
Abstract
Dietary patterns are strongly influenced by cultural background and perspectives. Levels of dietary acculturation need to be considered when talking with immigrants about healthy eating. Lower levels of dietary acculturation are associated with positive health outcomes. Encouraging healthy traditional foods is a positive approach to use with individuals who are at lower levels of dietary acculturation. Questions about languages spoken in different settings and foods most often consumed can help health care practitioners assess levels of dietary acculturation. General intake recommendations of lower saturated fat, more whole grains, more fruits, more vegetables, leaner proteins, and smaller portion sizes (for caloric balance) are general recommendations that can be applied within most cultural food patterns to optimize health outcomes.
Health professionals often need to advise patients from a variety of cultural groups on general healthy eating practices. A cultural group is often identified by similarities in ethnicity, country of origin, religion, ideals, characteristics, or behaviors. Most cultures have unique food-related behaviors that ultimately influence overall health outcomes of the population.
This role of food in culture1,2 is evidenced by the inclusion of food in cultural celebrations, including weddings, funerals, birthdays, national holidays, and religious holidays. On a less tangible level, many interpersonal relationships are associated with specific feeding behavior. Many in the general American culture may associate a good mother taking care of a sick child with warm chicken noodle soup or mending an emotional hurt with warm cookies and milk. Food is also a part of how individuals express and manage their impression to others, including use as a symbol of socioeconomic status. Knowing how to properly use table settings, eat a lobster, or pass the bread at a formal meal may communicate level of education and economic resource. Food also has connotations associated with age. Pizza and soda are commonly seen as stereotypical adolescent foods, whereas oat bran cereal and prunes might be associated more often with older adults. Food and food patterns also have gender associations. Steak with beer may be associated more with male consumption patterns, whereas salad with wine spritzer may seem to characterize female food consumption patterns. Although the role of culture and food can be seen in many of the different scenarios described above, the most recognized food and culture associations are the traditional foods of broadly defined ethnic or racial and geographic communities.
Although the traditional diets of many cultures around the world are often no longer fully intact, it is useful to examine what is known in general of traditional diet patterns . . .
In advising patients, it is important for health professionals to understand two things: (a) the individual’s current level of acculturation and (b) elements of the individual’s traditional diet pattern.
Acculturation
Acculturation is the process where an immigrant takes on the values, beliefs, practices, customs, and behaviors of a new culture. In general, immigrants are classified as being at a low, moderate, or high level of acculturation. At the lowest levels of acculturation, an immigrant has retained almost all of his or her traditional cultural patterns, whereas at the highest level of acculturation, an immigrant has adopted almost all of the new host country’s cultural patterns. Similar to general acculturation, dietary acculturation is the process by which immigrants adopt the food-related beliefs, values, attitudes, and dietary behaviors of the new culture. 3 In general in the United States, individuals at lower levels of acculturation tend to have healthier dietary intake patterns4,5 and lower rates of obesity and comorbidities than their more acculturated counterparts.6-8
Traditional Dietary Patterns
To understand dietary acculturation, it is necessary to understand traditional dietary patterns; however, identifying traditional diet patterns of many cultures is becoming increasingly difficult. Many children and adults today have grown up in a time where foods, which previous generations would have considered traditional, have been replaced by more processed, Westernized foods. Those people may not have a full concept of what traditional foods were or how to prepare them. 3
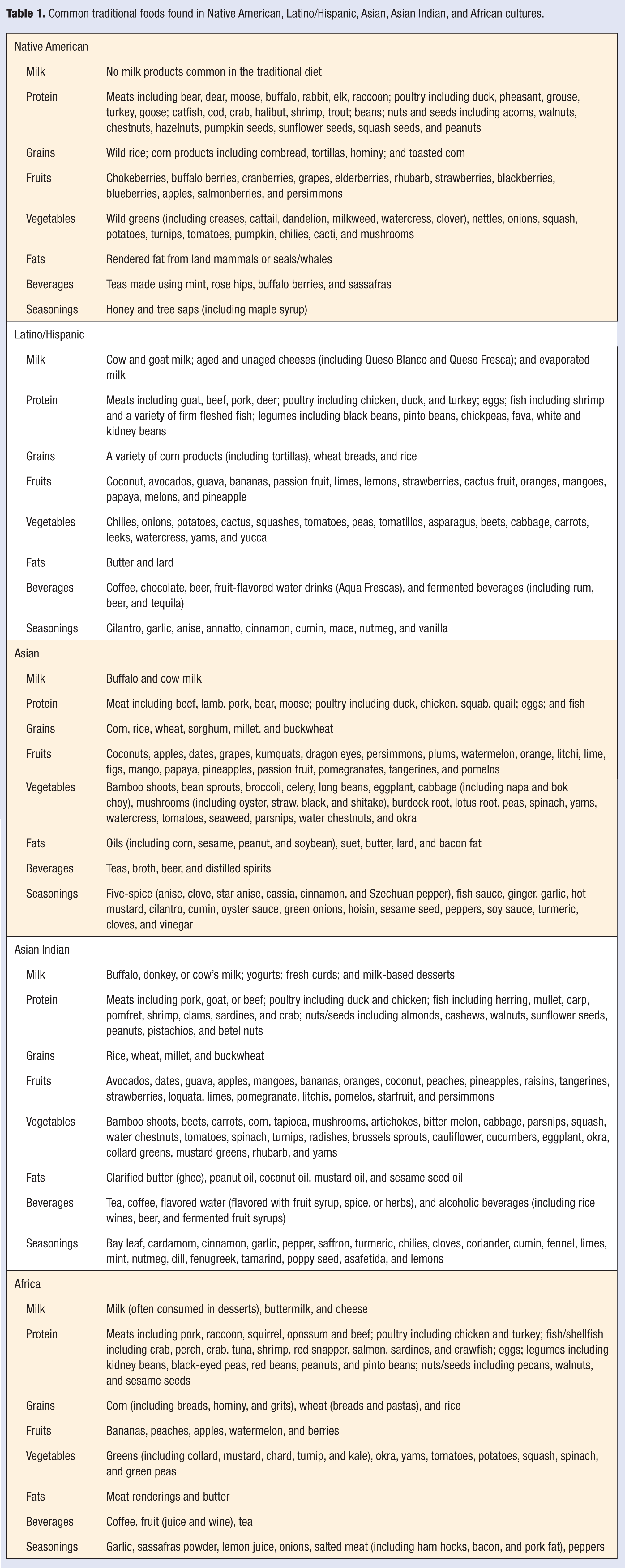
Although the traditional diets of many cultures around the world are often no longer fully intact, it is useful to examine what is known in general of traditional diet patterns as many of the traditional taste profiles still influence current food patterns. With this knowledge we can better understand the elements of the traditional diet that immigrants may have retained. The brief, general list of some common foods found in 5 cultures is found in Table 1. The cultural diet patterns of these groups are briefly described below. These descriptions are extremely generalized and do not take into account the wide variations in diet patterns that occur with geographical differences within each cultural group. The food patterns described in this article were researched (unless otherwise referenced) using the book Food and Culture by Kittler and Sucher. 9
Common traditional foods found in Native American, Latino/Hispanic, Asian, Asian Indian, and African cultures.
Native American Diet Patterns
Traditional Native American diet patterns are an excellent example of dietary diversity related to geographic location. In the Northern Plains region, Elders have primarily identified prairie turnips, fruits (chokecherries, June berries, plums, blueberries, cranberries, strawberries, buffalo berries, gooseberries), potatoes, squash, dried meats (venison, buffalo, jack rabbit, pheasant, and prairie chicken), corn, teas (spearmint, peppermint, bergamot), and wild rice as traditional foods. 10 Acorns are commonly used in traditional Native American dishes in California. 11 The traditional diet pattern of Pima Indians is higher in complex carbohydrates (often from beans and corn) and lower in fat than the current Westernized diet pattern. 12 Alaskan Native diets traditionally consisted largely of sea animals, and traditional harvesting activities commonly included smoking fish or meats, picking berries, fishing, and picking greens. 13
The traditional diet of Native Americans has many elements that are known to protect against disease. Many wild berries are rich in phytochemicals and are strong antioxidants that are antidiabetic, cardioprotective, antiviral, anti-inflammatory, anticancer, antibacterial, gastroprotective, radioprotective, and immunomodulatory.14,15 The observed high intakes of fat from sea animals (primarily seals and whales) and lower cardiovascular disease incidence was one of the initial findings that identified the role of omega-3 fatty acids in heart disease prevention.16,17
Latino/Hispanic Diet Patterns
The traditional Latino/Hispanic diet can been characterized as being high in fresh meats (eg, turkey, pork, beef), fish, vegetables (eg, squash, greens, cactus, chayote, tomatoes, onions, chili peppers, and cilantro), fruits (eg, avocados, bananas, coconut, guava, limes, mangoes, papaya), beans, rice, corn, and spices (eg, cinnamon, cocoa, garlic, anise, cumin, mace, and vanilla). 18 Some but not all traditional dishes are hot and spicy, with chili peppers commonly used. Beans, corn, and tomatoes form the basis for much of the cuisine. Spanish explorers brought many items to the Mexican diet that are now often considered quintessential Mexican flavors and foods, including onions, garlic, cinnamon, rice, sugarcane, and hogs.
An analysis of the national data from the National Health and Examination Survey (1999-2004) revealed that foreign-born Latino/Hispanic adults living in the United States reported consuming more fruits, vegetables, fruit and vegetable juices, and high-fiber/low-fat breads and less snacks, desserts, soda, fruit drinks, and fast foods than their US-born counterparts.19,20 Less acculturated Mexican Americans consume less fat and more fiber, protein, vitamins (A, C, E, and B6), folic acid, calcium, potassium, and magnesium than Mexican Americans born in the United States.21,22 These differences in nutrient intake are probably because of foreign-born Mexican Americans’ greater consumption of fruits, vegetables, whole grains, legumes, and traditional Mexican foods such as cornbread, corn tortillas, beans, and rice and less consumption of desserts and added fats.20,21 High intakes of legumes are associated with many health benefits, including helping prevent diabetes, obesity, some cancers, and cardiovascular disease. 23
Asian Diet Patterns
In many Asian cultures, traditionally there have been high intakes of tea, fish, and soybeans products (including tofu, soy milk, and soy flour). The traditional diet is also generally higher in rice, fresh vegetables, and fresh fruit and is lower in meat, sugar, and saturated fats than the typical American diet pattern. In addition to the well-documented benefits of consuming a diet lower in added sugar, saturated fat, and higher in fruits and vegetables, many of the elements of this traditional diet pattern have been found to have positive health effects (eg, omega-3 fatty acids in fish, polyphenols in tea, and isoflavones in soybeans).24-26
Asian Indian Diet Patterns
In general, the Asian Indian diet contains rice, wheat, legumes, fermented dairy products, clarified butter, and many characteristic spices. Although there are some common foods throughout India (including rice, chutneys, pickles, yogurts, coffee, coconut milk, and fresh fruits and vegetables), there are some unique differences between Northern and Southern Indian cuisines. The spices in the South tend to be hotter, whereas the spices in the North tend to be aromatic. Vegetarian diets are very common throughout India because of religious reasons. Many of these vegetarians also consume milk, eggs, and fish (lacto-ovo-peso-vegetarian). Many of the spices commonly used in Asian Indian cooking (eg, ginger, saffron, turmeric, cloves, and cinnamon) have been associated with the prevention of cancer, diabetes, and cardiovascular disease. 27
African Diet Patterns
Traditional diets in both West and Central Africa contain many starches (including plantains and root vegetables such as cassava), grilled meats with sauce, and stews. Many dishes may contain greens, spinach, tomatoes, chilies, peppers, peanuts, and onions. Although most meats are beef or chicken, other local animals such as monkey, crocodile, warthog, and antelope are sometimes consumed. Less meat is consumed in East Africa, where many animals are used as a form of currency. Corn and bananas are common starches used in East Africa. East African cuisine was influenced by many different populations that settled in the region. The influence of Arab settlers can be seen in the rice with spices (eg, saffron, cloves, and cinnamon) often served on the coast. British and Asian Indian settlers brought curries, pickled vegetables, and lentil soups. The Portuguese brought their own spices, cooking techniques (eg, roasting and marinating), vegetables (eg, chilies, peppers, tomatoes, and corn), and citrus fruits (eg, lime, lemons, pineapples, and oranges). North African cuisine was also influenced by the arrival of settlers and travelers including the Phoenicians (sausages), Carthaginians (wheat and semolina), Berbers (couscous), Romans (olives), Arabs (spices including nutmeg, cinnamon, ginger, saffron, and cloves), and the Ottoman Turks (pastries). Although some areas in Africa have a very limited consumption of milk products, the diet patterns in Southern Africa include milk and fermented milk products (including buttermilk, yogurt, and sour cream). Many of the traditional foods of Black Southern African Americans can be traced to the traditional foods of Southern Africa, including barbecued, roasted, and dried meats.
Many of the common ingredients in the traditional African diet pattern (including greens, spinach, tomatoes, chilies, peppers, peanuts, and onions) have each been found to have individual disease prevention capabilities.
These are only a small sample of the potential traditional food patterns in each of these cultures. Within each culture there are countless variations, specialties, and patterns. There are also many different cultures in the world not addressed in this article. It is impossible for any health provider to become proficient in the foods of all cultures. An excellent way for health providers to become more familiar with other cultures’ foods is to not only talk to patients about their traditional food and read about traditional food but also to try new unfamiliar food whenever possible. Explore local restaurants that serve “authentic” diverse cuisines (be aware that many ethnic restaurants serve an “Americanized” version of their traditional food) and visit small ethnic food outlets. At every grocery store trip, select one new unfamiliar food to try. The Internet serves as an excellent resource to learn to prepare a virtually unlimited number of unique ethnically diverse foods.
In addition to the vast quantity of different types of food consumed in each culture, there are an equally vast number of medicinal uses for foods and herbs in each culture. The ability to even begin to catalogue the potential medicinal uses of these foods and herbs is beyond the scope of this article.
Assessing Level of Acculturation
In addition to understanding some general concepts about an individual’s traditional diet pattern, tailoring dietary advice to an individual’s level of acculturation is very important. A short series of questions that can be used to assess an individual’s level of acculturation is provided in Table 2. However, it is essential that health providers do not try to use this approach to stereotype people. Cultural commonalties can be recognized without making assumptions about individuals. Health providers must also become aware of and eradicate any preconceptions or judgments they may hold against a culture before effective communication and counseling can occur. An initial essential step when working with any patient is to develop rapport. Establishing a climate where the patient feels he or she is being valued, listened to, and respected often is adequate to achieve essential baseline rapport. Only after this has been achieved should a health provider seek to understand the patient’s level of acculturation and provide advice on healthy choices within that acculturation level and context of traditional food pattern.
Questions to Assess Level of Acculturation and Corresponding Recommendation for Dietary Counseling.
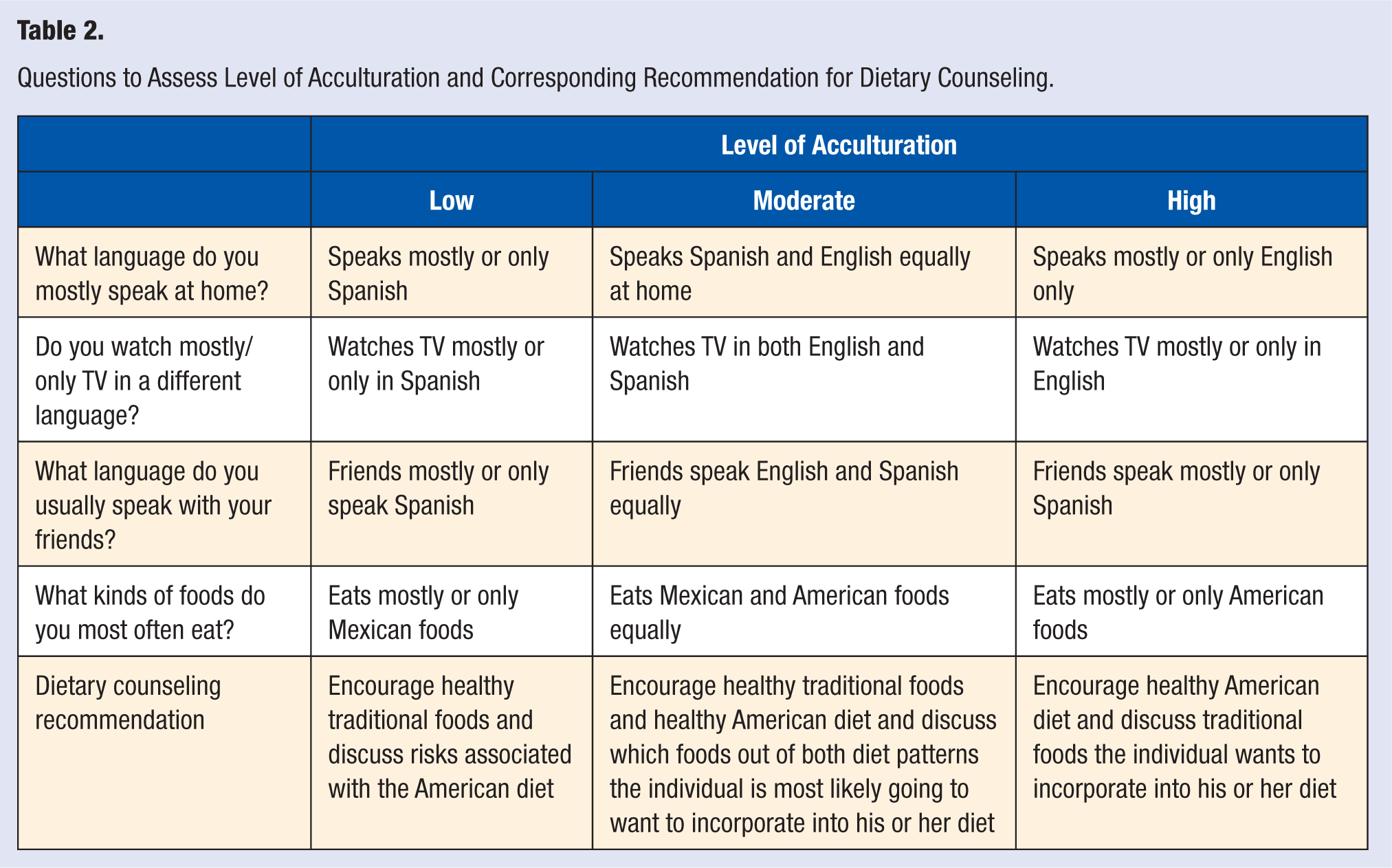
After rapport is established, a series of questions can be used to better understand the individual’s cultural perspectives and level of acculturation (see Table 2).
The acculturation process is very complex and unique to each individual. The questions should be used as general guidelines and not as absolute measures of level of acculturation. These questions should not be used in isolation, but when time is limited, the question “What kinds of foods do you most often eat?” would provide the best single indicator of level of dietary acculturation. Individuals will likely have more success achieving their goals if the discussion about food is tailored to meet their acculturation level. If individuals are asked to make healthy choices within a diet pattern outside of their current pattern, they are being asked to make two difficult changes. This would decrease the likelihood of successful behavior change. Additionally, by discussing the positive health benefits of a traditional diet with a patient who is at a lower level of acculturation, the health provider is using an empowering message. Using this positive, empowering approach may result in the patient being more likely to make successful healthy adjustments within his or her current diet pattern.
Summary
Overall, it is important to understand that each individual has his or her own unique cultural food background. Although it shows respect for different cultures by understanding some basic principles of their traditional food practices, it is impractical to try and understand all of the potential different cultural food backgrounds in detail. What is most important is to not make assumptions (or try to stereotype an individual) but instead to ask questions and listen to that individual. Based on the foods the individual currently consumes, you can help him or her set personal goals and modify his or her current diet as needed. These modifications and goals can be framed in a set of recommendations appropriate for most individuals. These common nutritional recommendations (based on the US Dietary Guidelines for Americans 28 ) can be incorporated in all cultural food patterns and include encouraging lower saturated fat, more whole grains, more fruits, more vegetables, leaner proteins, and smaller portion sizes to allow for caloric balance. Allowing an individual to set goals within these recommendations without suggesting changes in the basic structure of his or her cultural diet pattern is a simple, positive approach health providers can take when working with individuals from diverse cultural backgrounds.