
Abstract
Physical inactivity constitutes the fourth leading cause of death worldwide. Health care providers (HCPs) should play a key role in counseling and appropriately referring their patients to adopt physical activity (PA). Previous reports suggest that active HCPs are more likely to provide better, more credible, and motivating preventive counseling to their patients. This review summarizes the available evidence on the association between HCPs’ personal PA habits and their related PA counseling practices. Based on relevant studies, a snowball search strategy identified, out of 196 studies screened, a total of 47 pertinent articles published between 1979 and 2012. Of those, 23 described HCPs’ PA habits and/or their counseling practices and 24 analytic studies evaluated the association between HCPs’ personal PA habits and their PA counseling practices. The majority of studies came from the United States (n = 33), and 9 studies included nonphysicians (nurses, pharmacists, and other HCPs). PA levels were mostly self-reported, and counseling was typically assessed as self-reported frequency or perceived self-efficacy in clinical practice. Most (19 out of 24) analytic studies reported a significant positive association between HCPs’ PA habits and counseling frequency, with odds ratios ranging between 1.4 and 5.7 (P < .05), in 6 studies allowing direct comparison. This review found consistent evidence supporting the notion that physically active physicians and other HCPs are more likely to provide PA counseling to their patients and can indeed become powerful PA role models. This evidence appears sufficient to justify randomized trials to determine if adding interventions to promote PA among HCPs, also results in improvements in the frequency and quality of PA preventive counseling and referrals, delivered by HCPs, to patients in primary care settings. Future studies should also aim at objectively quantifying the effect of HCPs’ PA role-modeling and how it influences patients’ PA levels. More evidence from low-to-middle income countries is needed, where 80% of the deaths due to inactivity and related noncommunicable diseases already occur.
‘Physical inactivity ranks as the second leading cause of death worldwide and constitutes a priority target for global action to help control the rising burden of noncommunicable diseases.’
Physical activity (PA) recommendations encourage every adult to engage in at least 150 minutes a week of moderate to vigorous activity.1,2 Physical inactivity ranks as the fourth leading cause of death worldwide3,4 and constitutes a priority target for global action to help control the rising burden of noncommunicable diseases (NCDs). 5 In 2010, almost one third of the world population was categorized as being physically inactive, 6 and an estimated 5 million deaths worldwide could be attributable to inactivity. 4
Reducing physical inactivity requires a “whole of society” approach, including environmental and policy changes to make physically active choices an easier choice for leisure or transportation purposes. Beyond the physical environment, changes in the “social” environment are also required, including cultural and social norms in relation to PA and the value populations and health care providers (HCPs) assign to PA.
Counseling by physicians and other HCPs has been shown to be useful in helping patients improve their lifestyles. When done adequately, HCP-initiated PA counseling is moderately effective, resulting in short-term (12 months) improvements in patients’ PA levels7,8 and has the potential to improve years lived free from disease. 9 In addition, evidence suggests that schemes where PA counseling is done by a team of HCPs providing referrals to accessible community resources for PA can be cost-effective. 10 Regular PA counseling by HCPs is included as a national public health objective in the United States (Healthy People 2020). 11 Additionally, PA counseling and referral schemes are part of health care systems in the United Kingdom, 10 Sweden, 12 Switzerland, 13 and Brazil. 14 However, rates of PA counseling by physician and other HCPs still remain unacceptably low in those countries with available data.15-19
Many barriers have been identified as contributors to HCPs’ low rates of PA counseling, including inadequate knowledge, provider self-efficacy, office time constraints, lack of reimbursement, as well as intrinsic HCP factors, including poor personal habits.20,21 Although some studies show physicians’ lifestyle habits are relatively better when compared with those of the general population, 17 there is less evidence on the personal habits of other HCPs involved in primary health care, such as nurses, physician assistants, social workers, dietitians, physical therapists, or exercise specialists. In addition, studies report that HCPs who engage in healthy habits such as not smoking, eating a healthy diet, or having periodic preventive health screenings and immunizations also provide preventive counseling to their own patients more frequently and more confidently,22-25 and their patients engage in related preventive practices more often. 26 In addition, we and others have proposed that physically active HCPs will be more sensitive to the obstacles to starting or maintaining an active lifestyle and, therefore, may have higher success in initiating and sustaining counseling for their own patients on this topic.27-29
Based on the premise of “preach what you practice” and given that HCPs are one of the primary sources of preventive care information for the public, a better understanding of the relation between HCPs’ personal PA behaviors and their related counseling practices can help guide the development of interventions to promote active lifestyles among HCPs. In turn, these interventions may also help improve population health and reduce the risk of inactivity-related NCDs. Consequently, the purpose of this review is to summarize the evidence evaluating the role of health care providers as models for PA among their patients.
Methods
In 2010, the US Preventive Services Task Force (USPSTF) published an updated report of PA counseling in primary care, which included the latest evidence on PA interventions delivered in primary care settings. Results showed that, overall over an average follow-up of 12 months, counseling increased participants’ self-reported PA levels, by approximately 38 minutes per week, in randomized controlled trials (RCT) that provided at least medium-intensity interventions. Medium- to high-intensity PA counseling resulted in changes in self-reported PA. However, there was very limited evidence for maintenance of behavioral effects beyond 12 months, particularly for low- and medium-intensity interventions; so the Task Force concluded in 2012 that
although the correlation among healthful diet, physical activity, and the incidence of cardiovascular disease is strong, existing evidence indicates that the health benefit of initiating behavioral counseling in the primary care setting to promote a healthful diet and physical activity is small. Clinicians may choose to selectively counsel patients rather than incorporate counseling into the care of all adults in the general population.
Our framework for this review was based on the latest available evidence from the USPSTF review, which indicates that PA counseling by HCPs in primary care settings can be moderately effective in improving patients’ PA levels, at least in the short term. To inform our research, we summarized the information from the most recent USPSTF update regarding the effectiveness of PA behavioral counseling in the 31 RCTs included in the 2010 USPSTF review (Table 1). In addition, we went back to the original RCT reports to better understand which HCPs (physicians, nurses, health educators) were involved in providing the PA behavioral counseling and summarized that information in Table 1.
Summary of Available Evidence to Recommend PA Counseling by Health Care Provider and Setting (Adapted From USPSTF a ).
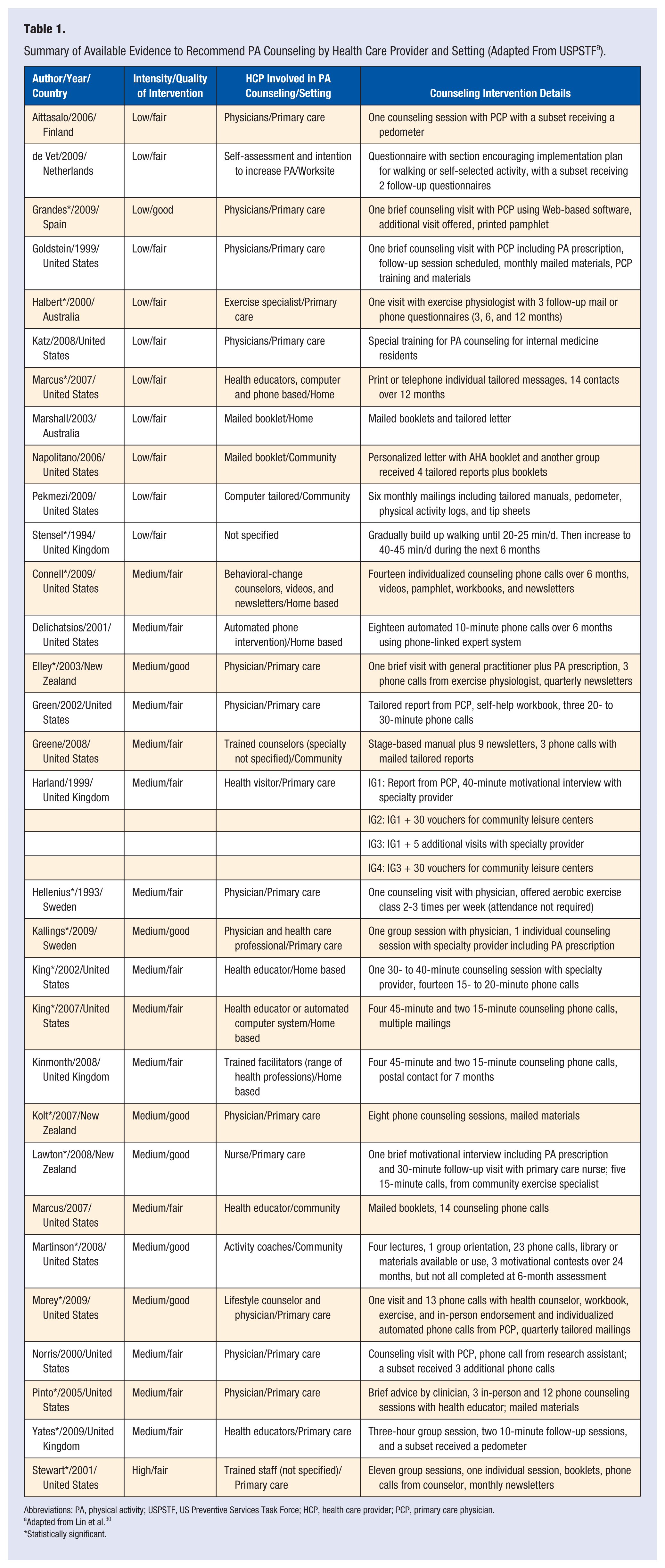
Abbreviations: PA, physical activity; USPSTF, US Preventive Services Task Force; HCP, health care provider; PCP, primary care physician.
Adapted from Lin et al. 30
Statistically significant.
Search Strategy
For this review, search terms such as “attitudes/habits,” “health personnel,” “health care providers,” “physical activity,” “exercise,” and “role model” were used to find articles evaluating the role of HCPs as models for PA among their patients in PubMed/Medline between 1979 and June 2012. The resulting articles were retrieved and an additional snowball literature search strategy was used 31 to identify other sources and relevant articles. Selected articles came from observational studies describing HCPs’ PA habits, HCPs’ counseling practices, and/or analytic studies describing the association between HCPs’ PA habits and their counseling on PA. Studies that did not report a measure of HCPs’ personal PA habits (either self-reported or objectively assessed) or HCPs’ PA counseling practices (self-reported frequency of PA counseling, self-efficacy for PA counseling, attitude toward PA counseling, perceived relevance of PA counseling, or patient report of receiving PA counseling) were excluded. The resulting studies were organized based on characteristics such as country of origin, study design, population, PA assessment methodology, and main outcome measure.
Results
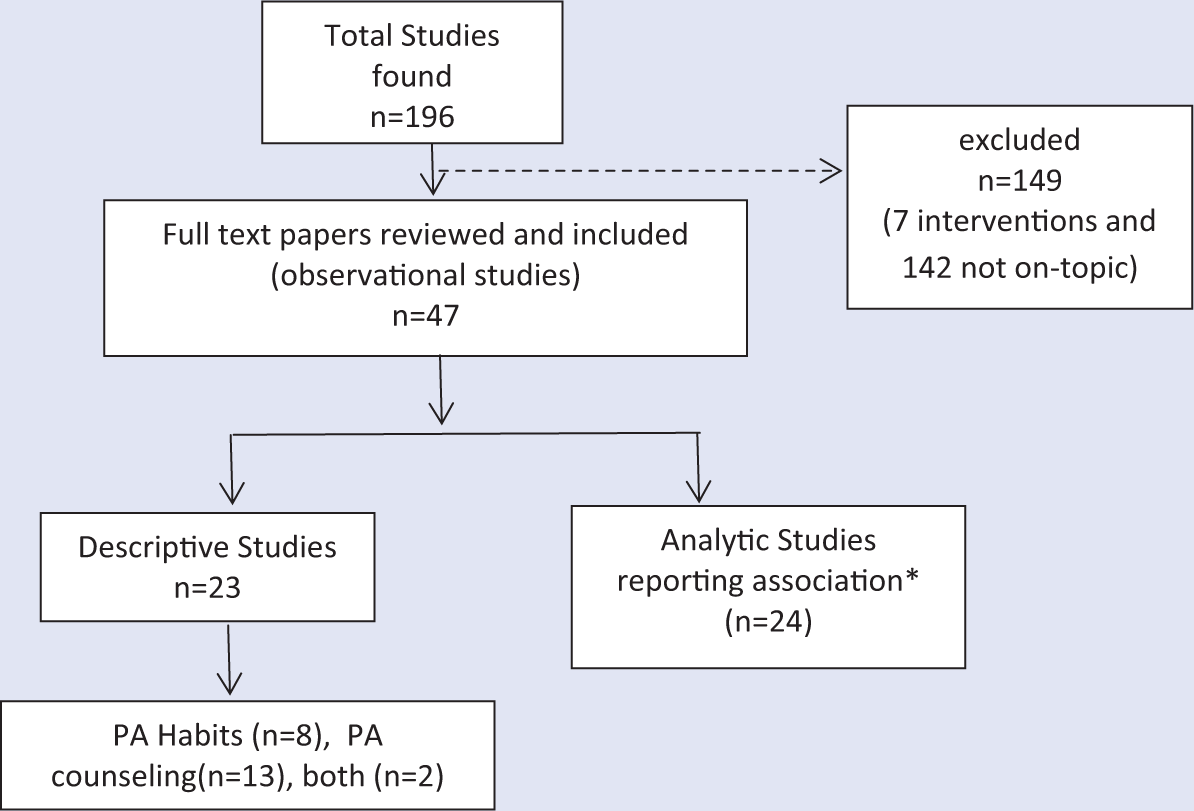
A total of 196 articles were screened from our search strategy, and of those, 47 were included in this review. Of the studies included, 23 described either the HCP PA habits or counseling practices and 24 studies evaluated the association between HCPs’ PA habits and their PA counseling practices (Figure 1).
Overview of Included Studies.
Most of the studies were conducted in the United States (n = 33). The rest took place in the United Kingdom (n = 6), Canada (n = 3), Spain (n = 2), India (n = 1), Colombia (n = 1), and the Netherlands (n = 1).
Several studies focused only on physicians (n = 35) while others (n = 9) included other HCPs such as nurses, dietitians, pharmacists, health educators, and health care staff in general. The rest (n = 3) were studies that included a multidisciplinary team of physicians and other HCPs. The most frequent PA assessment method was self-administered questionnaires, but there were also phone interviews and interviewer-administered questionnaires. Very few studies measured PA habits with objective methods. HCPs’ counseling practices and behaviors were mostly self-reported as perceived frequency or self-efficacy.
A total of 13 articles were published before 2000 (from 1984 to 1999), and the rest (n = 34) were published from 2000 to 2012. Studies done before 2000 (n = 13) were done mostly in physicians (n = 10) and the remaining (n = 3) in nurses; no other HCPs were included before 2000. There were no studies done in students before 2000, compared with the most recent findings after this date from medical and nursing students. Barriers reported for PA attainment did not differ from the old studies to the new ones published after 2000. Rates of PA counseling for studies published before 2000 were higher, ranging from 40% to 70%, compared to studies published after the year 2000, which found lower rates of PA counseling, ranging from 12% to 40%.
PA counseling was defined very differently from study to study, with some studies not defining clearly what method was used by the HCP to counsel their patients. Some studies defined counseling as the frequency of talking to their patients about PA or exercise habits (ie, “How frequently do you talk about PA with your patients?”),32-35 others defined it as a composite of measures between assessment (fitness, anthropometry) and education (providing pamphlets and discussion), 36 and fewer studies went into details such as counseling for intensity and type of activity.36,37
Out of the 47 studies included in this review, all but one 38 were cross-sectional and described either HCPs’ personal PA habits (n = 8), HCPs’ PA counseling practices (n = 13), both (n = 2), or the association between personal PA habits and related PA counseling (n = 24; Figure 1).
In Table 1, we summarized the USPSTF PA interventions offered by the 31 studies included in the latest review on PA behavioral counseling in primary care in particular as it related to the settings and type of HCPs providing the PA counseling. Out of 31 RCTs, 17 found a significant positive effect on participants’ PA levels. Out of those RCTs, health educators were primarily in charge of providing the PA behavioral counseling in 8 interventions, physicians in 6 interventions, nurses in 1 study, and technology-based approaches (Web-based, automated calls) in 2 interventions.
Physical Activity Habits of HCPs
Out of the 23 descriptive studies that reported PA habits or PA counseling practices (Table 2), 8 studies were identified that only described HCPs’ PA levels. Physicians reported higher compliance with current PA guidelines, ranging from 45% to 90%, while the reported compliance among other HCPs (nurses and dietitians) ranged from 39% to 70%.
Descriptive Studies Reporting HCPs’ Personal PA Habits, Their PA Counseling Practices, or Both, 1979-2012.
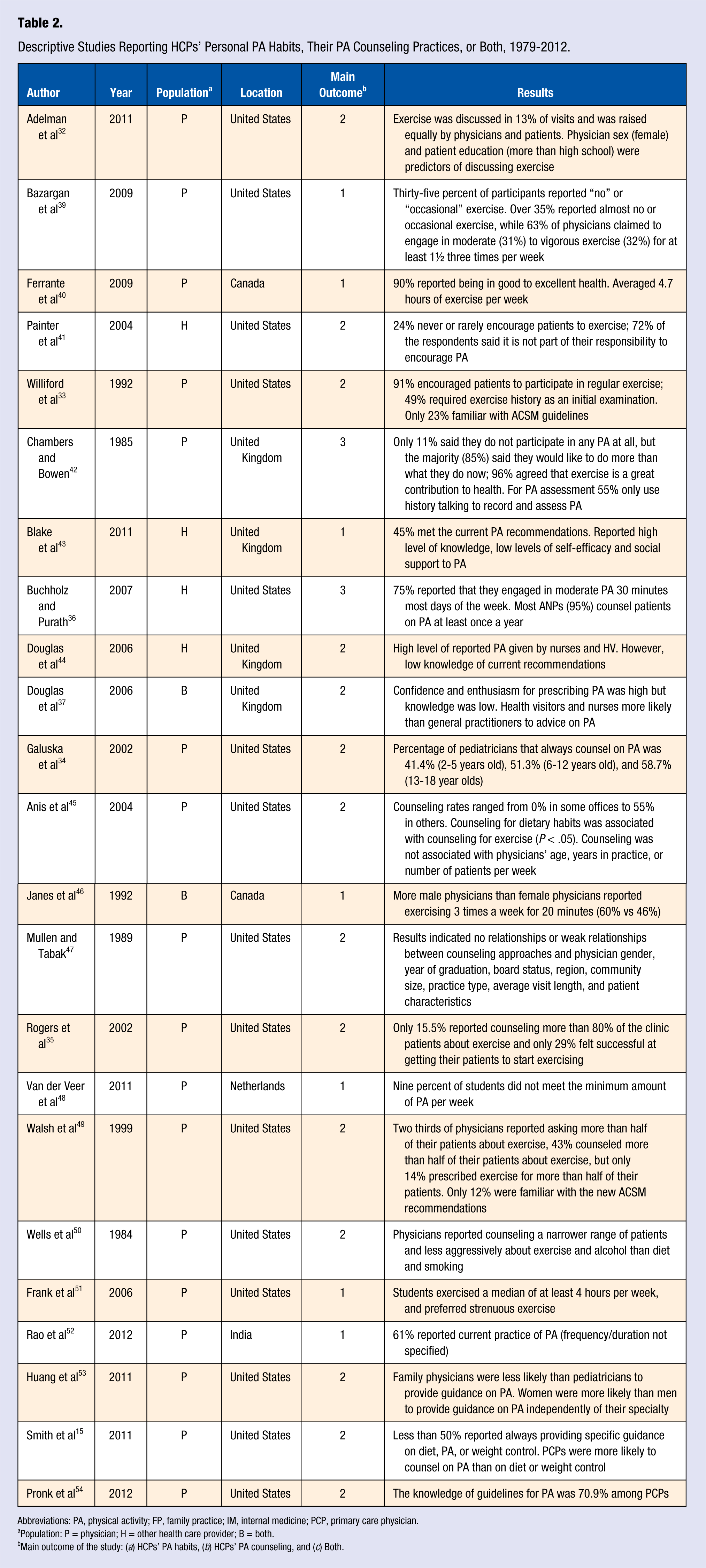
Abbreviations: PA, physical activity; FP, family practice; IM, internal medicine; PCP, primary care physician.
Population: P = physician; H = other health care provider; B = both.
Main outcome of the study: (a) HCPs’ PA habits, (b) HCPs’ PA counseling, and (c) Both.
We found 6 studies that reported PA habits and behaviors among medical (n = 5) or nursing students (n = 1).38,48,51,52,55,56 Medical students included in these studies, although not all samples were fully representative, also appear to have healthier habits than the general population, with less evidence from other HCPs. No information was found on studies evaluating the PA habits from other HCPs such as dietitians or social workers. For medical students, 4 studies were conducted in high-income countries (the United States, Spain, and the Netherlands) and 2 in low- to middle-income countries (India and Colombia). A study of medical students performed in 10 medical schools in Colombia (n = 661) found that half of first- and fifth-year students complied with PA guidelines. 56 The study also reported that 85% and 91% of first- and fifth-year students respectively, had a positive attitude toward always counseling patients about PA. Frank et al38,57 also studied PA habits and behaviors of medical students in the United States. In her study, which included 17 medical schools (n = 1906), students reported engaging on average in 80 minutes/week of moderate exercise and 100 minutes/week of vigorous exercise, with 74% of the sample meeting PA guidelines. In contrast, a study from Spain 55 found female nursing students to be somehow less active than students in non–health disciplines; however, these differences were not statistically significant: 50% physical inactivity among first-year nursing students, 47.5% among last-year nursing, and 43.6% among nonnursing students. Overall, the studies report that in general medical students complied with current PA recommendations (average between 70% and 90%). One study among nursing students showed higher rates of physical inactivity; however, the results were less consistent.
Physical Activity Counseling Among HCPs
We identified a total of 15 studies* (Table 2) describing the self-reported frequency, self-efficacy, and attitudes of HCPs toward PA and exercise counseling. The majority of studies (n = 12) included physicians or medical students’ PA counseling, 1 included a sample of both physicians and nonphysicians, and 2 included other HCPs such as nurses, social workers, and dietitians. We found several enabling factors for HCPs to counsel on PA and these were consistent among physicians and nonphysicians. Factors included higher patient level of education, 32 being a female HCP,32,34,53 primary care specialty,15,49,53 and in some cases provider’s age >35 years. 49 Specifically, a study with older adults found female physicians who cared for patients with a higher education (more than high school) to be significant predictors of the physicians’ likelihood of providing PA counseling among older patients. 32
Very few studies reported nonphysician HCPs’ counseling for PA36,37,41,44; however we found that these groups, especially nurses and social workers, include regular preventive counseling recommendations more frequently than physicians into their practice.
HCPs Continue to Be Often Ill Prepared for PA Counseling
Callaghan reported that nurses who exercised in the previous week were more likely to rate exercise as important to health (P < .0003) and thus recommend it more to their patients. 58 Douglas et al 37 found UK nurses and health visitors were more likely to recommend PA to their patients than physician assistants, even when knowledge of current PA recommendations was very low: 13% of general practitioners, 9% of health visitors, and 7% of nurses described correctly current PA recommendations. For all studies found, knowledge of current PA recommendations was low and ranged from 12% to 27% among physicians and from 7% to 9% among other HCPs.
In terms of who is responsible for providing PA advice, a study among internal medicine residents 35 found that more than 90% felt it was the physicians’ responsibility to counsel patients on exercise but only 15% of the residents reported counseling their patients. On the other hand, a study among dietitians, nurses, patient care technicians, and social workers showed that 72% of the respondents did not think it was their responsibility to encourage PA among their patients. 41
The most common perceived barriers for not counseling on PA were similar among physicians and nonphysician HCPs. We found a total of 7 studies reporting HCPs’ most frequent barriers to counsel on PA, all of them from either the United States or the United Kingdom. The most frequent reported barriers were lack of time,35,36,44,49,59 HCPs’ low self-efficacy for PA counseling,41,49,59 lack of PA counseling materials, 60 lack of reimbursement,36,37 lack of knowledge and counseling skills,37,41,44,60 and patient’s comorbidities. 35
Association Between HCPs’ Personal PA Habits and Their Related PA Counseling Practices
In this review, we found a total of 24 analytic studies (Table 3) describing HCPs’ own PA habits as a correlate of the PA counseling they provide to their patients. Out of these 24 studies, 19 reported a significant positive association between HCPs’ PA habits and counseling frequency, self-efficacy, or perceived importance. The remaining 5 studies either did not report a measure of association61-63 or had nonsignificant results, although a trend was observed toward a positive association.55,56
Analytic Studies That Have Evaluated the Association Between HCPs’ Personal PA Habits and Their Related PA Counseling, 1979-2012.
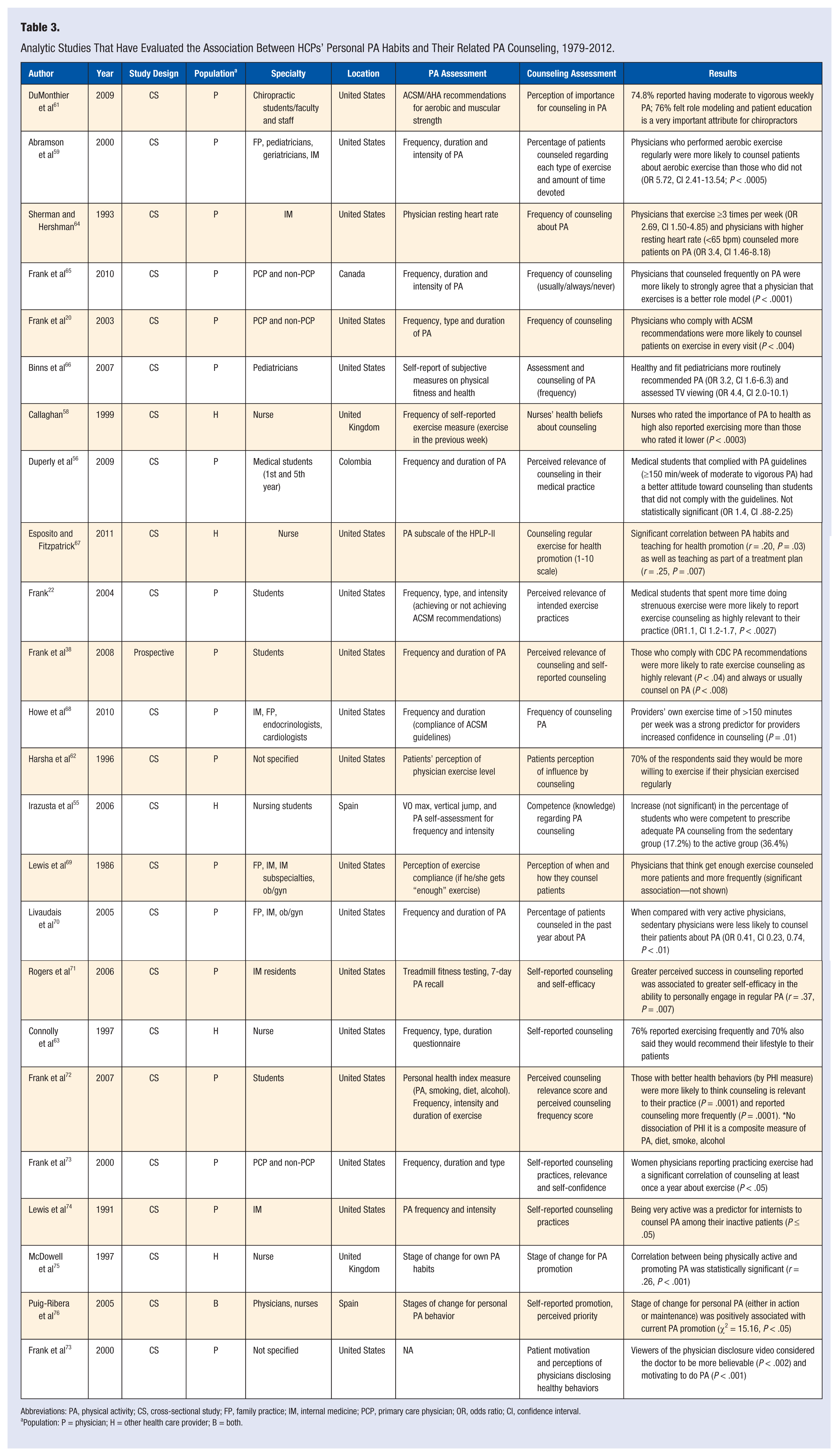
Abbreviations: PA, physical activity; CS, cross-sectional study; FP, family practice; IM, internal medicine; PCP, primary care physician; OR, odds ratio; CI, confidence interval.
Population: P = physician; H = other health care provider; B = both.
Figure 2 shows 6 studies found in this review that allowed a head-to-head comparison. These were studies that reported an odds ratio (OR) as a measure of the association between physicians self-reported PA habits and their PA counseling attitudes and practices, after controlling for potential measured confounders. Five out of these 6 studies reported a significant positive association, suggesting that physicians’ personal PA levels are a consistent and independent correlate of their PA counseling attitudes and practices (ORs ranging between 1.4 and 5.7; all P < .05). Other studies reported a significant positive association between the regularity and intensity of HCPs’ PA and the frequency with which they counseled their patients about PA.*
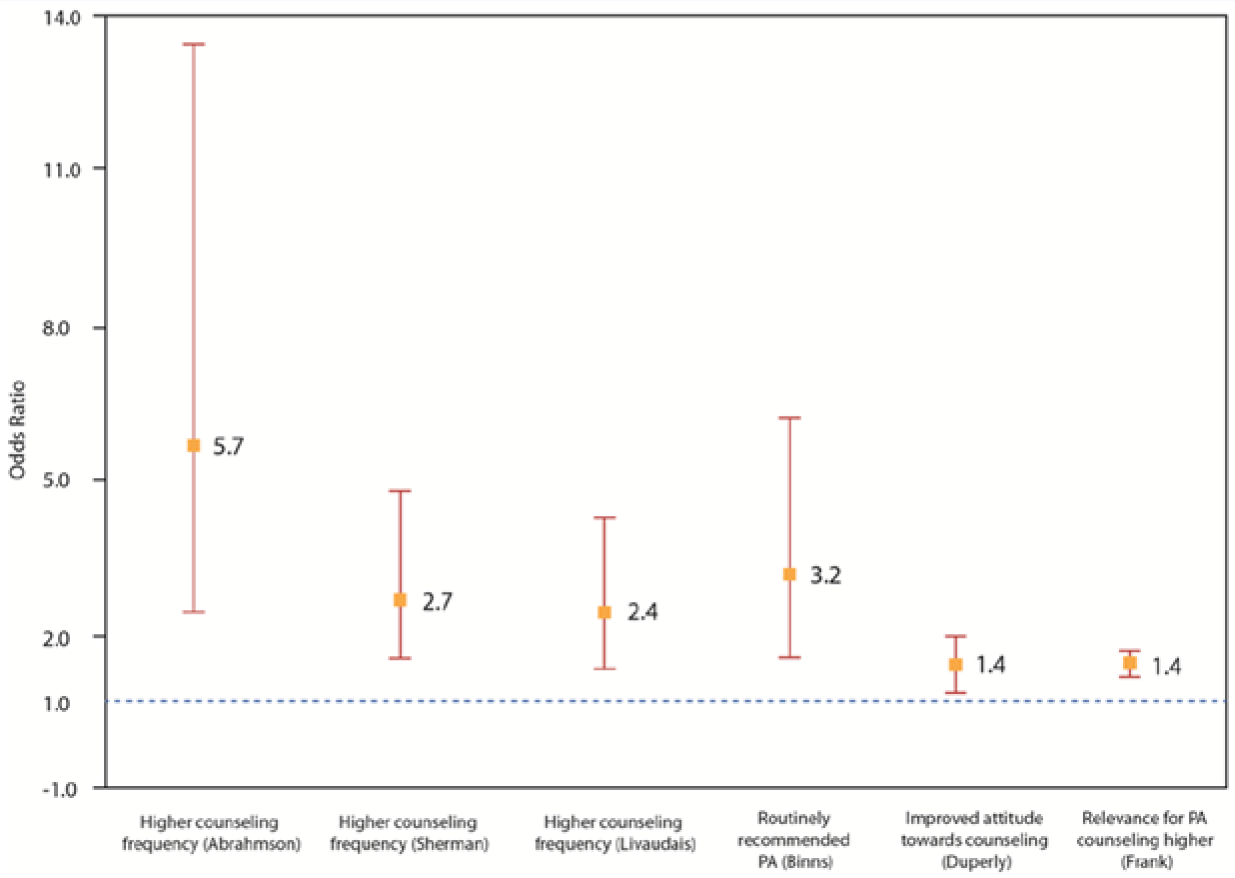
Association Between Physicians’ Personal PA Levels and Their Attitudes and Practices Toward PA Counseling.a
Active HCPs Provide More and Better PA Counseling Irrespective of Specialty or Time in Practice
With regard to physicians’ specialty, we found studies evaluating family practitioners, pediatricians, geriatricians, and internists,59,69,70,74 and they found the same positive association between personal PA habits and counseling provided on PA. Even those who perceived themselves as healthy and fit recommended PA more frequently (OR 3.2, CI 1.6-6.3) and assessed sedentary behavior such as TV viewing (OR 4.4, CI 2.0-10.1) more frequently among their patients. 66 Frank has studied this association in-depth, among Canadian physicians, 65 US physicians, 20 and medical students. 38 Among a sample of female physicians in the United States, those who complied with PA recommendations were more likely to counsel patients about exercise (P = .004). 20 Canadian physicians reported a positive association between attitudes toward being a role model for their patients and higher frequency of PA counseling (P < .001). 65 Another study 64 used resting heart rate as a proxy for cardiorespiratory fitness among physicians and found that those who reported counseling less frequently about PA had higher resting heart rates (OR 3.4, CI 1.46-8.18).
The association between frequency of counseling and PA habits was found among nurses too. McDowell et al 75 observed a sample of nurses in the United Kingdom and found that there was a correlation between nurses categorized as “active” and their PA counseling frequency (r = .26, P < .001). Puig-Ribera et al, 76 in Spain, reported a positive association between active nurses and higher frequency of PA counseling (P < .05). Esposito and Fitzpatrick found a significant correlation between registered nurses’ PA habits and increased health promotion activities (including PA counseling) among their patients (r = .20, P = .03). 67 Connolly and colleagues found that 76% of nurses reported exercising regularly, and among those, 70% would recommend their lifestyle to their patients. 63
Some studies among nursing and medical students show that even early in their training, there is an association between HCPs’ personal lifestyles and what they will preach in their future clinical practice. Frank et al showed, as part of the “Healthy Doctor = Healthy Patient” project, in a cross-sectional sample of 17 US medical schools, that first-year students who reported more vigorous exercise had a more positive attitude toward counseling for exercise in their future practice. 57 Students were followed-up for 4 years and it was found that those who complied with the PA guidelines were more likely to rate exercise counseling as important (P = .04). 38 Additionally, more students thought exercise counseling was highly relevant for their future clinical practice at their entry-to-ward year than in their senior year (69% vs 53%, P < .01). Duperly et al 56 replicated some aspects of the “Healthy Doctor = Healthy Patient” study in a sample of Colombian medical students, and even though the association between higher PA levels and better attitudes toward PA counseling was not statistically significant, the association was found for other health habits (better diet, not smoking, non–binge drinking) and related counseling. Among a sample of nursing students in Spain, 55 a lower proportion of inactive students felt competent to prescribe PA (17.2%) compared with the proportion among active students (36.4%).
Patients Find Active HCPs’ Counseling More Compelling
From the patients’ perspective, HCP habits appear to be also influential. Harsha et al 62 surveyed patients from a University Family Practice Center and found that 70% of patients said they would be more willing to exercise if their physicians also exercised regularly (P < .01). Patients were also more willing to comply with exercise recommendations if the recommending physicians were a family practitioner or a cardiologist. Patients in this study who met the PA guidelines were more willing to comply with their physicians if he or she exercised (P < .05) and almost 85% of them were more willing to comply if their physicians gave them a written exercise prescription. Frank et al 73 showed 2 brief videos about improving diet and PA to a group of patients. In one video the physician disclosed information about his or her diet and exercise personal habits and included a bike helmet and an apple visible on their desk; in the second video, the physician did not disclose any personal habits (control video). Patients who viewed the physician-disclosure video considered the physicians to be healthier (P = .001), more motivating (P = .001), and more believable (P = .002) than those patients that were exposed the control video.
Perceived importance, success, or self-efficacy was also associated with HCPs’ own PA habits: nurses who rated PA as highly important for their practice also reported exercising more than those who rated it lower (P < .0003). 58 Two other studies found a significant association between providers who complied with the PA guidelines and increased confidence in counseling (P = .01) 68 and greater perceived success in counseling PA to their patients (r = .37, P = .007). 71
Discussion
This literature review is a comprehensive evaluation of HCPs’ PA levels, the counseling they give patients, and the influence HCPs’ own personal habits may have on their PA counseling practices. Similar to other preventive measures such as smoking cessation, alcohol consumption, diet improvement, regular health screenings, or vaccinations,69,74,77 the available evidence shows that physicians and HCPs’ personal habits are a key, independent correlate, and may predict the manner in which they counsel and influence their patients’ behaviors on related health habits. For example, physicians who do not smoke are more likely to encourage patients to quit smoking. 78 In a recent study 26 among 1488 primary care physicians and their adult patients (n = 1 886 791), 8 different screening and vaccination preventive practices were objectively assessed using electronic medical records. Patients whose physicians were compliant with the preventive practices were significantly more likely to also have undergone these preventive measures, than patients with noncompliant physicians. For example, among patients whose physician had received the influenza vaccine, 49.1% of eligible patients received flu vaccines compared with 43.2% of patients whose physicians did not receive the vaccine (5.9% absolute difference, 13.7% relative difference). Additionally, physicians who are trying to improve their health habits counsel significantly more and with more confidence on that specific habit than HCPs not attempting to improve their behaviors. 69 It has even been suggested 79 that physician wellness, including PA levels, should be routinely measured in health systems as a quality indicator. This review found evidence to support the hypothesis that physically active HCPs, including those in the process of becoming more active, are more likely to counsel more frequently and more confidently about the importance of PA to their patients. Therefore, efforts to improve HCPs’ PA habits may not only benefit their health, but may also be an avenue to improve the frequency and quality of PA preventive counseling that patients and the general population receive. Such an approach, coupled with established referral mechanisms for community PA opportunities, can be effective in helping reduce inactivity, the fourth leading cause of death globally. 5
Out of 24 analytic studies found in our review that examined the association between HCPs’ personal habits and counseling practices, 19 reported statistically significant positive associations. Despite the existence of prevailing barriers to PA counseling by HCPs and the fact that there are other factors associated with the frequency and quality of HCPs’ PA counseling to patients, 80 HCPs’ personal PA habits were found to be a consistent correlate of counseling. In studies that allowed a head-to-head comparison, a measure of the magnitude of this association (OR) was found to range between 1.4 and 5.7.* Furthermore, this association was reported for physicians versus other HCPs, practicing or in-training HCPs, in different countries, health care systems, and settings, suggesting that the connection between HCPs’ habits and their PA counseling practices is consistent. The extent to which provider-initiated PA counseling can be translated into behavioral change among patients is modest and opens opportunities to further research. However, physicians and other HCPs are in a privileged position to provide PA advice as they are one of the first and most trusted sources of health information for patients, and some studies have described patients’ willingness to change a health behavior if their provider has a healthier, active lifestyle. 73
There Is a Lack of Global Data on Rates of HCP PA Counseling, and When They Are Assessed, Rates Are Often Unacceptably Low
Evidence indicates that physicians report having better health habits than the general population, including slightly higher compliance with PA guidelines, although still far from optimal.17,81,82 This is important since active physicians can be role models for patients and be more credible and motivating to help them adopt or maintain an active lifestyle. However, and partly because of HCPs’ PA habits have room for improvement, PA counseling rates by HCPs still remain unacceptably low in many countries. For example, it is estimated that less than 40% of US primary care providers provide regular counseling on PA, even though PA counseling is a national health objective and many physician professional and scientific organizations recommend counseling on PA. 83 On the other hand, more information is needed on the PA habits of HCPs other than physicians. Some studies report that nurses are somewhat more active than the general population, but when compared with physicians, studies show they have poorer health habits and report more barriers to engage in PA.43,46 However, nurses do report being more motivated and are enthusiastic about counseling on PA, and they ranked exercise as an important strategy to address NCDs among their patients. 37 Of interest, RCTs that have been shown to be effective in improving PA levels via primary care–based PA behavioral counseling as part of the 2010 USPSTF review update, included interventions delivered mostly by health educators and physicians and in one study by nurses. These data emphasize the need to incorporate strategies to support all HCPs’ PA habits as part of interventions to improve PA counseling in primary care and referral schemes.
Many System and Personal Barriers Hinder HCP PA Counseling Efforts
Our literature search also explored HCPs’ perception of barriers to provide counseling, mainly lack of time and low self-efficacy. A recent systematic literature review 80 on the perceptions of providers show physicians and nurses rank PA counseling as very important and agree that they should be involved in counseling activities; however, lack of needed skills, training, time, and reimbursement are still noted as important barriers to provide counseling. A persistent finding among all HCPs is the low level of knowledge on basic PA guidelines for health and the lack of training on simple exercise prescriptions, despite global efforts to elevate the status of PA as key for the prevention and management of NCDs.84-86 These findings highlight the importance of critically assessing and improving the lifestyle medicine and health promotion curriculums of medical and health sciences schools globally. One approach that needs to be thoroughly evaluated could be to implement continuing medical education programs for physicians and other HCPs on the basics of PA counseling. On this end, initiatives such as Exercise is Medicine,87-89 which aims to make PA assessment (PA “vital sign”), prescription, and referral an integral part of medical practice in the United States and globally, have the potential to effect change if implemented at a large scale and in addition to other environmental and community approaches. 90 There is no “silver-bullet” to solve the global inactivity epidemic. An “all of the above” and “whole of society” approach, including PA counseling and referral in the health care context, will be required.91,92
PA Counseling Is Not Standardized Across Studies
The majority of the studies included in this literature review had limitations because of their self-reported nature. PA habits and counseling were generally assessed through self-reports and very few studies used objective measures for activity or PA counseling.55,64,93,94 Additional studies that validate HCPs’ self-reports on counseling practices, possibly cross-checking with medical records or patients’ perceptions, and objective measures of HCPs’ PA levels are needed in order to decrease bias due to the desirability of HCPs to score well in both categories. Another limitation is the heterogeneity with which many studies reported both PA levels and counseling attitudes and practices, which prevented a more quantitative approach to summarizing the evidence using meta-analytic techniques. Finally, there is risk of under-ascertainment of studies since the literature review focused only in one database published in English or Spanish.
Health care providers’ health is not only important for their own benefit but also because of the potential positive effects it may bring to their patients. This review found that HCPs may preach what they practice and those that are active are more likely to advice PA to their patients. Increasing PA levels among HCPs may be an additional intervention that, in addition to other public health and clinical strategies, may help reduce inactivity levels in the general population.
In conclusion, this review found consistent evidence supporting the notion that physically active physicians and other HCPs are more likely to provide PA counseling to their patients and can indeed become powerful PA role models. This evidence appears sufficient to justify randomized trials to determine if adding interventions to promote PA among HCPs, also results in improvements in the frequency and quality of PA preventive counseling and referrals, delivered by HCPs, to patients in primary care settings. Future studies should aim at objectively quantifying the effect of physicians’ PA role-modeling and how it influences PA in their patients. Specifically, whether promoting PA among HCPs can independently result in meaningful increases in the PA levels of patients, or potentiate the effect of interventions to address barriers for effective PA counseling in health care settings. The fact that our search identified only 2 studies from low- and middle-income countries, India and Colombia,52,56 is of concern and constitutes a call for further research in these settings, where 80% of the deaths due to inactivity and related NCDs occur. 95
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.