
Abstract
Objective
This study aimed to explore the relationship between climatic parameters and the daily cases of Bell’s palsy (BP) among hospital outpatients, providing ecological evidence for understanding BP etiology and prevention.
Methods
Retrospective analysis was conducted on data from 2187 BP patients who attended Kunshan First People’s Hospital Outpatient Clinic from January 1, 2020, to December 31, 2022. Meteorological data, including temperature, relative humidity, precipitation, wind speed, sunshine duration, and atmospheric pressure, were collected and combined with daily BP case records. Additionally, air quality index was used as a covariate.
Results
The number of new BP cases among outpatients showed a negative correlation with average daily temperature. A nonlinear relationship between daily average temperature and BP cases was observed through the generalized additive model (GAM). A significant negative correlation was identified between daily average temperature and BP cases, with inflection points at temperatures above 4.2°C, suggesting a potential decrease in BP risk with temperature rise beyond this threshold.
Conclusion
This study provides ecological evidence of a link between climatic factors and BP occurrence. Temperature demonstrated a significant nonlinear negative correlation with daily BP incidence, highlighting temperature and cold exposure as key targets for BP prevention in Kunshan.
Keywords
Introduction
Bell’s palsy (BP), one type of peripheral facial paralysis, sometimes called facial neuritis or idiopathic facial palsy, is caused by an unknown inflammation of the facial nerve, which is housed within the stylomastoid foramen. BP is characterized by limited mobility of the affected side in tasks including closing one’s eyes, lifting one’s eyebrow, wrinkling one’s forehead, and smiling. 1 More cases also presented with unilateral paralysis of the facial expressive muscles. Based on that more and more cases were reported BP is becoming the most prevalent peripheral nerve dysfunction worldwide.2,3 A study carried out in Italy 4 found that the cumulative incidence rate of 53.3 per 100,000 per year could impact both males and women. An incidence rate of around 42.77 per 100,000 per year was reported in another investigation on US military personnel. 5 However, the etiology and pathophysiology of BP are yet unknown, though there are several possible causes of BP, such as viral neuropathy, local vascular dysregulation, hypertension, diabetes, and autoimmune events. 6
Numerous medical professionals have noticed a clustering of BP cases, with intervals of greater and lower incidence rates. This observation has prompted research into the potential relationship between climatic factors and the onset of BP. Numerous research works have investigated the influence of meteorological factors on the incidence of face neuritis. While some studies have failed to figure out this association, others have identified a correlation between lower temperatures and a greater incidence rate of BP.7,8 Furthermore, it has been proposed that other climatic factors, such as humidity and wind speed, may also have an impact on BP occurrence, 9 however, the findings of these investigations have not yet come to a consistent conclusion. It is noteworthy that the association of climatic factors with the onset of face neuritis is not conclusive and at some time it is contradictory. Of course, these inconsistent results may be attributed to study techniques, sample selection, and geography. Consequently, more investigation from different regions or countries is required to collect more data to elucidate the correlation between the incidence of BP and meteorological factors with focus on temperature.
Even though BP is not preventable, it is more critical to comprehend the relationship between climatic conditions and the beginning of BP, thus more practical measures can be made. For example, it is easy to distribute precautions like putting on a scarf and wearing a mask.
Therefore, our study is beneficial for understanding the relationship between climatic factors and the prevalence of BP, and for providing the stronger evidence for creating efficient preventive measures against this prevalent neurological disease.
Methods
Study Population
Patients with newly diagnosed BP who visited the outpatient clinic in a sequential and non-selective manner made up the study population. The hospital’s information department retrieves the information through the Hospital Information System (HIS) using the ID number as the only criterion for individual identification. We search using the International Classification of Diseases-10 (ICD-10) codes G51.802 and G51.002. Patients who have made repeated visits must be excluded from this study as it focuses mostly on incident instances. Patients who saw the doctor more than once in a month for the same illness were combined into a single medical record using a computer program; as a result, 2568 records were included in the study. The patients who met the following criteria were admitted: (1) sudden unilateral facial paralysis; (2) beginning on the same day as presentation; and (3) no history of trauma, tumor, or any infectious disease (eg, meningitis, middle ear infection, Ramsay’s syndrome). 340 medical records were excluded as a result of the exclusion of patients who were 13 years of age or younger. Patients under the age of thirteen were excluded due to Kunshan Maternal and Child Health Hospital’s existence, which specializes in providing healthcare for this age group in Kunshan. 340 patients in all who sought care at Kunshan First People’s Hospital were therefore not included in the study since they could not be regarded as typical of this specific demographic. The final sample size consisted of 2187 individuals after patients with incomplete primary complaints that prevented the onset time from being determined were eliminated. Figure 1 displays the investigation’s flow diagram. An investigation’s flow chart.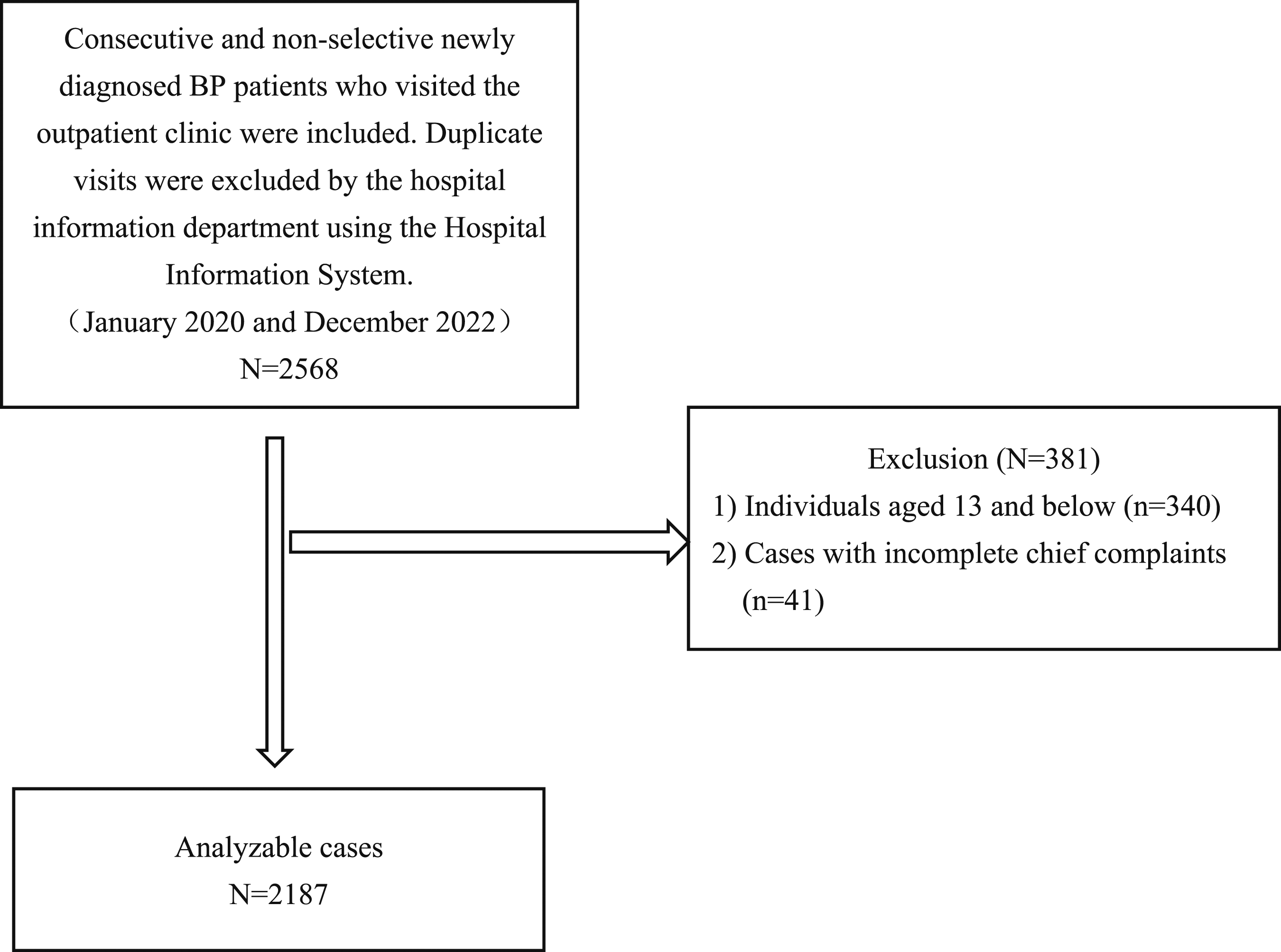
Location
The study was carried out in Kunshan City, which is a part of Suzhou City in Jiangsu Province, China, at the Kunshan First People’s Hospital. Kunshan City’s coordinates are 121°E and 31°N, placing it in the southeast of the Yangtze River Delta. Kunshan has a population of approximately 2 million and an average elevation of 3.5 meters above sea level, with the highest peak reaching 80.2 meters. It falls within the southern monsoon climate zone of the northern subtropics. The annual mean temperature is 17.6°C, with an average annual precipitation of 1200.4 millimeters and an average annual sunshine duration of 1789.2 h.
Variable
The number of new BP patients per day is the study’s outcome variable. The onset date was estimated using the date listed in the chief complaint that was noted by the first attending physician in our hospital because some patients did not seek medical attention in a timely manner or were referred to our hospital after the illness began, which caused discrepancies between the onset time and the time of visit. Every day’s total number of new cases is documented. This variable has a fluctuation range of 0 to 9 cases per day. The Kunshan Meteorological Bureau provided the meteorological parameters for the exposure variables, which include the average daily atmospheric pressure (kilopascal, kPa), temperature (degrees Celsius, °C), relative humidity (percent,%), daily precipitation (millimeters per day, mm/d), maximum wind speed (meters per second, m/s), average 2-min wind speed (meters per second, m/s), and duration of sunshine (hours, h). The environmental data, which are provided by the Kunshan Ecology and Environment Bureau in Suzhou, Jiangsu Province, include the 24-h mean SO2 concentration (μg/m3), 24-h mean NO2 concentration (μg/m3), 24-h mean CO concentration (mg/m3), an 8-h maximum O3 sliding mean concentration (μg/m3), 24-h mean PM2.5 concentration (μg/m3), and 24-h mean PM10 concentration (μg/m3). PM2.5 and PM10 refer to particulate matter in the air, distinguished by their respective diameters. PM2.5 denotes particles with a diameter less than or equal to 2.5 micrometers, capable of remaining suspended in the air for extended periods. PM2.5 particles are characterized by their small size, large surface area, high reactivity, and propensity to carry toxic substances. They can persist in the atmosphere for long distances and durations, and upon inhalation, can reach the lungs, significantly impacting pulmonary health. In contrast, PM10 refers to particles with a diameter less than or equal to 10 micrometers. While also inhalable, some PM10 particles can be expelled from the body through mucus, leading to relatively lower health risks compared to PM2.5. These environmental data are the adjustment variables.
Statistical Analysis
The mean standard deviation (normal distribution) or median (skewed distribution) were used to express continuous variables. Frequency or percentage were the 2 ways that categorical variables were expressed. Multiple linear regression models were used to evaluate the associations between daily average atmospheric pressure (kPa), average temperature (°C), average relative humidity (%), daily precipitation (mm/d), average 2-min wind speed (m/s), maximum wind speed (m/s), daily sunshine duration (h) and the daily number of new BP patients. Both non-adjusted and multivariate-adjusted models were used. A description of the 95% CI was given. Furthermore, the non-linear link was identified through the utilization of the generalized additive model (GAM). A two-piecewise linear regression model was used to determine the threshold influence of climatic parameters on the daily number of new patients with BP in terms of a smoothing plot when a nonlinear relationship was discovered.
R (https://www.R-project.org) and Empower Stats (https://www.empowerstats.com, X & Y solutions, Inc., Boston, MA, USA) tools were used for all analyses. The threshold of P < .05 (two-sided) was deemed statistically significant.
All the information was gathered from the hospital’s information department and was anonymized. This study is a retrospective analysis based on patients’ clinical data; no private patient data is needed. As a result, informed consent is waived. The study protocol has been sent for assessment to Kunshan First People’s Hospital’s Independent Medical Ethics Committee (IEC). After approval, it was assigned the number 2023-03-067-K01.
Results
The Results Obtained From Univariate and Multivariable Regression Model.

Adjustment I model adjusted for: PM10 24 h mean concentration/(μg/m3); PM10 24 h mean subindex; PM2.5 24 h mean concentration/(μg/m3); PM2.5 24 h mean subindex.
Adjustment II model adjusted for: NO2 24 h mean concentration/(μg/m3); NO2 24 h mean subindex; PM10 24 h mean concentration/(μg/m3); PM10 24 h mean subindex; O3 maximum 8-h sliding mean concentration/(μg/m3); O3 maximum 8-h sliding mean subindex; PM2.5 24 h mean concentration/(μg/m3); PM2.5 24 h mean subindex; AQI (Air Quality Index); SO2 24 h mean concentration/(μg/m3); SO2 24 h mean subindex; CO 24 h mean concentration/(mg/m3); CO 24 h mean subindex.
The daily average atmospheric pressure and the daily count of new patients with BP had a positive link in the unadjusted model (β = .021, 95% confidence interval (CI) (.011, .031), P < .001). There is a daily increase of .021 new patients with BP for every 1 kPa increase in the daily average atmospheric pressure. This implies that a rise in atmospheric pressure could be linked to a rise in the incidence of facial paralysis.
The frequency of new cases of facial paralysis per day and the average daily temperature have a negative connection (β = −.026, 95% CI (−.036, −.015), P < .001). The number of new cases of facial paralysis each day decreases by .026 for every degree Celsius as the daily average temperature rises. This suggests that a drop in the frequency of occurrences of facial paralysis may be linked to an increase in temperature.
Other climatic characteristics, such as the daily average relative humidity, the daily scheduled precipitation, the daily maximum wind speed, the daily average 2-min mean wind speed, and the daily duration of sunshine, do not significantly correlate with the number of new patients with BP per day (P > .05).
The following conclusions can be drawn after accounting for various model parameters:
The daily average atmospheric pressure and the number of new patients with facial paralysis continue to have a positive connection in model I, which takes into account the concentrations and indices of PM2.5 and PM10 (β = .022, 95% CI (.011, −.032), P < .001). In model I, the daily average temperature and the daily count of new patients with BP continue to have a negative connection (β = −.027, 95% CI (−.038, −.016), P < .001).
Model II, which incorporates further environmental monitoring variables such NO2, O3, PM2.5, PM10, SO2, CO, and Air Quality Index (AQI), shows a weaker association between the daily mean air pressure and the number of new occurrences of BP (β = .012, P = .070). The number of new instances of BP per day and the average daily temperature continue to be negatively correlated. This suggests that there is a steady relationship between the daily average temperature and the daily number of new cases of BP is stable.
Threshold Effect Study Analyzing the Correlation Between the Number of New Patients With BP Each Day and the Average Daily Temperature.

Abbreviations: OR, odds ratio; CI, confidence interval; LRT, logarithmic likelihood ratio test.
The inflection points were found to be 4.2°C, according to the research. There was no discernible relationship between the daily average temperature and the number of new instances of BP on the left side of the inflection points. On the right side of the inflection points, the number of new patients with BP per day decreased by .026 people for every 1°C increase in the daily mean temperature (β = −.026, 95% CI (−.042, −.009), P = .003).
aAdjusted variables: NO2 24 h mean concentration (μg/m3); NO2 24 h mean sub-index; PM10 24 h mean concentration (μg/m3); PM10 24 h mean sub-index; O3 maximum 8-h rolling mean concentration (μg/m3); O3 maximum 8-h rolling mean sub-index; PM2.5 24h mean concentration (μg/m3); PM2.5 24 h mean sub-index; AQI; SO2 24 h mean concentration (μg/m3); SO2 24 h mean sub-index; CO 24 h mean concentration (mg/m3); CO 24 h mean sub-index.
bLinear analysis, P-value <.05 indicates a linear relationship.
cNon-linear analysis.
dP-value <.05 means Model II is significantly different from model I, which indicates a non-linear relationship.
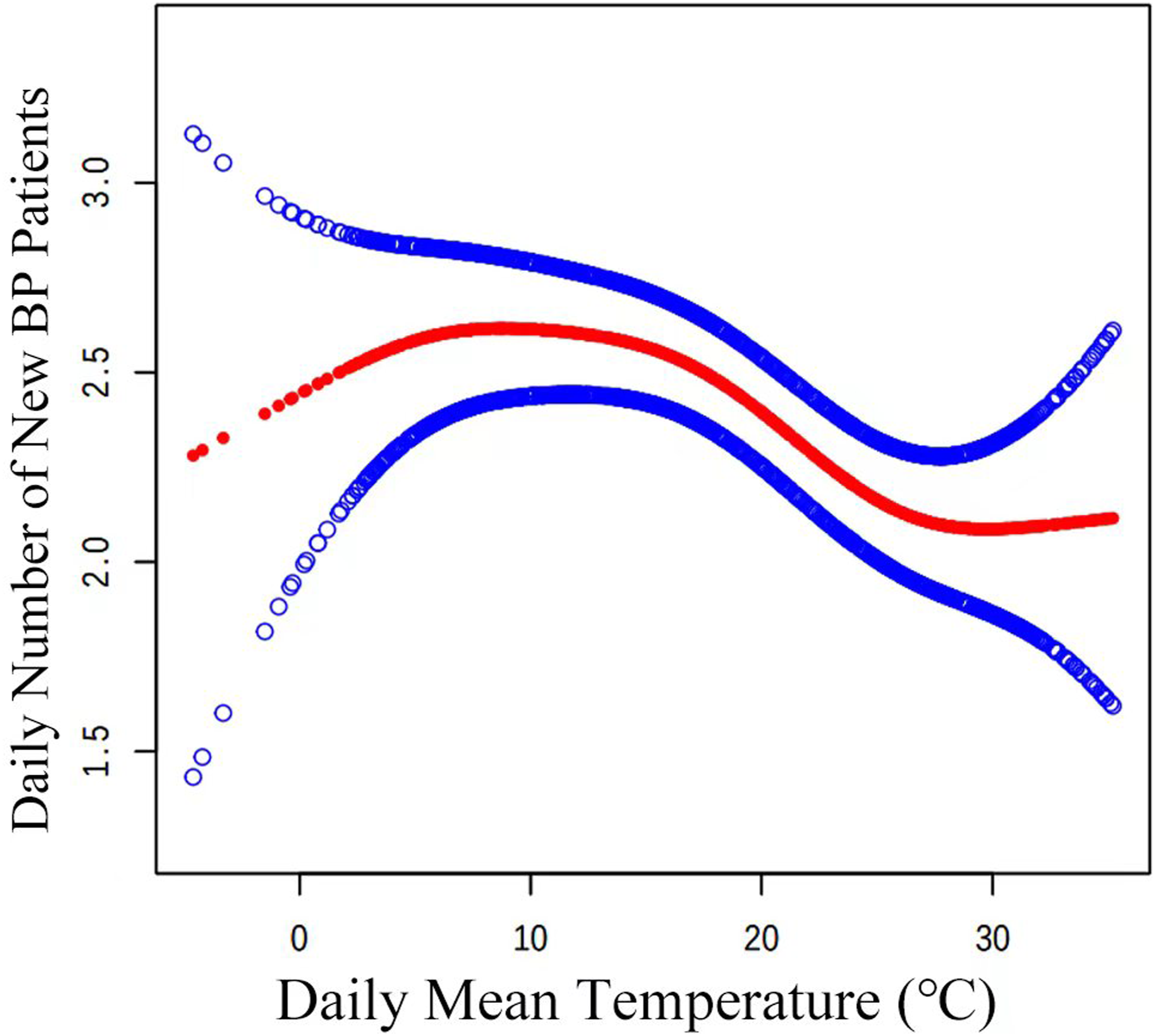
Non-linear correlation between the daily number of new patients with BP and mean temperature.
Discussion
To determine how meteorological elements affected the number of new instances of BP reported every day, the current study retrospectively analyzed 3 years’ worth of data. The average daily temperature and the number of new instances of BP each day were found to be negatively correlated. This negative correlation held true even after correcting for NO2, O3, PM2.5, PM10, SO2, CO, and AQI. A non-linear correlation was also seen between the daily average temperature and the number of new instances of BP. A daily average temperature increase of 1°C was linked to a daily decrease of .026 new instances of BP on the right side of the 4.2°C inflection point (β = −.026, 95% CI (−.042, −.009), P = .003).
The curve indicates that there is no significant correlation between the number of BP cases and a daily average temperature below 4.2°C. In Kunshan, Jiangsu, the only months with an average temperature below 4.2°C are December and January (Supplemental Table 2). People wear masks and scarves, among other anti-cold measures, during the coldest months of the year. This may help to explain why there is no rise in the number of patients with BP when the temperature is lowered. People often ignore preventive measures when the temperature hovers around 4.2°C, which may indicate the arrival of colder or warmer weather and temperature instability. This increases the risk of facial paralysis.
Hsieh et al studied 775 BP patients in Taiwanese hospitals, finding a seasonal BP prevalence peak in males during colder months, similar to our study. Patients under 50 had higher prevalence, with no significant seasonal correlation to nerve involvement extent. 10 In a retrospective investigation of 568 individuals with BP, Kokotis et al discovered a negative association between the number of medical records each month, the mean monthly temperature, and the summer. 11 Kim et al examined information from more than 70,000 people in the Korean National Health Insurance Claims Database (NHICD) between 2010 and 2018. The seasonal and monthly incidence rates of BP were linked to lowering temperature (P = .002), increasing air pressure (P = .034), and decreasing relative humidity (P < .001), according to their multivariate linear regression analysis. 12 199 patients with BP treated at the Kumluca and Serik State Hospitals in Antalya, Turkey, between January 2017 and December 2020 were the subject of a retrospective analysis by Murat Kar et al. They discovered that the incidence of facial paralysis varied with the seasons, peaking from December to February. 13 Using multivariate logistic regression analysis, Eszter Varga et al examined the data of 613 facial paralysis patients treated at a Hungarian hospital between January 1, 2015, and December 31, 2021, to investigate the parameters linked to BP recurrence. BP episodes were more common in the winter and spring than in the summer and fall, and their frequency increased with the arrival of colder seasons. 14 In a retrospective analysis, Chen and colleagues examined data from 5387 patients in Hangzhou, Zhejiang Province, China, between May 1, 2018, and June 30, 2023. They discovered that varying months and seasons were linked to various BP incidences. It was discovered that the beginning of BP was connected with temperature and air pressure. 15 The weather conditions of the season or month was the exposure variable in the investigations; the trend is also seen in Supplemental Figure 1. However, the actual daily weather varies with respect to temperature, humidity, wind direction, and length of sunshine. Furthermore, as facial paralysis is an acute-onset disorder, more accurate results can be obtained by controlling for daily weather conditions as an exposure variable. Peter Franzke et al examined the impact of relative humidity, air pressure, and ambient temperature on the occurrence of facial paralysis in 825 patients between 2006 and 2016. They discovered that a 24-h increase in atmospheric pressure above 6 kPa increased the probability of facial paralysis by 35% overall. Rapid variations in ambient temperature were associated with a more than 2-fold increase in the incidence of facial paralysis in diabetes patients. 16 According to the current investigation, there is a positive association (β = .021, 95% CI (.011, .031), P < .001) between the daily mean station atmospheric pressure and the number of new cases of facial paralysis that occur each day. This association remained true even after accounting for PM2.5 and PM10 concentrations. Ender Salbas et al used Google Trends to query data from 19 countries covering both the northern and southern hemispheres from January 2004 to October 2020. They found that facial paralysis exhibits seasonal variations, with higher incidence rates in the northern hemisphere during the winter-spring transition and in the southern hemisphere during winter. This further supports the correlation between the daily new cases of BP and the daily average temperature. 17
Thus, from 2002 to 2013, data from 15,740 control participants and 3935 patients with BP in Korea were evaluated by So Young Kim et al. Temperature, humidity, atmospheric pressure, and air pollutants like SO2, NO2, O3, CO, and PM10 were among the meteorological data they examined. They discovered no conclusive link between weather factors and the beginning of BP. They did discover, nonetheless, that the BP group had a greater NO2 ratio within 60 days. 18 A retrospective examination of 863 patients with excessive BP who were admitted to 7 hospitals in Shenzhen’s Futian area during an 11-year period was carried out by Cuiyi Zhang et al. They investigated a number of meteorological factors, including barometric pressure, temperature, humidity, and wind speed. They discovered that although average air pressure, visibility, total cloud cover, and particularly sunshine duration and solar radiation, were perhaps connected to the severity of clinical BP symptoms, wind speed was linked to the development of severe BP. 19 The study, which concentrated on inpatient initial visits, indicated a positive link between the frequency of daily BP cases and daily mean station atmospheric pressure, but not with temperature. This is an essential point to note. Given that the study population was hospitalized and that BP diagnosis and treatment are normally provided in an outpatient setting in the hospital where our study was conducted, it is likely that the variations in research outcomes are the result of the different study populations.
Environmental factors were selected as adjustment variables in this study for 2 reasons. Firstly, it cannot be adjusted because of the interactions between temperature, sunlight, humidity, and wind speed, among other meteorological parameters. Second, research indicates that air pollution, including PM10 and PM2.5, is associated with various diseases such as cardiovascular diseases 20 and depression, 21 possibly due to its potential to alter immune responses 22 and induce inflammation. 23 BP is seen as an inflammatory response as well. So, the initial adjustment variables were chosen to be PM10 and PM2.5, and the second set of adjustment variables to be PM10, PM2.5, NO2, SO2, CO, O3, etc. The findings showed that there was still a correlation between the daily mean temperature and the daily cases of BP even after the 2 modifications.
Limitations
Limitations of this study include several factors that restrict the generalizability of the findings. Firstly, the inclusion criteria excluded cases of facial nerve damage caused by trauma, tumors, or infectious factors, primarily due to their sporadic nature and limited correlation with weather variables. Consequently, the results of this study cannot be extrapolated to patients affected by these conditions. Secondly, patients aged 13 and below were excluded from the study due to specialized healthcare services for this age group at Kunshan Maternal and Child Health Hospital.
Additionally, the study focused on the daily new cases of BP and its relationship with meteorological and environmental factors, with daily fluctuations in new cases ranging between 0 and 9. Stratifying by demographic characteristics such as age, gender, pregnancy status, or diabetes would result in substantial differences in sample sizes across strata, potentially affecting the accuracy of conclusions drawn. Therefore, demographic stratification was not performed in this study.
Furthermore, it should be noted that patients included in the study may have traveled from other regions to seek treatment in Kunshan, although this proportion was likely minimal. Given the proximity of Kunshan to major cities such as Suzhou (30 kilometers away) and Shanghai (50 kilometers away), individuals seeking medical care may typically choose these larger cities. Moreover, Bell’s palsy is a common and well-diagnosed condition, reducing the likelihood of patients traveling outside the region for treatment.
Conclusion
In summary, research conducted in the Kunshan region has shown that extreme caution is necessary to avoid facial paralysis, especially when the temperature is close to 4.2°C. A possible pathogenic process involves a rise in plasma endothelin secretion brought on by low temperatures.24,25 This, in turn, promotes vascular smooth muscle cell contraction, vascular spasms, and thrombosis, 26 which ultimately lead to facial paralysis and ischemia of the nerves. To verify these results, more experimental study is needed.
Supplemental Material
Supplemental Material - Non-Linear Association Between Climatic Parameters and Bell’s Palsy Prevalence of Hospital Outpatients: An Ecological Proof in Kunshan, Suzhou, China
Supplemental Material for Non-Linear Association Between Climatic Parameters and Bell’s Palsy Prevalence of Hospital Outpatients: An Ecological Proof in Kunshan, Suzhou, China by Lu-Yuan Zhang, Ming-Zhu Jiang, Dong-Mei Li, Ya-Qin Gong, Yun-Yu Xia, Xiao-Chun Wang, Chen Lin, Shan-Jun Yan, Lu Rong-Zhu and Chong Li in Journal of Dose-Response.
Supplemental Material
Supplemental Material - Non-Linear Association Between Climatic Parameters and Bell’s Palsy Prevalence of Hospital Outpatients: An Ecological Proof in Kunshan, Suzhou, China
Supplemental Material for Non-Linear Association Between Climatic Parameters and Bell’s Palsy Prevalence of Hospital Outpatients: An Ecological Proof in Kunshan, Suzhou, China by Lu-Yuan Zhang, Ming-Zhu Jiang, Dong-Mei Li, Ya-Qin Gong, Yun-Yu Xia, Xiao-Chun Wang, Chen Lin, Shan-Jun Yan, Lu Rong-Zhu and Chong Li in Journal of Dose-Response.
Supplemental Material
Supplemental Material - Non-Linear Association Between Climatic Parameters and Bell’s Palsy Prevalence of Hospital Outpatients: An Ecological Proof in Kunshan, Suzhou, China
Supplemental Material for Non-Linear Association Between Climatic Parameters and Bell’s Palsy Prevalence of Hospital Outpatients: An Ecological Proof in Kunshan, Suzhou, China by Lu-Yuan Zhang, Ming-Zhu Jiang, Dong-Mei Li, Ya-Qin Gong, Yun-Yu Xia, Xiao-Chun Wang, Chen Lin, Shan-Jun Yan, Lu Rong-Zhu and Chong Li in Journal of Dose-Response.
Footnotes
Acknowledgments
We thank the Kunshan First People’s Hospital, the Meteorological Bureau, and the Ecology and Environment Bureau of Kunshan City, Suzhou, Jiangsu 215300, China for providing data support.
Author Contributions
All authors contributed to the study’s conception and design. Data collection and cleaning: LY. Z., MZ. J., DM. L., YY. X., XC. W., C.L., SJ. Y. Real data analysis and interpretation: LY. Z., MZ. J., YY. X. ,C. L. Drafting of the manuscript: LY. Z. LY. Z. is first authors. C.L.is the corresponding authors. RZ. L. and C. L. jointly directed this work. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported all by Special Funding for Jiangsu Province Science and Technology Plan (Key Research and Development Program for Social Development) (CN) (BE2023738), Suzhou Collaborative Innovation Research Project of Medical and Industrial Integration (CN) (SLJ2022023).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.