
Abstract
Changes in appearance and functional limitations of youth with chronic illness place them at greater risk for negative body image and poor psychosocial and medical outcomes compared with their healthy peers. Sociocultural pressures from the media, family, and peers, as well as social comparison processes to some extent explain the development of negative or positive body image in young people. This article discusses social theories applied to body image in young people with chronic illness, an overlooked population. A review of risk and protective factors of body dissatisfaction in this population and suggested treatment strategies/interventions in the prevention of body dissatisfaction are also considered. Reported findings may help health care providers become more aware of body image issues their young patients with chronic illness face, and posit the importance of regularly monitoring their psychosocial well-being in the efforts to curtail development of body dissatisfaction and consequential poor health outcomes.
‘A number of factors are thought to contribute to body dissatisfaction, including a combination of individual psychological characteristics, interpersonal interactions, and social influences.’
Body Image in Youth
Body image is a part of the concept of self, and this concept is formed from sensory and social experiences. An individual’s self-image is a reflection of a combination of both one’s own evaluation and perceptions of others’ attitudes toward a particular trait or characteristic.1,2 A person may have body dissatisfaction when there is a discourse between preferences for a body trait or characteristic that is different from how the body is currently perceived. During adolescence, an important developmental period where body and social changes occur, young people are increasingly vulnerable to body image disturbances which commonly involve body weight and shape dissatisfaction. Other body image concerns among girls and boys include physical and appearance attributes such as facial characteristics, skin appearance, muscularity, fitness, and strength.
The prevalence of body dissatisfaction continues to be high in both girls (24% to 46%) and boys (12% to 26%) and is a growing worldwide public health problem.3,4 An international report from the Health Behaviour in School-aged Children study of 43 countries found that by age 15 years, 40% of girls and 22% of boys were dissatisfied with their bodies. 5 Girls report wanting to be thinner than they are 6 while boys often report wanting to increase strength and muscle. 7 The high levels of body dissatisfaction among youth is troubling, given the risk for increased dieting for weight loss using unhealthy weight control behaviors 8 and negative psychological outcomes such as depression. 9
Theories of Body Image
A number of factors are thought to contribute to body dissatisfaction, including a combination of individual psychological characteristics, interpersonal interactions, and social influences.10,11 The sociocultural model has become a dominant theoretical framework for viewing body image. 12 In general, the sociocultural model contends that societal ideals of beauty are transmitted via a variety of sociocultural channels. These societal ideals are then internalized by individuals so that satisfaction or dissatisfaction with appearance is a function of the extent to which individuals do or do not match these standards. 12 Additionally, this model posits that perceived pressures concerning appearance from a variety of sociocultural channels such as media, family, and peers, leads to disordered eating through the internalization of cultural ideals and body dissatisfaction. 13
Internalization and appearance comparison, otherwise known as social comparison theory, play an integral part in the sociocultural model. Social comparison theory posits that individuals compare themselves with others “to determine their status or rank on certain appearance dimensions.”14(p179) Upward comparisons (ie, comparing oneself with others who are more attractive or thinner) may lead to body image dissatisfaction.15,16 It is important to note that not all individuals exposed to the societal ideal body (ie, thin and slender for women or muscular and fit for men) develop body dissatisfaction, but it has been suggested that some individuals have personality characteristics such as perfectionism, which may make them more susceptible to the sociocultural influences affecting body image. 14 Internalization of the thin or muscular ideal and social comparison15,17 are 2 characteristics that may be causal risk factors for the onset of body dissatisfaction. 18 Individuals who internalize the thin or muscular ideal endorse societal values to the point that this value becomes incorporated into their own belief system. 19 Thus, high internalizers buy into the societal norms of size and appearance 14 and are at greater risk for body image dissatisfaction. 19
Body Image Issues in Youth With Chronic Illness
Approximately 15% of children and adolescents have a chronic health condition 20 and may be at greater risk for developing negative body image than their healthy peers. 21 A recent meta-analytic study found that youth with chronic illness have less positive body image than their healthy peers. 21 In particular, comparisons by diseases showed that youth with cystic fibrosis, scoliosis, asthma, growth hormone deficits, spina bifida, cancer, and diabetes evaluated their bodies less positively than their healthy peers. 21 The body appearance changes and functional limitations that youth with chronic illness encounter may aid in the development of poor body image.
Appearance Changes
In many chronic illnesses, there are noticeable physical appearance changes such as pubertal delay, growth retardation, and weight gain. 22 It is common for adolescents with chronic illnesses to have a delay in growth and puberty, although it is more common in those where malnutrition and chronic inflammation are a factor (eg, cystic fibrosis, bowel disorders). 23 For example, cystic fibrosis patients commonly have observable changes to the body such as short stature, low weight, and pubertal delay because of their high risk of malnutrition due to maldigestion and malabsorption of food. 24 The body altering side effects from treatment medications such as insulin (eg, diabetes) and corticosteroids (eg, inflammatory bowel diseases) may also adversely affect body image. For instance, newly diagnosed type 1 diabetes patients may experience weight gain when placed on an insulin regimen (sometimes up to 10 pounds overnight), which could negatively affect body image and self-esteem. 25
Functional Limitations
The demands of managing a chronic illness and restrictions on life-style inherent in many disability conditions can influence social functioning. 23 For instance, youth with inflammatory bowel disease report they tend to perceive themselves negatively and differently than their peers (eg, “I’m thinner, pale, my hair is thinner. I don’t like how I look now. I look sickly”; “Everyone else is growing, but I’m shrinking”; “I want to be socially acceptable, but the medications make me break out and lose weight”; “They’ve name called me to death saying ‘fat girl’”). 26 Youth with visible appearance differences are also known to be at higher risk for experiencing stigmatization, 27 and thus, appearance-related teasing by peers may be detrimental to the development of positive body image. 28 In fact, a recent cross-sectional study found that young adults with bowel conditions were significantly more likely to recall being weight teased as a child and being more upset from the weight teasing insults than their healthy counterparts (V. Quick, R. McWilliams, C. Byrd-Bredbenner, unpublished data). At the same time, young adults with bowel conditions were also significantly more likely to have more mentally and physical unhealthy days, and depression and anxiety severity than their healthy peers (V. Quick, R. McWilliams, C. Byrd-Bredbenner, unpublished data).
Low school attendance and educational achievement from recurrent illness and demands of treatment regimens may occur. Youth with chronic illnesses are more likely than their healthy peers to miss school due to their condition or treatments needed. 29 For instance, youth with chronic arthritis have significantly higher school absence than the general population. 30 The school absences in youth with chronic arthritis are associated with decreased medical compliance and psychological disturbance. 30
Prevention of Body Dissatisfaction
Given youth with chronic illness are susceptible to body dissatisfaction 21 that can manifest to poor psychological outcomes, 9 it is prudent that health care providers and researchers take a preventive approach. The literature on protective factors of body dissatisfaction are mostly found in samples of healthy populations.10,11 However, research in some chronic illness populations has found protective factors of body dissatisfaction specific to those with chronic illnesses to include individual psychological characteristics, interpersonal interactions, and sociocultural influences (Table 1).
Summary of Risk and Protective Factors of Body Dissatisfaction in Youth With Chronic Illnesses a .
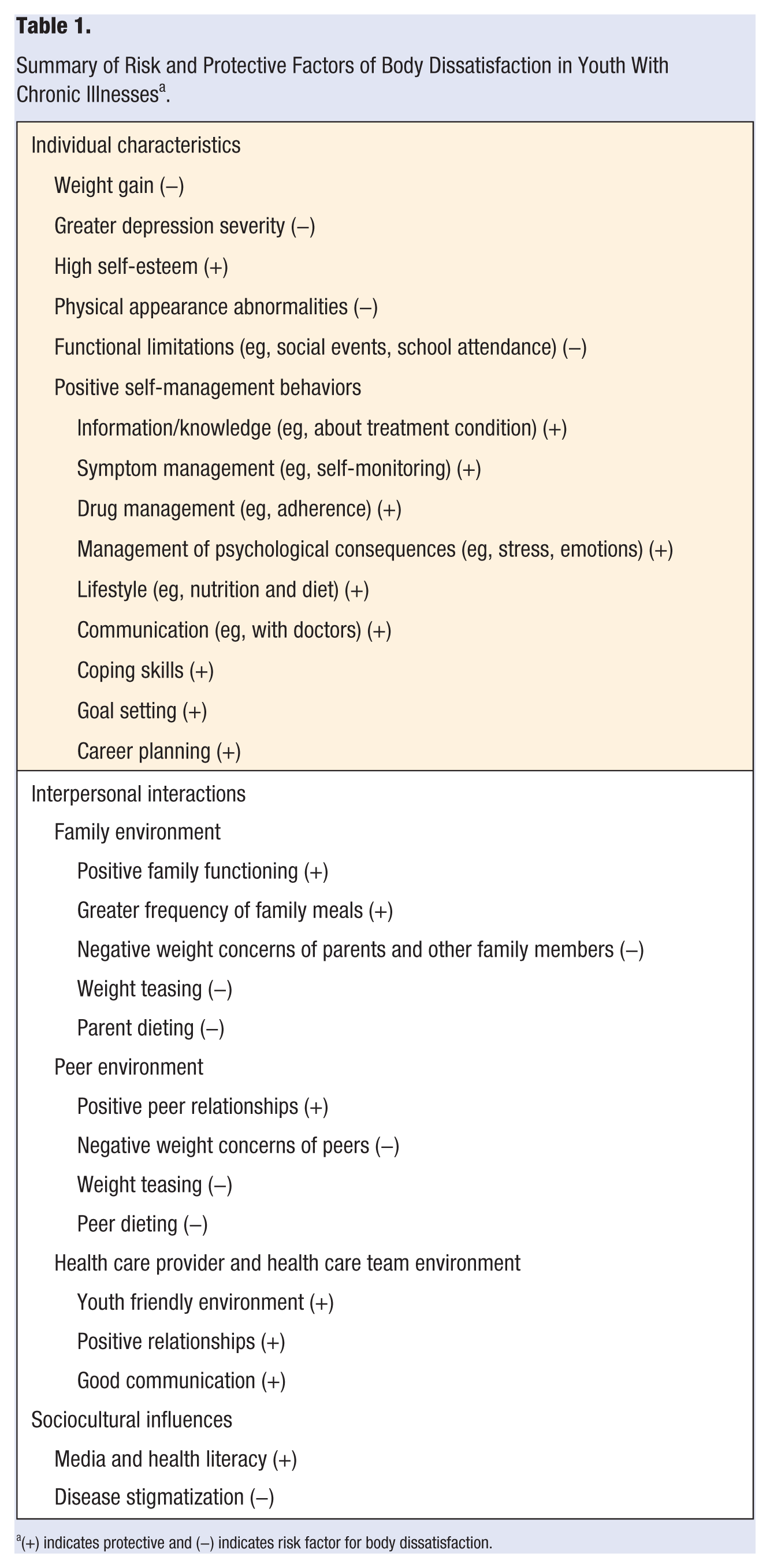
(+) indicates protective and (−) indicates risk factor for body dissatisfaction.
Individual Psychological Characteristics
Positive emotional and psychological well-being plays an important role in the management of any chronic condition, and thus should regularly be monitored by the health care team. 23 Indeed, psychosocial factors such as body image may negatively influence well-being beyond the influence of physical symptoms in patients with chronic illnesses such as inflammatory bowel disease. 31 Providing youth with coping skills may help in getting them to feel more confident (self-efficacy) in managing their chronic health condition, which in turn improves their self-image and outlook on life.
A growing body of evidence reveals that having the ability to self-manage one’s chronic illness is beneficial in terms of knowledge, performance of self-management behaviors, self-efficacy, and health status. 32 Self-management skills can include the following: information (eg, about treatment condition), symptom management (eg, self-monitoring), drug management (eg, adherence), management of psychological consequences (eg, stress, emotions, and disease acceptance), lifestyle (eg, nutrition and diet), communication (eg, with doctors), coping, goal setting, and career planning. 32 Moreover, youth with better self-management abilities may be protected from negative body image and consequentially poor health outcomes.
Interpersonal Interactions
Some parents of adolescents with a chronic illness may struggle with becoming too controlling of their adolescent’s disease and become overprotective, which can interfere with the adolescent’s individuation process. On the other hand, other parents may become uninterested in disease control and reject their adolescent as a consequence of ongoing arguments or as a result of their own emotional response to the disease. Having adequate family functioning is shown to improve both emotional well-being, and psychosocial and medical outcomes for adolescents who suffer from chronic illnesses. 33 A qualitative study of 30 female adolescents with type 1 diabetes found that family interactions around food and weight are common which can increase the risk of psychological problems such as disordered eating. 34 Findings from this same study suggest that frequent family meals may help to defend against body dissatisfaction and disordered eating in youth with type 1 diabetes. 34 Frequent family mealtimes may allow more time for parents to “check-in” with their child and provide emotional support when needed.
Adolescents with or without chronic illnesses who experience their families as emotionally supportive, free of weight-related teasing, and not overly concerned with physical attributes are less likely to report body dissatisfaction.11,35 In fact, adolescents who grow up in a household with family members who constantly criticize their own body or were subject to teasing, are more likely to develop negative body image than those who do not grow up with teasing/criticism. 35 Although there is limited research in youth with chronic illness, 36 findings are suggestive that supportive family environments with adequate family functioning are protective against negative body image in youth.33,37
Peer support structures where weight and physical appearance are not of high concern can be protective of negative body image. 10 Adolescent peers may exchange a lot of ideas and feelings that can contribute to identity formation and self-image. 38 Although most youth with chronic illness report good peer relationships, 39 there is evidence to suggest that attending camp with peers of the same illness may be protective of body dissatisfaction through social comparison processes. 40 For instance, adolescents with cancer who attended an oncology summer camp felt more similar to camp peers than home peers and these peer comparisons were related to social acceptance, physical appearance, and global self-worth. 40
Sociocultural Influences
For youth with chronic illnesses, body image issues extend beyond the framework of individual psychological characteristics and interpersonal interactions. Sociocultural pressures for women to attain an unrealistically slender ideal, and for men to attain and maintain a slender but muscular body is associated with body dissatisfaction.41,42 Media imagery may be involved in producing changes in the way the body is perceived and evaluated depending on the viewer’s perception of the importance of those cues. 16 In fact, research has found that the more women watch television and read fashion magazines in childhood the higher their levels of body concern will be in adulthood. 12 Youth with chronic illness are receiving the same media messages as their healthy peers and may not know how to process media images and messages in society. Media literacy, the ability to critically evaluate media messages, may help defend against negative body image 43 and is a construct in the framework for developing adolescent health literacy skills (ie, capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions), which are especially important skills to acquire for youth with chronic illness. 44
Role of the Health Care Provider
Health care providers can be the first step in line for prevention of body dissatisfaction in youth with chronic illnesses. A few screening questions regarding body image concerns and with regards to family and peer relationships may be incorporated into regular clinic visits of youth with chronic illnesses. Some suggested comments/questions adapted by Neumark-Sztainer et al
45
include the following:
I would like to ask you a few questions about any weight or appearance-related concerns you may have. On a scale from 0 (not at all concerned) to 10 (extremely concerned), how concerned are you about your weight and/or appearance? Are you currently or ever in the past done anything like dieting to change your weight or appearance? Do any of your friends or family members make comments to you about your weight or appearance? If yes, how do you feel about these comments?
The responses to these questions can be addressed within the treatment plan. This helps the health care provider get a better understanding of the body image issues their patients may be struggling with and allow time to assist them and their families at working through it together. Additional psychological support for troubled youth when needed should be provided, especially at times when they are emotionally distressed.
Treatment strategies and interventions aimed at reducing the effect of the chronic disease on appearance could have positive effects on body image. However, if the consequences of the chronic illness on appearance cannot be reduced or eliminated, interventions may be beneficial that teach young people that being attractive to others, especially important people in their lives such as family and friends, does not only depend on the appearance of the body that are affected by their illness. Teachable moments by health care providers or parents on how to be health and media literate (eg, rejecting and/or challenging images and messages that could endanger body image on a regular basis) would also help improve self-image. 44 Additionally, encouraging socialization with other peers with chronic illnesses may promote lateral or downward social comparisons with others in similar or worse circumstances and promote positive body image.21,40 Youth who choose to surround themselves with others who also hold a positive body image and are understanding and supportive of their illness are better off in being protected from body dissatisfaction. 23
Conclusion
Health care providers and families of young people with chronic illnesses should be aware of the body image issues they may endure and regularly monitor their psychosocial well-being. Treatment strategies and interventions aimed at reducing negative body image should take into account the needs of youth in their search for independence from their parents in managing their illness, the desire to “fit in” with their peers, and the sociocultural pressures to be thin/slender for girls and lean/muscular for boys. Special training for health care providers of youth with chronic illness may be warranted in helping them to identify and address body image issues early on in the prevention of future health complications.
Footnotes
Acknowledgements
This study was supported in part by the intramural research program of the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development.