
Abstract
An estimated 10% of head and spinal cord injuries are due to sports-related activities. As the popularity of sports increases so does the incidence of sports-related injuries. In recent years, concussion has received significant media attention as high-profile athletes have come forward to share their experiences and long-term struggles with this specific type of traumatic brain injury. Public health initiatives such as the “Heads Up: Concussion in Youth Sports” program run by the Center for Disease Control and Prevention have been developed to raise awareness regarding concussion injuries. These programs target not only athletes themselves but also include coaches, medical professionals, and parents to ensure that all individuals involved in sports, be it directly or peripherally, obtain the education required to prevent, correctly diagnose, and treat concussion. They are a testament to how elementary our understanding of concussion continues to be. They also demonstrate that misinformation and lack of awareness pose a significant obstacle to proper diagnosis and treatment. In this review, the authors discuss concussion both as a medical challenge and as a public health concern. The authors examine the definition as well as diagnostic criteria that have been agreed on during the Third International Conference on Concussion in Sport in Zurich 2008. Furthermore, current options and limitations in preventing and treating concussion are reviewed. Finally, the 2 most commonly used standardized grading systems as well as guidelines for return to play are reviewed. Overall, this article will offer health care providers and members of the general public alike the current understanding of concussion.
ports are an integral part of American culture and have been throughout most of our history. With increased sports participation especially by women and with a heightened public awareness of sports-related head injury, a greater emphasis has been placed on the safety of the participants. This holds true not only for professional athletes but perhaps more importantly for amateur and youth participants. It is estimated that 10% of head and spinal cord injuries are due to sports-related activities. 1 Approximately 1.4 million people in the United States sustain a traumatic brain injury (TBI) each year, and 5.3 million Americans currently require long-term or lifelong help with activities of daily living secondary to TBI.2,3 The Center for Disease Control and Prevention (CDC) estimates 207 830 emergency room visits per year during the period 2001 to 2005 were due to nonfatal sports-related head injuries. 4 These data confirm the clinical significance of sports-related head injuries and the need for stronger regulations, as well as a redirection of focus toward a better understanding of the injury process and subsequent development of preventative measures and management protocols. In 1904, President Teddy Roosevelt took a first step in this direction by calling for rule changes to improve safety after 19 athletes were killed or paralyzed playing football. Gang tackling and mass formations were banned and the forward pass was allowed transforming the game away from its roots in rugby. As a direct consequence, the National Collegiate Athlete Association (NCAA) was formed and stricter regulations were implemented, which led to significant improvement in player safety and a reduction in sports-related head injuries. Nevertheless, the risk of sports-related head injuries remains high with stronger and faster athletes and equipment enhancements, the modern helmet with face guard, which may paradoxically increase risk taking and result in blows to the head that have higher energy.
In recent years, concussion has received significant media attention as high-profile athletes have come forward to share their experiences and long-term struggles with this specific type of traumatic brain injury
Studies of high school athletes in 10 different sports over a 3-year study period revealed that all were at risk for concussive injuries. About 63% of concussions occurred in boys’ football, 10% in wrestling, 6% in boys’ and girls’ soccer, and the rest in boys’ and girls’ basketball, softball, baseball, field hockey, and volleyball. 5 Despite the fact that concussion is the most common form of TBI, our understanding of its mechanism and prevention remain inadequate. In addition to lack of information, there is also significant misinformation provided to players, coaches, and health care professionals that can lead to inadequate treatment and follow-up. Recently, the topic has garnered more media attention as high-profile athletes have come forward to speak about their experiences.
It has been estimated by PubMed Central that more refereed publications on sports-related concussion have appeared since the year 2000 than in all the previous years combined. 6 Since 2001, there have been 3 international conferences on concussion in sports: Vienna in 2001, Prague in 2004, and Zurich in 2008. They were convened to discuss and formulate not only a treatment strategy but also to determine a working definition of the syndrome with a goal of standardizing the management of concussive injuries. Proceedings were simultaneously published in multiple journals.7,8 Extensive documents on concussion have also emerged from the NATA (the National Athletic Trainers’ Association) position statement, 9 published in 2004, and the ACSM (A Consensus Statement on Concussion and the Team Physician, 10 which appeared in 2006). In addition, entire issues of the Clinical Journal of Sport Medicine (July 2001) 11 and the Journal Athletic Training (October 2001) 12 have been devoted to the subject. The senior author on this article has been fortunate to be a member of the writing group for all 5 publications.
Efforts have also been increased in educating parents, coaches, and the general public on signs and symptoms of concussion; its potential long-term sequelae; and prevention of permanent neurological deficits. The CDC has published multiple tool kits for parents, athletes, and coaches to raise awareness and improve the detection and treatment of concussion. Though media attention has often been focused on American football and boxing as the sports with the most potential for brain injury and permanent deficits, it is important to recognize that many other sports may also lead to concussion. In 2007, Gessel et al showed that while football had the highest concussion rate among high school students, partial contact sports such as soccer also had high rates. Interestingly, the rate for concussion in girls’ soccer was close to that of football and significantly higher than boys’ soccer. 13 Even more impressive was the fact that the rate of concussion was found to be 300% higher in girls’ basketball when compared with boys’ basketball. 13 These data support evidence that suggests that the incidence of concussion may be higher and recovery slower in girls versus boys playing the same sports and in our youth compared with adults.14-17
What Is Concussion?
During the Third International Conference on Concussion in Sport, held in Zurich 2008, concussion was defined as “a complex pathophysiological process affecting the brain induced by traumatic biomechanical forces.” 8 It can be caused either by a direct blow to the head or by an impulsive force that lead to acceleration of the head without direct blunt trauma to the cranium. In the majority of cases, the acute clinical findings are transient and resolve spontaneously. Contrary to common belief, loss of consciousness usually does not occur, and the absence of a reported loss of consciousness does not preclude the diagnosis of concussion. Finally, concussions do not produce structural abnormalities that can be detected with available imaging modalities. 8
From a biomechanical standpoint, acceleration–deceleration forces and linear as well as especially rotational forces have been implicated in causing concussive injuries. Depending on the severity of impact, the individual may sustain a coup or countercoup injury. In a coup injury, the damage occurs at the site of impact, whereas a countercoup injury leads to brain injury on the side opposite the impact.
It is estimated that 90% of sports-related concussions occur without loss of consciousness. 18 Overall, detection of concussion is made difficult by the lack of clear diagnostic factors, laboratory tests, or imaging modalities. Furthermore, the diagnosis is often complicated by the fact that clinical symptoms may be short-lived and easily ignored. The most common signs and symptoms are headaches, dizziness, confusion, disorientation, and blurred vision. In 2000, Guskiewicz et al reported the rate of loss of consciousness and headaches in 1019 cases of concussion injuries as 8.9% and 86%, respectively. 19
Importance of Awareness and Education on Concussion
In recent years, more athletes have come forward to share their experiences regarding concussion and how it has affected their health and lives. These intimate and honest accounts of the severity of long-term effects on the health and quality of life of the affected individuals have helped raise increasing interest in the subject. Sadly, despite an increase in attention on concussion, the injury often remains undiagnosed. In part this is due to a culture of “toughness” and “team sacrifice” that is pervasive in sports and is slow to change; however, it may also be due to underestimation of the seriousness of concussive injuries and failure to realize that a concussive injury has been sustained.20,21
As underreporting and lack of recognition continues to be a major obstacle in tackling this problem, it is imperative for health care professionals to focus on maintaining a low threshold for evaluating affected individuals for possible concussion. Furthermore, it is the clinician’s responsibility to provide stringent follow-up and educate his/her patients on this topic. Roux et al showed that a more rigorous follow-up protocol generally results in a higher percentage of athletes reporting concussion. 22 Educational programs are required to eliminate the misconception that concussive injuries are always minor and self-limiting. Instead, it should be emphasized that they may produce varying degrees of lifelong changes in neurological function, which may be delayed in onset. These changes vary in degree from transient headaches to serious neurological deficits such as persistent memory loss and emotional disturbance, and in rare cases they can be lethal as in second impact syndrome (SIS). Though signs of depression are common in individuals with concussion, the exact relationship between the 2 entities is not completely understood. In 1988, Schoenhuber and Gentilini reported a prospective case–control study in which individuals who had experienced a concussion were at a higher risk for developing depression compared with matched controls. The difference was statistically significant. 23 Since then no other study has established a clear cause-and-effect type of relationship. It is undeniable, however, that a large number of individuals experiencing a head injury will show signs of depression after the injury.
Prevention
Prevention of all serious concussive injuries is unrealistic particularly in contact sports; however, it remains an important goal since epidemiological studies show that the first concussion may increase the likelihood of a second concussion by up to 3-fold. 19 This is particularly significant as the repeat injuries may be more severe than the initial one, and in rare cases may be fatal.
Protective head gear such as helmets and mouth guards have long been recommended for contact sports, but their effectiveness in preventing concussion has not been clinically proven. For example, helmets are important in preventing skull fractures and direct injury to the head, but they have not been shown to prevent concussions despite the fact that they lessen the impact that is being transmitted to the brain itself. In fact, there is concern that protective equipment can result in more aggressive play and therefore an increase in the incidence of injuries. 24 Mouth guards have also not been shown to reduce or change the incidence of concussion injuries; however, they can prevent orofacial and dental injuries.
Despite the shortcomings of protective gear, screening questions regarding their proper and consistent use should be incorporated in routine clinic visits. The equipment should fit properly and it needs to meet the National Operating Committee on Standards for Athletic Equipment or American Society for Testing and Materials standards. 9 It is important that regulations be established that ensure adherence on both the professional and amateur levels.
In 2005, the CDC implemented a national concussion awareness and education initiative in collaboration with the Children’s Health Act of 2000. As part of this initiative, multimedia tool kits titled “Heads Up: Concussion in High School Sports” were developed for high school coaches and certified athletic trainers and directors. In addition to raising awareness and providing educational materials, the objective of the initiative was to allow coaches a means to inform others on the subject matter and to help them develop the skills to screen for and recognize concussion among their athletes. 4 According to a follow-up study conducted by the CDC, this program lead to a positive change in knowledge base, attitude, behavior, and skills toward concussion awareness. Most important, the tool kit solidified the understanding that concussion is a serious injury and needs to be addressed appropriately. 25 The study also confirmed that there remains skepticism among athletes, their parents, and coaches of the seriousness of concussions and a tendency toward downplaying its effects. 25 Recently, a number of states have enacted legislation with regard to concussion education and qualification for who can return an athlete to play after a concussion.
Evaluation
Clinicians should be aware that a wide array of mechanisms can lead to concussive injuries and that these injuries can present with a broad range of symptoms. Once any kind of potential head trauma has been sustained or head injury is suspected, it is important to properly evaluate the extent of the injury and to rule out other more serious processes. Potential neurosurgical emergencies such as subdural and epidural hematomas should be considered and, when appropriate, a computed tomography (CT) scan of the head needs to be ordered.
Several screening tools have been proposed for the management of sports-related concussion. Proper screening will allow for expeditious and appropriate management of the injury and prevent further damage. In particular, it will decrease the likelihood of a possibly fatal second impact injury. Finally, it will allow for long-term monitoring of symptoms and aid in determining the rate of improvement or worsening. In 1997, McCrea et al introduced a standardized assessment tool for concussion (SAC) that would be time efficient and easy for nonmedical professionals, yet accurate and precise in detecting concussion on the sidelines. 25 This assessment tool tests an individual’s orientation, immediate and delayed recall, and concentration using a battery of questions and physical tasks. Follow-up studies revealed that individuals who had sustained a concussion scored significantly lower than nonconcussed controls as well as their own baseline. Interestingly, affected individuals showed significant improvement in their scores within 48 hours of injury. 26 Overall sensitivity and specificity of the tool were 95% and 76%, respectively, which signified the utility of the assessment tool not only for identifying concussion but also for tracking progression of the individual. This tool has not been found to retain its high sensitivity and specificity beyond 48 hours.
One of the aims of the Second International Conference on Concussion in Sport, held in Prague in 2004, was to develop a standardized concussion assessment tool (SCAT) that was subsequently revised in 2008 during the third international meeting. This tool itself was created by combining previous existing methods including the SAC, the American Academy of Neurology assessment tool, and the sideline concussion check.27,28
The revised assessment tool SCAT2 consists of 8 parts including symptoms and signs, particularly cognitive ability, balance, coordination, Glasgow Coma Score, and Maddocks score. The Maddocks score uses recall of recent events to assess an individual for concussion. 16 With the exception of the Maddocks score, the remainder of the SCAT2 should be performed until the individual’s condition is stable. Changes in the score may indicate improvement or worsening of the individual’s condition. A pocket-sized abbreviated version of the SCAT2 was created for immediate sideline screening. This tool should not be used as the only form of diagnosis or severity of injury. Accurate functional evaluation requires knowledge of the individual’s baseline. Since this function varies significantly among individuals, baseline neuropsychological and SCAT2 testing would ideally be conducted on every athlete prior to any head injury.
Clinicians should be familiar with differences in athlete evaluations in an acute setting such as the sideline of a sports field or in a more controlled clinical setting where subacute or chronic symptoms may be determined. Evaluations during an ongoing game need to be quick and efficient to allow for prompt and accurate diagnosis, yet detailed enough to allow the clinician to rule out potential life-threatening injuries. In an office setting, it is important to take a complete history including a history or family history of migraines and question the patient about possible injuries sustained in the past that may have been minor enough to forget. These should not only include the number of injuries experienced but also the severity, the age at which the injury occurred, and the activity during which it occurred. Additionally, the clinician should be aware that conditions such as learning disabilities, attention deficit disorder/attention deficit hyperactivity disorder, migraine headaches, anxiety, mental illness, and/or depression can be both resulting effects of the injury as well as important predictors of outcome from a current concussion if they predated the injury. 10
Grading
As of 2001, about 25 different classification schemes had been published. Of these, the most commonly used are the American Academy of Neurology (AAN) and the Cantu scale.29,30 In addition to determining the severity of a sustained injury, a standardized grading system is also necessary to establish guidelines as to when an athlete can safely return to playing sports. However, even with the establishment of a grading system it is important to recognize that no 2 concussions are alike. Factors such as severity of the impact, the actual tissue damage, time needed to recover, and the number of previous concussions dictate individual concussion management.
While there currently is no clear consensus on the superiority of one system over the others, several faults with the AAN scale have it currently being revised. The components of the individual grading systems vary and their prognostic value remains questionable. For example, several of these grading systems including AAN continue to ascribe loss of consciousness (LOC) and amnesia to the highest grade, yet Guskiewicz et al found that LOC and amnesia occurred in only 9% and 27% of concussions, respectively. 19 More important, LOC of up to 1 minute has not been shown to significantly change the injury severity. 31 With respect to amnesia, some data indicate that amnesia correlated with abnormal neuropsychological testing at 48 hours postinjury and was a good indicator of concussion duration. 31 However, several recent studies failed to reveal any correlation between amnesia and duration of symptoms or neuropsychological testing at 3 to 96 hours postinjury.32-35Despite these conflicting data, neither LOC nor amnesia should be ignored if experienced by an individual. In 2009, Dischinger et al showed that postconcussive syndrome, which was defined as persistence of at least 4 symptoms long-term, was most commonly predicted by anxiety as well as noise intolerance compared with any other symptoms of concussion. 35
Among the various grading systems, the 2 most cited are the AAN Concussion Grading Scale (Table 1) and the Cantu Grading Scale (Table 2). The AAN Concussion Grading Scale differentiates between 3 grades: mild, moderate, and severe. Based on this system, any LOC will automatically classify a concussion as severe. Grades 1 and 2 may both present with transient confusion and absence of LOC and differ only in the duration of symptoms. If the symptoms resolve within 15 minutes, the concussion is classified as mild, otherwise it is classified as moderate. In comparison, the Cantu Evidence-Based System for Concussion classifies concussive injuries into mild, moderate, and severe categories based on a combination of duration of LOC, posttraumatic amnesia (PTA), and postconcussive signs and symptoms (PCSS). A mild concussion, therefore, signifies the absence of LOC as well as PTA and PCSS of less than 30 minutes and 24 hours duration, respectively. A moderate concussion is defined as the presence of LOC for less than 1 minute or PTA of greater than 30 minutes but less than 24 hours and PCSS of greater than 24 hours but less than 7 days. Finally, severe concussion is defined by LOC of greater than 1 minute duration or PTA of greater than 24 hours or PCSS of greater than 7 days.
American Academy of Neurology Concussion Grading Scale
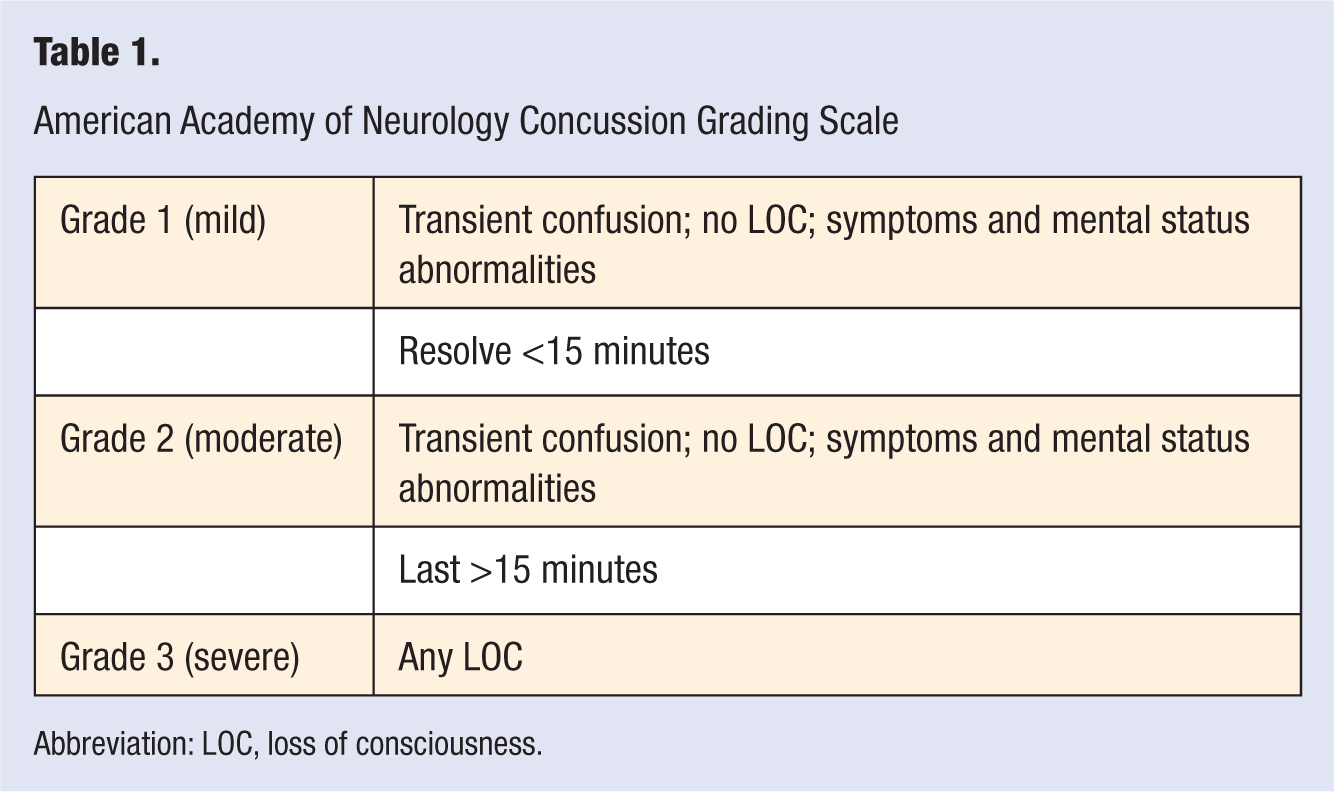
Abbreviation: LOC, loss of consciousness.
Cantu Evidence-Based Grading System for Concussion
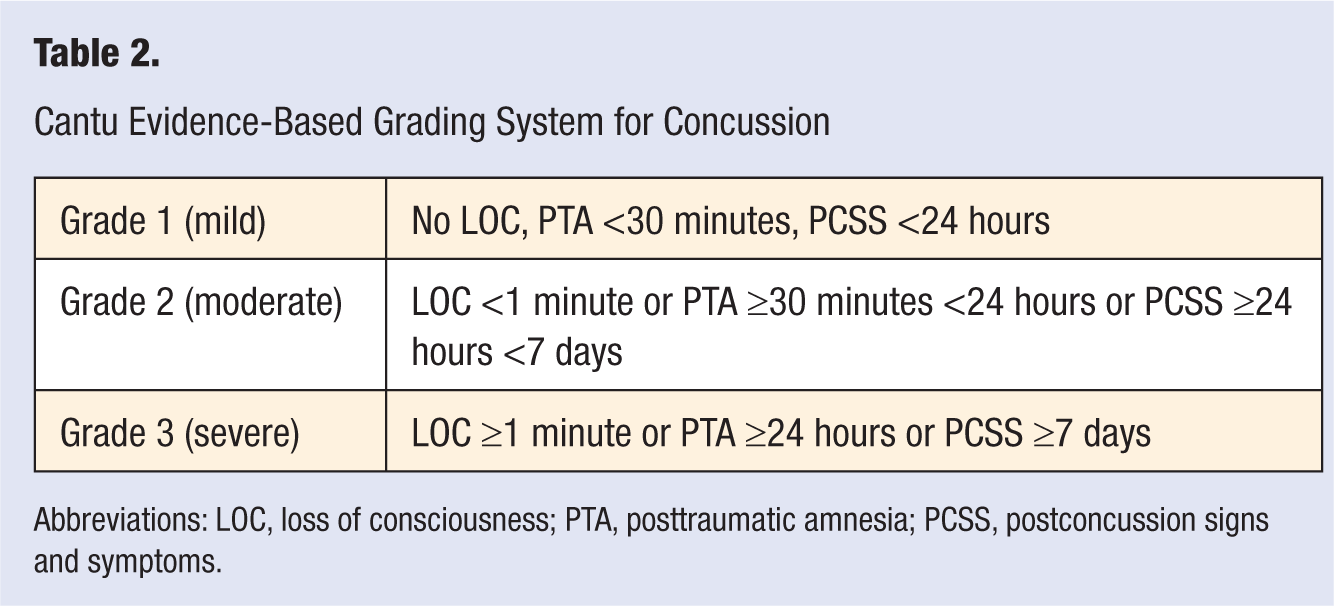
Abbreviations: LOC, loss of consciousness; PTA, posttraumatic amnesia; PCSS, postconcussion signs and symptoms.
Return to Play
One of the most important aspects of concussion management is determining when it is safe to return to play (RTP). Cantu published the first RTP guidelines in 1986. 36 Since rest is important in the recovery process, it is crucial that the individual has had adequate time to recuperate. In addition to injury severity, it is important to determine if previous concussions have occurred. Current guidelines for RTP remain controversial with regard to how long an athlete should be asymptomatic before RTP. The only recommendation that has been universally accepted is that while still symptomatic, athletes should not be allowed to return.
During the Third International Conference on Concussion in Sport in Zurich in 2008, the panel agreed that in order for an athlete to be cleared, he/she should follow a graduated protocol of RTP. In this stepwise approach, every stage ideally would take 24 hours, and only if the athlete were able to remain symptom-free would he/she be allowed to progress to the next level. Should he/she become symptomatic during any of these stages then the individual would be returned to the previous stage. For example, an individual with a grade 3 concussion based on the Cantu Grading Scale and LOC greater than 1 minute would not be allowed to RTP until he/she had been asymptomatic for a total of 2 weeks or longer depending on the prior concussion history and previously mentioned modifiers.
In general, same-day RTP is strongly discouraged based on the Zurich Consensus Statement; however, guidelines allow adult athletes to return to the game on the same day if they are completely asymptomatic. 8 It is believed that adult athletes with experienced physicians and neuropsychologists present may be assessed more accurately and that these athletes may recover from mild concussions more quickly. It is strongly advised to take a more conservative approach with younger and more inexperienced players. 37 Despite these recommendations, a recent study by Yard and Comstock found that 40.5% of high school athletes returned prematurely based on AAN guidelines. 38 Individuals who have sustained 2 or more concussions within 1 season should be treated very carefully. As a general rule, individuals without a concussion history or modifiers may be allowed to RTP after completing a graduated RTP protocol (1-2 weeks) if he/she has sustained 2 mild concussions (Cantu grading scale), and after 1 month if he/she has sustained 2 moderate concussions (Cantu grading scale). After 3 concussions regardless of grade or 2 severe concussions, the athlete should not be allowed to RTP for the remainder of the season and should also undergo imaging with CT or magnetic resonance imaging (MRI) to rule out an intracranial process. However, each athlete’s care must be individualized.
Second Impact Syndrome
What Saunders and Harbaugh 39 called “the second-impact syndrome of catastrophic head injury” in 1984 was described by Schneider in 1973. 40 The syndrome occurs when an athlete who sustains a head injury—often a concussion or worse injury, such as a cerebral contusion—sustains a second head injury before symptoms associated with the first have cleared.41,42 Typically, the athlete suffers postconcussion symptoms after the first head injury, and before these symptoms resolve, which may take days or weeks, the athlete returns to competition and receives a second blow to the head. The second blow may be remarkably minor, perhaps only involving a blow to the chest that jerks the athlete’s head and indirectly imparts accelerative forces to the brain. Affected athletes may appear stunned but usually do not lose consciousness and often complete the play. They usually remain on their feet for 15 seconds to 1 minute or so but seen dazed, like someone suffering from a grade I concussion without the loss of consciousness. Often, affected athletes remain on the playing field or walk off under their own power. What happens in the next 15 seconds to several minutes sets this syndrome apart from a concussion or even a subdural hematoma. Usually, within seconds to minutes of the second impact, the athlete— conscious yet stunned—quite precipitously collapses to the ground, with loss of eye movement and evidence of respiratory failure.
Saunders’s case involved a 19-year-old college football player who suffered a brief LOC after a fistfight. Four days later he was allowed to RTP only to walk off the field and collapse. Imaging revealed extensive intracranial swelling with significant midline brain shift. Despite aggressive management including a hemicraniectomy, the patient eventually died and was found on autopsy to have extensive anoxic changes. 39 Although this is considered the initial report of SIS, there was no report of trauma during the game he played in 4 days after the initial injury. Understandably, SIS is the most feared consequence of concussion, which may occur after sustaining multiple concussions in short succession. The short interval between concussions prevents brain recovery from the first injury and results in potentiation of concussion severity. Much concussion prevention and management is aimed at preventing this devastating injury.
The pathophysiology of SIS is still unclear, but it is believed that loss of cerebral blood flow autoregulation leads to vascular engorgement, venous congestion, and increased intracranial pressure. This results in cerebral herniation if not treated in a timely manner. Once brain herniation and brain stem compromise occur, ocular involvement and respiratory failure precipitously ensue. Demise occurs far more rapidly than usually seen with an epidural hematoma. MRI and CT scans are the neuroimaging studies most likely to demonstrate the SIS. Although MRI is more sensitive to traumatic brain injuries, especially true edema, the CT scan is usually adequate to show bleeding or midline shifts of the brain requiring neurosurgical intervention. Recently, 18 cases of SIS in conjunction with a small subdural hematoma have been published.43,44 Not all agree with calling this entity the second impact syndrome as not all published cases have the first impact well documented. McCrory proposed abandoning the term second impact syndrome and instead calling these cases “syndrome of diffuse cerebral swelling.” 45
Chronic Traumatic Encephalopathy
In 1928, Martland was the first to describe chronic traumatic encephalopathy (CTE) or dementia pugilistica. 46 Symptoms included confusion, tremors, and slowing of speech as well as Parkinsonian symptoms and overall mental deterioration. CTE was thought to be primarily present in boxers who had suffered repeated punches to the head. In 1954, Brandenburg and Hallervorden published a neuropathological report showing Alzheimer disease–like changes in a 51-year-old boxer who had suffered from delayed posttraumatic dementia. 47 Since then, various reports have confirmed characteristic neuropathological findings in patients with suspected CTE. These include tau-immunoreactive neurofibrillary tangles (NFTs) and neuropil threads (NTs) and uncommonly diffuse amyloid plaques. Overall, the changes though similar are clearly unique and easily differentiated from those seen in normal aging or Alzheimer’s disease (AD).
CTE has an insidious onset with initial symptoms of deficits in attention, memory, and concentration, which may lead to confusion and disorientation. Further progression results in dementia, poor judgment, irrational behavior, depression, and lack of insight. Changes in behavior as well as new onset of dementia can often be correlated with injury to the medial aspect of the temporal lobe. In addition, affected individuals may eventually develop Parkinsonian symptoms. It is important to realize that it is not the number of concussions but rather the severity of the brain injury that determine whether an individual will develop CTE.
Although it had long been suspected that CTE is not limited to boxers, it was not until 2005 that the first autopsy-confirmed case of CTE in a National Football League (NFL) player was reported by Omalu et al. 48 This individual died of coronary atherosclerotic disease 12 years after his retirement from a 17-year career in the NFL. Interviews with family members revealed that the patient had struggled with memory deficits and was suffering from Parkinsonian symptoms. An autopsy revealed diffuse amyloid plaques and NFTs in the neocortex only. Lewy bodies were not identified, and on gross examination the brain did not reveal cortical atrophy, contusion, hemorrhage, or infarcts. Apolipoprotein E genotyping was performed and the patient’s genotype was determined to be E3/E3. The E4 variant of this gene has previously been implicated in AD susceptibility. 49 In 2006, Omalu et al reported the second autopsy-confirmed case of CTE in an NFL player. Unlike the first case, amyloid plaques were not detected; however, NFTs and NTs were present in all regions of the brain. The apolipoprotein-E genotype of this patient was also E3/E4. 50 In a recent review of 48 reported cases of neuropathologically verified CTE, McKee et al found that NFTs and NTs are seen consistently while amyloid plaques were seen in only 40% of the cases. 51 Since the neuropathological process is still not understood, it is impossible to account for the differences in autopsy findings at this time. Interestingly, from an immunohistochemistry aspect there is significant overlap between CTE and AD. One possibility may be a synergistic path between traumatic injury and AD that leads to a mixed pathology resulting in a clinically more severe presentation. 51 It is evident that more research is necessary to improve our understanding of the processes resulting in CTE. The same article also revealed that even though sports is most often associated with development of CTE, any brain trauma regardless of its etiology may lead to CTE. The cases of spousal abuse and autistic head banging emphasize this. 51
Treatment
To date, our ability to treat and reduce the effects of concussion injuries remains ineffective. With the exception of rest to allow for complete or near complete recovery, there is little else we can offer. Serial testing can be used to track an individual’s progress, but it does not treat the primary problem. Therefore, the best treatment continues to be prevention of concussion and its sequelae. This requires education, public awareness, and cooperation between athletes, coaches, health care professionals, and organized sports. Organizations such as the NFL and NCAA are particularly important as their influence in safety measures and regulations concerning RTP are crucial to both minimizing and preventing TBI.
Future
Cleary, more research is required to improve our understanding of concussive brain injuries. This will entail long-term follow-up of individuals who have sustained concussions as well as investigations on a molecular level to understand the mechanisms responsible for acute and chronic brain injury. On a molecular level, it is crucial to identify pathways that lead to the observed tauopathy in CTE. Understanding of these mechanisms may make it possible to develop treatment options that prevent progressive degeneration and provide affected individuals with a higher quality of life. Finally, identification of possible genetic markers that predispose some individuals to more severe concussive injuries may also be helpful in identifying those at highest risk.
In addition to a better understanding of the pathogenesis of concussion, improvement of imaging techniques that may detect signs of concussion as well as more sophisticated and sensitive neuropsychological testing would be of great value by providing ways to identify concussion more quickly and accurately and therefore allow for more expeditious management. Importantly, these advances would allow for identification of at-risk individuals who could be protected from further injury and therefore from long-term sequela of concussion. AJLM