
Abstract
Bariatric surgery has been demonstrated to be an effective treatment for patients with severe obesity, producing improvements in many comorbid conditions, including type 2 diabetes, hypertension, obstructive sleep apnea, and dyslipidemia. The loss of body weight and resolution of comorbidities have been more recently found to be the result of functional and metabolic changes produced by the surgical procedures. Nonetheless, bariatric surgery is still considered to be a tool that is supported by health behaviors characteristic of all weight loss programs—that is, adoption of healthy eating patterns, engagement in robust physical activity, and implementation of constructive coping strategies. In addition, patients who undergo bariatric surgery face challenges that are particular to this population, including adjustment to rapid and significant reduction in body weight, forced alterations in eating behavior, and risk of alcohol misuse. This state-of-the-art review focuses on the research and resultant recommendations regarding lifestyle management for patients who have undergone bariatric surgery.
Keywords
‘Patients who undergo bariatric surgery are also likely to experience psychological and social challenges as they adapt to a changing eating style and reduced body weight.’
Introduction
Various expert panels have endorsed bariatric surgery as an acceptable weight loss option for patients with a BMI ≥40 kg/m2 or those with a BMI ≥35 kg/m2 who have comorbid conditions.1-7 An international survey of 36 nations or national groups estimated that more than 344 000 bariatric surgery operations were performed in 2008; 220 000 of these operations were performed in the United States or Canada). 8 The exponential growth in procedures is a result of several factors, including improved surgical techniques, reduction in the postoperative mortality rate, significant improvement in obesity-related comorbid conditions, 9 and increased media attention and profitability. The upsurge in surgical procedures also reflects the increasing prevalence of severe obesity in the United States. More than 6% of adult Americans are considered severely obese, with prevalence rates reaching as high as 18% among African American women. 10 It is therefore likely that health care professionals from all disciplines will encounter patients who have undergone a bariatric surgical procedure. Similarly, primary care providers will be expected to monitor and manage their patients on a long-term basis. Many of the weight loss surgeries, most notably the combined restrictive-malabsorptive surgical procedure—Roux-en-Y gastric bypass (RYGB)—and the 2 malabsorptive procedures—biliopancreatic diversion (BPD) and biliopancreatic diversion with duodenal switch (BPDDS)—place patients at high risk for development of micronutrient deficiencies and in some cases also macronutrient deficiencies. Because most of the deficiencies can be identified early at a preclinical stage, early treatment will prevent or reduce symptoms and deficiency syndromes. Although bariatric surgery is a powerful tool for weight loss and maintenance of weight loss, it does not cure obesity. As such, patients are at risk to experience weight regain several years following surgery. This state-of-the-art review will address the most commonly performed weight loss procedures, the importance of perioperative nonsurgical care, identification and management of nutritional deficiencies that may occur after bariatric surgery, and factors associated with weight regain.
Bariatric Surgical Procedures
Weight loss surgeries have traditionally been categorized into 3 groups—restrictive, restrictive-malabsorptive, and malabsorptive (Figure 1). Restrictive surgeries limit the amount of food the stomach can hold and slow the rate of gastric emptying. The laparoscopic adjustable gastric band (LAGB) is the prototypical restrictive operation. The first banding device, the LAP-BAND, was approved for use in the United States in 2001. A second device, the REALIZE band, was approved in the United States in 2007. In contrast to previous fixed devices, the diameter of these bands is adjustable by way of its connection to a reservoir that is implanted under the skin. Injection into or removal of saline from the reservoir tightens or loosens the band’s internal diameter, respectively, thus changing the size of the gastric opening. Because there is no rerouting of the intestine with LAGB, the risk for developing nutritional deficiencies is dependent on the patient’s diet and eating habits. The second and most recently developed restrictive procedure is the laparoscopic sleeve gastrectomy. In this procedure, the stomach is restricted by stapling and dividing it vertically and removing approximately 80% of the greater curvature, leaving a slim banana-shaped remnant stomach along the lesser curvature.
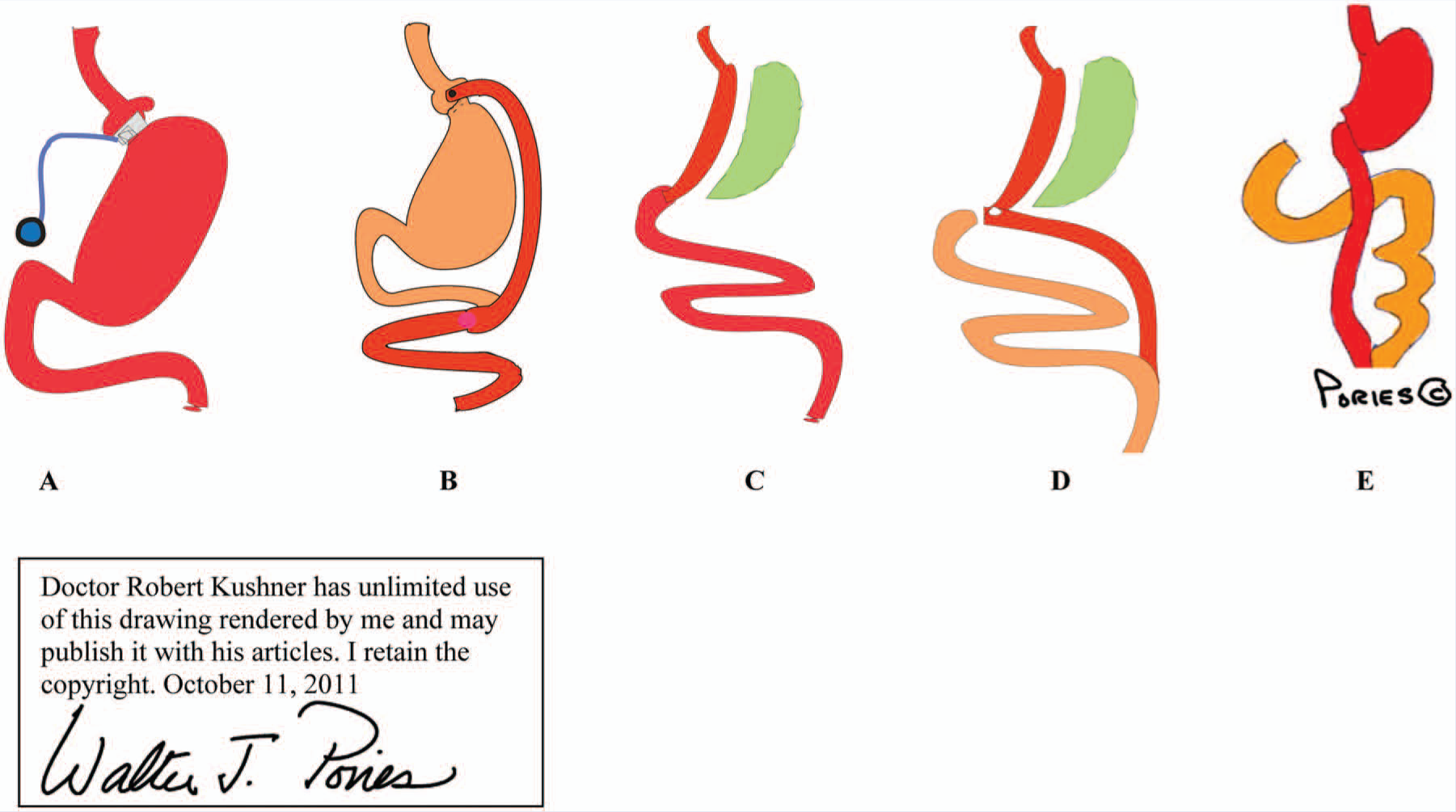
The 5 Commonly Performed Bariatric Surgical Procedures: A. Laparoscopic Adjustable Gastric Banding. B. The Roux-en-Y Gastric Bypass; C. Laparoscopic Sleeve Gastrectomy; D. Biliopancreatic Diversion; E. Biliopancreatic Diversion With Duodenal Switch.
The restrictive-malabsorptive bypass procedure combines the elements of gastric restriction and selective malabsorption. The RYGB is the most commonly performed procedure. It involves creation of a 10- to 30-mL proximal gastric pouch by either surgically separating or stapling the stomach across the fundus. Outflow from the pouch is created by performing a narrow (10-mm) gastrojejunostomy. The distal end of the jejunum is then anastomosed 50 to 150 cm below the gastrojejunostomy. Roux-en-Y refers to the Y-shaped section of small intestine created by the surgery; the Y is created at the point where the pancreobiliary conduit (afferent limb) and the Roux (efferent) limb are connected. Bypass refers to the exclusion or bypassing of the distal stomach, duodenum, and proximal jejunum. RYGB may be performed with an open incision or laparoscopically.
There are 2 malabsorptive procedures. In the BPD, a subtotal gastrectomy is performed, leaving a much larger gastric pouch compared with the RYGB. The small bowel is divided 250 cm proximal to the ileocecal valve and connected directly to the gastric pouch, producing a gastroileostomy. The remaining proximal limb (biliopancreatic conduit) is then anastomosed to the side of the distal ileum, 50 cm proximal to the ileocecal valve. In this procedure, the distal stomach, duodenum, and entire jejunum are bypassed, leaving only a 50-cm distal ileum common channel for nutrients to mix with pancreatic and biliary secretions. The BPDDS is a variant of the BPD, which preserves the first portion of the duodenum. In this procedure, a vertical subtotal gastrectomy is performed, and the duodenum is divided just beyond the pylorus. The distal small bowel is connected to the short stump of the duodenum, producing a 75- to 100-cm ileal-duodenal “common channel” for absorption of nutrients. The other end of the duodenum is closed, and the remaining small bowel connected onto the enteral limb at about 75 to 100 cm from the ileocecal valve.
Research over the past decade has identified multiple functional and hormonal changes involved in hunger, food intake, satiety, and glucose metabolism that occur as a result of the surgical procedures and further explain the differences in resultant weight loss and improvements in comorbid conditions. Changes in some or all of the gut hormones, including ghrelin, glucagon-like peptide-1, and peptide YY have been associated with the LGS, RYGB, BPD, and BPDDS procedures. 11 Thus, bariatric surgery may be more aptly referred to as metabolic surgery.
Importance of Lifestyle Intervention
Because obesity is fundamentally a disorder of energy balance, all treatments must include attention to caloric intake (energy in) and physical activity (energy out). By altering gastrointestinal anatomy and physiology, weight loss surgery is a powerful tool to reduce caloric intake. Nonetheless, all patients need counseling on diet and nutrition that is consistent with the specific surgical procedure (restrictive vs malabsorptive) and with optimal health. They also need guidance on implementing dietary, physical activity, and behavioral changes within the structure of their daily life. Patients who undergo bariatric surgery are also likely to experience psychological and social challenges as they adapt to a changing eating style and reduced body weight. Remarkably, the lifestyle aspects of perioperative management have received only a modest amount of research attention. 12
Preparing the Patient for Surgery
All patients who are considering weight loss surgery should undergo a comprehensive assessment by a multidisciplinary team of health care providers that includes a physician, registered dietitian, and mental health professional.1,5 Preparation for surgery commonly spans 3 to 12 months depending on the patient’s medical condition and criteria for insurance approval. During the preoperative process, patients are typically instructed on healthy eating and physical activity patterns, behavioral strategies to implement the lifestyle changes, and the importance of stress reduction and social support for long-term success. Specific dietary and nutritional recommendations pertinent to the surgical procedures include use of protein supplements, avoidance of meal skipping, consumption of portion-controlled meals and snacks, and slowing the rate of eating. Patients are seen either individually or in small groups. Many centers offer panel discussions between candidate patients and patients who have already undergone a procedure to provide a peer-to-peer discussion of the risks, benefits, and challenges of life after bariatric surgery.
Weight Loss Outcomes and Improvement in Obesity-Related Medical Conditions
Several meta-analyses and systematic reviews of bariatric surgery outcomes have been conducted.13-15 As compared with standard care, mean differences in BMI levels from baseline at year 1 are −2.4 kg/m2 for LAGB, −10.1 kg/m2 for LGS, −9.0 kg/m2 for RYGB, and −11.3 kg/m2 for BPD. 16 Weight loss at 2 to 3 years following a surgical procedure varies from a mean of 20% to 34% of total weight, depending on the procedure. 17 Significant improvement in multiple obesity-related comorbid conditions have been reported, including improvements in type 2 diabetes mellitus (T2DM), hypertension, dyslipidemia, obstructive sleep apnea, and quality of life. 13 The most striking effect of surgery has been to improve glycemic control in T2DM, leading to resolution of the disease in a large proportion of patients. In a recent meta-analysis by Buchwald et al 18 that included a database of 621 studies, T2DM was resolved in 75% of patients ≥2 years after undergoing bariatric surgery. In general, recovery from diabetes is greatest with the malabsorptive procedures (BPD and BPDDS), followed by the restrictive-malabsorptive procedure (RYGB) and is least following restrictive procedures (LAGB and laparoscopic sleeve gastrectomy). Although the mechanisms by which bariatric surgery mediates resolution of T2DM remain unclear, likely factors include reduced carbohydrate intake; loss of total, visceral, and intraorgan fat; increased insulin sensitivity; faster delivery of food through the gut allowing for earlier release of glucagon-like peptide-1 from the distal intestinal L cells; and exclusion of nutrients from the proximal intestine. Predictors of recurrence of diabetes include the use of insulin preoperatively and a longer duration of disease. Because the long-term outcome for diabetes control remains uncertain, all patients with T2DM who undergo bariatric surgery require lifelong surveillance of blood glucose and HbA1c. A recent meta-analysis of controlled clinical trials comparing bariatric surgery versus no surgery showed that surgery was associated with a reduced odds ratio (OR) of global mortality (OR = 0.55), cardiovascular mortality (OR = 0.58), and all-cause mortality (OR = 0.70). 19 Readers are referred to a comprehensive guideline for further information on perioperative medical care and outcomes from bariatric surgery. 20
Lifestyle Interventions in the Postoperative Care of Bariatric Surgical Patients
National guidelines suggest that continued attention to diet, physical activity, and emotional health after bariatric surgery is essential to ensure optimal outcomes. 1 Accordingly, patients are encouraged to participate in postoperative programs that support lifestyle modification.
Nutritional Care
Dietary Changes After Bariatric Surgery
A variety of dietary changes occur after bariatric surgery. Most important, there is a significant and sustained reduction in caloric intake. Although portion sizes tend to increase gradually over time in postoperative patients, caloric intake is typically still reduced by 25% or more for years after surgery.21-23
Food intolerances may occur and can lead to alterations in dietary patterns after bariatric surgery. Lactose intolerance can develop in patients who have undergone RYGB; as a result, nearly one-third of patients report avoiding milk after this procedure. 24 Dumping syndrome, which presents as a constellation of postprandial gastrointestinal, vasomotor, and neuroglycopenic symptoms, occurs in up to 76% of patients after RYGB. Dumping symptoms are thought to occur as a result of accelerated emptying of carbohydrates and hyperosmolar gastric contents into the jejunum, leading to enhanced secretion of insulin and gut peptides as well as an influx of fluid into the intestinal lumen with subsequent intestinal distention, fluid sequestration, decreased intravascular volume, and hypotension. The presence of dumping syndrome may lead patients to reduce their intake of concentrated sweets and fatty foods to avoid associated postprandial symptoms, such as abdominal cramping, nausea, diarrhea, lightheadedness, sweating, and tachycardia. 25 In fact, more than 60% of patients report avoiding sweets, and nearly 30% avoid fatty foods after gastric bypass surgery.24,26 Other food intolerances may occur as well. Among patients who have undergone a vertical banded gastroplasty (a restrictive procedure that is no longer performed), nearly two-thirds avoid consuming whole meats, one-third eschew bread, and one-third avoid fresh fruits and raw vegetables, presumably to avoid the phenomenon referred to as “plugging,” when a food becomes lodged in the gastric pouch.26,27 Similar eating patterns have been seen among patients who have undergone LAGB. 28 On the other hand, only around 10% or less of gastric bypass patients report avoidance of meats, fruits, and vegetables. 26 As a result, patients who have had RYGB may consume fewer fatty foods and sweets and more fruits and vegetables than patients who have had a purely restrictive procedure.22,26,28,29
Regardless of the types of foods consumed, regurgitation or vomiting can occur when patients eat too quickly, fail to chew food thoroughly, or eat in excess of what the gastric pouch will hold. However, it should be noted that vomiting is not an intended consequence of bariatric surgery, and it should not be viewed as normal, particularly in the late postoperative period once patients have advanced to a regular diet and have acclimated to the gastric restriction. Patients who have persistent vomiting or regurgitation after surgery should be evaluated for the presence of maladaptive eating behaviors as well as anatomical or functional problems, such as stomal stenosis or ulceration, reflux, and gastric dysmotility.20,30
Patients with symptoms of dumping syndrome can usually be managed by dietary modification, including avoidance of concentrated sweets and simple sugars, consumption of small frequent meals, and inclusion of protein at every meal. Patients with symptoms suggestive of postprandial hypoglycemia that are not ameliorated by dietary modification should undergo evaluation for the presence of endogenous (or postbypass) hyperinsulinemic hypoglycemia.20,31 Patients with more severe neuroglycopenic symptoms (such as confusion or loss of consciousness) should also undergo evaluation for this condition, which can occur after gastric bypass.
Recommended Dietary Patterns and Eating Behaviors
As a result of the reductions in gastric capacity and caloric intake after surgery, patients must take care to ensure that nutritional needs are met. Postoperative patients should be advised to consume small portions, have 4 to 6 small meals daily, and ensure an adequate intake of lean protein (60-120 g/d), fruits and vegetables (>5 servings/d), and whole grains.20,32 Protein intake is particularly emphasized because of its importance in maintaining lean body mass. Protein is typically derived from whole foods such as meats, eggs, soy, and dairy products along with concentrated protein supplements. 33 Patients should also eat slowly; chew thoroughly; avoid fatty foods, sweets, and sugar-sweetened beverages; and avoid ingestion of liquids within 30 minutes of meals. Unfortunately, many postoperative patients fail to follow the recommended guidelines, particularly regarding fruit and vegetable consumption and avoidance of sweets and caloric beverages. 32 For this reason, clinicians should routinely assess patients’ dietary intake during postoperative visits and reinforce recommended dietary goals.
Prevention of Micronutrient Deficiencies After Bariatric Surgery
Patients who have undergone bariatric surgery should be counseled that they are at risk for the development of micronutrient deficiencies after surgery. After RYGB, the most common micronutrient deficiencies include deficiencies of vitamin B12, vitamin D, calcium, and iron.34,35 Folic acid deficiency has also been reported but is largely preventable with regular use of a standard multivitamin preparation. 34 Sleeve gastrectomy has been reported to produce deficiencies similar to that in gastric bypass but at a somewhat lower frequency. 35 As compared with RYGB, the BPDDS is much more likely to produce deficiencies of the fat-soluble vitamins, including vitamin A. 36 The purely restrictive procedure LAGB is infrequently associated with specific nutritional deficiencies. 37
In many cases, micronutrient deficiencies can be prevented by regular vitamin and mineral supplementation along with appropriate clinical follow-up and routine biochemical surveillance. Expert guidelines are available regarding recommended vitamin and mineral supplementation after surgery and the frequency of laboratory screening for deficiency states. 20 Tables 1 and 2 summarize these recommendations. Patients who are found to have evidence of specific micronutrient deficiencies will need additional vitamin or mineral supplementation, as indicated.
Recommended Micronutrient Supplementation After Bariatric Surgery; Patients With Micronutrient Deficiency States Will Require Additional Supplementation as Indicated. a
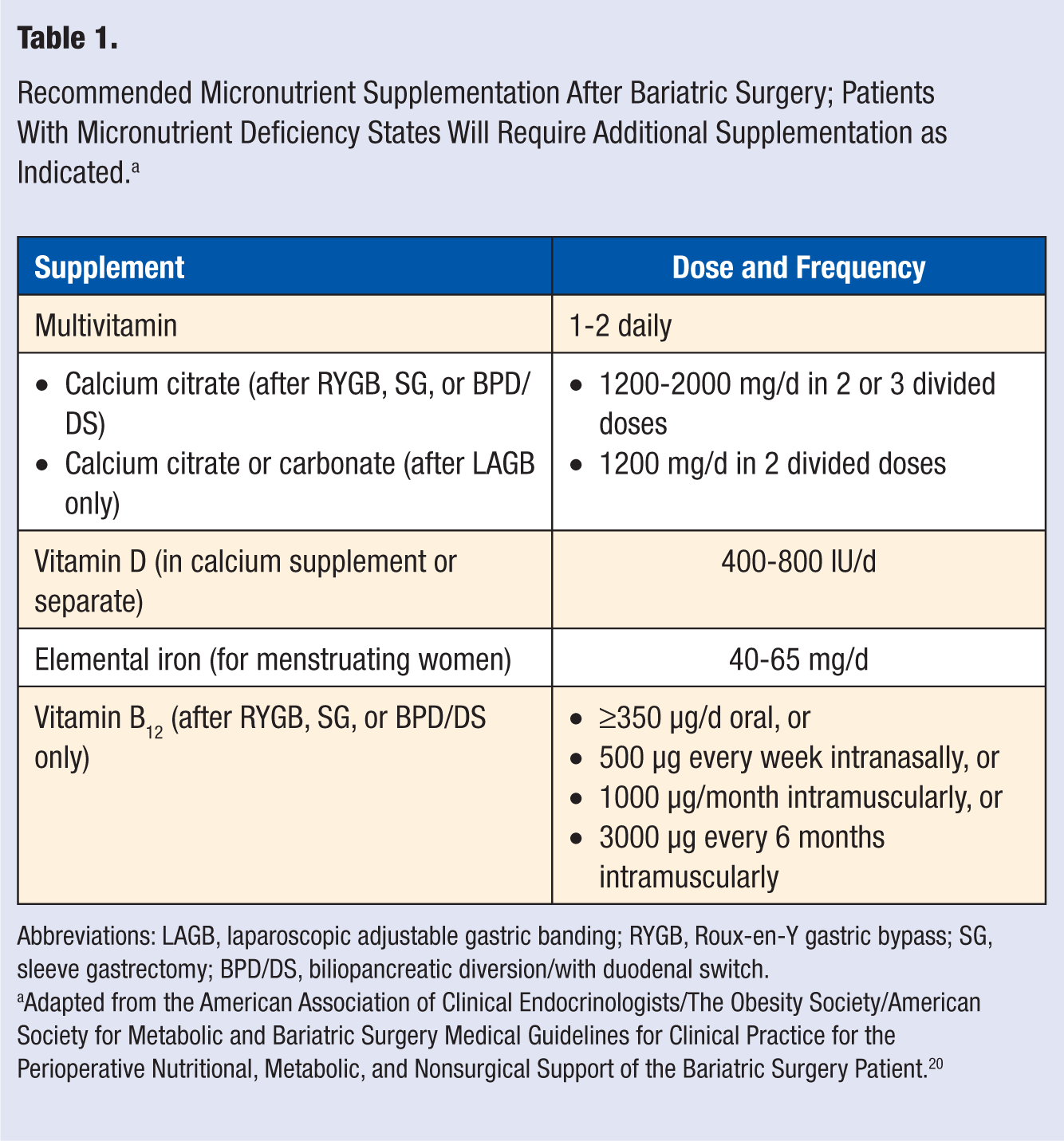
Abbreviations: LAGB, laparoscopic adjustable gastric banding; RYGB, Roux-en-Y gastric bypass; SG, sleeve gastrectomy; BPD/DS, biliopancreatic diversion/with duodenal switch.
Adapted from the American Association of Clinical Endocrinologists/The Obesity Society/American Society for Metabolic and Bariatric Surgery Medical Guidelines for Clinical Practice for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient. 20
Recommended Laboratory Tests and Frequency of Routine Biochemical Surveillance. a
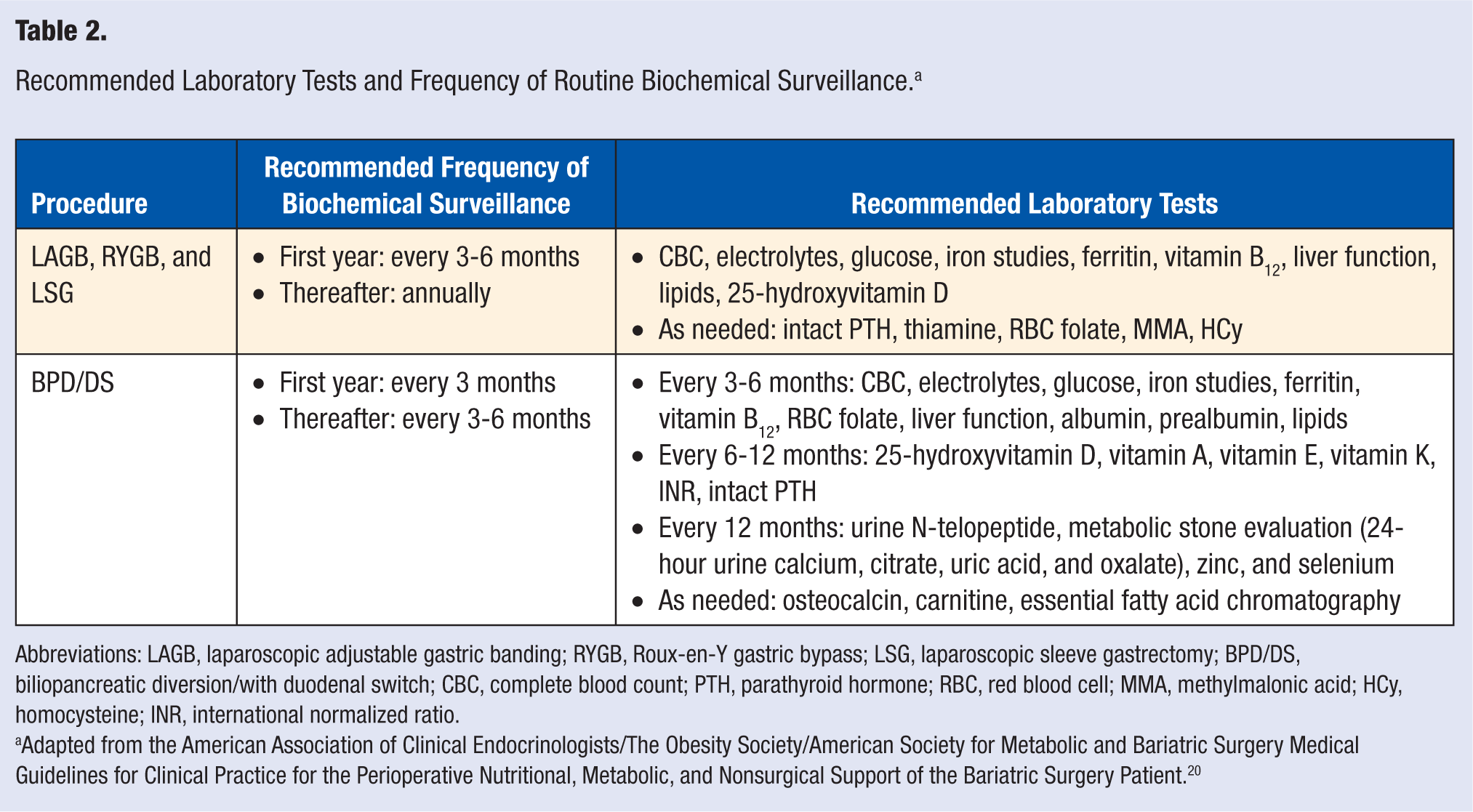
Abbreviations: LAGB, laparoscopic adjustable gastric banding; RYGB, Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy; BPD/DS, biliopancreatic diversion/with duodenal switch; CBC, complete blood count; PTH, parathyroid hormone; RBC, red blood cell; MMA, methylmalonic acid; HCy, homocysteine; INR, international normalized ratio.
Adapted from the American Association of Clinical Endocrinologists/The Obesity Society/American Society for Metabolic and Bariatric Surgery Medical Guidelines for Clinical Practice for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient. 20
Physical Activity
Among individuals who have lost weight with nonsurgical treatment approaches, physical activity clearly plays a vital role in long-term maintenance of weight loss.38,39 Much less is known about the role of physical activity in weight control after bariatric surgery, but it may be an important factor.
Physical Activity Levels After Bariatric Surgery
Numerous studies suggest that self-reported levels of physical activity increase significantly after bariatric surgery.40,41 However, there is little objective data regarding changes in physical activity levels in the postoperative period. In 1 study, patients reported a large increase in moderate to vigorous intensity activity after surgery, but accelerometer data suggested that such an increase did not actually occur in most individuals. 42 In fact, data suggest that only 10% to 24% of postbariatric surgery patients meet national guidelines regarding minimal physical activity levels for general health promotion (ie, ≥150 min/wk or moderate to vigorous physical activity in bouts of 10 minutes or more).32,43 Data from the National Weight Control Registry indicate that patients who have lost weight through bariatric surgery tend to be less physically active than individuals who have lost similar amounts of weight through nonsurgical approaches. 44
Benefits of Physical Activity in Postoperative Bariatric Surgery Patients
In epidemiological studies of postoperative patients, increased self-reported physical activity has been repeatedly associated with improved weight loss, mood, and psychosocial functioning.40,45,46 Similarly, in a cross-sectional study that used armband accelerometers to measure activity in patients who had undergone gastric bypass 2 to 5 years earlier, higher levels of moderate to vigorous physical activity were associated with greater postoperative weight loss. 43
However, data from intervention studies are lacking. In 1 small, nonrandomized, prospective study, participation in a postoperative exercise program (including 75 minutes of supervised aerobic exercise and resistance training 3 times a week) for 3 months did not significantly increase weight loss after RYGB surgery. 47 However, the intervention did prevent the observed decrease in dynamic muscle strength that was seen in postoperative patients who did not exercise, and it was also associated with an increase in functional and aerobic capacity. In a small, randomized controlled trial, Shah and colleagues 48 randomly assigned 33 obese (BMI ≥ 35.5 kg/m2) postoperative patients to either high-volume exercise (with a goal of expending ≥2000 kcal/wk in moderate-intensity aerobic exercise) or a usual activity control for 12 weeks. Participants assigned to the exercise intervention reported a greater than 3-fold increase in time spent in moderate physical activity and a nearly 2-fold increase in recorded step counts. In this small study, those in the intervention group did not have greater weight loss or greater improvements in body composition, fasting glucose or insulin levels, lipids, or blood pressure as compared with controls. However, they did have significantly greater improvements in physical fitness and glucose levels after an oral glucose challenge. Additional data are needed to further characterize the benefits of exercise in postoperative bariatric surgery patients and to determine the optimal physical activity levels in this group.
Barriers to Physical Activity After Bariatric Surgery
Significant weight loss, such as that achieved after bariatric surgery, may enable severely obese patients to become more active. However, cognitive barriers to physical activity may persist after bariatric surgery and may influence patients’ activity levels. 41 These barriers include reduced awareness of the health benefits of exercise, fear of injury, a lack of confidence in the ability to participate in physical activity, and self-consciousness or embarrassment. Treatment strategies that address these barriers may help patients become more physically active.
Recommendations for Physical Activity After Bariatric Surgery
National guidelines suggest that for optimal weight control, most overweight individuals will need to accumulate at least 150 to 300 minutes of moderate physical activity per week, or 30 to 60 minutes most days of the week. 49 In 1 recent study of those who had successfully maintained large weight losses over time after surgical or nonsurgical treatments, it was found that nearly 70% engaged in 150 minutes or more of moderate to vigorous physical activity per week, and more than 30% were physically active for at least 300 minutes per week. 39 Other data from the National Weight Control Registry indicate that walking is the preferred form of physical activity in this group of individuals. 50 In randomized controlled trials as well as epidemiological studies, individuals who use pedometers to reach a specific step-count goal (such as >10 000 steps/d) increase their activity levels more and lose slightly more weight than those who do not use pedometers. 51 Regular pedometer use may therefore be a practical and helpful strategy for patients who have had bariatric surgery.
Behavioral/Psychological Care
Bariatric surgical patients experience a variety of psychosocial challenges in the postoperative period. Initially, patients must adjust to the postoperative diet and to their altered relationship with food. As weight loss progresses, patients must adapt to changes in their appearance and their interactions with others. Dramatic weight loss, however desirable to the patient, can lead to unexpected consequences, such as body image issues related to excess skin, unwanted sexual attention from others, and jealousy from friends and loved ones. As a result of these many challenges, mood disorders, disordered eating patterns, and substance abuse are common among postoperative patients.52-62
Mood Disorders
Mood disorders are prevalent among candidates for bariatric surgery. For example, in 1 prospective study using structured clinical interviews to assess mood preoperatively and postoperatively, clinical depression was present in approximately one-third, and anxiety was present in almost 20% of preoperative patients. 63 In this population, the prevalence of clinical depression decreased by more than 50% in the 3 years following surgery, but the prevalence of anxiety remained relatively stable. Other studies have reported significant improvements in depressive symptoms that persist for up to 5 years postoperatively.64-66 Data from the large Swedish Obese Subjects study suggest that after dramatic improvements in both depression and anxiety in the first postoperative year, there may be some deterioration of mood over time. 67 However, even 10 years postoperatively, the prevalence of mood disorders did not return to baseline levels in this cohort.
It is important to note that some studies have yielded less encouraging findings. In 1 small cohort, levels of depression and anxiety did not change significantly after surgery. 23 In another cohort, improvements in mood seen in the first postoperative year eroded after 2 years. 68 Other reports suggest that clinical depression may occur for the first time in some postoperative patients, despite good weight loss outcomes. 52 Furthermore, patients who have undergone bariatric surgery may be at an increased risk of suicide, particularly in the first 3 years after surgery.52-55 In 1 large retrospective cohort study, individuals who had undergone gastric bypass surgery were twice as likely to commit suicide as obese controls matched for sex, age, and baseline BMI. 54 Case studies suggest that patients who commit suicide after bariatric surgery often have a history of recurrent major depression, both before and after surgery, and that their depression persists even if they have excellent weight loss results. 55 These reports highlight the importance of continued attention to psychosocial health in the postoperative period, regardless of weight loss outcomes.
Disordered Eating
The prevalence of disordered eating appears to be high after bariatric surgery. In fact, studies suggest that half of all postoperative patients experience recurrent episodes of loss of control over eating.56-58 Patients who have disordered eating patterns before surgery often continue to exhibit similar behaviors after surgery. In 1 prospective study, two-thirds of patients with preoperative binge eating disorder reported persistent eating pathology after surgery. 59 In many cases, patients may no longer be able to consume large amounts of food in a short period of time because of the restriction in gastric capacity after surgery. However, emotional eating and grazing, which is defined as repeated unplanned episodes of consumption of small amounts of food (eg, continuous nibbling), along with a perceived lack of control over these episodes, are common in this population. 60 Patients may not report these behaviors unless they are prompted by a clinician.
Alcohol Misuse
As a result of media attention in recent years, there has been heightened concern about the potential for development of alcohol dependence or abuse in postoperative patients. 61 In recently published results from the Longitudinal Assessment of Bariatric Surgery-2 observational study, 1945 patients who underwent a RYBG or LAGB procedure completed the Alcohol Use Disorders Identification Test (AUDIT) instrument prior to and 1 and 2 years after surgery. 62 Alcohol use disorder (AUD), defined as a total AUDIT score of at least 8 out of 40 or positive for symptoms of alcohol dependence or alcohol-related harm, increased from 7.6% at the preoperative assessment to 9.6% after the second postoperative year. Male sex and younger age were identified as predictive factors, and AUD was associated with worse postoperative mental health and postoperative treatment for psychiatric or emotional problems.
In another much smaller cross-sectional study, structured clinical interviews were used to determine the rates of current and lifetime AUDs in a group of 51 postoperative patients. 69 In this study, 35.3% of individuals met DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th ed) criteria for a lifetime history of AUD, and 11.8% had a current AUD, comparable to published rates in the general population (30.3% and 8.5%, for lifetime and current disorders, respectively). Patients with a prior history of AUDs (in remission at the time of surgery) appear to be at risk for recurrence after surgery. 69
The absorption and metabolism of alcohol may be altered after bariatric surgery, and as a result, postoperative patients may be more susceptible to the intoxicating effects of alcohol.70-73 Patients should therefore be counseled to exercise caution when consuming alcohol after surgery. In addition, clinicians who care for bariatric surgery patients should ask patients about alcohol intake after surgery and remain alert to the possible presence of AUDs in this population.
Psychological Counseling and Peer Support in the Postoperative Period
Data suggest that patients with postoperative depression experience poorer weight loss than those who are not depressed. 63 Similarly, postoperative patients who exhibit disordered eating patterns, such as grazing and loss of control over eating, have poorer weight loss and greater weight regain.57,59 Clearly, patients who are found to have mood disorders, disordered eating behavior, or substance abuse after bariatric surgery should be offered professional psychological counseling and support. It is not known, however, whether such treatment improves weight loss or other outcomes.
In epidemiological studies, attendance at postoperative support groups is associated with improved weight loss outcomes.74-76 There is a lack of data regarding the effects of other types of postoperative psychological support, such as group or individual therapy, on weight loss and other outcomes.
It is interesting to note that patients who exhibit disordered eating patterns may be more receptive to a behavioral intervention after surgery than before surgery. In 1 small nonrandomized prospective study, preoperative and postoperative bariatric surgical patients with binge eating or other disordered eating patterns were referred to a 10-week cognitive behavioral therapy program designed to address and improve the maladaptive eating patterns. 77 Patients who were referred to the program postoperatively were much more likely to attend the initial session and to complete the program than patients referred preoperatively.
Comprehensive Lifestyle Interventions After Bariatric Surgery
There is limited data regarding the benefits of comprehensive lifestyle interventions in the postoperative period. However, in 1 small, randomized controlled trial, those who were assigned to a multifaceted lifestyle intervention after vertically banded gastroplasty reported improved dietary habits, increased physical activity levels, and reduced television viewing as compared with those assigned to usual care. 78 Furthermore, those in the lifestyle intervention group lost significantly more weight at 1, 2, and 3 years after surgery than those in the usual care group.
The timing of the intervention may be important. Kalarchian and colleagues 79 reported the results of a small randomized controlled study (n = 36) involving patients who had undergone bariatric surgery at least 3 years earlier but who had failed to lose 50% or more of their excess weight. Participants were randomly assigned to a comprehensive lifestyle intervention, including 12 weekly group education sessions and 5 individual telephone coaching sessions over 6 months, or a waitlisted control group. Participants randomized to the intervention group lost slightly more weight (3.3 ± 8.1 kg) than those in the control group (1.3 ± 6.8 kg), but the difference was not statistically significant. It is interesting to note that in this study, the presence of depressive symptoms at the beginning of the study was associated with greater weight loss in the intervention group but not the control group, suggesting that the behavioral component of the intervention may have been helpful for patients with depression.
Weight Regain Following Bariatric Surgery
Although clinicians commonly see bariatric surgery patients regain some weight postoperatively, the prevalence and incidence of weight regain has not been well characterized. Using cross- sectional data, significant weight regain has been estimated to occur in 20% to 35% of patients, depending on the procedure performed and duration of time following surgery.15,30,34,80 This may be an underrepresentation of actual incidence rates. The causes of weight regain are likely to be multifactorial, similar to patients who regain weight after nonsurgical approaches. Specific to bariatric surgery, the anatomical factors for weight regain result directly from either malfunction or disruption of the surgical procedure. The physiological (menopause, smoking cessation, and use of medications that promote weight gain) and behavioral (diet and physical inactivity, alcohol abuse) causes are common to surgical and nonsurgical patients. In a mail survey of 203 individuals who underwent RYGB a mean of 28.1 ± 18.9 months previously, independent predictors of significant weight regain (≥15% from weight loss nadir) were increased food urges, severely decreased postoperative well-being, and concerns about alcohol or drug use. 81 Patients who experience significant weight regain should undergo a thorough evaluation addressing potential causes of weight gain, which may include an imaging procedure or upper endoscopy, particularly when nausea, vomiting, dysphagia, and abdominal pain are accompanying symptoms. 82 Additional studies are needed to better understand the frequency, etiology, and treatment of weight regain.
Conclusion
Bariatric surgery is an effective and acceptable treatment for individuals with severe obesity who are at risk for or have complications associated with obesity. Several surgical procedures are available with variable risk and weight loss outcomes. However, regardless of the procedure performed, surgery is considered a tool to be used along with lifestyle modification, including adoption of a healthy, calorie controlled diet and participation in daily physical activity. For patients who undergo restrictive- malabsorptive or malabsorptive operations, dietary supplementation is necessary to avoid micronutrient deficiencies. Patients are at risk for weight regain following surgery because of several biopsychosocial factors. To maximize successful outcomes, all patients should be monitored and managed by a multidisciplinary team of health care providers knowledgeable in bariatric surgical care.