
Abstract
Medical authorities advise US adults to perform a minimum of 30 minutes of moderate-intensity aerobic physical activity on most days of the week to improve health and reduce risk for many chronic conditions. New findings from epidemiologic studies suggest that physical activity not only reduces the risk of developing coronary heart disease, stroke, and type 2 diabetes but also may prevent certain cancers (including colon and breast cancer), osteoporotic fracture, falls, cognitive decline, mood disturbances, and adverse pregnancy outcomes. Physical activity is important for regulating body weight, but many cardiometabolic benefits of exercise are independent of such regulation. This article reviews recent epidemiologic evidence on physical activity with respect to a variety of health outcomes in women and concludes with guidance for clinicians seeking to boost activity levels in sedentary patients. However, additional research is needed on features of individual- and community-based interventions and policies that successfully promote healthful levels of physical activity.
Keywords
‘According to a recent national survey, 50% of US women do not meet the basic guideline for aerobic activity, and 75% do not meet the strength-training guideline. Only 18% of women meet both guidelines’.
To improve health and reduce risk for certain chronic diseases, medical authorities, including the US Surgeon General, the American Heart Association, and the American College of Sports Medicine, have long advised that adults perform at least 30 minutes of moderate-intensity aerobic physical activity on most days of the week or, alternatively, vigorous-intensity physical activity for at least 20 minutes on 3 days of the week.1-3 Similarly, a 2008 statement issued by the US Department of Health and Human Services calls for at least 150 minutes/week of moderate-intensity physical activity or 75 minutes/week of vigorous-intensity physical activity for “substantial health benefits” (basic guideline) and 300 minutes/week of moderate or 150 minutes/week of vigorous-intensity physical activity for “additional and more extensive health benefits” (advanced guideline). 4 Current guidelines also call for strength training (resistance exercise) at least twice per week.4-6 A large proportion of US women do not get sufficient physical activity. According to a recent national survey, 50% of US women do not meet the basic guideline for aerobic activity, and 75% do not meet the strength-training guideline. 7 Only 18% of women meet both guidelines. 7
Intensity of aerobic exercise is typically measured as kilocalories (kcal) burned per minute of activity or in metabolic equivalents (METs), defined as the ratio of the metabolic rate during exercise to the metabolic rate at rest. Moderate-intensity activities, such as brisk walking (at a pace of ≥3 miles/hour), burn 3.5 to 7 kcal/minutes or expend 3 to 6 METs. Vigorous activities, such as running, burn >7 kcal/minutes or expend >6 METs. Researchers often characterize findings in terms of MET-hour (total volume)/week of physical activity, but because a MET-hour score can reflect activity performed for (a) for long duration at low intensity or (b) short duration at high intensity, such analyses cannot separate the influence of duration and intensity on health.
This article, which is an updated and abridged version of a previously published textbook chapter, 8 reviews current epidemiologic evidence on physical activity and health outcomes in women (Table 1), highlighting results of recent meta-analyses as well as studies of aerobic activity that present findings in a way that readily translates into public health recommendations regarding exercise for disease prevention—that is, studies that assess, say, walking (the most common leisure activity in US adults) for a certain number of hours per week as opposed to achieving a certain number of MET-hours per week, and studies that assess physical activity, a behavior, rather than physical fitness, an attained physiologic state. Although most epidemiologic studies to date have focused on aerobic rather than muscle-strengthening activities, selected findings regarding the latter type of exercise in relation to cardiovascular outcomes, bone health, and falls are also presented.
Effects of Physical Activity on Health. *
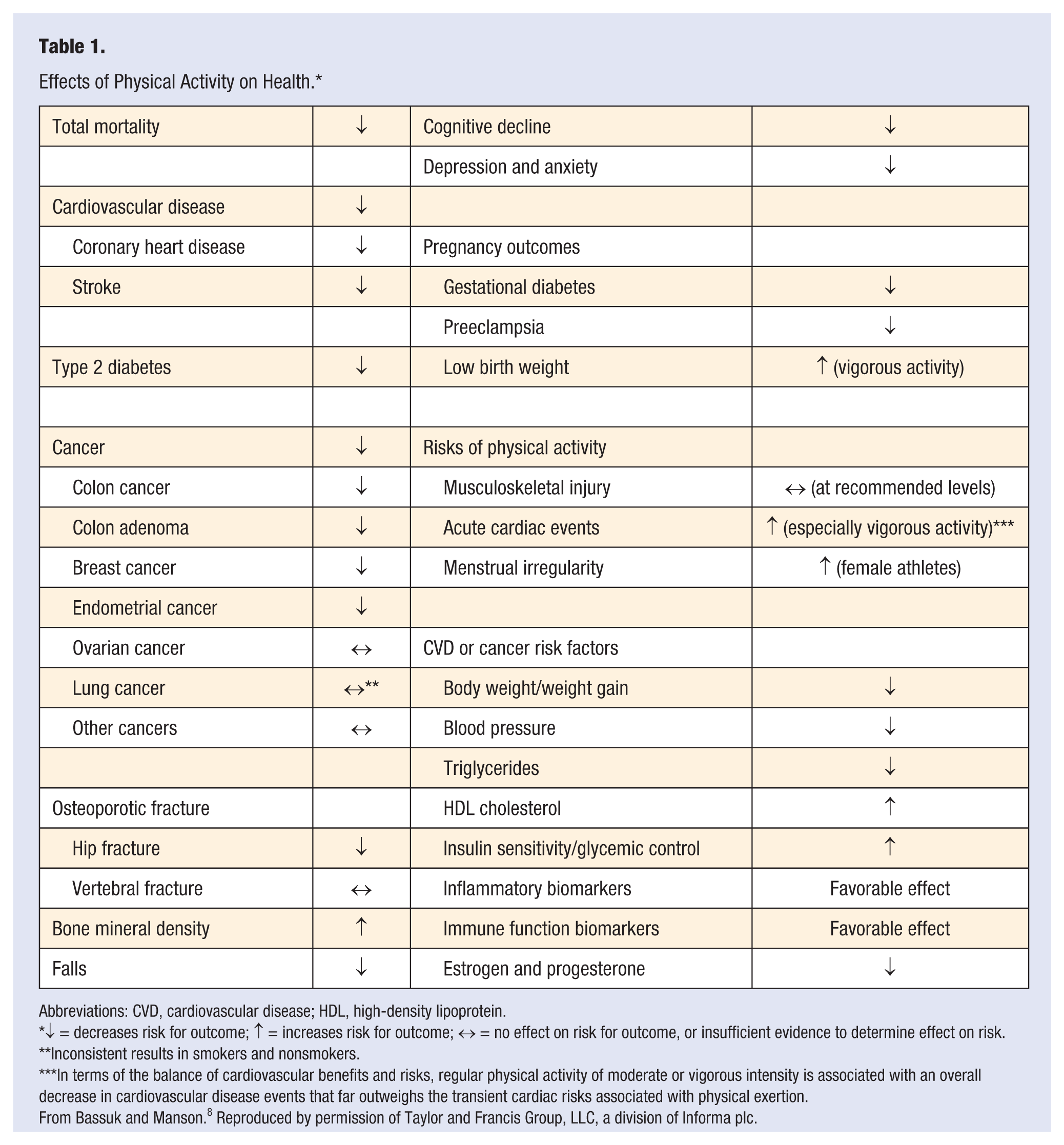
Abbreviations: CVD, cardiovascular disease; HDL, high-density lipoprotein.
↓ = decreases risk for outcome; ↑ = increases risk for outcome; ↔ = no effect on risk for outcome, or insufficient evidence to determine effect on risk.
Inconsistent results in smokers and nonsmokers.
In terms of the balance of cardiovascular benefits and risks, regular physical activity of moderate or vigorous intensity is associated with an overall decrease in cardiovascular disease events that far outweighs the transient cardiac risks associated with physical exertion.
From Bassuk and Manson. 8 Reproduced by permission of Taylor and Francis Group, LLC, a division of Informa plc.
Methodological Issues
Most epidemiologic investigations of physical activity in relation to disease risk have been observational studies rather than randomized clinical trials. In interpreting results of observational studies, various threats to validity must be considered: unmeasured or unknown factors may affect the selection and participation of study respondents (selection bias); unmeasured or unknown third factors may account for the association (confounding); flawed measures of physical activity or disease status may distort the findings (misclassification); respondents with physical inactivity, a putative risk factor for many conditions, may be more likely to receive screening for occult diseases such as diabetes or cancer and be diagnosed earlier than other respondents, leading to an overestimate of the strength of the exercise–disease relation (surveillance bias); and—in case–control studies—knowledge of one’s disease status may color one’s recall of prior physical activity (recall bias). Self-reported physical activity questionnaires—the typical method of physical activity measurement in epidemiologic settings—are not only imperfect measures of activity in the population overall but may also have differential accuracy in certain groups (eg, women vs men, or normal-weight vs overweight persons), causing artifactual interaction effects. However, for outcomes such as cardiovascular disease (CVD) and diabetes, the consistency of the main-effects results across studies—including studies that rely on exercise testing instead of questionnaires to assess exposure or, in the case of diabetes, on glucose tolerance or fasting glucose tests rather than self-reported diagnoses to assess outcome—supports a causal association, as does the biologic plausibility due to the known salutary effects of increased physical activity on cardiometabolic risk factors, many of which have been demonstrated in small randomized trials. On a related note, many studies, in an effort to minimize confounding, statistically correct for the effect of baseline characteristics such as hypertension, dyslipidemia, and glucose tolerance. However, because such factors are physiologic links in the causal pathway between physical activity and cardiometabolic disease, this strategy may unintentionally attenuate the strength of the association.
Mortality
A systematic evidence review conducted to inform the 2008 federal physical activity guidelines found a 30% risk reduction in total mortality in persons who were the most active compared with the least active. 9 Larger risk decreases occurred at the lower end of the activity spectrum than at the upper end. Compared with <0.5 hour/week, there was a reduction of ~20% in mortality from 1.5 hours/week of moderate to vigorous activity, and a further 20% reduction for an additional 5.5 hours/week (ie, a total of 7 hours/week) of activity.
A 2011 meta-analysis of 22 cohort studies with a total of 643 000 women and 335 000 men quantified the relation between moderate-intensity activity and mortality. 10 Compared with inactive adults, those who performed 2.5 hours/week of moderate activity (equivalent to 30 minutes/day on 5 days/week) experienced a 19% (95% confidence interval, 15% to 24%) reduction in mortality risk, and those who performed 7 hours/week of light and moderate activity reduced their risk by 24% (19% to 29%). Five studies in this meta-analysis analyzed walking specifically and found an 11% (4% to 18%) reduction in mortality risk for 2.5 hours/week of brisk walking compared with no walking. A 2008 meta-analysis of 10 prospective studies with a total of 106 000 women and 39 000 men found a stronger effect for walking; there was a 20% (9% to 29%) reduction in mortality risk associated with an exposure approximately equivalent to walking 3 hours/week at a normal pace (3 km/hour [1.9 miles/hour]), with the relation similar in women and men. 11
A 2012 analysis of data from 6 US cohorts with a total of 655 000 adults followed for a median of 10 years supports the idea that even minimal levels of physical activity can extend the lifespan. 12 Compared with their inactive peers, women who reported a low amount of leisure-time physical activity—an activity level of up to 75 minutes/week (~11 minutes/day)—had a 2.1-year (1.7-2.5) longer life expectancy after age 40. Women with a physical activity level at or just above the 30 minutes/day recommendation had additional gains in life expectancy (3.6 years [3.1-4.0]), while women with an activity level of 60 to <90 minutes/day experienced further gains (4.0 years [3.4-4.6]). The dose–response gradient was curvilinear, with the largest gains from the first hour or so of weekly exercise. Significant increases in life expectancy with even minimal activity were also observed in men, in both whites and blacks (findings for other racial/ethnic groups were not given), and across body mass index groups.
Amount of time spent sitting (such as in front of the TV or at work) has recently been implicated as a risk factor for mortality independent of amount of physical activity. For example, a 14-year follow-up of 70 000 women and 53 000 men aged 50 to 74 in the American Cancer Society’s Cancer Prevention Study II (CPS-II) Nutrition Cohort found that physical activity level and time spent sitting independently predicted mortality in both sexes. 13 For women with total physical activity of <17.5 (bottom decile), 17.5 to <24.5, 24.5 to <31.5, 31.5 to <42, 42 to <52.5, 52.5 to <63, and ≥63 MET-hours/ week, relative risks (RR) were 1 (referent), 0.98, 0.81, 0.78, 0.76, 0.75, and 0.73 (P, trend <.0001). Each categorical increase in the exposure is equivalent to ~3 hours/week (25 minutes/day) of light-intensity activity, which suggests that an increase of 1 hour/day of such activity reduces mortality risk in women by 19%. Daily sitting time was also predictive of mortality in both sexes, although the relation was stronger in women (for ≥6 vs <3 hours/day, RR = 1.37) than in men (RR = 1.18) (P, heterogeneity = .003). The relations remained “virtually unchanged” after adjustment for physical activity. The RR for the joint effects of sitting and physical inactivity (≥6 hours/day sitting and <24.5 MET-hours/week of physical activity) were 1.94 and 1.48 in women and men, respectively, compared with their counterparts who reported both sitting the least (<3 hours/day) and being the most physically active (≥52.2 MET-hours/week). A recent analysis of 5 long-term cohort studies, including the CPS-II, suggests that life expectancy in the United States would be 2.0 years higher if adults reduced their time spent sitting to <3 hours/day and 1.4 years higher if they reduced TV viewing to <2 hours/day. 14
Cardiovascular Disease
Of the many studies that have examined the relation between physical activity and CVD, most have focused on total major cardiovascular events (coronary heart disease [CHD], stroke, angina, coronary revascularization, heart failure, etc) or on CHD specifically. The findings support the prescription of either vigorous or moderate-intensity physical activity for cardiovascular benefit in sedentary women. 15
Among 73 000 postmenopausal participants aged 50 to 79 in the Women’s Health Initiative Observational Study, walking briskly for ≥2.5 hours/week (eg, 30 minutes 5 times/week) was associated with a 30% reduction in major cardiovascular events over a 3-year follow-up. 16 After controlling for total exercise energy expenditure, brisk walking and more vigorous exercise were associated with similar risk reductions in CVD events, and the results did not vary substantially by race, age, or baseline body mass index (BMI; Figure 1).
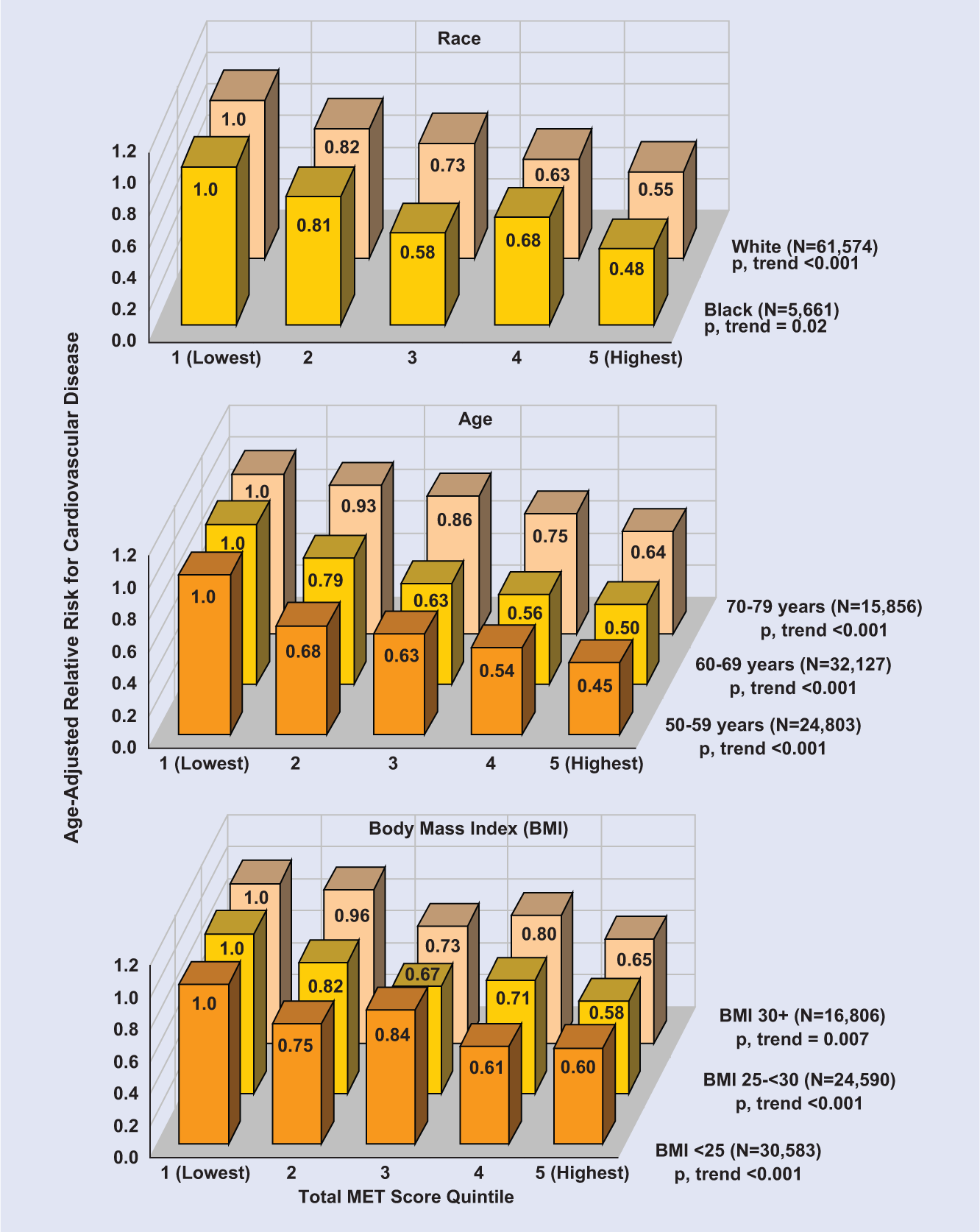
Age-Adjusted Relative Risks for Cardiovascular Disease According to Quintile of Energy Expenditure From Recreational Activities in Subgroups Defined by Race, Age, and Body Mass Index, Women’s Health Initiative.
A 2011 meta-analysis of data from nine prospective studies that quantified the dose-response relation between leisure-time physical activity and CHD found that that persons who met the federal government’s basic guideline had a 14% (4% to 23%) lower risk for this outcome than those who engaged in no activity, whereas those who met the advanced guideline had a 20% (12% to 26%) lower risk. 17 There was a significant interaction by sex. Women who met the basic guideline were at 20% (8% to 31%) lower risk than those who engaged in no leisure-time activity, whereas women who met the advanced guideline were at 28% (17% to 37%) lower risk. For men who met the basic and advanced guidelines, respectively, the RR were 0.91 (0.79-1.04) and 0.82 (0.74-0.91). The weaker association in men may be because their background physical activity levels are typically higher than women’s.
Several studies have examined walking as a predictor of CHD risk. For example, in an 8-year follow-up of 72 000 healthy female nurses aged 40 to 65 in the Nurses’ Health Study, 3 hours/week of brisk walking had the same protective effect on the heart as 1.5 hours/week of vigorous exercise. 18 Women reporting either type of exercise were 30% to 40% less likely to develop myocardial infarction than their sedentary peers. Among 39 000 healthy female health professionals aged ≥45 followed for 7 years in the Women’s Health Study, walking ≥1 hour/week was associated with a 50% reduction in CHD risk among participants reporting no vigorous physical activity. 19
Resistance exercise may lower risk for CHD. 5 For example, among 44 000 men aged 40 to 75 in the Health Professionals Follow-up Study, those who trained with weights for ≥30 minutes/week were 23% less likely to develop CHD during an 8-year follow-up than those who did not train with weights. 20 However, additional research is needed to confirm a protective effect, particularly in women. 5
With respect to stroke, findings from prospective studies suggest that aerobic physical activity reduces risk for this outcome, although the data are less extensive and consistent than those for CHD.21,22 A 2012 meta-analysis of 6 cohorts followed from 8 to 32 years found that moderately active and highly active women were 11% (0% to 21%) and 22% (8% to 34%) less likely to have a stroke than were women with low activity. 22 The meta-analysis included data from the Nurses’ Health Study and the Women’s Health Study. In the Nurses’ Health Study, the most active women were only half as likely to suffer an ischemic stroke during 8 years of follow-up as their least active counterparts; physical activity had little effect on hemorrhagic stroke. 23 In the Women’s Health Study, women who walked ≥2 hours/week had a 30% lower risk for stroke and women whose usual walking pace was brisk had a 37% lower risk for stroke during a 12-year follow-up compared with women who did not walk; protective associations were observed for both ischemic and hemorrhagic stroke, although they were significant only for the latter outcome. 24 Vigorous physical activity was unrelated to stroke risk in this cohort.
Other findings of note are as follows. Time spent sitting, independent of physical activity, has been significantly associated with CVD incidence or CVD mortality in several studies.13,16,25-27 In the Women’s Health Initiative, women who spent ≥16 hours/day sitting were 68% more likely to develop CVD than those who spent <4 hours/day sitting. 16
Short bouts of activity (10-15 minutes) favorably affect the cardiovascular risk profile of otherwise sedentary persons. 28 One prospective study in men has examined the relation between brief bouts of exercise and clinical CVD. After controlling for total energy expenditure, exercise sessions lasting 15, 30, or 45 minutes offered equal protection against incident CVD in a cohort of 7307 middle-aged and elderly Harvard alumni followed for 5 years. 29 Incorporating such findings into public health messages may help convince busy individuals to treat exercise as a manageable part of their daily routine rather than as a time-consuming activity reserved for rare occasions.
Becoming physically active during mid- or late life offers cardiovascular benefits. For example, among initially sedentary participants in the Nurses’ Health Study, 6-year changes in activity level were significantly associated in dose–response fashion with CHD incidence during the subsequent 8 years. 18 Compared with women who remained sedentary, women with increasing quintiles of total physical activity energy expenditure were 15%, 21%, 33%, and 29% less likely to have a coronary event. Knowing that “it’s not too late” may motivate older individuals to become physically active.
Cardiorespiratory fitness as assessed by maximal treadmill exercise test is inversely associated with cardiovascular mortality in persons without coronary symptoms at baseline. A 2009 meta-analysis of data from 24 prospective cohorts with a total of >84 000 initially healthy participants and nearly 4500 CVD endpoints (primarily cardiovascular mortality) found a significant 15% decline in cardiovascular risk for each 1-MET increase in exercise capacity, with a similar benefit for women and men. 30
Physiologic variables favorably affected by physical activity include adiposity, insulin sensitivity, glycemic control, type 2 diabetes incidence (see below), blood pressure, lipids, endothelial function, hemostasis, and inflammatory defense systems. 15 These factors explained 59% of the observed inverse relation between physical activity and incident CVD over 11 years of follow-up in the Women’s Health Study. 31 Observational and randomized trial data show that habitual moderate-intensity aerobic activity is as effective as more vigorous activity in reducing blood pressure and improving insulin sensitivity. 15 In contrast, there are strong dose–response associations between exercise intensity and blood lipids—specifically, triglycerides and high-density lipoprotein cholesterol. 15 Resistance exercise also reduces blood pressure. 32 Two randomized trials in patients with type 2 diabetes found that a combination of aerobic and resistance exercise improved glycemic control more than either type of exercise alone.33,34 However, whether resistance exercise alone favorably affects other cardiovascular risk markers in patients with type 2 diabetes remains unclear. 35
Type 2 Diabetes
Prospective studies consistently show an inverse association between physical activity and risk for type 2 diabetes. A 2007 meta-analysis of 10 cohort studies with a total of 301 000 participants found that, compared with inactivity, habitual moderate-intensity activity predicted a 17% reduction (10% to 24%) in diabetes risk, after adjustment for BMI. 36 Among >70 000 participants followed for 8 years in the Nurses’ Health Study, brisk walking for at least 2.5 hours/week (30 minutes/day for 5 days/week) without any vigorous exercise was associated with a 25% reduction in diabetes risk. 37 Given equivalent total exercise energy expenditures, brisk walking and more vigorous exercise were associated with similar risk reductions. In the Women’s Health Study, participants who reported walking 2 to 3 hours/week were 34% less likely to develop diabetes during 7 years of follow-up than women who reported not walking. 38 In the Iowa Women’s Health Study, which tracked >34 000 participants aged 55 to 69 for 12 years, women engaging in moderate-intensity exercise 1, 2 to 4, and >4 times/week were 10%, 14%, and 27% less likely, respectively, to develop diabetes than women engaging in such exercise <1 time/week. 39 All of the above estimates reflect adjustment for the effects of BMI and other cardiometabolic risk factors; thus, they can be viewed as conservative estimates that exclude the risk reduction attributable to lower body mass from physical activity. As is the case for CVD, some data suggest that the inverse association between physical activity and diabetes risk may be stronger for women than for men, perhaps due to generally lower baseline activity levels for former as compared with the latter. 15
Cardiorespiratory fitness as assessed by bicycle ergometer or treadmill test also correlates inversely with incidence of type 2 diabetes. For example, in a 17-year follow-up of 6249 female participants in the Aerobics Center Longitudinal Study, the adjusted RR for diabetes across increasing tertiles of fitness were 1.0 (referent), 0.86 (0.59-1.25), and 0.61 (0.38-0.96). 40
Randomized trials provide strong evidence that regular physical activity can delay the onset of type 2 diabetes in high-risk populations.41-46 The largest such trial, the US Diabetes Prevention Program, randomly assigned 3234 overweight adults with impaired glucose tolerance to 1 of 3 groups—a diet and exercise program, the drug metformin, or placebo—and found a 58% reduction in risk for diabetes associated with the lifestyle intervention (vs placebo) after 3 years of follow-up, 44 with benefits observed in both sexes and in all age, racial/ethnic, and BMI groups. On average, participants in the lifestyle modification group performed moderate-intensity exercise for 150 minutes/week and lost 5% to 7% of their body weight. (The metformin vs placebo comparison yielded a 31% risk reduction.) A 10-year follow-up, in which all participants were offered lifestyle intervention and metformin was continued in the metformin group, found that, although incidence rates of diabetes were similar in the 3 groups during follow-up, the cumulative incidence remained lowest in the original lifestyle group. 45
A meta-analysis of 17 randomized trials with a total of 8084 participants followed for a mean of 4 years—12 trials evaluated lifestyle interventions, mainly weight loss and exercise; 12 trials evaluated diabetes medications; and several trials evaluated both—found a summary RR for developing diabetes of 0.51 (0.40-0.60) with lifestyle intervention and 0.70 (0.62-0.79) with oral diabetes drugs. 47
Prospective studies have found that walking (or more vigorous physical activity) is predictive of reduced CVD incidence or CVD mortality among persons with type 2 diabetes. For example, among Nurses’ Health Study participants with diabetes who reported no vigorous exercise, the 14-year RRs for incident cardiovascular events across increasing quartiles of walking energy expenditure were 1.0 (referent), 0.85, 0.63, and 0.56, after adjustment for BMI and other covariates. 48 Among 5859 adults with diabetes followed for a median of 9 years in the European Prospective Investigation into Cancer and Nutrition, walking 2 to 4.5 hours/week was associated with a 46% reduction in CVD mortality as compared with walking less than 2 hours/week. 49 Recent meta-analyses of diabetic cohorts report risk reductions of 29% (16% to 40%) 50 for CVD incidence (12 cohorts) and 37% (17% to 52%) 49 for CVD mortality (5 cohorts) for persons in the highest versus lowest physical activity category. However, results of randomized trials of exercise for CVD reduction in patients with diabetes have been mixed. An 8-year randomized trial among 160 Danish adults that included 30 minutes of brisk walking 3 to 5 times/week as part of a multifaceted, intensive approach to managing diabetes found a 53% reduction in CVD events compared with conventional treatment. 51 The 8-year Japan Diabetes Complications Study among 2033 patients found that an intensive lifestyle intervention that included counseling on physical activity, diet, and medication adherence lowered the risk for stroke but not CHD (at 5 years, the intervention group scored significantly higher than the usual-care group on an index of sports activities but not leisure or work-related physical activities). 52 In the United States, the 11-year Look AHEAD (Action For Health in Diabetes) trial among 5145 obese adults with diabetes found no effect on CVD risk of an intensive lifestyle intervention to promote weight loss through decreased caloric intake and exercise, despite greater weight loss in the intervention group. 53
Cancer
To prevent cancer, the American Cancer Society recommends at least 30 minutes of moderate to vigorous physical activity on ≥5 days of the week but notes that 45 to 60 minutes are preferable. 54 The World Cancer Research Fund and the American Institute for Cancer Research also recommend moderate physical activity for at least 30 minutes every day but state, “As fitness improves, aim for 60 minutes or more of moderate, or for 30 minutes or more of vigorous, physical activity every day.” 55
Although some investigators report inverse associations between physical activity and total cancer incidence or mortality,56-58 most have focused on site-specific cancers. To date, evidence for a protective effect of physical activity is most convincing for colon, breast, and endometrial cancer. Data from observational studies and small randomized trials suggest that physical activity may prevent cancer by reducing risk for obesity and favorably affecting circulating levels of sex hormones, insulin, and inflammatory cytokines, as well as immune function and apoptosis.59-61 Other potential protective mechanisms include decreases in insulin-like growth factors, favorable changes in prostaglandin profile, strengthened DNA repair systems, increased gut motility and shortened intestinal transit time for potential carcinogens (colon cancer), and improved pulmonary function and reduced exposure time between lung tissue and carcinogens (lung cancer). 60 However, the mechanistic evidence is not definitive, and more research is needed to clarify the biologic pathway or pathways linking physical activity and cancer.
With respect to colon cancer, a 2009 meta-analysis of 28 cohort and 24 case–control studies reported a summary RR of 0.76 (0.72-0.81) comparing the most with the least active individuals, with similar reductions for women and men. 62 However, the cohort studies showed smaller risk reductions (RR = 0.83) than the case–control studies (RR = 0.69), perhaps because of recall bias in the latter. Moreover, the risk reduction in the cohort studies was smaller in women (RR = 0.89) than in men (RR = 0.81), perhaps because of sex differences in the absolute physical activity levels being compared. Women typically engage in less physical activity than men, and higher amounts may be necessary for colon cancer prevention.
The meta-analysis did not quantify the amount of physical activity associated with the observed colon cancer risk reductions. Some authorities believe that at least 30 to 60 minutes/day of moderate to vigorous activity may be required to yield significant benefit.4,54 For example, in a 16-year follow-up of 79 000 Nurses’ Health Study participants, there was a 23% risk reduction comparing the most with the least active women (RR = 0.77 [0.58-1.01]). 63 The most active women expended >21.5 MET-hours/week in leisure-time physical activity (equivalent to brisk walking for ~5-6 hours/week), whereas the least active expended <2 MET-hours/week (equivalent to brisk walking for 0.5 hour/week). However, among women whose only reported activity was walking, there was a 31% risk reduction in those who walked 1 to 1.9 hours/week (RR = 0.69 [0.47-1.03]) compared with those who did not walk, with little additional benefit for more time spent walking (Figure 2A). A faster walking pace was also associated with reduced risk (very brisk vs easy walking pace: RR = 0.43 [0.17-1.05]). Among women who participated in moderate or vigorous activity other than walking, those exercising >4 hours/week had a 44% lower risk for colon cancer than those exercising <1 hour/week, with a significant dose–response relation (P, trend = .01) (Figure 2B). On the other hand, in the CPS-II Nutrition Cohort, walking alone (in the absence of other recreational physical activity) was not significantly related to colon cancer risk during 6 years of follow-up, 64 although a protective association was observed for those who reported walking plus other recreational activity. For women, the RRs for <4, 4 to 6, and ≥7 hours/week of activity versus no activity were 0.99 (0.67-1.47), 0.72 (0.43-1.19), and 0.59 (0.36-0.98) (P, trend = .07).
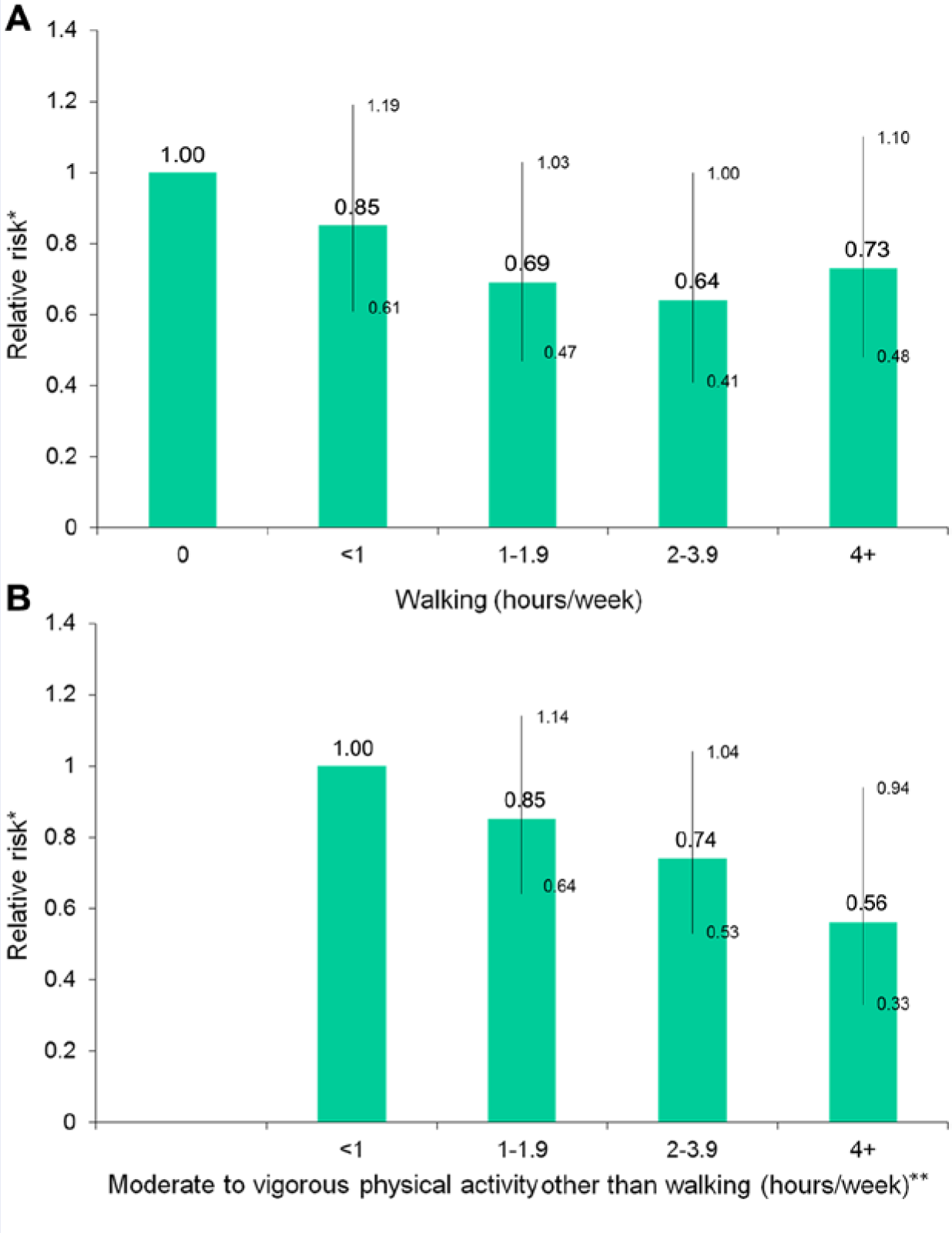
(A) Relative Risk for Colon Cancer According to Hours per Week Spent Walking. (B) Relative Risk for Colon Cancer According to Hours per Week Spent in Moderate to Vigorous Activity Other Than Walking. Nurses’ Health Study, 1986-2002.
Recent meta-analyses indicate that physical activity appears to confer similar protection against both proximal and distal colon cancers 65 and also to protect against the development of colon adenoma, 66 the precursor lesion that is detected and removed during sigmoidoscopy or colonoscopy.
For breast cancer, a 2011 systematic review of 33 cohort and 40 case–control studies found an average risk reduction of 25% when comparing the most active with the least active women, with a stronger effect in the case–control (average risk reduction, 30%) than in the cohort studies (average risk reduction, 20%). 67 Some but not all studies suggest a more pronounced benefit among women who are past menopause, of normal weight (BMI < 25 kg/m2), parous, and who have no family history of breast cancer. In many studies, statistically significant risk reductions in breast cancer have been seen only for women with at least 4 to 7 hours/week of moderate to vigorous physical activity. For example, among 95 000 Nurses’ Health Study participants followed for 20 years, women with ≥27 MET-hours/week of activity (equivalent to ~1 hour/day of brisk walking) during follow-up were 15% less likely to develop postmenopausal breast cancer than those with <3 MET-hours/week of activity. (Also, inactive women who stepped up their activity level after menopause were less likely to develop breast cancer than women who remained inactive.) However, in other studies, a lower activity level has also been associated with reduced risk. For example, among 74 000 Women’s Health Initiative participants followed for 4.7 years, women with 5.1 to 10 MET-hours/week of physical activity (equivalent to 1.25-2.5 hours/week of brisk walking) at the start of the study had an 18% risk decrease compared with inactive women, while women who exercised >40 MET-hours/week (equivalent to >10 hours/week of brisk walking) had only a slightly greater reduction in risk. 68
For endometrial cancer, a 2010 meta-analysis of 9 prospective cohort studies reported a summary RR of 0.73 (0.58-0.93) for a comparison of women with the most versus the least leisure-time physical activity. 69 Despite the fact that obesity is a strong risk factor for endometrial cancer, adjustment for BMI produced only a small change in the estimate (RR = 0.78 [0.63-0.95]). Some reviewers have suggested that ~1 hour/day of moderate-intensity activity reduces the risk for endometrial cancer. 60 However, results of large prospective studies published in recent years (2008 or later) have been equivocal regarding the level of intensity required for significant benefit. In a 7-year follow-up of >109 000 women in the NIH-AARP Diet and Health Study, vigorous physical activity predicted a reduced risk after adjustment for BMI and other potential confounders (≥5 times/week for ≥20 minutes vs never/rarely: RR = 0.77), but light/moderate, daily routine, and occupational physical activity did not. 70 In a 9-year follow-up of >32 000 Women’s Health Study participants, women reporting any vigorous activity had lower risk than those reporting none (BMI-adjusted RR = 0.74, with no trend of declining risk with increasing energy expended in such activities), but walking was unrelated to risk. 71 In a 10-year follow-up of >42 000 women in the CPS-II Nutrition Cohort, recreational physical activity of primarily low to moderate intensity was associated with lower risk in analyses unadjusted for BMI (≥31.5 vs <7 MET-hours/week: RR = 0.67 [0.44-1.03]; P, trend = .007), but adjustment for this variable weakened the association (RR = 0.79 [0.52-1.22]; P, trend = .18). 72
Whether physical activity plays a role in the prevention of ovarian cancer is uncertain. A 2007 meta-analysis of 6 cohort studies of recreational physical activity reported a nonsignificant 19% risk reduction for the most versus least active women. 73 However, results from several large prospective studies published since completion of this meta-analysis do not support a protective effect.74-77 Indeed, data from one such study, the NIH-AARP Diet and Health Study, 77 suggest that vigorous activity is linked to an increased risk for ovarian cancer, a finding also noted in 2 earlier studies, the Iowa Women’s Health Study 78 and the Nurses’ Health Study. 79 A plausible physiologic explanation remains elusive. With respect to lung cancer, studies that have stratified results by smoking status have tended to find either no effect or a much smaller protective effect of physical activity on lung cancer risk among never smokers than among current/former smokers. 80 Because smoking is such a strong determinant of lung cancer, it is likely that residual confounding by this variable accounts at least in part for the protective effect in the latter group. Physical activity does not appear to be related to risk for rectal cancer. 60 More data are needed to determine whether physical activity reduces risk for pancreatic, esophageal, kidney, bladder, cervical, and hematological cancers. 60
Bone Health and Falls
Osteoporosis is characterized by rapid loss of bone density after menopause that greatly increases risk for fracture. Physical activity may protect against osteoporotic fracture by strengthening bone (weight-bearing aerobic and resistance exercise) and preventing falls (resistance, balance, and flexibility exercise). A 2011 meta-analysis of 43 small, short-term randomized trials designed to assess the effect of exercise on bone mineral density in postmenopausal women reported that interventions that used a combination of exercise types slowed loss of bone density at the spine by a statistically significant 3.2% and that exercise interventions of any type slowed loss of bone density at the hip by a statistically significant 1.0%. 81 The size of these effects is of questionable relevance for fracture prevention. 82 However, risk for fracture is also a function of risk for falls. A 2008 meta-analysis of 12 trials of exercise (primary balance and strength training) to prevent falls in community-dwelling older persons reported a 29% (18% to 39%) reduction in risk. 9 An earlier meta-analysis of 8 randomized trials found a marginally significant 10% reduction in risk for falls associated with general exercise and a significant 17% reduction associated with balance training but no significant effect of aerobic, resistance, or flexibility training. 83
Observational data show stronger links between physical activity and reduction in hip fracture risk than might be expected based on the above findings. In a 2008 meta-analysis of 13 prospective studies, women reporting moderate to vigorous physical activity were 38% (31% to 44%) less likely to suffer hip fracture than women who were inactive; the corresponding statistic for men was 45% (31% to 56%). 82 Among >61 000 postmenopausal Nurses’ Health Study participants followed for 12 years, each increase of 3 MET-hours/week of activity (equivalent to 1 hour/week of walking at an average pace) was associated with a statistically significant 6% reduction in risk for hip fracture. 84 Among women who reported no other exercise, walking for ≥4 hours/week was associated with a 41% lower risk for hip fracture compared with walking <1 hour/week. Research on other fracture sites is limited but suggests that physical activity has little effect on vertebral fracture and increases the risk for wrist and other upper-limb fractures. 82 Randomized trials with fracture as a primary endpoint are lacking. The aforementioned meta-analysis of 43 trials of exercise and bone mineral density found a nonsignificant reduction in fracture risk (odds ratio [OR] = 0.61 [0.23-1.64]), but most trials were not powered to detect this endpoint. 81
Cognitive Decline
Habitual physical activity is associated with better cognitive function in many cohorts of older persons.9,85 For example, among Nurses’ Health Study participants aged 70 to 81, higher levels of long-term regular physical activity (average of biennial assessments occurring in the 8-15 years prior to cognitive testing) were predictive of better cognitive performance. 86 The apparent benefit for women in the highest versus lowest quintile of physical activity was similar in magnitude to that conferred by being ~3 years younger. A higher activity level was also predictive of less cognitive decline over the subsequent 2 years. The protective effect was not limited to vigorous exercisers; those who performed the equivalent of walking at an easy pace for ≥1.5 hours/week had better cognitive function than those who walked <40 minutes/week, with the magnitude of the difference equivalent to that observed for women ~1.5 years apart in age. Physical activity also appears to protect against dementia. A 2009 meta-analysis of 16 prospective studies reported a 28% (14% to 40%) reduction in risk for dementia and a 45% (16% to 64%) reduction in risk for Alzheimer’s disease for the most versus least active individuals. 87 In short-term randomized trials, exercise training yields improvements in certain cognitive processes, particularly executive function (the ability to complete tasks that require attention, organization, and planning). 88 Moreover, brain imaging trials have shown beneficial changes in brain activity 89 and volume 90 in aerobically trained older adults. Experiments in both young and old rodents demonstrate that exercise has favorable effects on cognition (water maze performance), neurogenesis, neurotransmitter systems, and expression of brain-derived neurotrophic factor (BDNF), 85 suggesting mechanisms by which physical activity may prevent cognitive decline. Physical activity also sustains brain vasculature via favorable effects on blood pressure, lipoprotein profile, insulin and glucose parameters, endothelial nitric oxide production, and cerebral perfusion. 86
Mood Symptoms
In an analysis of data from 28 prospective cohorts followed for an average of 4 years, the odds of experiencing elevated depressive symptomatology were 14% to 25% lower among physically active individuals compared with their inactive counterparts. 9 A benefit was observed not only for people meeting the basic physical activity guideline (OR = 0.77 [0.72-0.82]) but also for those who exercised at less than recommended levels (OR = 0.84 [0.78-0.90]). Physical activity appears to protect against clinical depression in prospective cohort studies. The relation between physical activity and anxiety is less well studied. However, in short-term randomized trials, physical activity reduces symptoms of depression and anxiety in healthy adults,9,91 nonpsychiatric medical patients,9,92 and patients with mood disorders.9,93,94 In addition to the improvements to BDNF described in the previous paragraph, exercise at moderate intensity fosters parasympathetic control95,96 and activates the endocannabinoid system,97,98 both of which promote relaxation and sense of well-being.
Pregnancy Outcomes
The American College of Obstetricians and Gynecologists advises that, in the absence of medical/obstetrical contraindications, pregnant women engage in ≥30 minutes of moderate-intensity physical activity on most days of the week. 99 It neither counsels for or against vigorous activity, for which information on pregnancy outcomes is sparse. Similarly, the 2008 federal physical activity guidelines state that, during pregnancy, “it is reasonable . . . to follow the moderate-intensity physical activity recommendations set for adults unless specific medical concerns warrant a reduction in activity.” 9 A 2011 meta-analysis of 5 prospective cohort studies, 2 retrospective case–control studies, and 2 cross-sectional studies concluded that physical activity before pregnancy (OR = 0.45 [0.28-0.75]) or in early pregnancy (OR = 0.76 [0.70-0.83]) was associated with a lower risk for gestational diabetes. 100 Observational and very limited animal and randomized trial data suggest that physical activity during pregnancy may also reduce risk for preeclampsia.101-104 Moderate-intensity activity during pregnancy does not appear to raise risk for early pregnancy loss, preterm delivery, or low birth weight; vigorous activity has been linked to small decreases (~200-400 g) in birth weight.102,103 Large randomized trials of the effect of physical activity on pregnancy outcomes are needed.
Regulation of Body Weight
Physical activity is important for weight control. In 2002, the Institute of Medicine recommended 60—rather than 30— minutes/day of moderate-intensity physical activity for weight maintenance. 105 In 2005, the Dietary Guidelines for Americans issued by the federal government included a recommendation for 60 minutes/day of physical activity to prevent weight gain and 60 to 90 minutes/day to sustain weight loss. 106 In 2009, the American College of Sports Medicine concluded that, in the absence of dietary change, 150 to 250 minutes/week of moderate-intensity activity appears effective for preventing weight gain but not for producing clinically significant weight loss, while >250 minutes/week appears necessary for clinically significant weight loss as well as for weight maintenance following weight loss. 107
Recent findings provide perspective. In the Women’s Health Study, physical activity was associated with less weight gain among normal-weight women (BMI < 25 kg/m2) but not among overweight (BMI 25 to <30) or obese women (BMI ≥ 30). 108 Women who were successful in maintaining a normal weight and gaining <2.3 kg over 13 years of follow-up averaged ~60 minutes/day of moderate-intensity activity throughout the study. On the other hand, in an 8-year follow-up of >46 000 women aged 25 to 43 in the Nurses’ Health Study II, physical activity for ≥30 minutes/day was associated with a significantly lower likelihood of weight gain of >5%, with the strongest effect in overweight women. Compared with women who maintained <30 minutes/day of physical activity over 8 years, women were ~33% less likely to gain weight if they sustained or increased to ≥30 minutes/day. However, even a small activity increase (11-20 minutes/day) in sedentary women appeared beneficial. There was also no threshold above which physical activity was unrelated to weight gain. Indeed, the amount of daily discretionary physical activity needed to eliminate, not just reduce, the risk for weight gain in normal-weight, overweight, and obese women was estimated to be 1.6 hours, 1.5 hours, and 45 minutes, respectively. 109 Also, women who had intentionally lost >5% of their body weight in the previous 2 years were less likely to regain >30% of the lost weight during the subsequent 6 years if they maintained ≥30/day of physical activity (OR = 0.69) or increased to this level (OR = 0.48) than if they remained inactive. 110
Emphasizing weight control—though a desirable goal—as the primary reason for performing physical activity may undercut motivation to exercise and also gives an incomplete picture of exercise’s effect on health. In many studies, including the Nurses’ Health Study, 111,112 physical activity remains inversely related to risk for cardiometabolic disease after factoring out the influence of BMI (Figure 3).
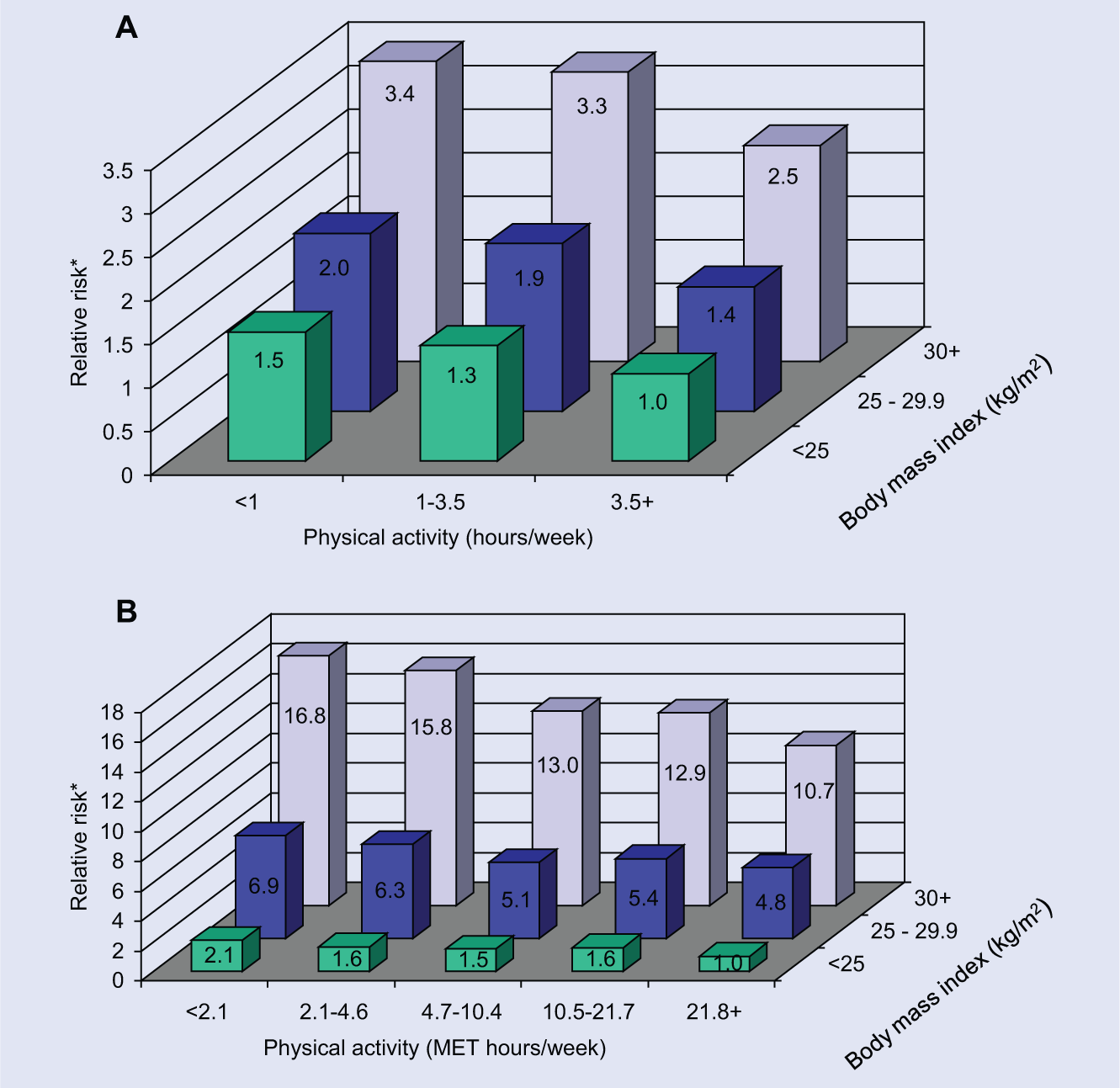
(A) Relative Risk for Coronary Heart Disease According to Body Mass Index and Physical Activity Level, Nurses’ Health Study, 1980-2000. (B) Relative Risk for Type 2 Diabetes According to Body Mass Index and Physical Activity Level, Nurses’ Health Study, 1986-2002.
Risks of Physical Activity
Physical activity confers risks as well as benefits. Although a person who engages in habitual moderate physical activity at recommended levels is generally at low risk for musculoskeletal injury, this risk rises with the rate of increase in one’s usual amount of activity. 9 Gradual increases allow for bodily adaptation. Safely attaining a desired activity level may require up to a year, especially for sedentary, older, or obese persons. 9 After adjustment for sex differences in activity and fitness levels, women and men are equally susceptible to most types of activity-related injuries—exceptions are stress fractures and injuries to the anterior cruciate ligament of the knee, which occur more often in females. 9
Popular belief holds that physical exertion can precipitate acute cardiac events, and available epidemiologic data confirm that belief. 113 However, the absolute risk associated with a bout of moderate or vigorous physical activity is low—on the order of 2 to 3 additional myocardial infarctions and 1 additional sudden cardiac death per 10 000 person-years of exercise—and is even lower in people who are habitual rather than sporadic exercisers. 113 It is important to recognize that regular activity of moderate or vigorous intensity is associated with an overall decrease in CVD events that far outweighs transient heart risks associated with sporadic exertion. 9
Research on the connection between physical activity and menstrual irregularities has focused on competitive athletes. Indeed, the term female athlete triad was coined 20 years ago to describe the co-occurrence of eating disorders, amenorrhea, and osteoporosis in such women. 114 Women engaged in sports that place a premium on leanness (eg, ballet, gymnastics, and distance running) are particularly susceptible to the condition, which suggests that restricted caloric intake insufficient to balance high exercise energy expenditure plays a role. 115
Conclusion
The epidemiologic findings reviewed in this article suggest that performing 30 minutes/day of habitual physical activity of moderate intensity reduce risk for a wide variety of chronic conditions among sedentary women. Accumulating data also suggest that sitting for extended periods of time adversely affects health. Given the high prevalence of physical inactivity in the United States, efforts by clinicians and policymakers to help patients and the general public achieve and maintain even modest activity levels and avoid prolonged sitting would be expected to translate into measurable improvements in health.
The proportion of North American physicians who routinely dispense advice about physical activity to their patients is unclear. One survey of primary care physicians in Canada found that 70% report doing so, 116 but surveys of patients in the United States suggest a figure closer to 30%.117,118 A perceived lack of time, training, and/or appropriate patient materials may dissuade physicians from initiating activity counseling. However, results of a multicenter trial suggest that clinicians can easily learn to add 3 to 4 minutes of physical activity advice into routine office visits 119 and that counseling can increase activity in sedentary patients. 120 In addition, many patient-friendly resources are now available online free of charge.121-123
Physicians who are uncertain how to incorporate brief counseling into daily practice may find a simple blueprint, including advice on writing exercise “prescriptions” (Table 2), to be helpful. 124 Interventions that encourage the incorporation of physical activity into daily life (eg, walking during lunch breaks, doing yard work or gardening, and taking the stairs rather than the elevator) may be more effective at first boosting and then sustaining activity levels—and improving cardiometabolic parameters—than structured exercise programs. 125 The use of self-monitoring strategies such as pedometers or exercise diaries can also help patients attain these goals. 126 In a sedentary society, identifying additional features of individual- and community-based interventions and policies that successfully promote healthful levels of physical activity over the long term should be a top research priority. 127
Possible Elements of a “Prescription” to Increase Physical Activity.
From Manson et al. 124