
Abstract
Pharmacotherapy can have a significant impact on a patient’s quality of life and health status, potentially affecting multiple lifestyle areas, including weight, smoking status, sleep, and mood. Although pharmacotherapy can have a positive effect on such areas, its effects can also be detrimental. Pharmacists may be the most accessible health care providers to the general public, and their role in advising patients and other health care providers in making appropriate pharmacotherapy choices to positively affect one’s health and lifestyle areas is essential. This review will examine the effects of pharmacotherapy on different areas of lifestyle medicine and the role of the pharmacist as the medication expert in advising and informing patients and providers.
Pharmacotherapy can have a positive or negative effect on many lifestyle areas, including weight control, smoking status, sleep, and mood. In the United States, as a culture we have a propensity for immediate gratification, which over the past several decades has fueled the cultural response to look to pharmacotherapy as a fix for many ailments. This culture shift brings with it considerations of potential beneficial and detrimental effects of prescription and nonprescription medications and supplements. Some of the more significant lifestyle categories that pharmacotherapy has affected will be discussed in this article. In addition, we will discuss the important role that pharmacists have in informing patients about the impact of pharmacotherapy on lifestyle areas and assisting them in making appropriate pharmacotherapy choices to positively affect their health and well-being.
. . . we have a propensity for immediate gratification, which over the past several decades has fueled the cultural response to look to pharmacotherapy as a fix for many ailments.”
Dietary Supplements
The use of dietary supplements, including “natural” or herbal products as well as vitamin and mineral supplements, is extensive in the United States.1,2 Unlike prescription and over-the-counter medications, supplements are not considered medicines, and therefore they are not subject to the same strict regulations required by the Food and Drug Administration (FDA) for medications. As a consequence, dietary supplements do not need to have proven efficacy or safety before being marketed, and variability in product consistency, potency, and purity is another potential concern. A recent investigation that found heavy metal and/or pesticide contamination in the majority of supplements tested underlines this concern. 3 With so many products on the market, consumers can become overwhelmed with choosing a product for themselves. Pharmacists can assist consumers by helping them choose a product with the US Pharmacopoeia (USP) seal of approval. The USP seal indicates that the supplement has been manufactured under quality standards and contains the ingredients it claims to contain in the amount indicated and without contaminants. 4 Other third parties that analyze and rate the quality standards of supplements include the National Sanitation Foundation, a nonprofit foundation, 5 and Consumer Lab.com, an independent company. 6 It is very important, however, that pharmacists help patients to understand that such seals do not indicate that a product is efficacious or safe, and for many products there is considerable doubt regarding suggested clinical benefits.
Herbal Supplements
According to a 2007 national survey, almost 1 in 5 adults in the United States takes a nonvitamin natural product. 1 There are a multitude of herbal supplements available to consumers, and many people may prefer these alternative products over conventional medications because of their “natural” components. However, just like conventional medications, herbal supplements can be associated with side effects, serious adverse reactions, and drug and disease interactions. An example of this is the case of St. John’s wort, a commonly used supplement for mood that has numerous drug interactions due to it’s serotonergic effects and induction of the cytochrome P450 drug metabolizing system. Examples of clinically significant drug interactions with St. John’s wort include the risk for serotonin syndrome with other serotonergic drugs, particularly antidepressants, and the potential to decrease the effectiveness of some hormonal contraceptives, a drug interaction with potentially life-altering consequences in female patients of childbearing age.
In addition to the risk for drug–herb interactions, many herbal supplements on the market lack strong and consistent evidence regarding their effectiveness for intended purposes and overall safety. Supplements such as kava, often used for anxiety, have been linked to liver failure, and for many patients, especially those with other risk factors for hepatotoxicity, the risks of taking kava will outweigh any potential therapeutic benefits. Table 1 summarizes the efficacy and safety of some of the more common herbal products taken by consumers.
Common Natural Supplements 7
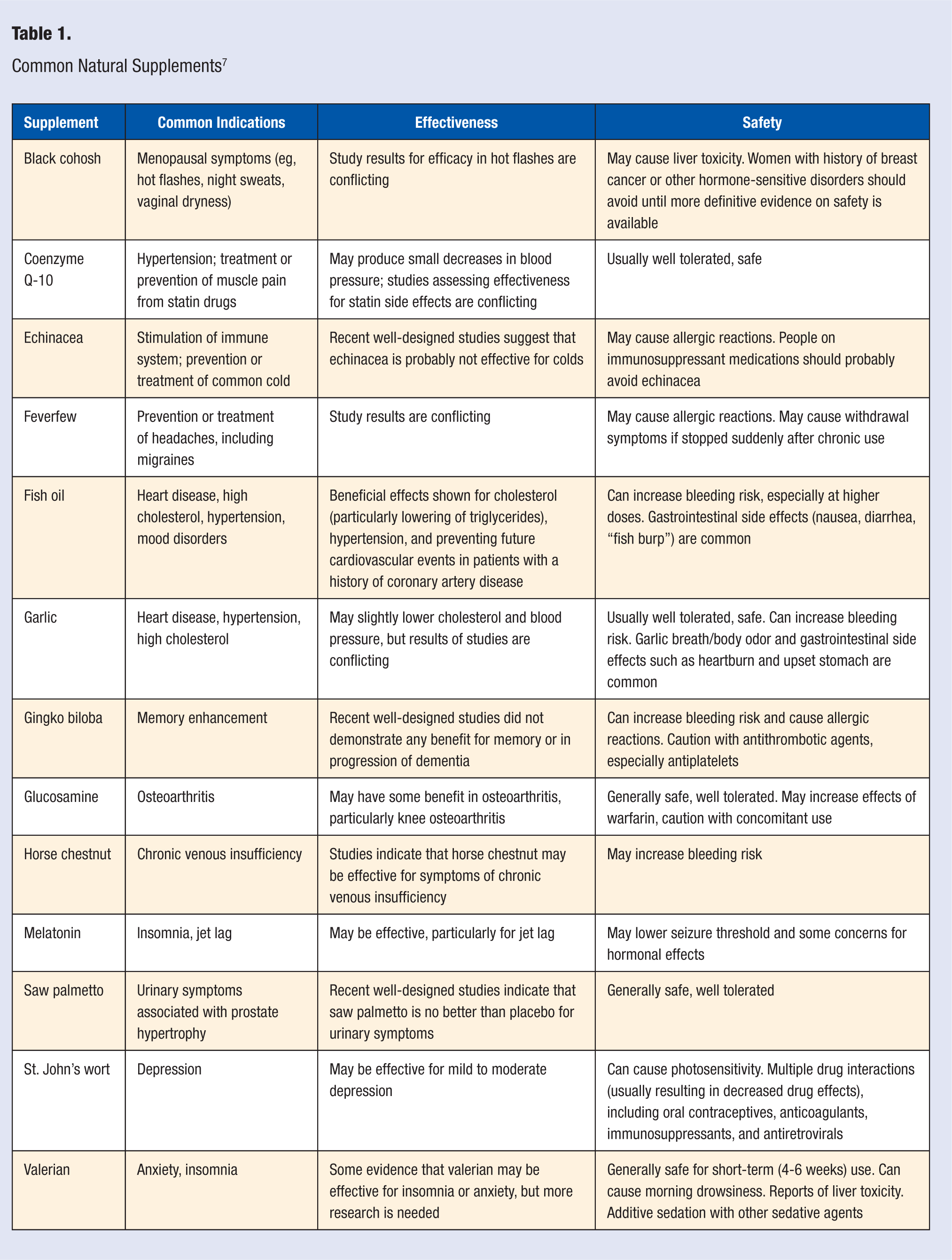
Pharmacists, with their access to reputable drug and natural supplement references, have the opportunity and knowledge to inform patients about the risks and benefits of herbal products. Pharmacists can help interpret the available information to assist patients and their providers in making the best decisions and appropriately weigh the risks and benefits. A common, well-respected resource that pharmacists can refer consumers to for accurate, nonbiased information about individual supplements is the Web site for the National Center for Complementary and Alternative Medicine (http://nccam.nih.gov). It is not the intent of pharmacists to ward patients away from natural remedies and supplements. However, it is the intent of pharmacists to work with patients collaboratively to arrive at an informed decision regarding each individual’s health.
Vitamin and Mineral Supplements
Vitamin supplements, including single-entity and multivitamin products, are the most commonly used dietary supplements. 8 This is despite the fact that true vitamin deficiencies, apart from vitamin D and iron, are very rare in the United States. The Food and Nutrition Board of the Institute of Medicine makes recommendations regarding nutrient intake levels; these are referred to as dietary reference intakes (DRIs). 9 The labeling on vitamin and mineral products lists nutrients per serving as a percentage of daily value (%DV), which is based on the recommended intake for a healthy adult on a 2000-calorie diet. Individual needs may vary based on age, gender, and health status.
Consistent and convincing evidence for health benefits, from vitamin supplementation in healthy, nondeficient adults is lacking.10-13 In fact, some studies have shown an increased risk of cancer with supplementation of certain vitamins. This is the case for beta-carotene (a form of vitamin A), which was associated with an increased risk of lung cancer and mortality when it was given as a supplement to current or former smokers.14,15 Although many people may take high doses of some vitamins, such as vitamin C for the common cold and vitamin E for prevention of heart disease, their effectiveness for such purposes is not consistently supported by studies.16,17 Additionally, consumption of higher than recommended doses of vitamins can result in adverse events, including serious ones. Many patients may not realize that “too much of a good thing” applies to vitamins as well, and they should be encouraged to talk to their health care provider if they are concerned about a deficiency. True vitamin deficiencies should not be self-treated, and the pharmacist should refer these patients for evaluation by their health care provider. Table 2 summarizes some of the more commonly supplemented vitamins and minerals and recommended intakes.
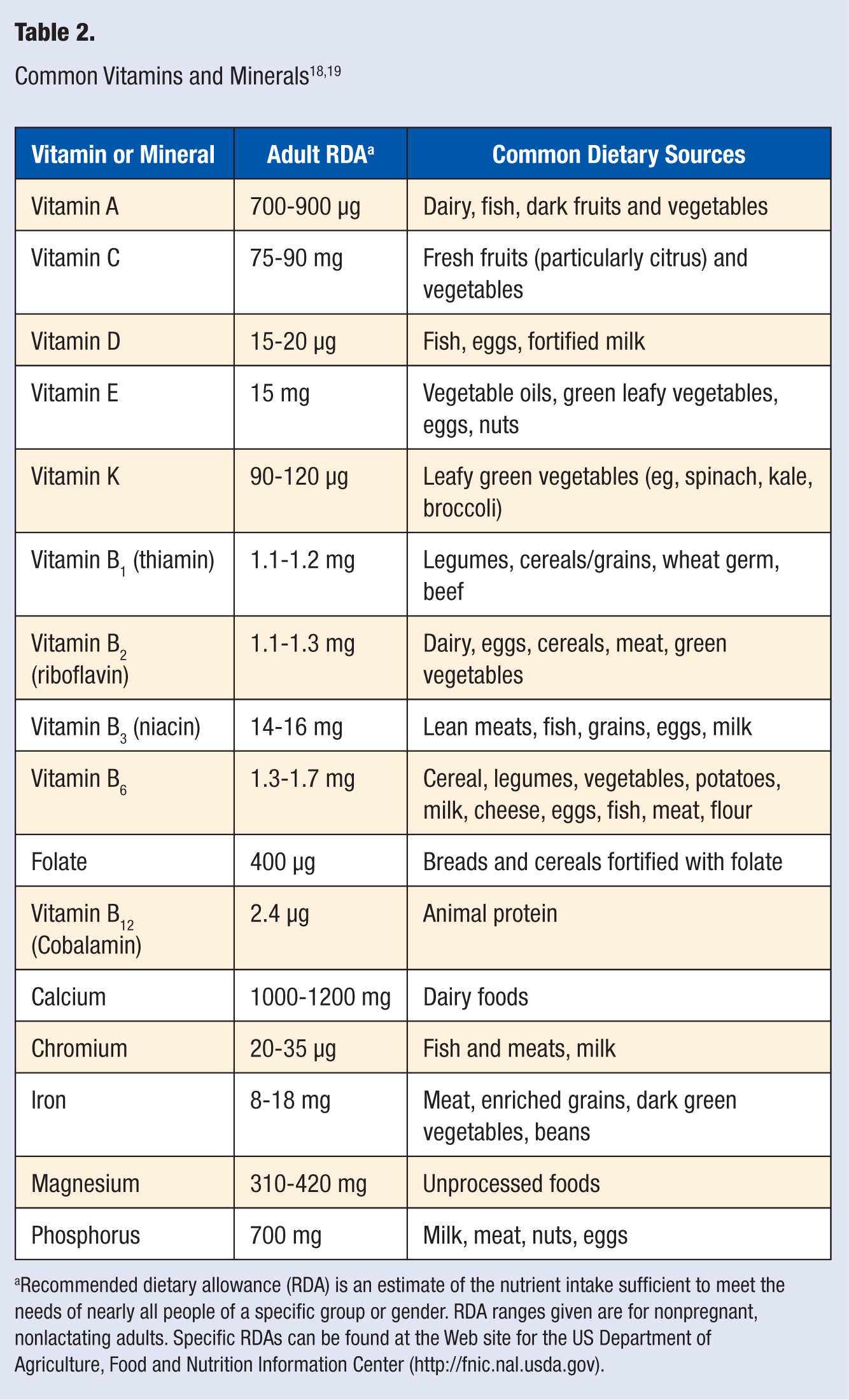
Recommended dietary allowance (RDA) is an estimate of the nutrient intake sufficient to meet the needs of nearly all people of a specific group or gender. RDA ranges given are for nonpregnant, nonlactating adults. Specific RDAs can be found at the Web site for the US Department of Agriculture, Food and Nutrition Information Center (http://fnic.nal.usda.gov).
Although the utility of multivitamin or individual vitamin supplementation in healthy adults is unclear, there are known benefits from the supplementation of some vitamins in certain populations. For example, folic acid supplementation is recommended for women of childbearing age to prevent birth defects, 20 and calcium and vitamin D supplementation is recommended in most postmenopausal women to prevent bone density loss. 21
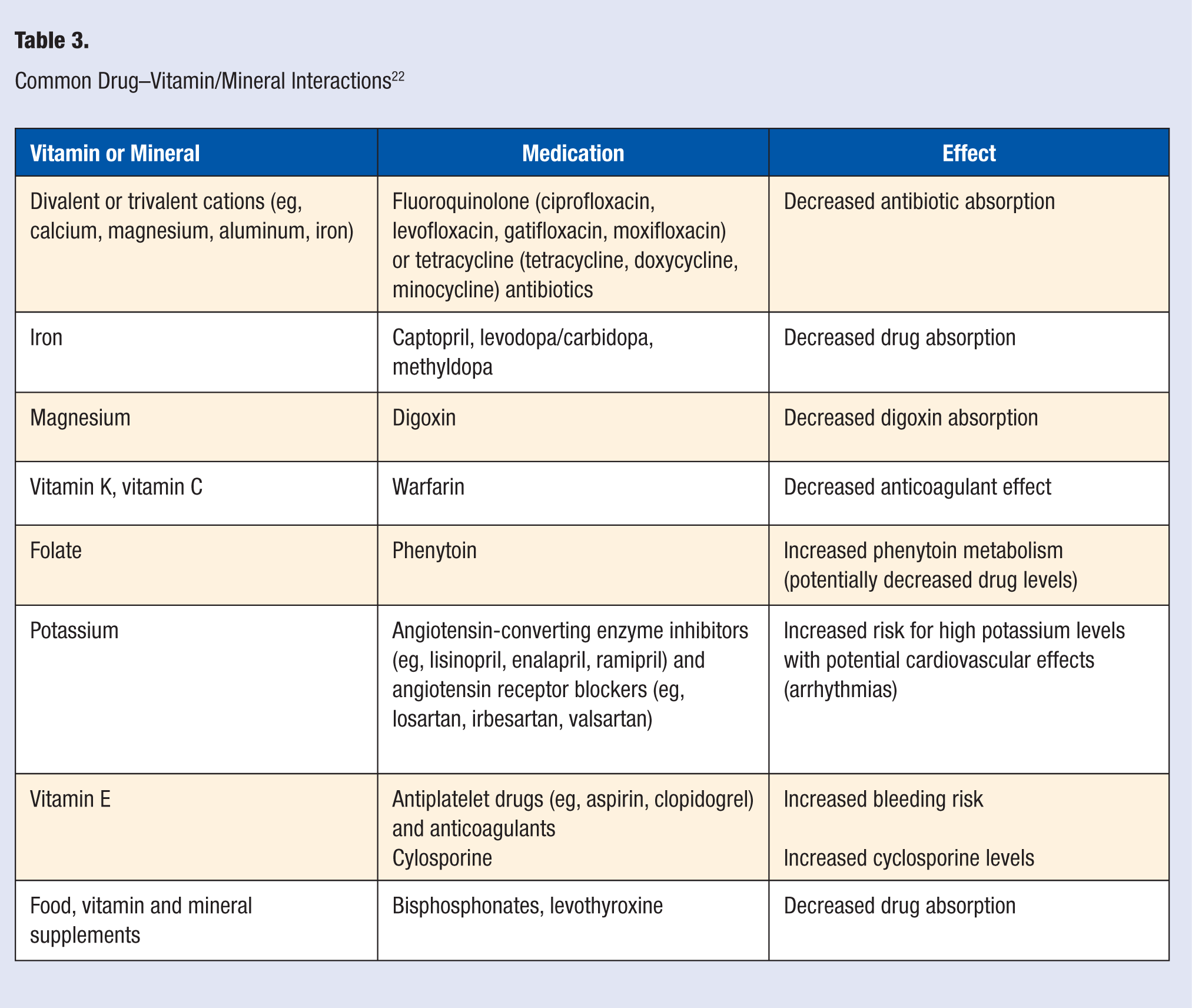
Many clinicians’ knowledge of drug–nutrient interactions is lacking, and the pharmacist can play an active role in assessing patients’ supplement use and the potential for interactions with their medication regimens. For example, multivalent cations (calcium, magnesium, iron) can affect the absorption of many prescription medications, including certain antibiotics (eg, fluoroquinolones and tetracyclines), leading to the potential for inadequate antibiotic absorption, therapeutic failure, and resistant infections. The pharmacist can help patients determine proper timing of administration to avoid such drug–nutrient interactions, or recommend other therapeutic options that avoid a potential interaction. Table 3 summarizes some of the more common and clinically significant drug–nutrient interactions.
Common Drug–Vitamin/Mineral Interactions 22
Pharmacotherapy in Smoking Cessation
Cigarette smoking is a lifestyle habit that is the primary known preventable cause of death in the United States, accounting for approximately 1 out of every 5 deaths in the country every year.23,24 Despite the known adverse health consequences of cigarette smoking, about 20% of adults continue to be current smokers. 25
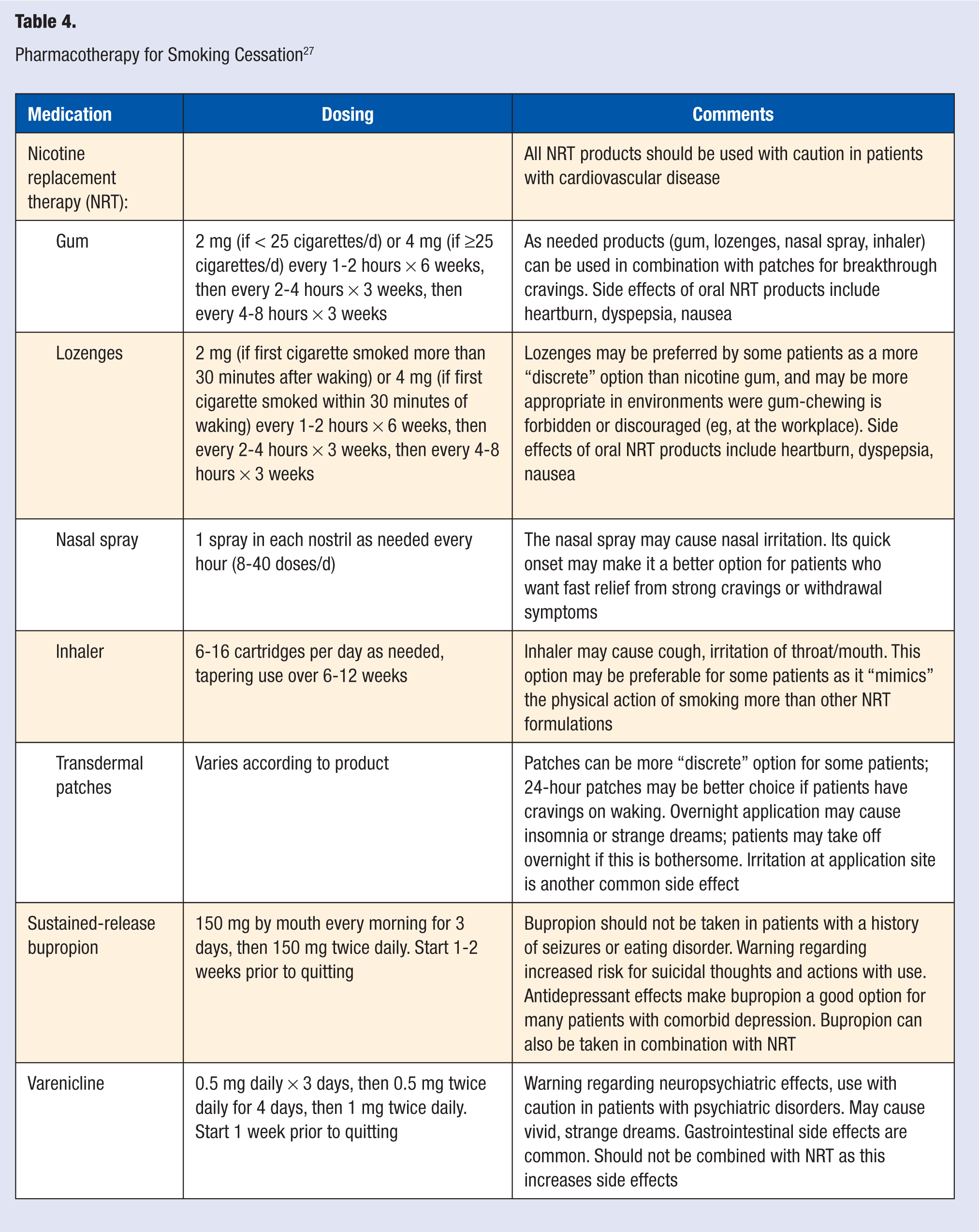
Although many patients may attempt to quit smoking without the assistance of counseling or pharmacotherapy, the chances of a successful quit attempt are increased with both, especially when used simultaneously. 26 Pharmacotherapy options for smoking cessation include nicotine replacement therapy (NRT), which helps reduce nicotine withdrawal by exposure to low levels of nicotine; bupropion, an antidepressant that primarily affects dopamine and norepinephrine levels in the brain; and varenicline, a novel drug class that interacts with nicotine receptors in the body to reduce cravings and withdrawal symptoms. Table 4 reviews the current FDA-approved pharmacotherapy options for smoking cessation.
Pharmacotherapy for Smoking Cessation 27
Nicotine Replacement Therapy
Nicotine replacement therapy products are available in multiple formulations (see Table 4). NRT use results in quit rates of about 25%, which is almost twice the rate seen with placebo. 26 The combination of the nicotine patch and as needed products results in a higher quit rate than either product alone. 26
Bupropion
Bupropion is a prescription medication originally marketed as an antidepressant but later approved for smoking cessation as well. Bupropion alone results in a 24% abstinence rate; this rate is higher (about 29%) when it is used in combination with nicotine patches. 26 Bupropion should not be taken by certain people, including those with eating disorders or a history of seizures, and the labeling has a warning regarding mood changes reported in people taking the drug. 28
Varenicline
Varenicline is the newest medication for smoking cessation. Varenicline use is associated with a quit rate of about 33%. 28 Similar to bupropion, varenicline has a warning regarding mood change and suicidal thoughts and actions that have been reported in people taking the drug, and more recently, there have been data regarding an increased rate of cardiovascular events compared with placebo. 29
Other Pharmacotherapy Options for Smoking Cessation
Nortriptyline, an antidepressant, and clonidine, a medication with a primary indication for treating high blood pressure, are also used for smoking cessation, although they are not approved by the FDA for this use and are not considered first-line therapies. 26 These agents are usually reserved for people unable to take or unsuccessful with other smoking cessation medications.
Smokers should discuss pharmacotherapy options with a health care provider to assist them with a quit attempt. Pharmacists can also help encourage patients in their quit attempt and provide support to increase their chances for success. In some instances, there are pharmacist-run clinics that can facilitate quitting. Although all of the above medications have been shown to increase a smoker’s chances of quitting successfully, they all have potential side effects and may not be appropriate for use in certain patients. NRT products are the most commonly used pharmacotherapy for smoking cessation, and because many of these products are available over the counter, pharmacists are in the position to advise patients on their use and choose a formulation that best meets their needs.
Pharmacotherapy for Mood Disorders
There are many different kinds of medications used for treating various mood-related disorders, including depression, bipolar disorder, and various anxiety disorders. A comprehensive review of all the pharmacotherapy options and mood-related disorders is beyond the scope of this article; however, we will address some common issues since there is so much pharmacotherapy that is prevalent in this arena. Medications alone or in combination with other therapies (such as psychotherapy or cognitive behavioral therapy) have been shown to have a beneficial effect on functioning and quality of life in people with diagnosed mood disorders. Many prescription medications, such as antidepressants (selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, tricyclic antidepressants, bupropion, and others) affect mood by altering levels of chemicals in the brain (primarily serotonin, norepinephrine, and dopamine).
If pharmacotherapy is appropriate, choice of agent will often be guided by the side effect profile and patient preference. Pharmacotherapy for mood disorders is often prescribed in small amounts, especially on initiation of therapy. This practice can result in frequent interaction between the patient and the pharmacist to routinely acquire medication. Having knowledge of a patient’s medication profile places the pharmacist in a place in therapy where monitoring can occur. If the patient reports a medication intolerance or an adverse effect on mood, the pharmacist can notify the physician of the encounter.
There are several natural, nonprescription products that are touted for their potential effects on mood. Omega-3 fatty acids, St. John’s wort, and S-adenosyl-
Although pharmacotherapy can help in the treatment of mood disorders, it can also have detrimental effects on mood. Examples of medications that can have psychiatric adverse effects include antiepileptic drugs and, perhaps paradoxically, antidepressants. Both these drug classes have strong warnings regarding an increased risk for depression and/or suicidal thoughts or behavior. In fact, the FDA requires that these drugs be dispensed with a patient medication guide that reviews these risks for the patient. Other medications that have been reported to cause psychiatric adverse effects such as depression, anxiety, and mood or personality changes, include corticosteroids, beta-blockers, hormonal contraceptives, benzodiazepines, and fluoroquinolone-type antibiotics. 34 Although many medications may have psychiatric side effects listed in their labeling, this does not necessarily mean that a causal relationship has been established. Interactions between patients and pharmacists can be sentinel events that can identify both success and problems with therapeutic efficacy.
Ultimately, people who suffer from psychiatric or mood conditions or who suspect they may be having a psychiatric side effect to a drug should discuss this and be routinely monitored by their health care provider.
Weight
The struggle to maintain weight in our society is one of the largest health problems we face as a population. It has been estimated that two thirds of American adults suffer from obesity. 35 Obesity encompasses 3 phases of lifestyle management with loss of control in the following areas: diet, physical activity, and behavior. 36 Diet is a concept that many people cannot fully embrace.
One way to influence diet is through behaviors that encompass food selection. Filling the home with foods that have been available since the beginning of time such as items that are not processed, packaged, or laden with unpronounceable additives is a key step in living a healthy lifestyle and provides the infrastructure for weight control and positive lifestyle behaviors. 37 Motivational interviewing and exercise programs are also key concepts needed for weight loss prior to seeking pharmacotherapeutic measures. 38 It is easy to make a statement such as “you need to lose weight.” It is more difficult to work with patients to understand what motivates them and what, if any program, whether dietary or exercise, may be beneficial to facilitate a lifestyle change. Pharmacists who establish relationships with their patients have the opportunity to help patients help themselves toward a healthier lifestyle by gaining knowledge of dietary programs available as well as various forms of exercise and movement regimens. It may be unhealthy for a patient to be on a “fad” diet and drastically increase their exercise regimen. This scenario, and others, may lead to an unhealthy situation for the patient and may exacerbate adverse drug reactions should the patient be on medications.
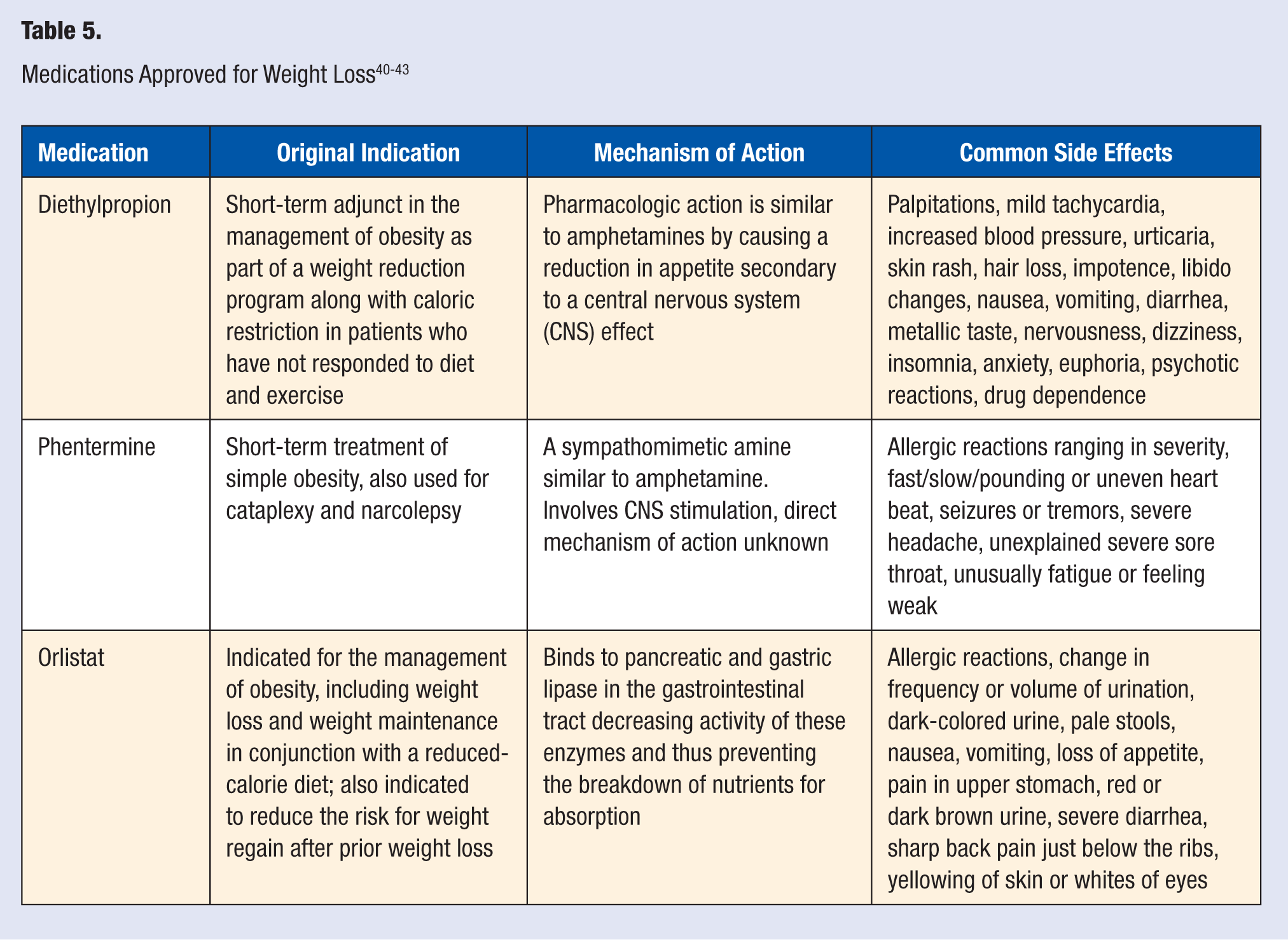
Pharmacotherapy is typically regarded as the second to last step of obesity management prior to surgical intervention. Failure of gaining control of obesity may result in other chronic disease manifestations such as hypertension, type 2 diabetes mellitus, hyperlipidemia, heart disease, pulmonary disease, hepatobiliary disease, cancer, and psychosocial complications. 35 There are a host of medications that people look to for weight reduction; however, only 2 have been approved by the FDA for long-term use specifically for weight reduction. Sibutramine, a medication that suppresses appetite in the brain by altering monoamine neurotransmitters, was withdrawn from the market in 2010 because of an increased risk of strokes and cardiovascular events. Orlistat, the newer of the 2 agents, uses a distinctly different mechanism of action by reducing the absorption of selected macronutrients from the gastrointestinal tract, namely fat. Other medications that may be used for weight loss over the short term include phentermine and diethylpropion, amphetamine-like medications that suppress the appetite. Other mechanisms are currently being researched and there will hopefully be some positive pharmacological outcomes through research in the future.36,39 Table 540-43 reviews the FDA-approved weight loss medications.
Some medications, such as fluoxetine or metformin, may be used for other indications but can also result in weight loss, a positive side effect for many patients. On the other hand, many medications, including atypical antipsychotics, some antidepressants (eg, paroxetine), and antidiabetics can cause significant weight gain.
Pharmacists are in a position to inform patients about the potential side effects, efficacy and safety concerns of weight loss medications as well as other medications with weight-related side effects. Very often, patients’ expectations for weight loss from pharmacotherapy alone far exceed actual weight loss achieved in clinical trials. However, patients should be informed that even just a 5% to 10% reduction in body weight has been associated with improvement of many obesity-related issues. 44 Unfortunately, there are a multitude of nonprescription products that are touted for weight loss that have no evidence regarding efficacy. Patients routinely pour dollars into these products for hope of an instant cure to the problem. If efficacy and safety data are lacking, pharmacists should discourage use of such products and instead encourage healthy behaviors.
Sleep
Insomnia is the most prevalent sleep disorder, affecting 10% to 15% of the US population. 45 In today’s technologically complex society with 24/7 stimulation available via computers, television, cell phones, and gaming systems, sleep disorders affect not only adults in our society but also children because of overstimulation of brain activity. 46 Sleep deprivation has been associated with depression, weight gain, automobile accidents, decreased class attendance in school, decreased overall productivity, and mood and behavior issues. 47
Nonpharmacologic measures used to improve or promote sleep should always be the first line of therapy for sleep disorders. Increasing physical activity during the day, decreasing caffeine intake, managing anxiety, minimizing aches and pains, avoiding jet lag, and avoiding alcohol intake within 3 hours of bedtime are some common approaches prior to consideration of pharmacotherapy. 48
The first pharmacological step that patients take in treating sleep disorders often involves over-the-counter options such as alcohol or antihistamines. Alcohol aids patients in falling to sleep; however, in general, it is associated with sleep disturbances throughout the night. This practice may also lead to abuse and subsequent withdrawal, which has an enormous impact on sleep. Antihistamines that have a significant anticholinergic effect such as diphenhydramine may prove useful in an intermittent basis; however, when used chronically, patients may build up a tolerance to them rendering them less effective. These agents may be especially problematic in the elderly, in whom the anticholinergic side effects associated with use may exacerbate other health related issues. 49
The benzodiazepines and nonbenzodiazepine sedative hypnotics are prescription remedies that have proven to be the most useful in patients with insomnia. The most commonly used prescription agents include zaleplon, zolpidem, triazolam, eszopiclone, temazepam, and lorazepam. The goal with these agents is to use compounds with the shortest half-life, resulting in low or undetectable serum concentrations during the daytime hours and minimizing next day effects such as daytime drowsiness or a “hangover effect.” In general, there are limited data on long-term use of most of these agents and there are significant concerns regarding rebound insomnia and tolerance with prolonged use, particularly with the benzodiazepines. The general recommendation is to use these pharmacologic agents for the shortest period of time needed, and to use the minimum effective dose and taper when conditions allow. 50
Ramelteon is a melatonin receptor agonist that helps patients fall asleep and stay asleep. 51 This pharmacotherapeutic intervention has a mechanism of action that is unique from the other prescription sedative hypnotics. Ramelteon essentially mimics the effects of melatonin, an endogenous hormone involved in the regulation of the sleep–wake cycle. Additional agents used for insomnia that are less expensive and have no potential for abuse compared with the benzodiazepines and nonbenzodiazepine sedative hypnotics are the heterocyclic antidepressants such as trazodone, amitryptyline, and doxepin.
Many medications can also contribute to insomnia; these include stimulants such as methylphenidate, amphetamine, and over-the-counter decongestants such as pseudoephedrine. If a patient is complaining of insomnia, the pharmacist should consider the possibility that this may be a side effect of a medication and ask about such use. Discouraging use of such medications or counseling patients about administration time to avoid this side effect can have a profound effect on eliminating insomnia. The same approach is routinely adhered to for caffeine intake in patients who complain of not being able to sleep.
Conclusion
In conclusion, pharmacotherapy can have many benefits for patients in multiple lifestyle areas, but it also has the potential for detrimental effects. Pharmacists are often the health care provider most accessible to patients. Their extensive knowledge of over-the-counter and prescription medications and their expertise in assessing the appropriateness of self-care for individuals put them in a position to have a profound effect on patients’ health. Educating patients and health care providers about the risks and benefits of pharmacotherapy and making health care decisions that consider the entire patient and their medication regimen are essential roles of pharmacists in all practice settings.