
Abstract
With life expectancy increasing and the symptomatology of HIV being altered since the advent of antiretroviral therapy (ART), we now have begun to see metabolic changes with negative implications among people living with HIV/AIDS (PLWHA). Some of these changes include increased blood lipids, central fat accumulation, lipodystrophy, and decreased aerobic capacity. All of which are known risk factors for cardiovascular disease, cancer, and all-cause mortality. A common practice among healthy and other clinical populations to help modify these risk factors is some form of aerobic exercise, resistance exercise, or a combination of both. It has been demonstrated that PLWHA could respond in a similar manner, which in turn may enhance life expectancy and/or quality of life. The purpose of this literature review was to examine the evidence of health benefits of routine exercise training among PLWHA since the advent of ART. Although limited in strength because of small sample sizes and limited intervention durations, there is overall consistency in the general findings. An overview of the findings would indicate that physical activity and exercise are both safe and effective in improving cardiorespiratory fitness, metabolic profile, and quality of life among PLWHA.
‘The use of exercise training to reduce the risk of chronic disease is supported within the literature and could potentially have similar health benefits among HIV-infected persons.’
Although advances in the treatment of HIV and AIDS have reduced the number of AIDS-related cases and deaths worldwide, new cases of reported HIV infections have remained relatively stable, resulting in a continued increase in overall prevalence. Approximately 40 000 new infections are reported every year in the United States alone. 1 Since the discovery of antiretroviral therapy (ART) medications, we have also observed drastic changes in the pathophysiology of HIV disease and symptomatology of infection. People living with HIV/AIDS (PLWHA) no longer exhibit high rates of muscle wasting or AIDS-related opportunistic infections. 2 Now the symptomatology has transgressed into just the opposite. With the success of ART, life expectancy of PLWHA has nearly tripled from the onset of new diagnoses. As a result we have begun to observe PLWHA well into their adult lives for multiple decades. Because of the toxic side effects of ART medications and the long-term consequences of viral infection, PLWHA have begun to show increased rates of metabolic abnormalities, including lipodystrophy, increased circulating blood lipids, and increased fat accumulation in the abdominal region.
People living with HIV/AIDS have a variety of psychological and physiological symptoms associated with the virus itself, the related medications, or a combination of both. Because of the nature of concurrent symptoms being experienced at frequent rates, the general well-being and overall quality of life are often reduced.3,4 Furthermore, the frequency of reported symptoms is associated with increased disease progression, decreased functional capacity, reduced adherence to pharmacological treatment, self-medication, increased psychological distress, as well as anxiety and depression.5 -11 Recent data indicate that the primary cause of death among PLWHA are chronic diseases generally associated with aging such as cardiovascular disease (CVD) and kidney failure, among others. 12
There are multiple factors present that one must consider as potential contributors of this increased risk of chronic disease, most of which are metabolic in nature. For example, now that the population demographics have shifted into minority and lower socioeconomic classes, we have seen a growing population of PLWHA who already have personal and environmental factors predisposing them to high visceral fat mass and obesity. 13 These would include poor diet, inactive/sedentary lifestyle, chronic stress, and negative lifestyle choices. Other factors include the low cost of energy-dense food with large amounts of sugars and fats. As a result many patients are beginning ART treatment with a higher body mass index (BMI) and fat mass. 14 In addition, it is commonly known that the side effects of most ART combinations include lipodystrophy and increased blood lipid accumulation. 15
The use of exercise training to reduce the risk of chronic disease is supported within the literature and could potentially have similar health benefits among HIV-infected persons. The benefits of aerobic and resistance exercise have been established among general populations and various clinical groups from longitudinal investigations such as the Aerobics Center Longitudinal Study16 -18 and the Framingham Heart study (among others).19 -21 Although shorter in duration, a number of studies indicate that PLWHA can obtain similar benefits within 6 weeks following a prescribed physical activity intervention.22,23 The purpose of this state of the art review is to examine the literature and better understand the health benefits of aerobic, resistance, and combined aerobic/resistance training among PLWHA and its effects on immune status.
Methods
The methods used for this review included a search of relevant journal articles using a combination of major electronic databases (ie, PubMed, Medline, and Google Scholar). Specific keywords (or combinations of) used in the search included the following: HIV, exercise, aerobic, resistance, and training. Combinations of keywords included HIV and exercise OR aerobic training OR resistance training; HIV and aerobic resistance training OR aerobic resistance exercise. Since the symptomatology of HIV/AIDS infection has changed since the advent of ART we chose to only include studies published since the year 2000. Additionally, since new medications could possibly hinder or alter the effects of exercise training any study that introduced new medications to any of the subjects at the time of the research investigation were excluded as well.
Using the keywords stated previously with a custom date range of 2000-2013, a total of 96 articles were identified. Out of those identified 40 were not reviewed because the purpose of the investigation was not exercise related, leaving us with 56 relevant articles for the purpose of this literature review. Of those 56 articles, 32 were excluded leaving a total of 24 included in this review. Reasons for excluding studies included the following inclusion of people younger than 18 years, not a randomized controlled trial, introduction of new medications, and nonexercise related. For a complete list of the studies please refer to Tables 1 and 2.
Exercise-Based Clinical Trials Since the Development of Antiretroviral Therapy: Physiological and Psychological Changes.
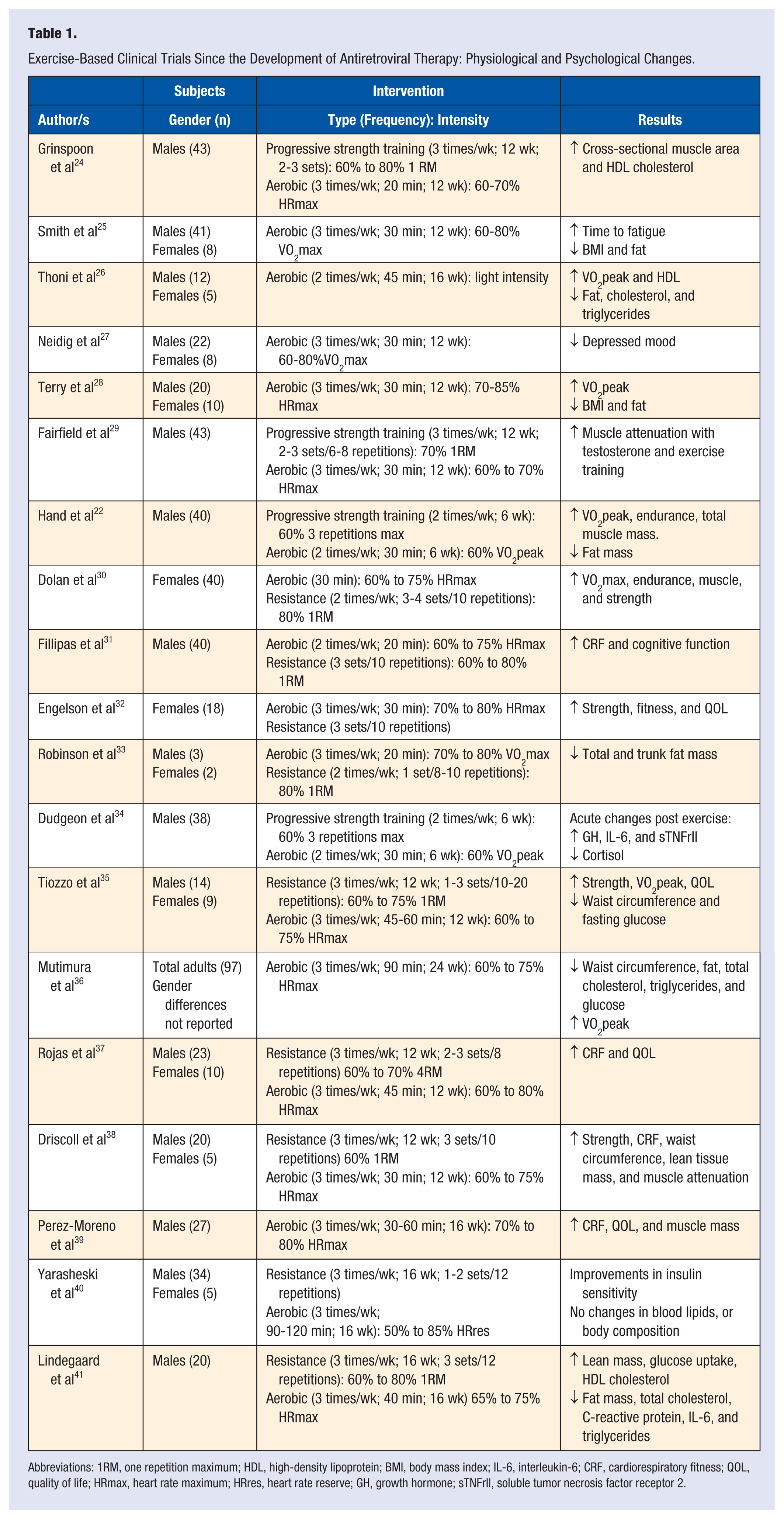
Abbreviations: 1RM, one repetition maximum; HDL, high-density lipoprotein; BMI, body mass index; IL-6, interleukin-6; CRF, cardiorespiratory fitness; QOL, quality of life; HRmax, heart rate maximum; HRres, heart rate reserve; GH, growth hormone; sTNFrII, soluble tumor necrosis factor receptor 2.
Exercise-Based Clinical Trials Since the Development of Antiretroviral Therapy: Immunological Changes.
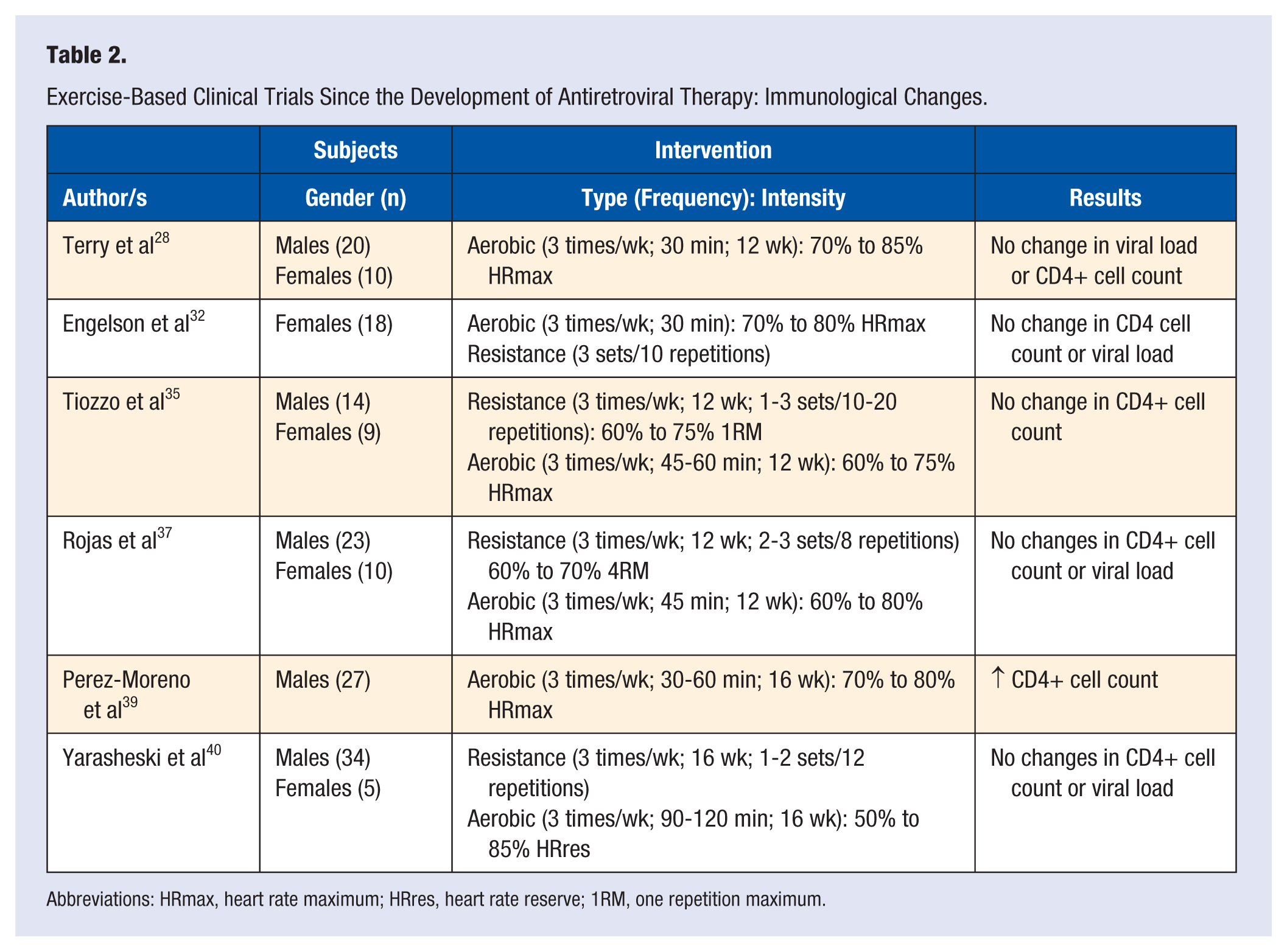
Abbreviations: HRmax, heart rate maximum; HRres, heart rate reserve; 1RM, one repetition maximum.
Physiological Improvements With Exercise
Studies have consistently shown physiological improvements across clinical measurements of health such as BMI, waist circumference, blood lipids, muscular strength, and cardiorespiratory fitness (CRF) among others. A 24-week aerobic exercise intervention using 2 levels of intensity (medium or high) found that both intensities yielded significant improvements in CRF and reduced perceived stress. The medium-intensity group exercised 3 times a week at 50% to 60% of their VO2max for 40 minutes, and the high-intensity group exercise 3 times a week at 75% to 85% of their VO2max for 24 minutes. A major limitation to that study, however, was a high attrition rate of 76%, which was possibly due to the long duration and/or intensity of the study. 42 In a similar clinical trial, participants were randomized into either a high- or moderate-intensity aerobic exercise group and exercised for a total of 30 minutes, 3 days a week for 12 weeks. Findings showed similar significant improvements in CRF in both groups. 43
Interventions consisting exclusively of low-intensity aerobic exercise, but with a longer duration of 16 weeks, have also shown significant improvements among CRF and serum high-density lipoprotein cholesterol among PLWHA when compared with a control group. Findings have also indicated significant decreases in total abdominal adipose tissue, total cholesterol, and circulating triglycerides. 26 Similar results have been reported by other researchers who have found significant increases in CRF, oxygen pulse, and maximum tidal volume.31,39,44,45 In addition, aerobic exercise has demonstrated decreases in BMI, waist-to-hip ratio, and body fat after a 12 week moderate-intensity intervention.43,46 The reported findings would, thus, indicate that PLWHA are able to elicit significant health improvements when following a prescribed exercise routine lasting 12 weeks or longer. These effects have been observed with various combinations of the exercise intensity, participant disease status, and/or current antiretroviral treatment.*
In addition to the findings on physiological variables, no significant changes in CD4+ cell count have been reported in high- or moderate-intensity exercise groups.26,42,48 Furthermore, there have been no significant changes from baseline reported in CD8+ cell count, leukocytes, or lymphocytes following moderate- or high- intensity exercise. 28 Recently, it was shown that patients with dyslipidemia and lipodystrophy had no significant changes in immunological variables after completing 12 weeks or moderate-intensity aerobic exercise as well. 28 Notably, there are no published reports of exercise-induced immunosuppression in PLWHA who participated in physical activity regimens designed to reduce the psychological or physiological symptomatology associated with HIV.
Psychological Improvements With Exercise
In the era of widespread use of ART, there has only been one investigation using aerobic exercise as the primary intervention for HIV-associated depressive symptoms. Like those investigations previously discussed, reductions in depressive symptoms and/or significant improvements in quality of life were shown. 27 Findings from this study suggest that 60 minutes of moderate intensity (60% to 80% VO2peak) aerobic exercise conducted 3 days a week can be used as a beneficial method for improving the psychological disturbances experienced by PLWHA.
Early investigations conducted prior to widespread use of ART compared the effects of aerobic exercise on psychological components, such as depression and anxiety. Eight weeks of moderate-intensity aerobic exercise completed twice weekly for 60 minutes have shown significant reductions in anxiety and depression. 49 Other investigators reported significant improvements after only 5 weeks of aerobic exercise. Men who exercised for 45 minutes a day, 3 days a week, reduced anxiety and depression on learning of their seropositive status.45,50 As these investigations were performed before ART, the results are limited to symptoms specific to viral progression and not treatment. Furthermore, the majority of study demographics also consisted of middle-class heterosexual males. Because of the shift in patient demographics and treatments, these findings lack generalizability with today’s predominantly impoverished minority seropositive populations. It is unknown whether or not the virus, or any ART medications, would inhibit specific exercise-induced psychological improvements that are observed among other clinical and healthy populations.
Effects of Exercise on Immunological Variables
Research has also looked at the effects of exercise on immunological variables in the HIV-infection population (see Table 2). In addition to their findings on physiological and psychological variables, Engelson et al 32 reported no significant changes in CD4+ cell count or viral load. A small number of other studies have reported similar results showing no effect on immunological measured variables regardless of exercise intensity. This would include no reports of adverse events on health or immune status resulting from exercise training. For a list of these studies and a description of the intervention please refer to Table 2.
When looking at the studies published since the advent of ART only 1 study has shown positive changes in CD4+ cell count among PLWHA following a moderate-intensity exercise program. Perez-Moreno et al 39 reported that following combination aerobic and resistance training, completed at a moderate-intensity, increased CD4 cell counts and that this form of exercise can be completed safely by PLWHA. The authors went on to conclude that this improvement in CD4+ cells generally enhances resistance to infection by activating various immune cell populations. However, this particular study has several limitations making it difficult to compare with other HIV-related exercise studies. For example, their participant population consisted of previously incarcerated inmates currently enrolled in methadone treatment for opioid addiction. Another major limitation is that only 2 of their participants were currently on a stable ART regimen so it would be expected for them to have unstable CD4+ cell counts and viral load.
The study by Tiozzo et al 35 is the most recent one to report CD4+ cell count before and after an exercise intervention. In their study, they showed a significant decrease of CD4+ cells in the control group, with no change reported in the exercise group. Considering all participants in both groups were currently on a stable ART regimen, these findings would suggest that there is potentially an added benefit to maintaining a stable CD4+ cell count when engaging in routine moderate-intensity while taking ART. However, one must assume that the control group was either sedentary or highly inactive. With limited evidence to confirm this finding it is suggested that future investigations look into the relationship between physical inactivity and immune cell response. Because of the lack of research and inconsistency between findings further research on the topic of exercise and immune function among PLWHA is warranted.
Although there is a lack of strong evidence suggesting a beneficial effect of exercise training on immune function in PLWHA, it is important to note that any short-term exercise performed at low, moderate, or even high intensities does not have any effect on disease progression or immune function in this population. No study to date has shown an exercise-induced reduction in immune cell count or function at any exercise intensity when looking specifically at an HIV-infected population.
Exercise as an Alternative Form of Treatment to ART-Related Toxicities
In populations with a broad range of chronic diseases, there is a growing body of evidence showing that health benefits can be obtained by incorporating structured aerobic and resistance exercise into an individual’s recovery and/or treatment plan. For those stricken with conditions such as HIV, cancer, and type 2 diabetes, aerobic combined with resistance exercises can have positive effects in alleviating symptoms associated with the diseases and side effects of the medical interventions. Only in the past few years has there been an association established between HIV and increased risk of chronic diseases such as CVD and diabetes.15,51,52 As a result, there is limited evidence to make a definitive statement as to whether or not exercise is a beneficial alternative to pharmacological therapy for decreasing the risk of CVD among PLWHA. Although limited, the data that are available suggest that even modest amounts of routine exercise can yield both psychological and physiological health improvements that are known to reduce the risk of CVD within the general population. Table 1 provides of list of studies completed after the implementation of ART indicating the form of exercise training and its effects among PLWHA.
Strength of Evidence
Although there are a limited number of investigations with minimal sample sizes, results have been fairly consistent with regard to the anticipated adaptations one would expect to observe within the general population free from disease. From the current state of the literature, there is no reason to think that PLWHA would not show similar improvements in overall health and risk reduction, even while receiving ART.
Cardiorespiratory Fitness (VO2peak)
Most of exercise-related interventions measure CRF as common practice prior to any low- or moderate-intensity intervention. As a result, there are substantial data consistently showing both functional aerobic impairment (FAI) and training adaptations that increase CRF in as little as 6 weeks. † FAI is defined as a peak VO2 less than 25% of one’s age-predicted VO2peak. This aerobic impairment results in a reduced CRF level, which is known to be a significant indicator of various chronic conditions and all-cause mortality.18,54 -58 Even before the introduction of ART, a common consistency among exercise interventions has been significant FAI. Whether this is due to lifestyle factors or disease-related pathologies is not well understood. In a previous investigation from our lab we have demonstrated significant improvements in VO2peak and reductions in submaximal heart rate.22,37 Hand et al 22 show evidence of these findings, which suggest that PLWHA can reverse any indications of FAI, even when meeting less than half of the Surgeon General’s recommendations of 150 minutes per week. This study also demonstrated that there were additional cardiovascular adaptations such as a reduced resting heart rate and a reduced heart rate at submaximal workloads, which is a cardiovascular adaptation known as training bradycardia. These findings have also been in agreement with others.26 -28,30 -32
Blood Lipids
Another variable of interest with regard to CVD risk is the blood lipid panel. Although not as strong as CRF, evidence suggests a potential effect regarding improvements in blood lipids following routine exercise. Thoni et al 26 and Grinspoon et al 24 both showed increases in high-density lipoprotein cholesterol following light- to moderate-intensity aerobic exercise. Thoni et al also reported decreases in cholesterol and triglycerides. However there is still limited evidence to draw any formative conclusions regarding blood lipids and exercise training. One of the common side effects of ART includes increased blood lipids and fat deposits. Future studies should look into the long-term protective effects exercise may have with regard to normalizing blood lipids panels for PLWHA taking ART.
Body Composition
As stated previously, an increase in central fat accumulation is a common side effect of various ART regimens. Additionally it is well known that an increased waist circumference is a strong indicator of CVD risk. Multiple investigations have reported significant improvements in body composition by decreasing fat mass, waist circumference, and/or body mass index, as well as increasing lean tissue mass (see Table 1). More recently, Dudgeon et al 59 confirmed these findings by showing significant decreases in trunk fat, and total fat while also increasing lean tissue mass following a 6-week combination aerobic and resistance training intervention. Although still limited by the small sample sizes, this evidence appears strong enough to confirm that similar benefits in body composition (specifically fat mass and lean tissue mass) can be obtained by PLWHA that is commonly observed among general populations.
Immune System
With regard to immune function and inflammatory markers, there have been consistent findings showing no effect of exercise training at any intensity level. Only one investigation reported an increase in CD4+ cell count following a 16-week aerobic intervention 39 ; however, no one has confirmed this in other investigations. What the evidence does strongly suggest is that aerobic and/or resistance training at any intensity neither helps nor hinders immune function or viral load for PLWHA.
Recommendations for Exercise
Current exercise training recommendations as described in ACSM’s Exercise Management for Persons With Chronic Disease and Disabilities (third edition) for PLWHA suggest a moderate-intensity aerobic and resistance training regimen. 60 This includes accumulating a total of 150 minutes of moderate-intensity physical activity a week, as well as 2 days of full body resistance training at approximately 60% of one repetition maximum. Regardless of disease status, it is strongly recommended that anyone living with HIV or AIDS receive medical clearance from their primary health care provider prior to beginning an exercise program. Even though the majority of PLWHA have a reduced aerobic capacity, most of the standard physical fitness tests are applicable to this population and can be completed with little or no risk to the individual. Table 3 outlines potential HIV-associated changes that may be observed during exercise testing and/or training according to disease state.
HIV-Associated Changes to Exercise Testing a .
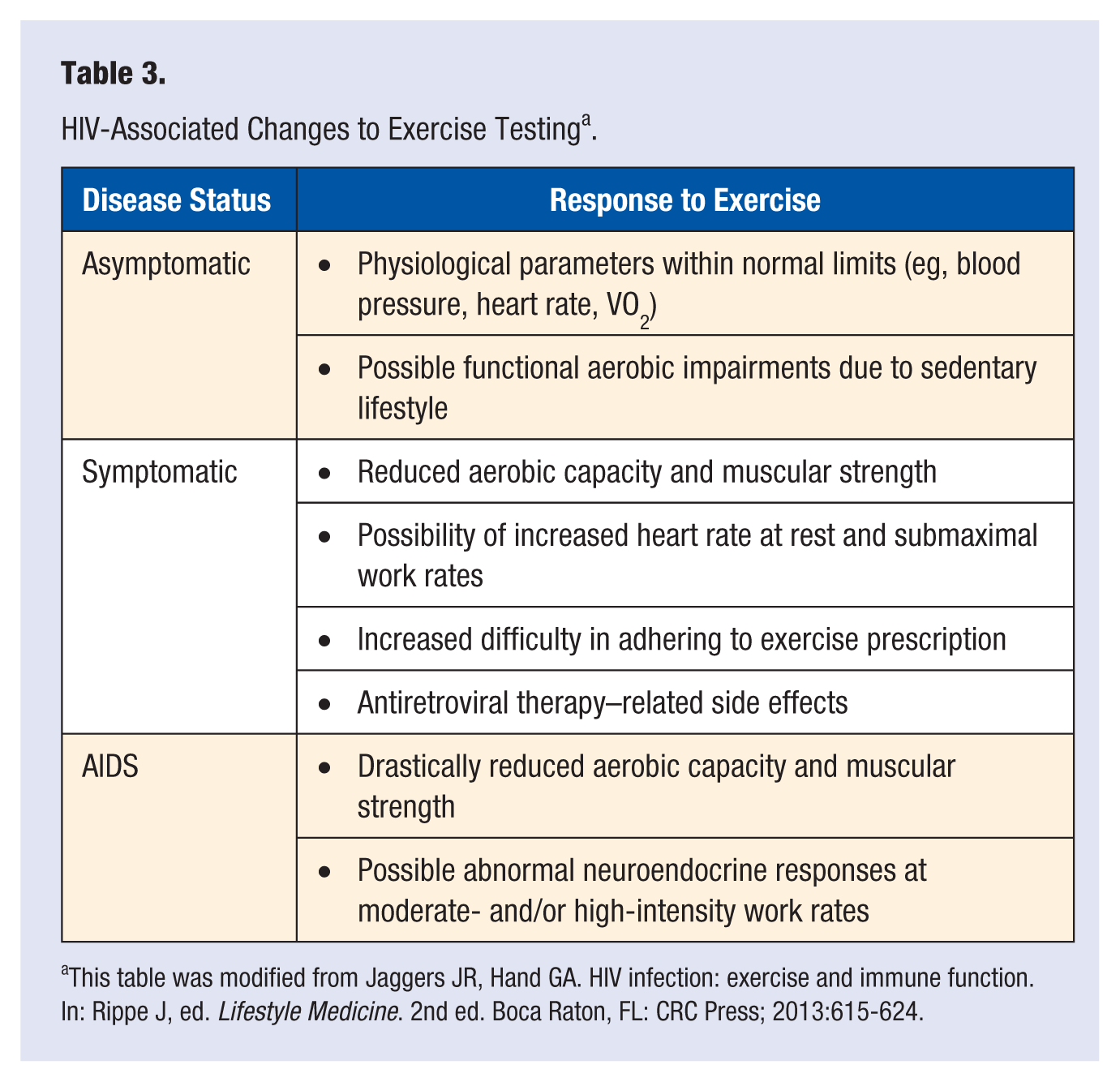
This table was modified from Jaggers JR, Hand GA. HIV infection: exercise and immune function. In: Rippe J, ed. Lifestyle Medicine. 2nd ed. Boca Raton, FL: CRC Press; 2013:615-624.
Conclusion
Evidence would suggest that PLWHA, regardless of disease status, can obtain similar short-term health benefits from routine physical activity reported within general populations. Research has shown significant improvements following moderate levels of routine exercise in as little as 6 weeks. It is also clear that across various populations routine moderate-intensity physical activity reduces the risk of chronic disease and that many of these conditions have been established as major causes of morbidity and mortality among PLWHA.
With regard to immunity, research among PLWHA has demonstrated that aerobic exercise performed at low-, moderate-, or high-intensity does not negatively impact immune function or disease progression at any stage of HIV infection. ‡ This clearly shows that aerobic exercise can be both safe and beneficial for this clinical population. However, it is recommended that if aerobic exercise is to be performed by this population, that they do so at a low- or moderate-intensity level as data are lacking to draw the conclusion that a high-intensity aerobic regimen will not have a negative impact on overall health or quality of life in this population.
Responses and adaptations to exercise training will vary depending on current fitness level, disease status and whether or not that patient is currently on an ART regimen. Asymptomatic individuals generally respond in a manner similar to someone without HIV of the same body size, age, and gender. However, some may be more deconditioned because of psychological disturbances commonly associated with daily sedentary behavior such as depression or anxiety, among others. Further, individuals with symptomatic status will generally be on a current ART regimen which also puts them at an increased risk of CVD. Therefore, extra caution should be taken prior to beginning an exercise prescription.
Although exercise itself is not going to eliminate the burdens of health care costs, social stigmatization, or other daily stressors, it could potentially reduce the health consequences of chronic stress, improve quality of life, and possibly increase the reduced life span of PLWHA. Most of the negative side effects from both the virus itself and treatment-related toxicities, including impaired glucose tolerance, fatigue, increased blood lipid profile, chronic inflammation, anxiety, depression, circulating cortisol, and others, are known to improve with routine exercise in various populations. Additional evidence from longitudinal studies have clearly shown that modest increases in CRF can decrease the risk of all-cause mortality as well as the risk of most chronic diseases. Whether or not PLWHA would have a similar response to long-term exercise is unknown because of insufficient research. Furthermore, there are no reported exercise-related interventions lasting longer than 6 months, making it impossible to determine the long-term effects on overall health and life longevity. However, benefits observed in a short time frame as reported by multiple investigations would suggest long-term gains in the physical and psychological well-being of PLWHA who participate in routine physical activity.
Footnotes
Acknowledgements
The work from our laboratory discussed in this article was supported by the National Center on Minority Health and Health Disparities (1-P20-MD001770-030003) and the National Institute or Nursing Research (1-R21-NR011281).