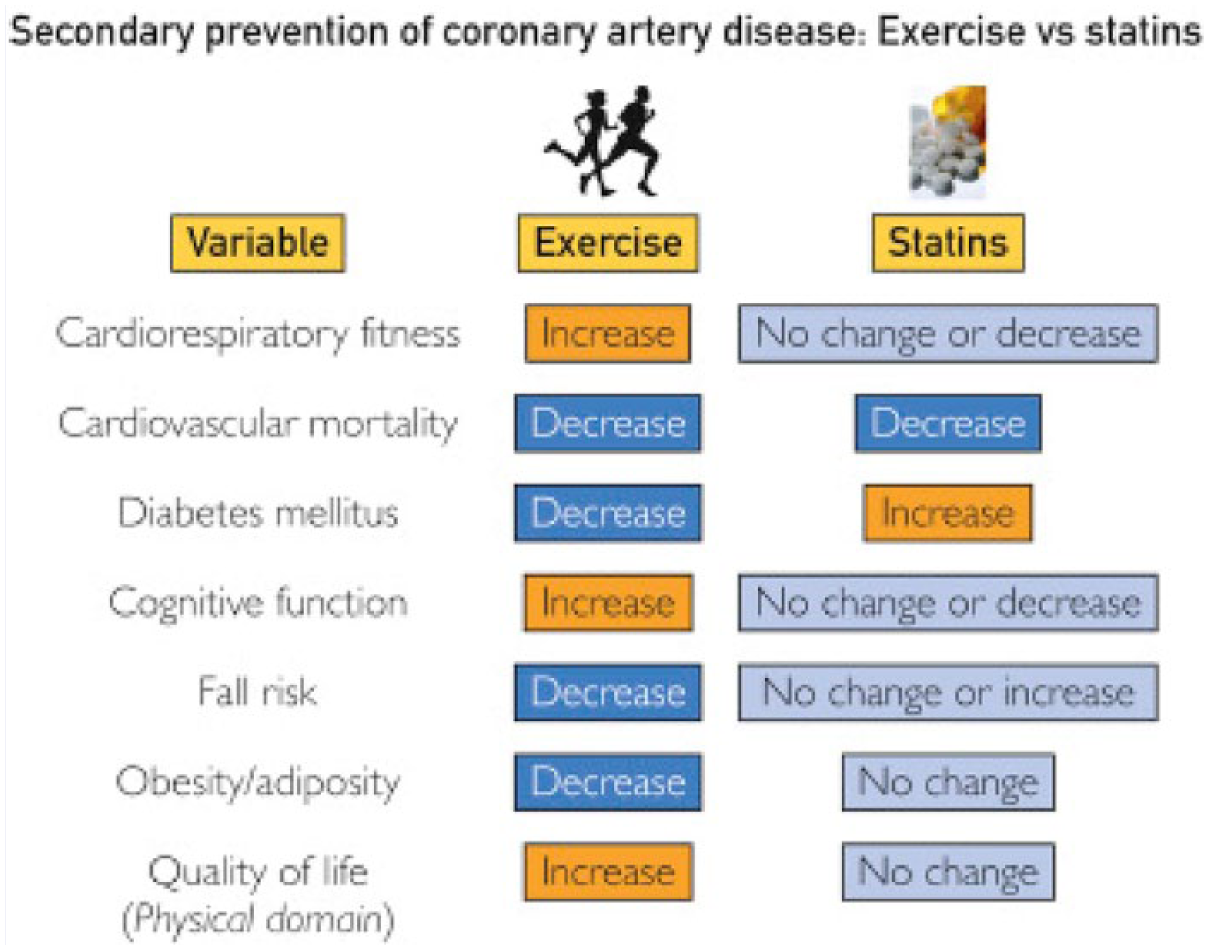
Comparison of the effects of exercise training and statins on varied risk factors and health outcome modulators in the prevention of initial and recurrent cardiovascular events. Although both regular exercise and statins appear to confer substantial reductions in cardiovascular mortality, there are numerous independent and additive benefits of exercise over statins when other variables are considered.
Conclusion
SJ’s weight and BMI did not predict her degree of dyslipidemia and insulin resistance. Her elevated waist-to-hip ratio and percent body fat near the upper third were more predictive. This underscores the importance of assessing body composition and metabolic markers of insulin resistance even in people with “normal” weight, given the increased risk of diabetes and cardiovascular disease in those with MUH-NW. Weight loss, correction of her hypothyroidism, improved dietary quality, and more vigorous exercise were not enough to reduce her lipids to a low-risk range, which resulted in the initiation of statin therapy with good results. However, one of the biggest contributors to her cardiovascular risk reduction was the significant improvement in her fitness level and body composition. Given the recent reports of increased calorie and fat intake in people prescribed statins, overall low numbers of people meeting minimum exercise guidelines at baseline, and the potential decrease in activity that may accompany statin use, it is all the more imperative for physicians and health care practitioners to look beyond cholesterol in the discussion with patients about lowering cardiovascular risk. Exercise and fitness; a fiber-dense, whole foods diet; and avoiding weight gain are particularly beneficial in lowering risk of diabetes and cardiovascular disease for patients with metabolically unhealthy normal weight.