
Abstract
Many health care providers are concerned with the role environmental exposures play in the development of respiratory disease. While most individuals understand that outdoor air quality is important to their health status, many are unaware of the detrimental effects indoor air pollution can potentially have on them. The Environmental Protection Agency (EPA) regulates both outdoor and indoor air quality. According to the EPA, indoor levels of pollutants may be up to 100 times higher than outdoor pollutant levels and have been ranked among the top 5 environmental risks to the public. There has been a strong correlation between air quality and health, which is why it is crucial to obtain a complete environmental exposure history from a patient. This article focuses on the effects indoor air quality has on the respiratory system. Specifically, this article will address secondhand smoke, radon, carbon monoxide, nitrogen dioxide, formaldehyde, house cleaning agents, indoor mold, animal dander, and dust mites. These are common agents that may lead to hazardous exposures among individuals living in the United States. It is important for health care providers to be educated on the potential risks of indoor air pollution and the effects it may have on patient outcomes. Health problems resulting from poor indoor air quality are not easily recognized and may affect a patient’s health years after the onset of exposure.
‘The relationship between health and air quality has been recognized as far back as Hippocrates.’
Clean environmental air is a basic right for all humans. The relationship between health and air quality has been recognized as far back as Hippocrates. Indoor air quality is particularly important to humans since we spend up to 90% of time indoors. 1 Outdoor and indoor air quality in the United States is regulated by the federal government through the Environmental Protection Agency (EPA). In this article, we will concentrate primarily on indoor quality and will highlight the sources of potential morbidity of indoor air quality as it pertains to lung health.
One of the most important tasks of the health care worker, meeting a patient for the first time, is to take a comprehensive history of environmental exposures both at work and in the home. The health care worker should ask the patient about contemporary exposures and also about exposures “in the home in which you grew up.” 2 Household factors that may affect respiratory health include home water damage, heating and ventilation, renovation work, cleaning product accidents, the presence of a pool or hot tub, and hobbies, including arts and crafts and model building. Also, activities such as do-it-yourself repair work, gardening, pet exposure, wood or coal exposure, and dirty clothes exposure are discussed.
Secondhand Smoke
The awareness of smoking and its adverse effects is as widespread today as at any point of time in history. Globally, smoking remains a highly prevalent lifestyle choice. Secondhand smoke exposure is a leading public health problem. Approximately 1 nonsmoker dies from secondhand smoke exposure for every 8 smokers who die from smoking. 3 Three publications serve as landmark summaries of the effects of environmental tobacco smoke (ETS) on human health. First, the US Surgeon General’s Report in 1986 4 and a report of the National Research Council 5 described the health risks associated with passive smoking. Last, the EPA released a report in 1992 that causally linked secondhand smoke exposure to lung cancer 6 effectively classifying ETS as a group A carcinogen. While secondhand smoke has been referred to as ETS in the past, the term secondhand smoke better captures the involuntary nature of the exposure. The 2006 US Surgeon General’s report uses the term involuntary smoke in the title because most nonsmokers do not want to breathe tobacco smoke. 7
Secondhand smoke is composed of a mixture of both a sidestream smoke, the smoke released from burning the end of a cigarette, and exhaled mainstream smoke, the smoke exhaled by the smoker. 8 During cigarette burning, there are more than 4000 chemical compounds created of which many are toxic and carcinogenic.9,10 The chemical composition (Table 1) of both sidestream and mainstream smoke is similar in the number of compounds they contain. However, the concentration and the physicochemical properties of these compounds can vary significantly. Sidestream smoke is 3 to 4 times more toxic than mainstream smoke. It tends to linger in the local indoor environment about 1.5 to 2 hours. With its composition of oils and waxes, it may increase both the exposure period and entry into lung tissue and body cells more easily. 11 Sidestream smoke composition does not vary significantly by tobacco product brand but it remains as much as 10 or more times toxic than mainstream smoke. 12 Individuals may be exposed to secondhand smoke in homes, cars, the workplace, public places, and recreational settings. In the United States, the source of most secondhand smoke is from cigarettes, followed by pipes, cigars, and other tobacco products.
Carcinogens and Suspected Carcinogens in Secondhand Cigarette Smoke.
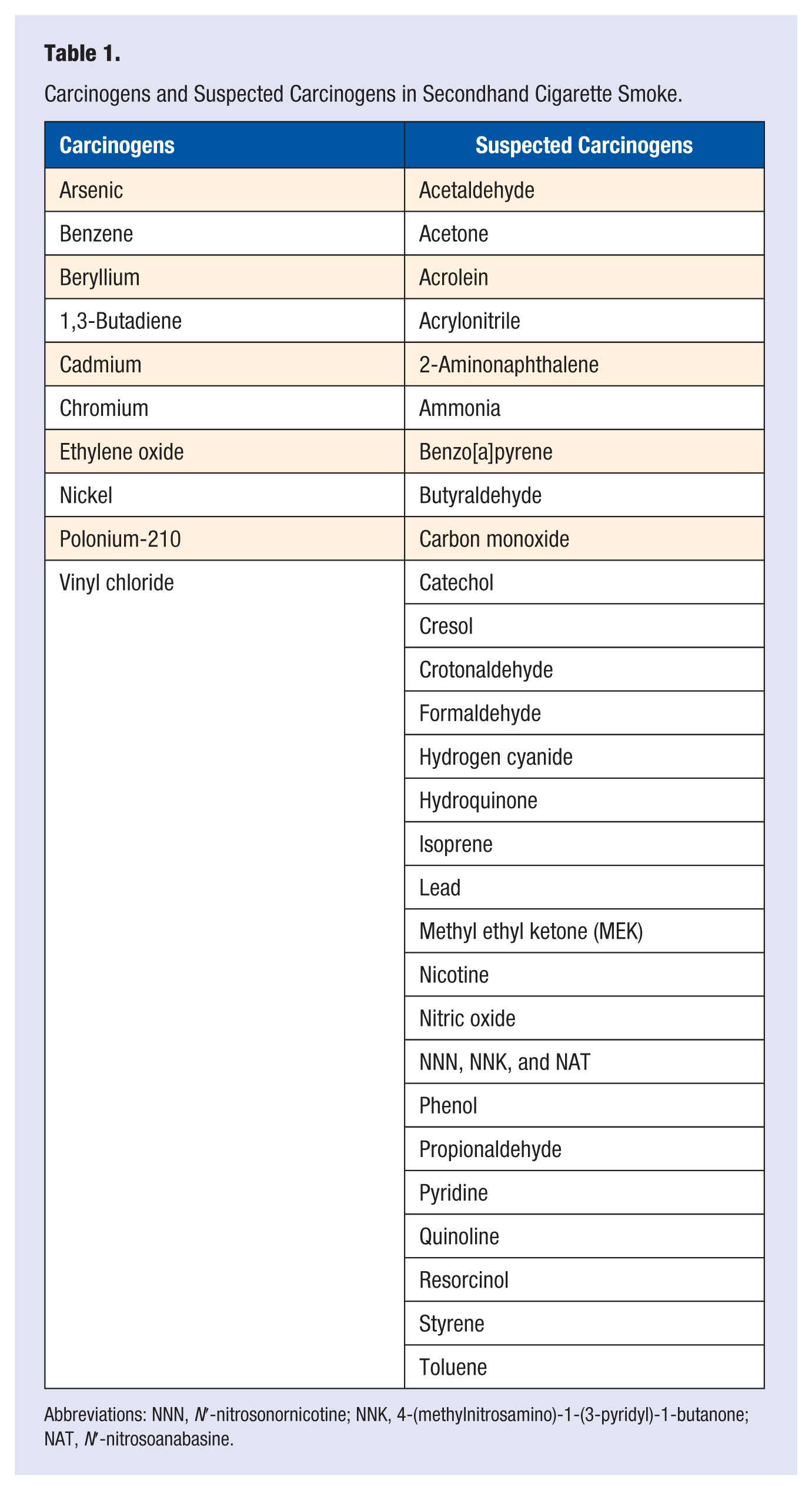
Abbreviations: NNN, N′-nitrosonornicotine; NNK, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone; NAT, N′-nitrosoanabasine.
The term thirdhand smoke has been referred to as cigarette byproducts that cling to smoker’s hair and clothing as well as to household fabrics, carpets, and surfaces even after secondhand smoke has cleared. 13 These invisible tobacco toxins pose danger to small children, who are especially susceptible when they come in contact with contaminated surfaces. 14
Secondhand smoke exposure can be measured by testing indoor environments for nicotine and other chemicals in tobacco smoke. It can also be tested by measuring the level of cotinine (a by-product of the breakdown of nicotine) in a nonsmoker’s blood, saliva, or urine. 15 Nicotine, cotinine, carbon monoxide, and other smoke-related chemicals have been found in the body fluids of nonsmokers exposed to secondhand smoke by way of passive personal sampling exposure devices. 16 The average exposure is directly related to room size and ventilation rate within that room.17,18 Older devices would take days to weeks to yield a result, but more modern devices can perform active sampling of the environment with more efficacy. These devices can measure nicotine and several other markers including carbon monoxide, nitrogen oxides, and polycyclic aromatic hydrocarbons.
Recent concerns of possible harm and toxicity have been raised about electronic cigarettes or e-cigarettes. While data are still being compiled on these devices, there has been a dramatic increase in the number of calls made to poison control with an average of 215 calls per month. The majority (51.1%) involved children younger than 5 years while 42% of poison calls were made for people older than 20 years. Some of the side effects reported include nausea, headache, seizures, pneumonia, and congestive heart failure. These devices are not approved by the Food and Drug Administration as smoking cessation devices. More research is needed to determine their safety.19,20
Carcinogens and Suspected Carcinogens Found in Secondhand Tobacco Smoke: Risks of Exposure to Secondhand Smoke
In June of 2002, the International Agency for Research on Cancer (IARC) concluded that “involuntary smoking, exposure to secondhand smoke or ‘environmental’ tobacco smoke, is carcinogenic to humans.” Furthermore, the IARC concluded that there is a “statistically significant and consistent association between lung cancer risk in spouses of smokers and exposure to secondhand tobacco smoke from their spouse who smokes. The excess risk is on the order of 20% for women and 30% for men.” 21
In January 2005, the US Public Health Service’s National Toxicology Program issued its 11th report on carcinogens. This report unambiguously states “environmental tobacco smoke is known to be a human carcinogen based on sufficient evidence of carcinogenicity from studies in humans that indicate a causal relationship between passive exposure to tobacco smoke and human lung cancer.” Some studies also support an association of environmental tobacco with cancers of the nasal sinus cavity, breast cancer, leukemia, lymphoma, and brain tumors in children.22-24 Evidence of an increased cancer risk from environmental tobacco smoke stems from studies examining nonsmoking spouses living with individuals who smoke cigarettes,25,26 exposures of nonsmokers to environmental tobacco smoke in occupational settings, and exposure to parents’ smoking during childhood.8,13 Many epidemiological studies, including large population-based case-control studies, demonstrate an increased risk of developing lung cancer following prolonged exposure to environmental tobacco smoke. Lifelong nonsmokers living with smokers had, on average, a 24% higher chance of developing lung cancer than those living with nonsmokers. Those exposed to the heaviest smokers for the longest time had the highest risks.27,28 Similarly, there is a growing body of evidence suggesting a higher risk of death from the association of secondhand smoke exposure and ischemic heart disease. Most of the data surround spousal smoke exposure and risk ratios that range between 20% and a 2-fold excess risk of cardiac death in this population.29-32 There may be a confounding effect in these studies, as there may be an innate risk in the US population to develop cardiovascular disease. In addition, there are pathophysiologic changes due to secondhand smoke that have not been fully elucidated. It is known that the elevation in serum carboxyhemoglobin levels decreases exercise tolerance in both healthy and individuals with ischemic heart disease. 32 Also, “time until angina” decreases with increasing concentrations of serum carboxyhemoglobin 33 as does the frequency of arrhythmias during exercise, 34 vascular endothelium damage, 32 lower high-density cholesterol levels, and increase in fibrinogen with associated fibrinogenesis. 33
Secondhand Smoke Exposure in Children
The Pro-Children Act of 1994 prohibits smoking in facilities that routinely provide federally funded services to children. Many state and local governments have passed laws prohibiting smoking in public facilities, such as schools, hospitals, airports, bus terminals, parks and beaches, as well as private workplaces, including restaurants and bars. There is no doubt that the impact caused by secondhand smoke exposure raises the frequency and severity of respiratory illnesses and respiratory symptoms in children. In a 1993 report, the EPA estimated between 150 000 and 300 000 annual cases of bronchitis and pneumonia in children could be attributed to secondhand smoke in the United States. Of these, between 7000 and 15 000 will result in hospitalization. Secondhand smoke was also estimated to increase the rate of asthma exacerbations with between 200 000 and 1 000 000 affected children. 4 In addition, secondhand smoke exposure increases the risk of sudden infant death syndrome (SIDS), and one survey found the risk of SIDS to be up to 3-fold higher in children exposed to active maternal smoking in utero and secondhand smoke exposure after birth. 35 Apart from the obvious medical implications, the economic burden associated with this increase in morbidity is responsible for a rise in health care costs likely to be in the millions if not, billions of dollars. A recent study in Germany attempted to quantify this effect finding a near doubling in health care cost between nonsmoker parents and children exposed to secondhand smoke. 36
Radon
Radon-222 is a noble gas that is produced from the decay of uranium-238 and radium-226, these are naturally present in the earth’s rock and soil. It decays with a half-life of 3.8 days. It can diffuse itself into the soil and air before decaying. The breakdown of radon-222 by emission of an alpha particle, which produces radioactive progeny that include polonium-218 and polonium-214.37,38 These are known as the “short-lived” progeny and they, in turn, break down into “long-lived” progeny that include lead-210, which yields bismuth-210, which yields the stable isotopes polonium-210 and lead-206. This whole decay process takes hundreds of years. When inhaled into the lung, the alpha-particles can damage cellular DNA and lead to mutagenesis. 39
Radon gas can seep into buildings through porous soil. The rate of diffusion is related to the pressure gradient created by the building structure across the soil, which in turn, is influenced by atmospheric pressure, wind flow over the structure, and the buoyancy of the air taking advantage of cracks or gaps in building foundations, floors, walls, and along with gaps along pipes, pumps, and drains. It can easily dissolve into and evaporate out of water. Therefore, water drawn from private wells in areas enriched with uranium can increase the exposure to radon. Inhaled radon poses a much higher risk to lung cancer than ingested forms.40,41
Inhaled radon progeny have been linked to increase the risk of lung cancer in underground miners. 37 These progeny are the number one cause of lung cancer in never smokers and the second leading cause of lung cancer overall. The EPA estimates that radon exposure may account for over 20 000 lung cancer deaths each year, including 2900 never-smokers, and the remaining deaths in smokers with radon exposure at concentrations as low as 2 pCi/L of air. 42 It is difficult to ascertain the exact amount, length, and degree of exposure needed to cause lung cancer. Most studies causally link the exposure of uranium and underground miners. A meta-analysis of 13 European case-control studies of uranium exposure showed an increased risk of lung cancer, to smokers and recent former smokers, and accounted for 2% of all cancer deaths in Europe, although it is difficult to accurately estimate the lifetime exposure to radon in these settings. 38
The EPA recommends testing of radon in homes and schools below the third floor since toxic effects have not been reported in high-rise dwellings. A “do-it-yourself” kit can be left in place for 48 to 72 hours in the bottommost floor and first floor rooms without fans, open windows or doors. Long-term or 90 day trackers give a better estimate of year-round radon exposure. They may be used when short-term devices yield a value higher than 4 pCi/L. If levels higher than 4 pCi/L are detected, interventions that range from sealing gaps or cracks in the foundation to installing a new ventilation or radon mitigation system that will ventilate air to the outside environment require a professional contractor.
Carbon Monoxide
Carbon monoxide (CO), the byproduct of the combustion of carbonaceous fuels, is a colorless, odorless gas. Sources of CO include unvented kerosene heaters, gas space heaters, leaking chimneys, furnaces, gas water heaters, wood stoves, generators and other gas powered equipment, automobile exhaust, and tobacco smoke.24,39,43-45 Approximately 15 000 emergency department visits and 500 accidental deaths in the United States are attributed to accidental exposure to CO inhalation.46,47 Mortality rates are highest among adults older than 65 years, men, non-Hispanic whites and non-Hispanic blacks. January has the highest number of averaged deaths, and in the United States, Nebraska has the highest mortality whereas California has the lowest mortality. Interestingly, weather patterns of recent years have brought about large storms that may increase the risk of CO exposure; Hurricane Sandy in 2012 was associated with a marked spike in the number of cases in the New York City area. 48 CO binds with a high affinity for hemoglobin, 200 times greater than oxygen, forming carboxyhemoglobin (COHb), which disrupts oxygen transport. Additionally, CO or COHb binds to heme proteins in myoglobin and cytochrome oxidase.49,50 Tissues with the highest oxygen demands, including myocardium, brain, and exercising muscle are first affected. The effects of CO are directly related to the level and duration of exposure. Initial symptoms include headache, fatigue, shortness of breath, nausea, dizziness, and tachycardia. At higher concentrations, worsening cognitive impairment, loss of muscle coordination, coma and death are possible. Symptom progression illustrated in Table 2. Reductions in maximal oxygen consumption occur in normal, young men with COHb levels near 5%. 51 Individuals with ischemic heart disease have a shorter interval to the onset of angina at COHb levels ranging from 2% to 6%.52,53 For this reason, subjects with cardiovascular disease are considered to be at high risk of morbidity with CO exposure. 54 A clear distinction should be made between angina and onset of cardiovascular disease as related to carbon monoxide exposure. A link between morbidity and mortality has been shown with moderate to severe CO exposures resulting in myocardial injury. The correlation between low-level CO exposure and heart disease has not been made presumably because of inaccurate measures of personal exposure in previous studies.55,56
Symptoms associated with carboxyhemoglobin exposure.
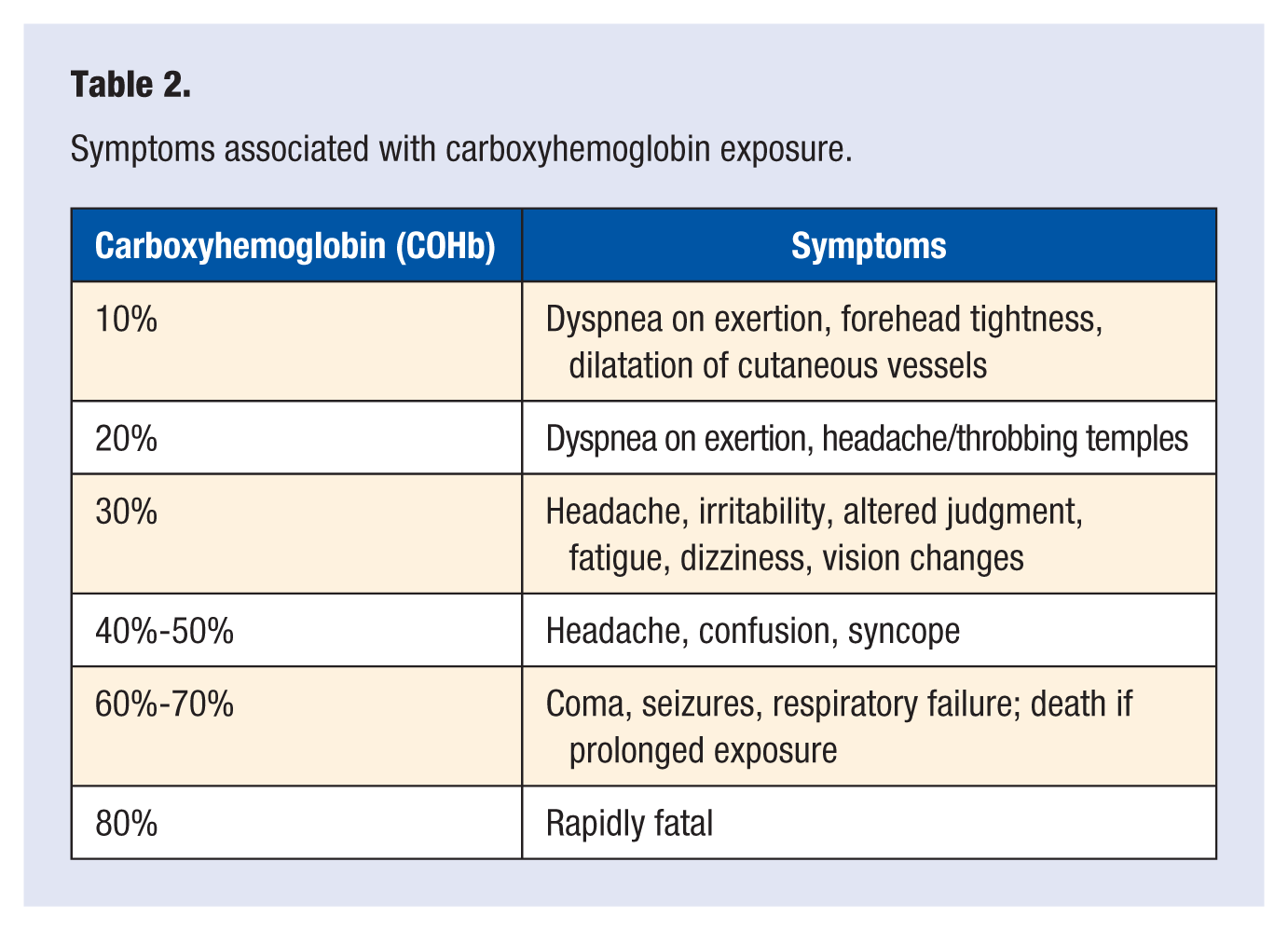
The average level of CO in homes without gas stoves is generally low at 0.5 to 5 parts per million (ppm). Levels near properly adjusted gas stoves vary between 5 and 15 ppm, but in poorly adjusted stoves, these levels can rise as high as 30 ppm or higher. At CO levels of 70 ppm, symptoms become more noticeable and at levels greater than 150 to 200 ppm disorientation, unconsciousness, and death may occur (Table 2).
CO levels can be monitored at home with a commercially available detector. The Consumer Product Safety Commission (CPSC) recommends that a detector be located near the home sleeping area to alert sleeping household members in the event of elevated CO levels. They should not be directly above or beside burning appliances, as appliances may emit a small amount of CO on start-up. A detector should not be placed within 15 feet of heating or cooking appliances or near very humid areas such as bathrooms. 24
Nitrogen Dioxide
Nitrogen dioxide (NO2) belongs to a group of air pollutants from combustion processes where nitrogen is oxidized. Outdoor sources of NO2 are most commonly from automobile emissions, and in home sources include gas-fueled appliances such as gas cooking stoves and kerosene space heaters. Approximately 60% of the residences in the United States have gas-fueled heating appliances, and about 40% are estimated to have a gas powered stove range. 57 During the winter, indoor concentrations of NO2 can be as much as twice the outdoor levels. Some of the highest levels have been measured in small city apartments and residences that use ovens for space heating. Nitrogen dioxide may exacerbate symptoms for individuals with respiratory illnesses because most of the inhaled gas is deposited in large and small airways with little deposition in the alveoli. Nitrogen dioxide’s high degree of tissue solubility allows it to interact with the alveolar epithelium, the interstitium and the alveolar capillaries. Oxidant injury occurs secondary to the formation of nitric and nitrous acids. Also, there is some evidence that NO2 may impair mucociliary clearance in the lung. In high concentrations, it can lead to fatal pulmonary edema and pneumonia while lower concentrations are mainly associated with bronchitis, bronchiolitis, and pneumonia. The physiologic effects of NO2 on pulmonary function include a reduction in the forced expiratory volume in 1 second (FEV1) and increased airway resistance (Raw).58,59 In addition, NO2 is capable of inducing activation of prostanoids, leukotrienes, and histamine leading to increased airway inflammation. 24 These effects are seen mostly in asthmatics. Although there is conflicting evidence, there is a general consensus that extended exposure and high levels can affect respiratory physiology negatively by increasing the incidence of asthma in children.60,61
The acceptable level of exposure for NO2 varies widely between different governmental agencies and private organizations, but the EPA has set a 53 parts per billion (ppb) highest allowable limit. Adequate installation of all gas appliances and wood stoves with tight-fitting connections, proper fuel, ventilation and maintenance are important to reduce exposure. 24
Formaldehyde
Formaldehyde is a colorless, flammable gas at room temperature. It has a pungent, distinct odor and may cause a burning sensation to the eyes, nose, and lungs at high concentrations. Formaldehyde is an indoor pollutant that is commonly found in wood building materials and more specifically in resins that bind together wood products such as plywood, fiberboard and particle board. Formaldehyde is also found in plastics, textiles, carpet, furniture, pesticides, paint glue, and cleaning products. It can reach higher concentrations in smaller homes because of the relatively large ratio of pressed wood products to air volume. 62 Several studies have found an association with formaldehyde exposure in plywood workers and respiratory symptoms, which include cough, sputum production, asthma, colds and chronic bronchitis.63-65 The role of formaldehyde in human cancer has not been elucidated however, the IARC has determined that it is possibly carcinogenic based on limited evidence in humans and sufficient evidence in animals. 66 Some of this evidence points to nasopharyngeal cancer.67,68 On July 2010, the Formaldehyde Standards for Composite Wood Products Act was signed by President Obama. 69 In addition to the Occupational Safety and Health Administration (OSHA) guidelines, these standards are intended to reduce the exposure to composite wood products and to use air conditioning and dehumidifiers to maintain temperature and reduce humidity thereby limiting human exposure.
Household Cleaning and Cooking
Household cleaning is estimated to occupy approximately 30 minutes daily of an average adult life. Cleaning agents are designed to reduce the burden of viruses, bacteria, mold, toxins, and allergens to name a few; but these products may also contribute to indoor pollution and health problems. When using household cleaning products a survey, which included 27 countries in the European Union, showed a majority of those surveyed declared little to no attention to safety labels. 70 Accidents involving inhalation of toxic fumes resulting in significant respiratory morbidity are well documented and most involve the improper mixing of agents. Women are at a higher risk of exposure than men possibly because they perform more household cleaning.71-73 It is also worth noting that over the past 2 decades, there has been a steady increase in the exposure to volatile organic compounds (VOCs) such as limonene, linalool, citronellol, eucalyptol, geraniol, and α-pinene found in cleaning products. 74 These compounds add fragrance to everyday products, some products have more than 2600 ingredients. 75 Currently, neither US manufacturers of consumer products nor the owners of chemical formulations are required to disclose all ingredients and one reason is to protect trade secrets. 74 A study published in 2007 evaluated use of home cleaning agents and their association with asthma. In this study that included 10 European countries, 3503 persons who cleaned their homes and were free of asthma were followed on average 9 years. The results showed 42%of participants, who cleaned at least once weekly, experienced asthma symptoms or were using asthma medications and wheezing. The association was linked to the most commonly used glass cleaner, air freshener, and furniture cleaning sprays and was not related to atopy. The investigators surmised that use of household cleaning sprays may be an important factor in the development of asthma in adults. 76
Other cleaning products, including household bleach, consist of a 5.25% sodium hypochlorite solution (NaOCl) when mixed with an acid such as either 4% phosphoric acid (a rust, mineral deposit, water stain remover), household ammonia (NH3), or hydrochloric acid (HCl), chlorine gas and water are released. 24 Chlorine gas and hydrochloric acid exposure can lead to a myriad of upper and lower respiratory tract injuries, which include mucous membrane irritation, chest pain, cough, shortness of breath, pneumomediastinum, bronchospasm, pulmonary edema, and reactive airways disease.77-80 A case report of a healthy 53-year-old woman illustrates the dramatic effect of combining ammonia and household bleach who developed pneumonitis and acute respiratory failure requiring life support. 81 Inhalational injuries can also be seen with oven cleaners that contain sodium hydroxide, monoethanolamine (MEA), diethylene glycol monobutyl ether, and butane or isobutene when sprayed onto hot surfaces. Reported injuries include chemical pneumonitis, asthma-like symptoms, and bronchiolitis obliterans organizing pneumonia (BOOP).24,82
Approximately 3 billion people use solid fuels and rudimentary stoves to cook and heat their households. 83 This chronic exposure to indoor air pollution from this biomass fuel has led to health concerns, including development of chronic obstructive pulmonary disease (COPD) and lung cancer. Cooking accidents with overheated oil fumes and recent studies have suggested a possible risk secondary to inhalation of toxic by-products, including polycyclic aromatic hydrocarbons (PAH).24,84 A Norwegian study showed a high concentration of PAH while frying on gas stoves; however, these concentrations were found to be within normal limits. 24 In addition, there is no evidence that brief exposure to cooking fumes affects pulmonary function testing in healthy or asthmatic subject.85,86 However, in developing countries worldwide, chronic exposure to indoor biomass and fumes from cooking has been shown to be a leading cause of COPD, especially in women. These patients tend to have less emphysema and more bronchial involvement leading to greater effects on quality of life and mortality. It is thought that interventions to reduce exposure to cooking fumes and biomass can reduce the risk, but more data on longitudinal outcomes is needed. 83 The risk of lung cancer is of concern in patients chronically exposed to cooking fumes from oil based products. Studies in Chinese women and a recent review of American household that consisted of Chinese immigrants and restaurant workers have suggested a causal association with an increased risk of lung cancer.87,88 Based on these results, the IARC has classified exposure to high temperature frying as probably carcinogenic to humans. 89
Indoor Mold
Mold is ubiquitous in the outside environment, and plays an important role in breaking down organic matter such as trees and leaves. The abundance of mold in the outside environment allows for easy transportation into the indoor environment including homes, schools, and businesses where they can raise concerns for long-term adverse health effects and worsening of preexisting lung disease. Approximately 100 molds have been identified to be potentially harmful to human health, although only a few are commonly found in indoor environments. The molds most commonly found in the indoor environment include Cladosporium, Alternaria, Epicoccum, Fusarium, Penicillium, Geotrichum, Rhodotorula, Chaetomium, and Aspergillus. 90
Molds are organisms with rigid cell walls that are a subset of the diverse group of organisms that lack chlorophyll and vascular tissue called fungi. Mold, like others in the kingdom Fungi, live on organic matter such as decaying plants and living animal tissue. They have the capability to digest materials deemed unusable by other organisms, which allows mold to grow on home materials such as carpeting, drywall, ceiling tiles, and building materials made from organic matter. Molds do not produce leaves and reproduce by germination of small particles called spores. Spores are not readily seen by the naked eye and range in size from 2 to 20 µm in diameter and up to 100 mm in length with characteristic microscopic shapes sizes and colors. Molds need a moisture-rich environment with an average humidity of greater than 65%, a temperature of 50°F to 90°F and an organic substrate such as wood on which reproduce and germinate. Once germination occurs, spores can grow, aerosolize, and be inhaled or come in contact by humans in the environment. This was seen in the aftermath of hurricanes Katrina and Rita 91 where many homes had to be demolished due to excessive mold growth.
A small subset of molds in the indoor environment is known to induce an immunoglobulin mediated antibody response in humans. 92 Molds produce antigens, which are substances known to cause allergic reactions, by either contact or direct inhalation. Illness brought on by molds can be classified into 2 types, infectious or noninfectious. Noninfectious causes include allergic bronchopulmonary aspergillosis (ABPA), hypersensitivity pneumonitis and worsening of preexisting asthma. Infectious causes are less common and very rarely cause disease in immunocompetent individuals. The most common infectious cause is seen with the mold of the Aspergillus genus. Inhalation may result in pulmonary infection and formation of a fungus ball called an Aspergilloma. In severe cases of aspergillus infection, invasion of the lung and blood vessels may result in severe invasive Aspergillus and may be seen in immunocompromised hosts who are HIV positive, post–organ transplantation, receiving chemotherapy or other immunosuppressive drugs.
The most common symptoms of excessive indoor mold exposure include nonasthmatic cough, wheezing, headache, and sneezing. This can be exacerbated by energy efficient homes, so-called tight homes, with closed ventilation systems with high indoor temperatures and humidity. 24
Fungal sensitization and exposure appears to play an important role in the development of lower respiratory tract disease. 93 A study done with severe asthmatics and fungal sensitization (SAFS) showed a 60% improvement in asthma quality of life scores after treatment with the antifungal medication itraconazole. This suggests that controlling the mold burden may play a significant role in reducing the severity of asthma.94,95 However, the American Thoracic society does not recommend antifungal therapy for fungal sensitivity from causes not related to underlying ABPA. 96 A 2008 study also estimated that up to 21% of asthma cases in the United States may be due to excessive exposure to mold and damp living conditions. 97
The keys to preventing the potential harmful effects of mold exposure include both identification of areas infected and removal of both the mold and moisture-rich environment. Mold growth is readily identified in areas of prior water damage or constant high humidity. The mold can be detected by both visual identification and by the pungent odors it produces from the breakdown of organic matter into volatile organic compounds such as aldehydes and ketones. 98 Mold can be successfully removed from hard nonporous surfaces with the use of a simple detergent and water, and then allowing for complete drying of the area. Porous areas, including ceiling tiles and carpets, should be disposed of as the mold cannot be eliminated with cleaning alone. 98 Areas with dead mold may cause significant health effects and must also be removed. Mold removal will not be complete until the moisture source that is required for growth is eliminated.
Animal Dander
Animal dander is most commonly associated with allergens from the dead skin cells of animals such as cats, dogs, and other furred pets. Cats and dogs seem to have the greatest risk of causing sensitization and the potential for causing health issues. Many epidemiologic studies have shown that sensitization to dog and cat allergens are strongly associated with asthma. 99 Cats are well known to induce sensitization by a protein Fel d1, which is found in the saliva and salivary glands. This protein is approximately 2.5 µm in diameter and is easily inhaled deep into the lower respiratory tract.100-102 Because of its small size, up to 1 µg of the Fel d1 protein may be inhaled per day, which is similar to the amount used in sublingual immunotherapy. 103 Even homes without cats can have high concentrations of up to 80 µg of Fel d1 per 1 g of dust.104,105 Current evidence suggests that early exposure to animal dander in childhood reduces the likelihood of sensitization and subsequent development of asthma from both cats and dogs. It is important to tell patients that completely nonallergenic animals do not exist, but there are some breeds that are thought to be less allergenic. 106 Certain dog breeds are promoted as hypoallergenic breeds, such as the Labradoodle, Poodle, Spanish Waterdog, and Airedale terrier.107,108 Recent studies were performed comparing the amount of Can r1 and r2, an antigen released by dogs, found that these proteins were significantly higher in breeds promoted as hypoallergenic.107,109 The amount of protein was nearly double in these “hypoallergenic” breeds as compared to ones classified as allergenic. Reducing exposure to animal dander may be accomplished by using HEPA (high-efficiency particulate air) filters, frequent bathing, or by removing the animal from the environment altogether.
Dust Mites
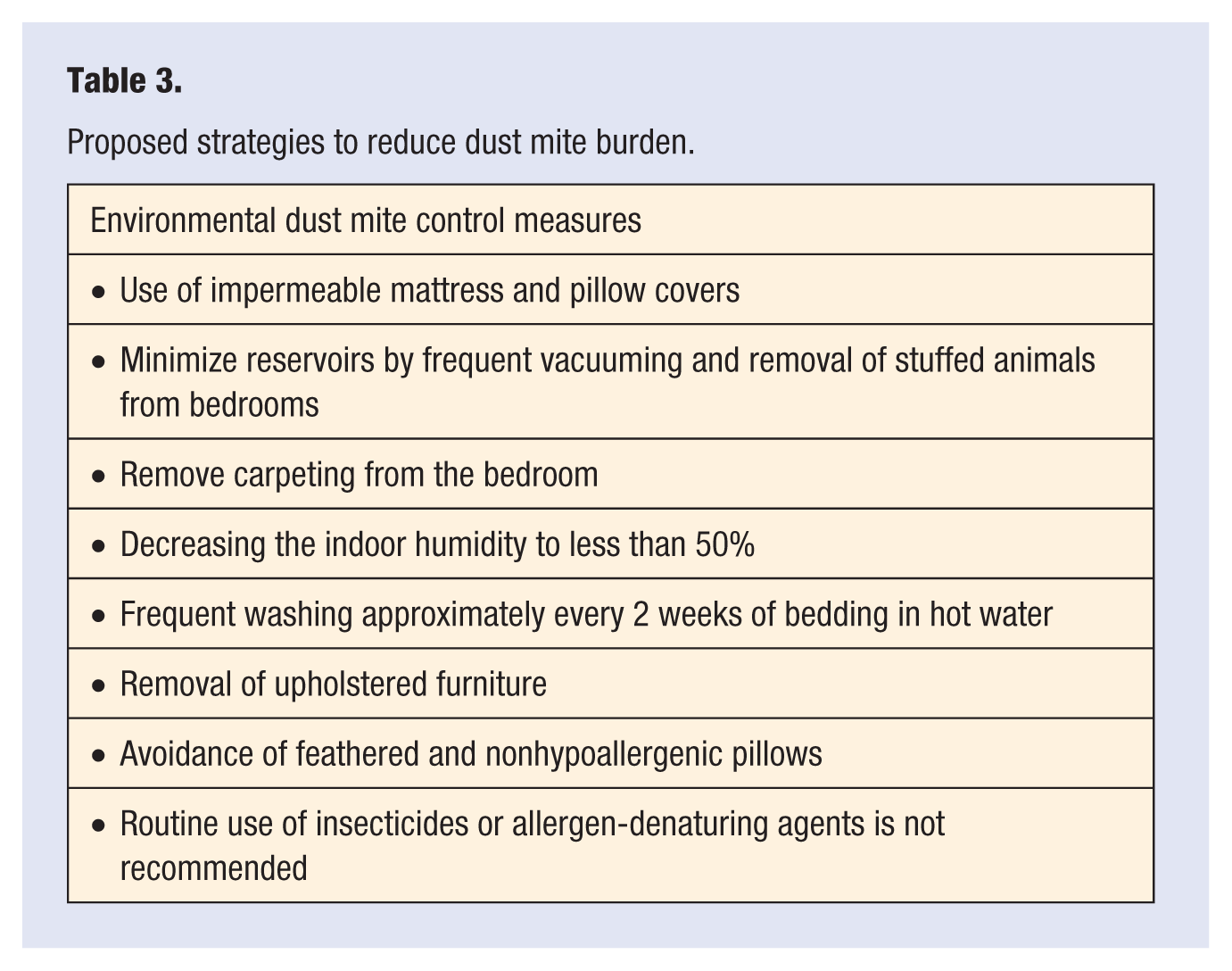
Dust mites, Dermatophagoides pteronyssinus and Dermatophagoides farinae, are arthropods from the class Arachnida that colonize bedding sofas, carpets, and any other woven material within the home. Dust mites are the most common allergen worldwide. They are found infrequently at high altitude, in arid conditions, and in areas exposed to long cold winters due to low humidity. Aside from causing allergic disease, dust mites do not pose any other risk to human health. Mites, and the debris they produce, are microscopic, absorb moisture from the environment and feed on dead animal and human skin cells. It is not the mite itself, but its fecal particles, that result in a strong allergic response in up to 26% of Americans. 110 Dust mite particles are large and heavy and when dispersed from their source only remain aerosolized for up to 15 minutes then settle very quickly. 111 This makes air purifiers such as HEPA filters ineffective with dust mite antigen removal. Although dust mites are found frequently in carpets and upholstered furniture, the most common sources are bed mattresses. Dust mite allergens can worsen preexisting asthma, but are not known to directly cause it. Table 3 contains control measures that can reduce dust mite allergen burden.
Proposed strategies to reduce dust mite burden.
Cockroaches
Cockroaches are a common occurrence in the urban environment, and play an important role in indoor air quality and development of asthma in the inner city. While there are more than 3500 different species known, the most common species are the German species Blatella germanica and American species Periplaneta americana. Antigenic particles Bla g1 and Bla g2, similar to dust mites are found in the fecal particles as well as their secretions. 112 High levels of cockroach infestations are seen with living in densely populated areas, urban environments, inner-city communities, and low socioeconomic status. 113 Conditions that favor cockroach infestation include: food left uncovered, humid and warm conditions, poor sanitation, and crowding. 114 Inner-city children sensitized to cockroach antigen in high levels (>8 U/g) were more likely to develop asthma, have higher asthma morbidity, more office visits and hospitalizations due to asthma. 115 A recent study by Turyk et al 116 showed similar findings in inner-city children in a low-income neighborhood in Chicago.
Several techniques have been recommended to reduce cockroach antigen exposure, and include controlling humidity, improving indoor sanitation, and both chemical and nonchemical extermination. 114 Although a difficult task, simple measures such as improved sanitation, reducing overcrowding may have a significant impact on reducing the severity and development of asthma in inner-city children. 117
Mice
Mice and the allergens they release, pose a significant health risk in both urban and rural indoor air quality. Mus m 1 and Mus m 2 are the major allergens found in mice dander, hair, and urine. 118 These allergens are more commonly found in inner-city urban environments and highest in rooms where food products are stored, including the cafeteria or kitchen. Mice allergens were found in 95% of homes in large study of inner-city children with asthma. 119 The greatest predictor of high levels of mice allergen exposure was the presence of visible droppings. 120 The impact of these allergens was noted by Sheehan et al 121 where children, with preexisting asthma, in homes with high levels of mouse allergen had more missed school days due asthma related events. Exposure to mouse allergen is associated with high rates of sensitization. Children sensitized to mouse allergen were found to have increased risk of developing asthma and have higher rates of asthma-related morbidity. 122 Homes with every 10-fold increase in mouse allergen were shown to have an 87% increase in use of asthma related health care in urban children with asthma. 123
Overall, mice contributed a significant impact on the lung heath of the people exposed and sensitized to their allergen. The most effective way to limit their impact is to prevent or reduce the chance of exposure. The use of rodent-proof construction, improved sanitation, and population control using traps and chemicals may also reduce exposure.
Water Pipe Smoking, Also Known as “Hookah”
Water pipe smoking is becoming an increasing trend among young adults aged 18 to 24 years as a “safe” alternative to smoking. It is also known by other names, including shisha and narghile. The concept is not a new one, with reports of its use dating back to the 15th century in both the Middle East and Europe. 124 Because of recent laws limiting the use of tobacco products within public buildings and restaurants, hookah bars have opened up, most within the past 10 years. 124 Hookah bars are small cafés and clubs that rent the use of hookahs and sell special hookah. These bars have been directly marketed to young adults aged 18 to 24 years, with most of them residing near universities and college campuses. One study found that in 1 in 5 boys and 1 in 6 girls aged 18 years had used water pipe tobacco in the past year. 125 Further smaller studies in college students show its use to be as high as 40%. 125
Smoking is done through directly heating the tobacco with items such as burning embers or charcoal. The smoke is then filtered through a water medium that is sometimes flavored with artificial flavorings such as apple or watermelon. The smoke is then drawn through a pipe to a mouthpiece to be inhaled. When combined with other flavors, it is called shisha. 124
Although limited research has been done on the health risks of water pipe use, the existing evidence indicates that water pipe smoking carries the same or similar health risks as cigarette smoking. Links have been made to many of the same adverse health effects, including lung, oral, and bladder cancer, as well as coronary artery and heart disease.126,127 Despite knowing the risks, almost 90% of beginning hookah smokers thought that cigarette smoking was more addictive. 128 Trends suggest that its use is increasing worldwide. Analysis of mainstream smoke from water pipes found that it contains significant amounts of nicotine, tar, and heavy metals.128,129 Analysis of nicotine and cotinine, a chemical marker of nicotine exposure, before and after water pipe use revealed that nicotine levels increased up to 250% and cotinine levels to 120% with just one session of use lasting 40 minutes. 129 Because water pipe smoking has a more prolonged inhalation time and exposure than a conventional cigarette, it has been estimated that one session can be equivalent to smoking 100 cigarettes within that time. 129 These results may be complicated by the routine concurrent use of cigarettes.
Other risks are also seen with use of the heat sources that are used to light the tobacco such as wood or charcoal. These substances when ignited alone put one at risk for exposure to smoke that contains heavy metals and carbon monoxide. These compounds are known to cause cancer and obstructive lung disease more commonly in developing countries that use fire to cook. There is also a concern for transmission of infectious diseases such as tuberculosis, hepatitis, and herpes, although this had not been extensively studied. 127
Continued research is needed to determine the absolute long-term health risks with water pipe smoking. The current evidence supports that both direct exposure and secondhand exposure are similar to that of cigarette smoking and does not support its use as a “safe” alternative. 125
Conclusion
This article has identified key elements of indoor quality that significantly affect the health of individuals in the United States. We have attempted to target areas of significance to health care practitioners as well as educated professionals. During this process, we have emphasized the relationship between indoor air quality and health as it pertains to exposure to the many different agents described in this review. There are many different hazardous agents that can potentially affect persons from secondhand smoke and cleaning agents to the family pet, many individuals remain unaware of the potential detrimental effects associated with these exposures. Lung health is important to both young and old alike and so it becomes crucial to target environmental exposures that may increase the risk for health problems, including asthma, allergic reactions, lung cancer, and in a small but significant fraction, accidental death. The federal government through various agencies continues to monitor and provide guidelines, reports, and recommended testing for many of these agents. However, simple interventions that can promote health, including not allowing smoking indoors; checking radon levels; reducing conditions that promote mold growth, dust mites, and animal dander; monitoring carbon monoxide levels; and using chemical products with care are but a few interventions that can easily improve overall quality of life. More research is needed to cope with the growing number of new pollutants and their possible side effects, better define the effects of volatile organic compounds, and the effect of poor indoor air quality on health care cost. Certainly, life-long awareness, elimination of potential indoor environmental hazards, and increased awareness within health care providers and professional are essential to promote long-term lung health and well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.