
Abstract

Introduction
Gram-positive cocci (gram-positive cocci) are common pathogens causing infections after surgery or trauma, such as Staphylococcus aureus. Due to the extensive use of broad-spectrum antibiotics, the resistance of gram-positive cocci is increasing year by year and leads to a high rate of serious infection and mortality of methicillin-resistant gram-positive cocci, which seriously threatens human health and life.1,2
Methicillin resistant Staphylococcus aureus (MRSA) is resistant to most β-lactam antibiotics such as penicillin, cephalosporins, Carbapenem, Macrolide, and quinolones; however, it has good sensitivity to glycopeptides, oxazolidin-2-one antibiotics. Vancomycin is a representative glycopeptide antimicrobial agent and is currently the first choice for the treatment of infections caused by methicillin-resistant gram-positive cocci, such as MRSA.3,4 However, it is necessary to perform vancomycin concentration measurements in plasma due to its narrow therapeutic index and dose response varies from individual to individual. The previous study confirmed that individualized Vancomycin administration based on an individualized dosing decision-making system can effectively improve the Vancomycin trough concentration compliance rate, improve the clinical treatment efficiency, and reduce nephrotoxicity in patients.5,6 Of note, higher Vancomycin trough levels and ICU residence might be associated with a greater risk for Vancomycin-associated nephrotoxicity. 7 Chinese guidelines for therapeutic drug monitoring of Vancomycin (2020) recommended Vancomycin concentrations of 10-20 μg/mL for the treatment of common infections and 15-20 μg/mL for the severe infections. However, Vancomycin concentration can be affected by various factors, such as dosage, pathophysiology and combination of drugs. 8 The high concentration of Vancomycin usually results in higher incidence of adverse reactions, nausea, vomiting, skin rash, and renal damage. 9 Notably, the acute kidney injury is usually seen in patients with high Vancomycin concentrations. 10 Therefore, to explore the influencing factors of Vancomycin concentration in blood and construct the predicting model of Vancomycin concentration are important for Vancomycin therapeutic drug monitoring and improve the clinical therapeutic efficacy.
In this paper, we sought to explore the risk factors affecting the concentration of Vancomycin based on the retrospectively analysis of Vancomycin drug concentration monitoring in our hospital. Moreover, we also aimed to construct a model to evaluating Vancomycin concentration for patients, which will provide a reference for the formulation of individualized Vancomycin dose in patients, especially in critically ill patients.
Data and Methods
Data Source
Pass Pharm Assist (Sichuan Meikang Pharmaceutical Software R & D Co., Ltd.), data of 80 patients with Vancomycin from June 2020 to December 2022 were retrospectively selected and their clinical data were collected, including gender, age, height (cm), weight (kg), clinical diagnosis, department of examination, Vancomycin and dosage, albumin (ALB, reference value 40-55 g/L), serum total bilirubin (TBIL, reference value 4-26 μmol/L), alanine amino transferase (Alt, reference value 7-40 U/L), creatinine (CR, reference value 40-130 μmol/L), urea (BUN, reference value 2.3-7.1 mmol/L), Vancomycin valley concentration and time of Blood Collection (d). The creatinine clearance rate (Ccr, mL/min) was calculated according to the age, weight and CR of the patients. The Ccr male= (140-year-old) × weight/ (0.818 × serum creatinine), the Ccr female = 0.85 × Ccr male.
Inclusion criteria: (1) Vancomycin therapy for at least 3 days; (2) patients who agree to therapeutic drug monitoring of Vancomycin; (3) patients with clear diagnosis of infection; (4) written informed consent. Exclusion criteria: (1) pregnant or breastfeeding women; (2) unable to cooperate with drug monitoring of Vancomycin; (3) Vancomycin therapy for less than 3 days; (4) patients with undefined diagnosis of infection; (5) patients with incomplete clinical data.
Vancomycin Concentration Test
BMbio-POCT10 automatic chemiluminescence analyzer for Vancomycin concentration detection was bought from Beijing Danda Biotechnology Co., Ltd. Micro-high speed centrifuge was purchased from Hangzhou Aosen Instruments Co., Ltd. The Vancomycin blood concentration test kit, the quality control solution and the standard solution were all bought from Jiangsu Bayming Biotechnology Co., Ltd.
After Vancomycin treatment, approximately 2∼3 mL of peripheral venous blood was collected from patients with potassium EDTA anticoagulation, and 150 μL of upper serum was obtained by centrifugating at a speed of 3000 R/MIN, with a radius of 10 cm. Then, the valley concentration of Vancomycin in plasma was detected by fluorescence polarization immunoassay and a parallel quality control was set up. The detection range was 5-30 μg/mL. The effective plasma concentration range of Vancomycin was 10-20 μg/mL. 11
Research Methods
“Questionnaire on Vancomycin use and monitoring of plasma valley drug concentration in hospitalized patients” was performed. The differences of Vancomycin concentrations in different sex, age, body mass index (BMI, Kg/cm2), administration method, cumulative dose (g) Alb, Tbil, ALT, CR, Bun, CCR and time of blood Vancomycin collection were compared. In addition, patients were divided into 3 groups according to their Vancomycin trough blood pressure concentrations: normal group (10-20 μg/mL), low concentration group (<10 μg/mL) and high concentration group (>20 μg/mL). The difference of each study index in the 3 groups was analyzed.
Statistical Treatment
SPSS 25.0 statistical software package was used for statistical analysis. Measurement data are expressed as
Results
General Patient Information
A total of 80 patients were enrolled, including 49 men (61.25%) and 31 women (38.75%), with a mean age of 54.46 ± 13.48 years. There were 21 cases of peritoneal dialysis related peritonitis (26.25%), 17 cases of bloodstream infection (21.25%), 12 cases of pulmonary infection (15.00%), 12 cases of Endocarditis infection (15.00%), 5 cases of urinary system infection (6.25%), 5 cases of skin, mucosa and muscle tissue infection (6.25%), 2 cases of central nervous system infection (2.5%) and 1 case of liver abscess (1.25%). Sixty-six patients (82.5%) were treated with Vancomycin by intravenous drip and fifteen patients (18.75%) were administrated by peritoneal perfusion. The average cumulative dose of Vancomycin was 7.62 ± 8.77 g and the average time of blood sampling was 6.11 ± 3.62 d.
Plasma Vancomycin Concentration and its Influencing Factors
Distribution of Plasma Trough Concentrations in Patients With Different Vancomycin (

The Distribution of Each Evaluation Index in Different Groups of Patients (Cases, %).

Pearson Correlation Analysis and Model Construction of Plasma Vancomycin Concentration
Pearson correlation analysis showed that Ccr was negatively correlated with Vancomycin concentration (R = -0.411, P < 0.001), no significant correlation was found between other independent variables and Vancomycin plasma trough concentration. In addition, multiple linear stepwise regression was performed on Vancomycin plasma concentrations using different independent variables, the regression equation of plasma Vancomycin concentration was y (μg/mL) = 40.911 - 10.971 × method of administration - 1.715 × collection time (d) + 1.018 × cumulative dose (g) - 0.178 × Ccr (ml/Min)(R2 = 0.413 , P < 0.001). For method of administration, 1 was defined as the intravenous drip and 2 was defined as peritoneal perfusion. See Figure 1-3 for details. Concentration distribution and regression standardized residual histogram of vancomycin. Normal P-P plot of vancomycin concentration regression standardized residuals. Scatterplot of standardized residuals versus standardized predictecValues for vancomycin concentration regression model.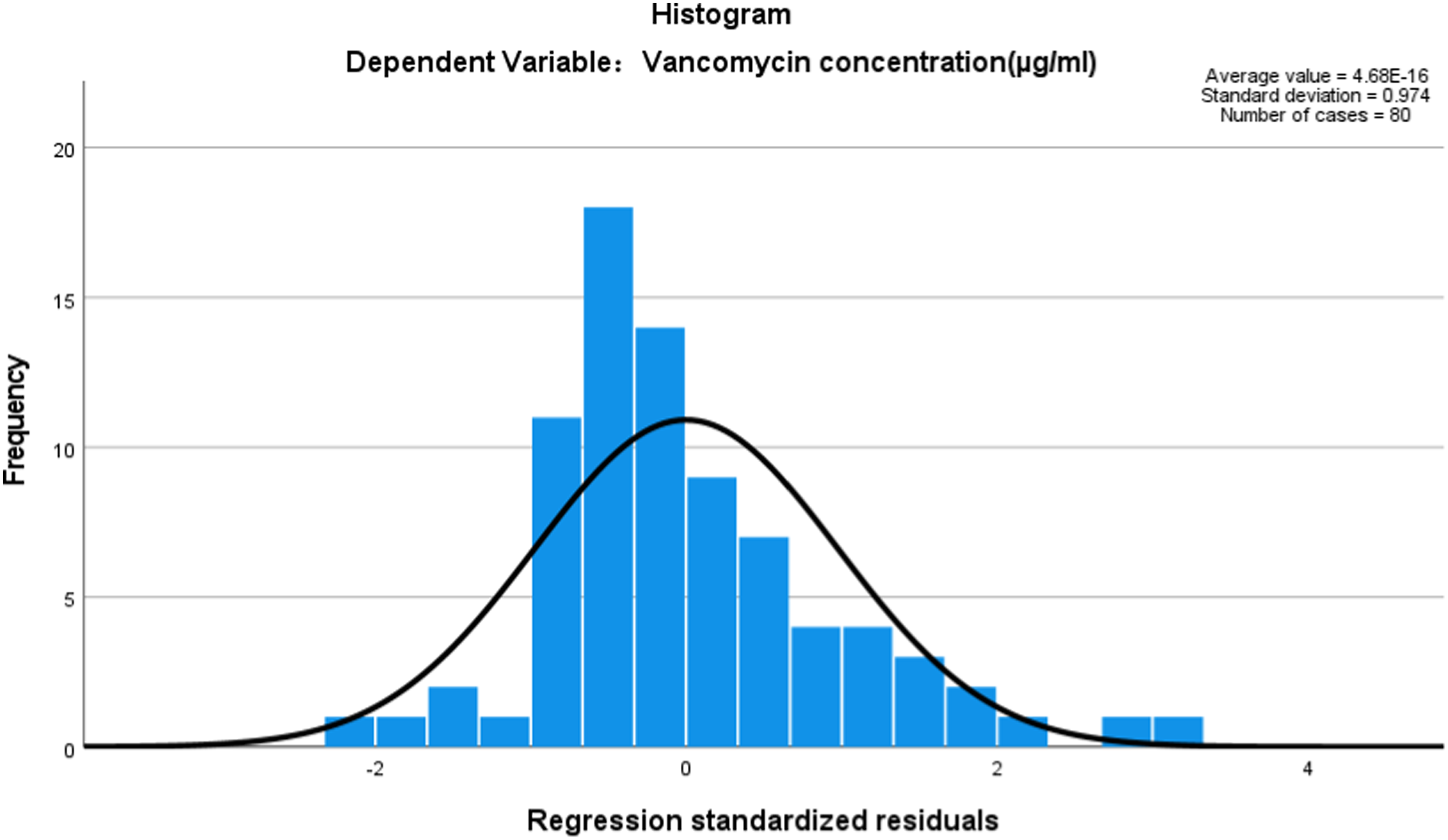


Discussion
Association of Vancomycin Trough Concentration with Efficacy and Adverse Drug Reactions
The common adverse reactions of Vancomycin are nausea, vomiting, skin rash, and renal damage. High Vancomycin trough concentration usually lead to higher incidence of adverse reactions relative to the low Vancomycin concentrations. 9 Li Yan et al 10 found that there was no significant difference in the effect of different Vancomycin concentrations, but the incidence of acute kidney injury was significantly higher in high concentration group than in the low concentration group (34.30% vs 6.40%, P = 0.001). Intriguingly, an emerging retrospective cohort study reveals a significant correlation between vancomycin concentrations of <15 mg/L at initial steady-state and poor clinical outcomes in patients with enterococcus infections, such as mortality, clinical failure and microbiological failure, when compared with concentrations of ≥15 mg/L, indicating that the target vancomycin trough concentration was ≥15 mg/L may be an optimal alternative to the use of area under the curve (AUC) values for monitoring the treatment of enterococcal infection. 12 Although the effective rate of trough concentration of blood >20 μg/mL is significantly higher than that of <10 μg/mL, the incidence of renal injury was significantly increased. 13 Therefore, we selected the effective plasma concentration range of Vancomycin ranging from 10 to 20 μg/mL.
In this study, we determined Vancomycin trough concentration in blood in 80 patients. The results showed that peritoneal dialysis-associated peritonitis was the most common type of peritonitis (21 cases, 26.25%), the second was blood stream infection (17 cases, 21.25%). 66 patients (82.5%) were administrated with Vancomycin by intravenous drip and 15 patients (18.75%) were treated by peritoneal perfusion. Peritoneal dialysis-associated peritonitis is a common serious complication of peritoneal dialysis. The international peritoneal Dialysis Association recommends that local administration of drugs in peritoneal cavity is superior to intravenous administration, but the correlation between Vancomycin levels in peritoneal dialysate and plasma levels remains unclear. Up to now, there are few studies on the concentration of Vancomycin in peritoneal dialysate in China. As a result of intraperitoneal administration, drugs need to be transported to blood through the abdominal cavity, resulting in low blood drug concentrations. Therefore, the traditional blood drug concentration detection methods may not be able to truly reflect patient’s blood drug concentration. The concentration of Vancomycin in peritoneal dialysate was determined by lc-ms-ms, which was positively correlated with the concentration of Vancomycin in plasma (r = 0.6427, P = 0.0005). 14
The average trough concentration of Vancomycin was 17.92 ± 12.03 μg/mL in 80 patients, including 28 patients in normal concentration group (35.00%), 26 patients in low concentration group (32.5%) and 26 patients in high concentration group (32.5%), which indicated that about 60.00% of patients might be at risk for poor outcomes or increased toxicity. Therefore, it is necessary to make a comprehensive clinical evaluation, adjust the dosing regimen under the guidance of blood drug concentration detection, ensure the clinical efficacy of patients and reduce the risk of drug use. Intriguingly, a previous study confirmed that a target Vancomycin AUC/ minimum inhibitory concentration (MIC) of ≥400 mgh/L could be optimal for the use for monitoring treatment of enterococcal infections, suggesting that Vancomycin dosage should be adjusted to achieve the AUC/MIC target and closely monitored for renal function. 15
Factors Affecting Vancomycin Concentration
The influence factors of Vancomycin plasma concentration were complex, and the patients’ age, body mass, serum protein, Vancomycin dose and creatinine clearance were linearly correlated with Vancomycin concentration. 16 Moreover, serum vancomycin concentration decreases progressively with increasing BMI and the augmentation in Ccr in adult patients, and the continuous monitor for patients with a BMI ≥24 kg/m2 will help to reach the target trough concentration in these patients. 17 Furthermore, there is a positive correlation between plasma albumin level and Vancomycin plasma concentration, unreasonable usage and co-existing underlying diseases are the independent risk factors for Vancomycin drug concentration. 18 A recent study evaluated the effect of different dosages of Vancomycin on plasma concentrations in elderly patients, and found that high-dose “1g, bid”Vancomycin leads to higher plasma concentrations than other dosages, concomitant with the increased incidence of nephrotoxicity. 19
In this study, we substantiated that the intravenous drip administration affected the blood trough concentration of Vancomycin. Of note, the previous study confirmed that compared to the intravenous infusion, rational use of intra-articular Vancomycin infusion might help to achieve effective therapeutic concentrations of Vancomycin in the serum and synovial fluid of patients with prosthetic joint infection. 20 Intriguingly, previous research also substantiated that the advanced age and severity of infection were independent risk factors for Vancomycin treatment failure in patients with heterogeneous vancomycin-intermediate Staphylococcus aureus (hVISA). 21 In this study, patients with high plasma Cr and low Ccr levels had higher Vancomycin trough concentration and proportion of high concentration, indicating that vancomycin trough levels of >20 mg/L may be related to a very high nephrotoxicity rate. The contents of Cr can reveal the injury of kidney. The previous study showed that Cr levels and Vancomycin concentrations were associated with the risk of renal dysfunction (hazard ratios 1.03 and 1.74, respectively). 22 Pearson correlation analysis showed that Ccr was negatively correlated with Vancomycin plasma trough concentration. Thus, the renal function of the patients should be evaluated dynamically during the course of Vancomycin treatment, especially in the elderly with impaired renal function. Moreover, for patients with renal dysfunction (Cr > 130 μmol/L), the certain approaches may be performed to achieve the situation of Vancomycin concentration reaching the standard in clinical practice, such as regulating the method of administration (e.g. peritoneal perfusion) and CCR levels.
Model-Based Individualized Vancomycin
With the development of population pharmacokinetic studies of Vancomycin, population pharmacokinetic models can help to design individualized dosing regimens for Vancomycin. A study of population pharmacokinetic parameters of Vancomycin in Chinese population combined with Bayes feedback developed an individualized drug administration decision aid system, Smart Dose, individualized dosing regimens can be developed for general adults, newborns, children, the elderly, and neurosurgical patients. 23 Notably, a recent study establishes a population pharmacokinetic (PPK) model of Vancomycin in Chinese critically ill patients, and individualized dosing of Vancomycin by model-informed Bayesian estimation to maintain an AUC24 target at 400-650 mg h/L has been successfully applied in clinic, supporting the continued use of model-informed Bayesian estimation to Vancomycin treatment in critically ill patients. 6 Emerging evidence reveals that to avoid Vancomycin-induced acute kidney injury, AUC-based monitoring approach would be superior in terms of nephrotoxicity prediction by using individualized pharmacokinetic parameters via the control of AUCτ values below the cut-off points. 24 Chen et al. constructed a Vancomycin model with a sensitivity of 92.1% and a specificity of 78.1% to predict Vancomycin plasma concentration. 25
In this study, multiple linear stepwise regression was used to determine the trough concentration of Vancomycin in blood by analyzing the patient’s age, BMI, Vancomycin administration method, cumulative dose, Alb, Tbil, Alt, Cr, Bun, Ccr, and time of blood sample collection, the regression model of y = 40.911 - 10.971 × method of administration - 1.715 × collection time (d) + 1.018 × cumulative dose (g) - 0.178 × Ccr was used to predict Vancomycin trough concentration in blood in 41.30% patients. The model can be used to predict Vancomycin plasma concentration and design individualized Vancomycin regimen. However, the clinical utility of the model needs to be validated and modified by prospective clinical studies. Intriguingly, a multicenter prospective study reveals that individualized intermittent vancomycin dosing using a model-based online calculator results in 75% and 83% of infants achieving target trough and AUC0-24, respectively, at first steady-state level. 5
Conclusion
This study explored the influencing factors of Vancomycin plasma trough concentrations and confirmed that patients’ age, method of administration, and renal function might affect the individual differences of plasma concentrations, thus affecting clinical efficacy and adverse reactions of patients. In addition, a multiple linear regression model of Vancomycin concentration in plasma was established to provide a scientific reference for individualized administration of Vancomycin. In this study, though we constructed a model to predicate vancomycin serum trough concentration. However, only 80 patients were involved in this retrospective study. Our finding just can provide some suggestions to guideline. For instance, the vancomycin serum trough concentration can be affected by the method of administration, collection time and contents of CCR. Moreover, based on our finding, we suggest to achieve vancomycin trough concentration not to exceed 20 mg/L to avoid excessive nephrotoxicity. Based on the risk factor and predicated model, the clinical doctors may design an individualized dosing regimen to improve the attainment rate of target trough concentration of Vancomycin in patients.
However, there are several limitations in this study. First, this study did not perform the sample size and efficacy analysis. Second, the influencing factors in this study are imitated due to the small sample number. Third, due to the limited sample size and influence factors, and the lack of patient assessment of clinical efficacy, the results may be biased. In addition, Ion transporter and MDR-1 polymorphism can also affect Vancomycin blood drug concentrations and clinical outcomes. Therefore, large-scale, multi-center, prospective studies should be carried out in the future to confirm our findings and help developing professional guidelines. Moreover, the regression models fitted in this study will incorporate more factors for further clinical validation, with a view to providing more clinical evidence to improve the reliability and generalization of our results. Moreover, a more detailed individualized dosing regimen of Vancomycin needs to be formulated according to relevant guidelines and our constructed model of Vancomycin trough concentration in blood, in order to provide clinical guidance for patients treated with Vancomycin worldwide in the future. Additionally, we will focus on the exploration of more reliable Vancomycin medication strategy for critically ill patients to achieve target concentration attainment and improve patients’ outcomes in our future.
Supplemental Material
Supplemental Material - The Influencing Factors of Vancomycin Trough Concentration in Blood and the Construction of Multiple Linear Regression Model
Supplemental Material for The Influencing Factors of Vancomycin Trough Concentration in Blood and the Construction of Multiple Linear Regression Model by Lin Wang, Yuhuang Wang, Chunyan Yang, Jia Jiang, Huifang Wang and Mingcai Wu in Dose-Response.
Footnotes
Author Contributions
M.W., H. W. and L. W. designed the research. Y. W., C. Y., and J. J. conducted experiments. Y. W., and J. J. analyzed the data. L. W. and M. W. wrote the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by Anhui Health Research Project (AHWJ2023BAA10016), provincial quality engineering project of higher education institutions (2022ZYRC01), Wannan Medical College teaching quality and teaching reform project (2022ZYRC103), and Three new projects of the first affiliated hospital of the WANNAN Medical College (Yijishan Hospital) (Y23062).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.