
Abstract
Few randomized controlled trials of family-based psychosocial interventions involving patients and at least one other family member have been conducted in the context of advanced cancer. Moreover, existing interventions have largely been stand-alone programs that have not been well integrated into routine palliative and clinical care. Programs that address this gap may not only improve patient and caregiver quality of life (QOL) but also the quality of palliative and supportive care services. The aim of this narrative review is to describe published interventions that have attempted to improve the QOL of advanced cancer patients and their family caregivers (eg, spouses, partners, and other family members) and to describe some of the challenges that make it difficult to implement such programs in clinical settings. Toward that end, the added value that family-based psychosocial interventions can bring to advanced cancer care is first described. Next, the literature on family-based interventions in advanced cancer is reviewed, and different theoretical approaches and outcomes are highlighted. This is followed by a description of some of the health system barriers to supportive family care in advanced cancer care. The article concludes with a synthesis of research findings and proposes directions for future research.
‘Strengthening relationships with loved ones has also been identified by patients to be among the most important facets of end-of-life care.’
Introduction
Quality of life (QOL) is a broad, multifaceted construct that encompasses the physical, emotional, social, and spiritual aspects of an individual’s life.1,2 A small body of literature suggests that advanced cancer patients experience unique QOL challenges that differ from patients who have early-stage disease.3,4 For example, advanced cancer patients endure persistent and sometimes severe physical and psychological symptoms, including pain, fatigue, anxiety and depression, shortness of breath, anorexia, insomnia, and constipation.5,6 Left unaddressed, these symptoms contribute to functional disability and adversely affect all aspects of QOL. They also can adversely affect the QOL of patients’ family members who are key providers of caregiving and emotional support. 7
Family members are under extreme stress and are profoundly affected by their loved one’s disease in addition to the changes in roles, responsibilities, and lifestyle that accompany it.8,9 For example, family caregivers (usually the patient’s spouse, partner, or other close family member) must figure out how patient care and assistance with daily activities will be provided, negotiate difficult choices regarding end-of-life treatment and care, and cope with anticipatory grief.10-13 These stressors can severely impair the ability of family members to fulfill their caregiving role as well as their relationship with the patient, which is the basis for caregiving. Indeed, the quality of spousal and family relationships has been shown to be important in terms of both patient and caregiver adjustment to advanced cancer.14-16 Strengthening relationships with loved ones has also been identified by patients to be among the most important facets of end-of-life care. 17
Palliative care seeks to decrease pain and suffering for patients with serious, advanced illness. It focuses on preventing and relieving physical, emotional, and spiritual distress; facilitating effective communication about treatment preferences and care goals; and easing transitions of care. 18 According to the World Health Organization, palliative care should not only improve QOL for patients but also for their families. 19 Although support for the family is deeply rooted within the core of palliative care philosophy, 20 the reality is that the support that is provided is often suboptimal. 21 To truly be family centered, there is a need to go beyond the traditional family meetings used in palliative care to communicate and support patients’ families, to addressing family caregiver distress, family communication, and relationship functioning. 22 Despite the fact that there is a growing literature on family-based interventions involving the patient and at least one other family member, usually the patient’s primary caregiver, 23 few randomized controlled trials (RCTs) have been conducted in the context of advanced cancer. Moreover, existing interventions have largely been stand-alone programs that have not been well integrated into routine palliative and clinical care. 21 Programs that address this gap may not only improve patient and caregiver QOL but also the quality of palliative and supportive care services that are offered to advanced cancer patients and their families.24,25
The purpose of this narrative review is to describe published family-based interventions that have attempted to improve the QOL of advanced cancer patients and their caregivers and to describe some of the challenges that may make it difficult to implement such programs in palliative care and clinical settings. Toward that end, this article first describes the potential added value that family-based interventions can bring to advanced cancer care. Next, the literature on family-based psychosocial interventions in advanced cancer is reviewed, and different theoretical approaches and outcomes are highlighted. This is followed by a description of some of the health system barriers to supportive family care in advanced cancer. The article concludes with a synthesis of research findings and proposes directions for future research.
What Can Family-Based Psychosocial Interventions Add to Advanced Cancer Care?
In cancer, the vast majority of psychosocial interventions have either focused exclusively on the patient26-28 or on the patient’s caregiver, who is most often the patient’s spouse, significant other, or another close family member.29,30 Family-based interventions that target patients and caregivers (as opposed to patients or caregivers alone) are beneficial for a number of reasons. First, treating patients and caregivers together can stimulate communication about difficult topics (eg, existential issues, legacy, fears about the future, and wishes about end-of-life care) and encourage families to work together as a team. Second, when caregivers are properly trained to recognize and deal with warning signs and problems, they may be more likely to provide effective support, prompting, and reinforcement to the patient. Greater support and reinforcement may be especially useful in helping patients overcome obstacles to adaptive coping and symptom management. Third, actively involving caregivers by addressing their needs and concerns may help them manage their own distress and enhance their self-efficacy for caregiving.31-33 Indeed, research has shown that family caregivers can help improve the palliative care of patients, 34 have the potential to gain positive outcomes from their caregiving role, 35 and are pivotal to achieving “successful” home care, where most patients choose to die.36,37 Participating in such interventions may also help to ease the bereavement process after the patient’s death. 38 Fourth, actively involving the family may result in higher intervention retention rates and symptom control compared to interventions offered only to patients or caregivers.39-41 Finally, because patient and caregiver distress and QOL are related, programs that consider how one person affects the other and how that influences the coordination of care may result in improvements for both.42-44 Unfortunately, despite their potentially beneficial effects, very few family-based interventions have been conducted and rigorously tested in advanced cancer populations.
Family-Based Psychosocial Interventions in the Advanced Cancer Context
Based on our review of the empirical literature, 11 family-based studies that sought to improve the QOL of advanced cancer patients and their caregivers were identified. Because of the limited number and diversity of studies published in this area, both RCTs and pilot studies were included in this review. Study participant and design characteristics are summarized below, and Table 1 provides a description of the characteristics and key findings for each study. Overall, the interventions that were reviewed provided health information and taught skills to improve coping, communication in the family, and problem solving. Studies that sought to improve general QOL did not evidence significant effects for patients or partners.45,46 However, modest improvements in patient and caregiver relationship functioning, patient distress, and caregiver burden were found across studies. With only a few exceptions,38,47,48 these modest improvements following intervention were not maintained over time. Often, researchers did not articulate a theoretical model or examine the mechanisms by which interventions affected outcomes. Most studies had small sample sizes and were underpowered to examine changes in the multiple outcomes that were measured. Some studies did not include information on refusal or attrition rates, suggesting that reporting standards could improve. Finally, questions remain regarding when and how family-based interventions should be optimally delivered.
Studies of Family-Based Psychosocial Interventions in Advanced Cancer.
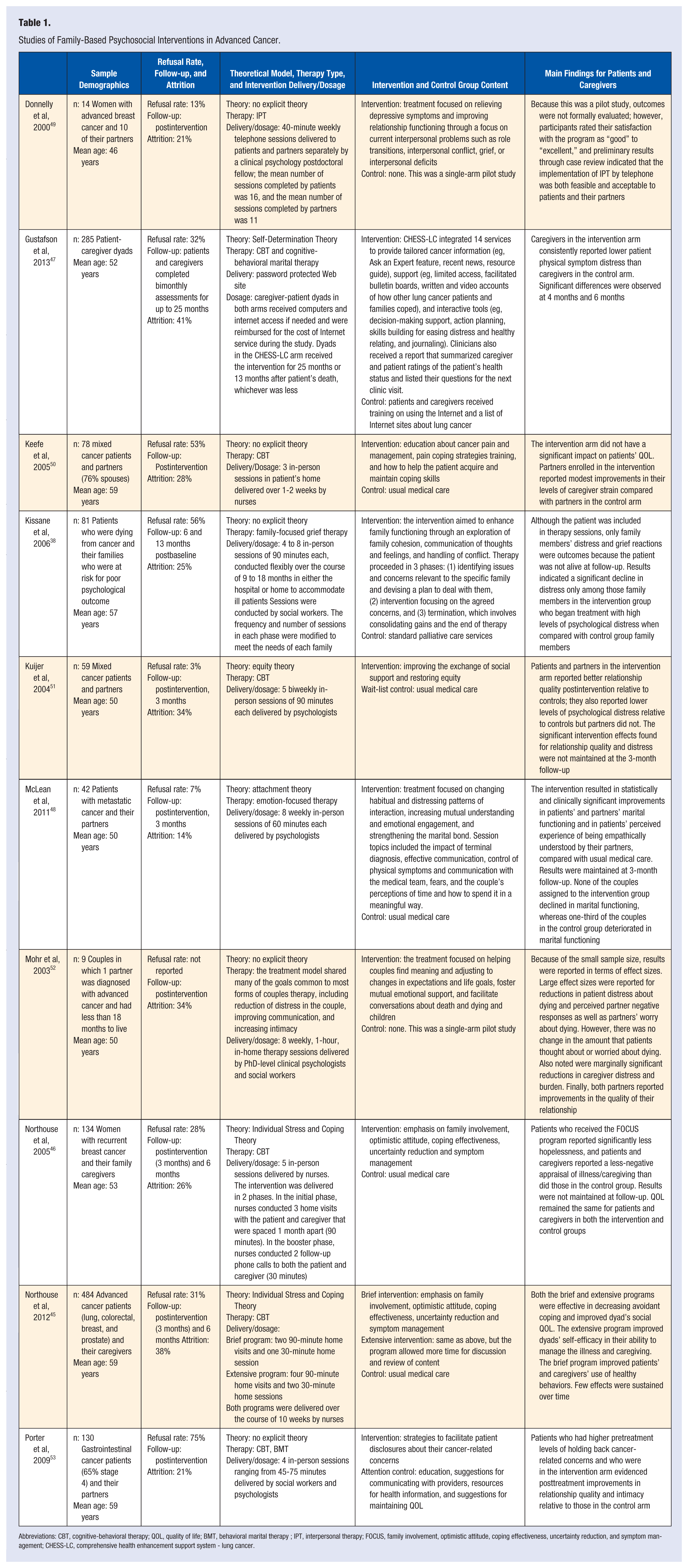
Abbreviations: CBT, cognitive-behavioral therapy; QOL, quality of life; BMT, behavioral marital therapy ; IPT, interpersonal therapy; FOCUS, family involvement, optimistic attitude, coping effectiveness, uncertainty reduction, and symptom management; CHESS-LC, comprehensive health enhancement support system - lung cancer.
Participant Characteristics
The mean age for study participants was 53 years. The total number of couples enrolled varied considerably by study, from 9 11 to 484. 45 Six studies had sample sizes ≥100.38,48-52 Refusal rates varied widely from 3% 51 to 75% 53 (mean = 33%). At final follow-up, the mean attrition rate was 28% (range = 14% 48 to 41% 47 ).
Design Characteristics
With the exception of 1 study that treated the family as a unit, 38 all the studies were dyadic in terms of format, enrolling the patient and 1 other person. However, studies were relatively evenly divided in terms of who that other person could be. Five studies focused exclusively on couples and restricted enrollment to spouses/significant others11,48,49,51,53; 4 studies took a broader approach and restricted enrollment to the patient’s primary caregiver (could be a spouse/partner or another family member).45-47,50 The primary intervention target varied across studies, with some studies focusing on individual patient outcomes (eg, pain), 37 some studies focusing on caregiver/family member outcomes (eg, distress),38,47 and some studies focusing on the couple as a unit and seeking to address couple-level outcomes (eg, marital functioning) as well as individual patient and caregiver outcomes (eg, distress and QOL).11,45,46,48,51,53 Likewise, the therapeutic techniques that were used were similarly varied and included cognitive-behavioral therapy, emotion-focused therapy, interpersonal therapy, behavioral marital therapy, and family-focused grief therapy.
Half of the studies38,49,50,52,53 had no explicit theoretical framework. With the exception of the Gustafson et al 47 study, which used a motivational theory of health behavior change, the remainder of the studies utilized theoretical models of either stress and coping or marital adjustment. For example, 2 studies39,40 were grounded by the stress-appraisal model of Lazarus and Folkman 54 which posits that person-, social-, and illness-related factors influence how people appraise and cope with an illness, which in turn affects their QOL. Therapies based on this model focus on reducing negative appraisals of stress and improving individuals’ self-efficacy or confidence in their ability to deal effectively with stressful situations. Equity theory, 55 which grounded one study, 51 acknowledges that help and support may have flowed back and forth between partners before the onset of illness but that that exchange may become more unidirectional after illness, causing both partners to feel inequitably treated and experience more psychological and marital distress. Finally, one study utilized attachment theory 48 based on its relevance in the context of advanced cancer because of the impending separation caused by the ill partner’s death and the idea that emphasis on the quality of the attachment bond and involvement between spouses can mitigate grief and loss. 56
In terms of structure, the number of intervention sessions ranged from 345,50 to 8, 48 and session-length varied from 40 to 90 minutes. Most interventions involved in-person sessions, either in the patient’s home or in the hospital; however, 1 study was Internet based, 47 1 study was telephone based, 49 and 2 studies involved a combination of in-person and telephone sessions45,46 Follow-up assessments were conducted postintervention to up to 13 months later.
Health-System Barriers Make It Difficult to Provide Family-Centered Care
Although the above review suggests that family-based interventions are acceptable to advanced cancer patients and their family members and have been modestly successful in reducing distress and improving marital functioning in the advanced cancer setting, researchers must carefully consider their practical application in order to increase the likelihood of uptake and dissemination. It is difficult within existing models for palliative care to meet the needs of patients and families 57 because resources are barely sufficient to care for patients, 58 and doctors/nurses often lack the skills and training to confidently evaluate and address family needs.59,60 Short hospital stays may restrict the time available for health professionals to implement supportive interventions for families, and health professionals may not want to dwell on discussions about poor prognosis with the patient because they may be fearful that such discussions may do more harm than good. 25 Mental health specialists with specialized training to work with couples and families often work in systems that are separated from oncology and palliative care teams by location and insurance. 61 Family members may not seek out information or support because they feel that their role is more tangential and that their needs are not as important as those of the patient.62,63 Compounding the problem, most educational materials in the palliative setting are written and geared toward patients despite research showing that family caregivers need their own educational materials that incorporate problem-solving strategies, how to provide care, and how to maintain their own health while caring for the patient. 64 Together, these challenges adversely affect the ability of health care professionals to provide comprehensive, family-centered care, and an awareness of these obstacles allows the development of interventions that are designed to address them.
Review Synthesis and Future Research Directions
As this review shows, there is a great unmet need in supporting family systems and caregiver-patient dyads, and finding ways to deliver effective interventions in the context of advanced-stage cancer presents an equally great challenge. Overall, the impacts of the interventions in this review were limited by small sample sizes; varying theoretical, therapeutic, and methodological approaches; and a lack of integration with clinical care systems. Greater attention to these issues is necessary for this research area to move forward.
Whereas all the studies that were reviewed specified a particular therapeutic approach, only half specified a theoretical framework. In clinical psychology, the emphasis on evidence-based treatments has resulted in attention being paid to manualized treatment methods to change targeted outcomes. Less attention has been paid to the development and validation of comprehensive evidence-based theories that focus on the process of change or specify how particular treatment tools can be optimally applied. 65 None of the studies that were reviewed examined mediators of effect, and 2 that examined moderators found that their interventions only benefited a subset of couples—specifically, those who had greater cancer-related distress or poor communication skills at the outset.38,53 In contrast, one intervention 45 found that patient distress accounted for very few moderator effects. The authors postulated that just because dyads are identified as being at high risk for poorer outcomes, it does not necessarily mean that they will obtain more benefit from an intervention than low-risk dyads. Clearly, more research is needed to determine whether there are profiles of at-risk couples who may benefit more from intervention and whether it is necessary to screen for marital and/or psychological distress in both the patient and partner.
A number of the studies found differential effects for patients and caregivers, with several reporting significant effects of intervention on patient but not caregiver outcomes.11,46,48,51 More work is needed to disentangle gender and role effects on couples’ psychosocial adaptation to advanced cancer and to ensure that interventions involve caregivers by actively addressing their needs and concerns instead of enlisting them merely as supporters of the patient. More work is also needed to determine whether intervention content should be tailored based on the type of caregiver who is participating. Of the 11 studies that were reviewed, 5 restricted enrollment to spouses/significant others. Although we were unable to discern any systematic differences between those studies that enrolled spouses and those that were open to other family members, the caregiving literature suggests that spouses may be at higher risk for distress because romantic partners are the primary attachment figures in adulthood, 66 and closer relationships tend to be associated with greater caregiver stress. 67 Although few studies in cancer have explored whether the challenges of caregiving differ for spouses and other family caregivers, 68 a recent meta-analysis 69 of 168 empirical studies found that the spouses of older adults provided more caregiving support than adult child caregivers and children-in-law. Spouses also reported more depressive symptoms, and their distress levels were largely explained by the amount of time they spent providing care. Children-in-law perceived their relationship with the care recipient as less positive than spouses, and they reported fewer uplifts of caregiving. These findings suggest that spousal caregivers may benefit most from programs that help them to reduce caregiving demands (eg, respite), and children-in-law may benefit most from programs that target strengthening their relationship with the patient.
In terms of intervention content, most studies provided health information and taught skills to improve coping, communication, and problem solving. Few addressed the impact of physical changes, negotiation of role changes caused by disease progression or the coordination of care, and reconciliation of the family’s need to provide caregiving with the patient’s need to maintain autonomy and dignity. Moreover, despite the fact that cancer patients are often inadequately trained to manage side effects at home70-72 and their family members often assume their caregiving role with little or no formal preparation and training,68,73 surprisingly few studies addressed symptom control or symptom management or alerted families about palliative care/hospice resources and services. Given that the communication needs of families extend to their relationship with the patient’s physician, strategies for communicating with the medical team may be a useful component in future interventions. Finally, interventions that include the process of reviewing one’s life, along with ways individuals can maintain or enhance their relationships and continue to relate as spouses or family members instead of patient and caregiver, may be important issues to address in family-based protocols at the end of life.74,75
Researchers interested in developing family-based interventions in advanced cancer care should give careful consideration to their choice of outcomes and what such interventions can realistically be expected to accomplish.10,76 Overall, the studies in this review were not successful in improving general QOL or multiple dimensions of QOL. Studies that sought to improve specific aspects of QOL such as psychological or relationship functioning were more successful, but few had sustained effects over time. Given the functional deterioration and impending death of the patient, it is possible that long-term expectations of improvement in general or multiple aspects of QOL are not realistic. 46 It is also possible that different intervention dosages may be required to effect change in different types of outcomes. Indeed, results from the only study in this review that examined intervention dosage suggest that short-term interventions (3 sessions) are more likely to produce change in single-dimension domains (eg, information or support seeking skills) and that longer interventions are needed to improve multidimensional outcomes such as depression. 45 Additional therapy sessions (also known as booster sessions) may also be needed to maintain the impact of intervention once it is completed. However, booster sessions involving both the patient and caregiver may not be realistic or feasible given the patient’s increasing physical deterioration and functional disability. More research is needed to determine if booster sessions offered to the caregiver alone can result in improved outcomes for both partners.
To date, only a handful of RCTs of family-based interventions have been conducted in advanced cancer, and some researchers have suggested that other designs should be considered because the integrity of the traditional RCT may be seriously compromised in the advanced cancer setting. 77 For example, there are ethical questions regarding the withholding of services from those who are in need and the true comprehension of allocation methods for patients who are at the end of life who may be experiencing problems with cognition. 78 Often, trials use wait-list controls as an ethical solution to withholding new services, but this may not be feasible in cases where patients have only a few months or weeks to live, particularly if follow-up data are to be collected. 77 Finally, the selection of those who meet strict eligibility criteria may threaten generalizability, and low rates of participation coupled with high rates of dropout may hamper statistical power to detect important effects. 79
The recruitment and retention issues faced by family-based RCTs are even more complicated than those faced by traditional RCTs involving the patient alone because 2 (or more) individuals must participate and complete all the follow-ups. Reflecting this, refusal rates in the studies that we reviewed varied widely from 3% to 75%. One way to view these refusal rates is to consider them in the larger context of enrollment clinical trials, where only 5% to 30% of adult cancer patients participate.80,81 Although detailed descriptions of the barriers to enrolling families was not routinely provided in the studies that we reviewed, interventions involving couples coping with early-stage cancers have cited scheduling problems and older age as factors affecting enrollment.82,83 Reflecting this, the average age of study participants in this review was only 53 years. Given the likelihood that older cancer patients may experience different symptom management profiles and challenges than younger patients, 84 the findings reported here may not be generalizable to older cancer patients and their family caregivers.
The overall burden placed on the patient and caregiver as a result of their participation in RCTs must also be considered. Many studies require substantial travel and time commitments to attend sessions and complete assessments. Looking broadly at the accrual rates for family-based interventions, Fredman et al 85 found that interventions that involved high levels of burden were associated with lower rates of enrollment and that rates of participation increased as study burden decreased. Thus, rather than completely abandon the RCT, researchers may need to adapt their designs to address the unique needs of advanced cancer patients and their families. For example, enlisting physicians or clinic staff to introduce the study and reinforce that it is an important part of the patient’s overall medical care may help bolster recruitment. 85 Likewise, incorporating strategies such as scheduling study-related appointments with medical appointments or conducting sessions by phone, the Internet, or in patients’ homes may help reduce travel burden and improve scheduling convenience for patients and their busy families. Such modalities also have the potential for more widespread dissemination of psychosocial interventions through “remote counseling.” 86
In sum, the experience of advanced cancer profoundly affects patients and their family members. Family-based interventions hold great promise for empowering families with skills to provide care and meet the challenges of advanced cancer, improving patient and caregiver QOL, and improving the quality of care provided to patients and their families at the end of life. However, more work is needed to refine intervention focus and outcomes, specify mechanisms of effect, integrate these programs into routine clinic care, and expand their dissemination and outreach. Taking a more rigorous scientific approach by conducting theoretically grounded RCTs that are adapted for practical application in the setting of advanced cancer and developing a clearer understanding of why different intervention approaches do or do not work will go a long way toward informing future intervention efforts and improving the quality of palliative care for patients and their families.
Footnotes
Acknowledgements
This research was supported by a career development award from the National Cancer Institute K07CA124668 (Hoda Badr, PhD, Principal Investigator) and a pilot grant awarded to Dr Badr under P30 AG028741 (Albert Siu, MD, Principal Investigator).