
Abstract
Background and purpose
Perfusion Computed Tomography (CTp) is an imaging technique which allows quantitative and qualitative evaluation of tissue perfusion through dynamic CT acquisitions. Since CTp is still considered a research tool in the field of abdominal imaging, the aim of this work is to provide a systematic summary of the current literature on CTp in the abdominal region to clarify the role of this technique for abdominal cancer applications.
Materials and Methods
A systematic literature search of PubMed, Web of Science, and Scopus was performed to identify original articles involving the use of CTp for clinical applications in abdominal cancer since 2011. Studies were included if they reported original data on CTp and investigated the clinical applications of CTp in abdominal cancer.
Results
Fifty-seven studies were finally included in the study. Most of the included articles (33/57) dealt with CTp at the level of the liver, while a low number of studies investigated CTp for oncologic diseases involving UGI tract (8/57), pancreas (8/57), kidneys (3/57), and colon–rectum (5/57).
Conclusions
Our study revealed that CTp could be a valuable functional imaging tool in the field of abdominal oncology, particularly as a biomarker for monitoring the response to anti-tumoral treatment.
Introduction
Perfusion Computed Tomography (CTp) is a minimally invasive technique which allows quantitative and qualitative evaluation of tissue perfusion by injecting an iodinated contrast agent and performing dynamic CT acquisitions to estimate time enhancement curves within organs and tissues.1-3 Physiological parameters, such as flow rate or local blood volume, can subsequently be calculated from the time enhancement curves by means of mathematical perfusion models. From a technical standpoint, CTp is the result of the development of new multi-slice CT systems and post-processing software and consists in a rapid serial images acquisition after bolus injection of a high flow (4–10 mL/s) iodinated contrast with a low contrast media volume (generally 40 to 50 mL). 4 The contrast injection with a high iodine concentration allows to increase the enhancement of the examined tissues. Then, by means of post-processing software, it is possible to obtain attenuation curves based on kinetic models and perfusion algorithms which vary depending on the organ investigated. Time attenuation curves are then analyzed to quantify color maps that represent the functional state of the vascular system such as blood flow (BF), blood volume (BV), and contrast transit measurements such as mean transit time (MTT) and time to peak (TTP). Among the innovations that lead to the CTp development, there are the increase in the number of detectors, which allows to investigate larger body areas and reduce the thickness of the individual slices, improving the spatial resolution of the CT and consequently the image quality and information obtained. Moreover, the increase in the rotation frequency of the X-ray tube-detector complex improved the temporal resolution of the CT and reduced the duration of the scan, thus allowing to perform the breath examination suspended and reduce breath artifacts thanks also to the introduction of new filters for the noise attenuation and the use of special software for correction of patient movements. Finally, with the development of new image processing software, it is possible to calculate perfusion parameters with the creation of color maps relating to each pixel of tissue analyzed. 5 Based on these technical evolutions, CTp has been well established in the study of brain perfusion and has turned out to be the modality of choice for applications in this field. 6 In particular, CTp is largely used to assess acute stroke,7,8 as well as to explore the tissue viability highlighting the changes in the mechanisms of self-regulation following an acute ischemia. 9 In the field of oncology, there has been an increasing interest in the use of CTp, with a wide range of clinical applications, including lesion detection and characterization, identification of metastases, prediction of prognostic information based on tumor vascularity, and prediction and assessment of response to chemoradiation treatments and antiangiogenetic drugs. 2
In the field of abdominal imaging, CTp is still considered a research tool. 10 This is mainly because it requires the acquisition of multiple samples of the same anatomical region with relatively high temporal resolution, and this is generally associated with relatively high radiation exposure. Furthermore, results of CTp studies depend on the choice of acquisition parameters, mathematical perfusion model, software implementation, and the anatomical region. 11 However, the increasing availability and simplicity of CTp, together with its ability in quantification of the abnormal vasculature within tumors (thus allowing the assessment of tumor aggressiveness) led to a growing interest in CTp imaging method to examine several oncologic diseases associated with abdominal organs.4,10 In particular, the ability of CTp to study microvascular changes in angiogenesis reflecting tumor perfusion in vivo could be of particular interest for investigating liver and pancreatic lesions.12-15 In the management of hepatocarcinoma (HCC), CTp is considered a safe and specific imaging tool for diagnosis, choosing a therapeutic procedure, and evaluating response to therapy by showing changes in various perfusion parameters such as BV and TTP. 16 Moreover, in case of liver metastases, CTp allows the visualization of occult lesions in comparison to other imaging methods, thanks to the hemodynamic changes highlighted by an increase in the enhancement of the liver parenchyma during CT acquisition 17 and resulted useful for survival prediction and response to treatment. 18 CTp was also able to assess changes in liver cancer perfusion in response to a specific anticancer therapy. 19 CTp can help in the evaluation of malignant pancreatic tumors. 20 In fact, it was observed that extrapolated values from CTp, such as BF and BV, provided optimal sensitivity and specificity to differentiate pancreatic adenocarcinoma from mass-forming chronic pancreatitis.21,22 Other studies have shown promising results concerning the role of CTp for colorectal cancer applications, such as diagnosis, angiogenesis evaluation, and pre-operative pathological grading.23-26 The role of CTp was also investigated for diagnosis of kidney carcinoma. 27
Based on these results, and thanks to the development of advanced equipment and the availability of commercial software platforms, CTp may provide a solid basis for obtaining additional functional imaging information, as an integral part of a conventional CT exam that could change the diagnostic and therapeutic process of patients with tumors involving abdominal district tumors. 6 However, the still present drawbacks, mainly related with the lacking consensus on which CT protocol to use and the fact that published literature is based on small studies with different perfusion algorithms, have resulted in the missing integration of CTp into routine clinical practice protocols for abdominal imaging. 28 In this context, we performed a systematic literature review on the application of CTp in abdominal cancer to provide a systematic overview of the application of CTp in abdominal cancer and clarify the role of this technique for abdominal imaging in clinical practice.
Materials and Methods
Search Strategy and Selection Criteria
A systematic literature research was performed to identify all original articles investigating the role of CTp for oncological applications in the abdominal district. The most relevant scientific electronic databases (PubMed, Web of Science, and Scopus) were explored and used to build the literature search. Studies published from 2011 to April 2021 were selected. The search strategy included keywords listed in Supplementary Materials-S1 section. The literature search was limited to English language publications and studies on human subjects. Two reviewers, after having independently screened identified titles and abstracts, assessed the full text of articles that evaluated the use of CTp in the abdominal district and that were original articles (not review articles, case studies). For articles meeting these criteria with full text available, the following further selection criteria had to be fulfilled: involvement of adult patients (age > 18); missing information on the CTp parameters investigated.
Data Extraction and Study Planning
After selection procedure, the following data were extrapolated from selected articles and collected in a table: author names; publication year; study type (retrospective and/or prospective); clinical purpose (diagnosis, grading, prognosis, response to treatment); sample number; info on study group analyzed in the study; anatomic district of interest; perfusion acquisition details; information on placement of regions of interest (ROIs), namely the segmentation method (manual, semi-automatic, automatic) and the ROI type (2D or 3D); main results; and conclusions. The articles were classified and analyzed according to the abdominal area investigated in the study.
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 29 (See Supplementary Materials-S2 section-for PRISMA Checklist).
Quality Assessment
The quality of the included studies was assessed through the QUADAS-2 tool for diagnostic studies and the QUIPS tool for prognostic studies. Two reviewers independently assessed the quality of each study, and any disagreements were resolved by consensus. For the QUADAS-2 tool, four domains were evaluated: (1) patient selection, (2) index test, (3) reference standard, and (4) flow and timing. At each domain, the quality of the elements was classified as “low,” “high,” or “unclear.” 30 For QUIPS, six domains were evaluated: (1) study participant selection, (2) study dropout, (3) prognostic factor measurement, (4) outcome measurement, (5) study confusion, and (6) statistical analysis and reporting. The bias risk assessment was obtained using the answers “yes,” “partial,” “no,” or “don't know” for 3 to 7 elements within each domain and were combined to assign an overall rating for each domain as “high,” “moderate,” or “low” risk of bias.31,32
Results
Study Selection
A total of 544 articles were retrieved from the PubMed, Web of Science, and Scopus databases. Following the removal of 72 duplicate articles, was performed a screening based on titles and abstracts of the remaining 472 articles. 364 records in this step were excluded for the following reasons: 100 were case reports and 264 were off-topic/review articles. The screening by titles and abstracts produced 108 articles, potentially usable for the systematic review description, of which the full text was evaluated. Of these articles, 17 records were excluded because they were not in English and 34 articles were off-topic and/or review articles. Among articles that were out of topic, 4 studies were excluded because they had a methodological purpose, while 3 were excluded because they aimed at investigated repeatability and reproducibility of CTp parameters. Finally, 57 records were included for the qualitative synthesis. The PRISMA flowchart of studies included according to the inclusion and exclusion criteria was reported in Figure 1. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Characteristics of Included Studies
Characteristics of Included Studies. R = retrospective; P = prospective; FOV = field of view; M = manual; S = semi-automatic; A = automatic; mVI = microvascular invasion; MVD = microvessel density; HCC = Hepatocellular carcinoma; PDAC = pancreatic ductal adenocarcinoma; mNET = neuroendocrine tumors; PanNETs = pancreatic neuroendocrine tumors; AP = acute pancreatitis; CP = chronic pancreatitis; AML = angiomyolipoma; NASH = Non-Alcoholic SteatoHepatitis; CRC = colorectal cancer; pRCC = papillary renal cell carcinoma; ccRCC = clear cell RCC; CRLM = colorectal cancer liver metastases; CCRT = concurrent chemoradiotherapy; GEJ = gastroesophageal junction; GIST = Gastrointestinal stromal tumor; AGC = Advanced Gastric Cancer; LAGC = locally advanced gastric cancer; RFA = radiofrequency ablation; IL-8 = interleukin 8; FU1 = after TACE; FU2 = follow-up; TACE = transarterial chemoembolization; TARE = transarterial radioembolization; TACLI = transarterial chemo-lipiodol infusion; CR = complete response; PR = partial response; SD = stable disease; PD = progressive disease; SBRT = Stereotactic body radiotherapy; TZ = transition zone; CZ = central zone; PZ = surrounding parenchymal zone; DEB‐TACE = doxorubicin‐eluted bead-TACE; AUC = area under the curve; MFCP = mass-forming chronic pancreatitis.

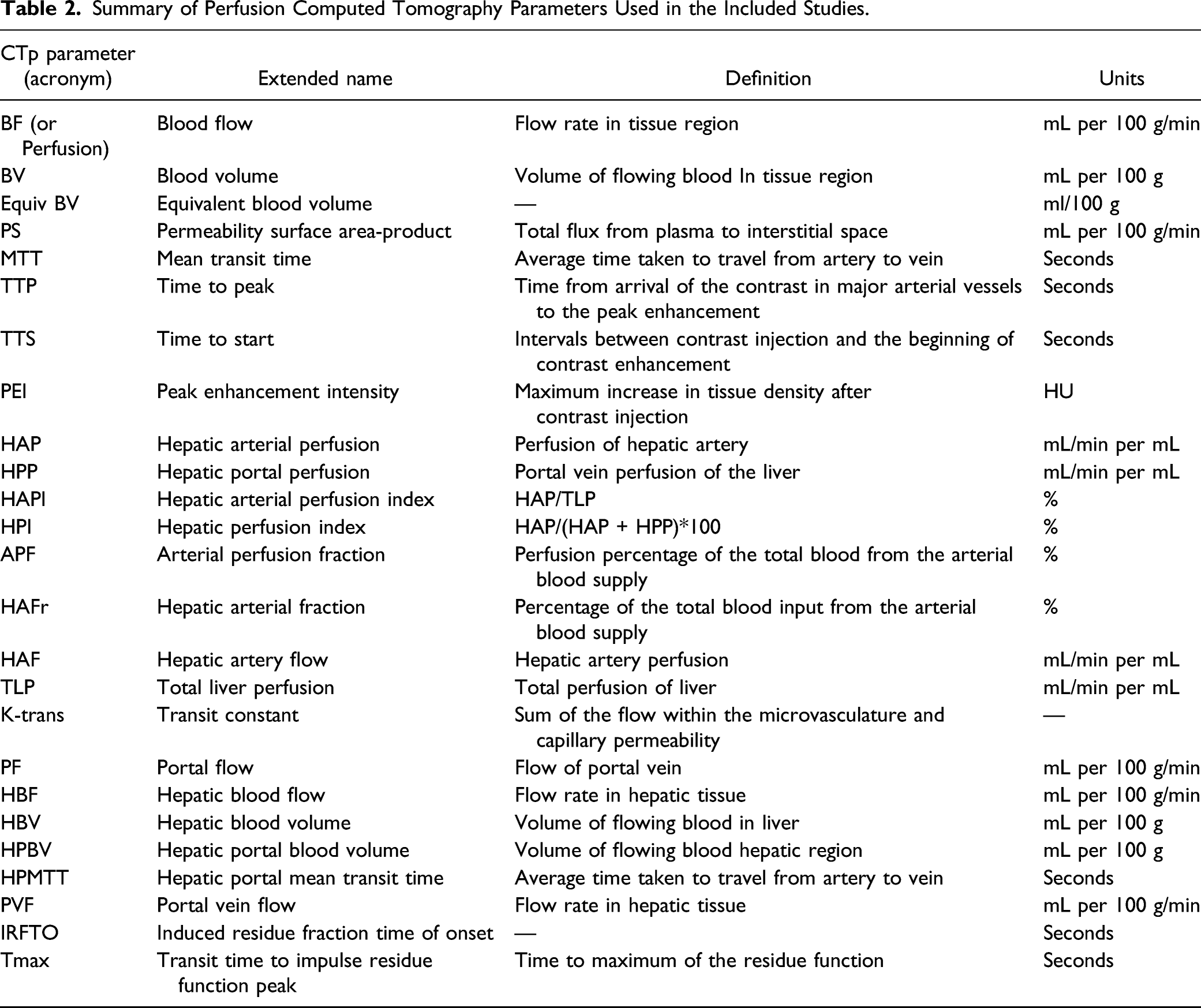
Summary of Perfusion Computed Tomography Parameters Used in the Included Studies.

Graphic summary of the systematic review results according to the abdominal zone and clinical purposes investigated in the selected studies. The donut chart shows the number of included studies according to the abdominal zone investigated (liver in orange; upper gastrointestinal tract in yellow; pancreas in green; kidneys in blue; colon/rectum in red). Number and percentage of studies included in each of the five groups were reported investigates. For each group, the bar plots show the number of studies according to the clinical purpose investigated. Abbreviations: UGI = Upper Gastrointestinal.
Perfusion Computed Tomography (CTp) Parameters Investigated in the Included Studies, According to the Specific Abdominal Area and the Clinical Purpose. Refer to Table 2 for the Extended Name and Meaning of CTp Parameters. Abbreviations: UGI = Upper Gastrointestinal.

Computed Tomography in Liver Cancer
Among studies on liver tumors, fourteen aimed at evaluating the role of CTp for prediction and assessment of response to treatment. Ippolito et al 40 found that CTp was able to assess HCC vascularity after radiofrequency ablation treatment by means of perfusion, HAO, and HPI features. Similar results were found by Marque et al, even if their study also involved patients with liver metastases other than HCC. Promising results were found by Yang et al 45 for patients with HCC treated with chemoembolization. Wang et al 54 found that all CTp parameters investigated in their study were significantly decreasing in HCC after argon–helium knife therapy. Four studies found that CTp parameters were able to assess response to TACE treatment in HCC patients.55,57,69,72 Results from 3 studies68,76,80 revealed that CTp could help to evaluate the therapeutic response in HCC patients treated with sorafenib. D’Onofrio et al 67 and Ng et al 79 evaluated the role of CTp in patients with liver metastases arising from pancreatic neuroendocrine tumors and found that CTp was able to predict response to everolimus and bevacizumab therapy. Similar results were found by Detsky et al 75 for patients with liver metastases treated with both bevacizumab and stereotactic body radiotherapy. Three studies on liver tumors had diagnostic clinical purpose. Bai et al 47 found that CTp parameters (BF, HAFr, HAP, and HPP) were able to detect HCC lesion from healthy liver. Similar results were found by Bayraktutan et al. 48 However, their study did not involve control patients, but they used as reference only the surrounding liver parenchyma of HCC patients. Singh et al 53 found that CTp was a helpful tool in differentiating hemangiomas from HCC and liver metastases. Three studies investigated CTp for prognostic purposes. Kaufmann 56 found that CTp was able to quantify the degree of HCC arterialization. Wu et al 62 findings were in line with those from Kaufmann et al 56 since they found that values associated with PVF parameter were able to predict microvascular invasion in patients with HCC. Chen et al 46 found that arterial BF of HCC lesions was correlated with circulating angiogenetic factors. The remaining thirteen studies had multiple purposes. Specifically, ten investigated CTp for both prognosis and response to treatment assessment of liver cancer and 3 were on diagnosis and response to treatment. Among studies on prognosis and response to treatment, seven were on HCC. Petralia et al 36 found that BF and BV could predict response to thalidomide treatment and progressive disease. Jiang et al 41 found that, in HCC patients treated with bevacizumab, CTp parameters were able to monitor treatment effect as well as predict progression-free survival. By means of a histogram analysis of HAP, the work by Reiner et al 59 revealed that CTp was able to predict response to TARE in HCC. Similar results were also found by Su et al in HCC patients treated with TACE. Results by Popovic et al 71 revealed that CTp could predict survival in patients with intermediate stage HCC treated with DEB-TACE. However, this technique was not able to assess response to treatment. Nakamura et al 78 found that CTp was able to predict overall survival in HCC patients treated with sorafenib. Three studies assessed the role of CTp to predict response to treatment and prognosis in patients with liver metastases,18,52,58 of which one involved patients with both liver metastases and HCC. 52 Finally, the remaining 3 studies found that several CTp parameters had both diagnostic power and were able to predict response to treatment.16,42,50 Any study on grading of liver cancer was found.
Computed Tomography in UGI Cancer
Considering the 8 articles highlighting the role of CTp in UGI tract, three investigated the power of CTp parameters for grade assessment of gastric cancer and both 3 found that BF, BV, and PS were able to differentiate poor-, moderately-, and well-differentiated gastric cancer.60,61,66 Three studies aimed at assessing the role of CTp for response to treatment in patient with UGI cancer, of which two involved patients with gastric cancer49,83 and the other one included patients with metastatic gastrointestinal stromal tumors (GIST). 37 Both found that CTp parameters were able to assess clinical response to different treatment regimens. Yao et al 38 aimed at evaluating prognosis in patients with gastric adenocarcinoma, focusing on the possible association between CTp and tumor angiogenesis. They found that BV could reflect the angiogenesis due to its significant correlation with microvessel density. The remaining study aimed at assessing both response to treatment and prognosis in patients with gastric cancer by means of CTp parameters. 77 They found that CTp was able to predict response to concurrent chemoradiotherapy and survival by means of BF, BV, and PF.
Computed Tomography in Pancreatic Cancer
Among studies on CTp role in pancreatic cancer, six had diagnostic purpose and the remaining two aimed at assessing prognosis 51 and response to treatment 82 of pancreatic cancer patients. Among diagnostic studies, two were performed by Delrue et al33,34 who investigated the utility of 3 CTp parameters (BV, BF, and PS) for differential diagnosis of patients with pancreatic cancer. Specifically, they observed an overall decreasing of BF and BV perfusion values in tumoral tissues with respect to control populations. Similar results were found by Lu et al 35 who included also TTP and PEI among CTp parameters under investigation, finding promising results also for these features. The power of CTp for differential diagnosis of pancreatic cancer was also highlighted in a recent study performed by Zaboriene et al 22 who, in a study involving patients with pancreatic ductal adenocarcinoma (PDAC), found that BF and BV were independent predictors of PDAC. Aslan et al 73 showed that CTp was able to diagnose PDAC and isoattenuating pancreatic lesions thanks to the differences in BV, BF, PS, and MTT values. BV and BF were also found to be useful for the characterization of adenocarcinoma and mass-forming chronic pancreatitis in study by Yadav et al 21 Concerning works aiming at assessing response to treatment and prognosis, BF was the most significant parameter, with high BF values corresponding to a lower survival and response to treatment.51,82
Computed Tomography in Renal Cancer
Similar to what has been found for studies on pancreatic cancer, all 3 studies on CTp for renal cancer applications had diagnostic purposes. Chen et al 27 found that CTp parameters were useful for differential diagnosis of kidney tumors. Similar results were found by Deniffel et al. 74 The third included study involved patients with adrenal tumors and revealed that BV parameter was able to characterize adenomas from non-adenomas. 70
Computed Tomography in Colon–rectal Cancer
Finally, concerning the five included works focused on CTp for the study of colon–rectal cancer, Khan et al 43 investigated the role of CTp parameters for quantifying different anatomical segments of colon–rectum. Significant differences were found in BF, BV, MTT, and PS. The same parameters were investigated to evaluate their association with CRC grade in study by Kim et al. 44 They found that BF and MTT were able to predict moderately differentiated CRCs. These findings were also confirmed by Xu et al. 63 Of note, BF and MTT were also found to be useful for the assessment of response to chemoradiation therapy in locally advanced CRC patients. 39 Finally, Andersen et al. showed the ability of CTp for the assessment of response to regorafenib treatment in patients with treatment-refractory metastatic CRC. 81
Quality Assessment
Based on the QUADAS-2 and QUIPS results, the overall quality of the included studies was considered good for our purposes. The results of the qualitative assessment are shown in Figures 3 and 4 and reported in the Supplementary Materials Tables S1 and S2. Regarding the QUADAS-2 assessment, the risk of bias was classified as low or unclear in all diagnostic studies, for all four QUADAS-2 domains. Concerns about applicability were classified as low across all diagnostic studies. Similarly, for the QUIPS assessment, the risk of bias was classified as low or moderate in all prognostic studies, for all 6 QUIPS domains. Quality assessment using QUADAS-2 tool for diagnostic studies. Quality assessment using QUIPS tool for prognostic studies.

Discussion
In this systematic review we aimed at investigating the role and clinical applications of CTp for clinical application in abdominal cancer, including diagnosis, grading, response to treatment, and prognosis. In recent years, the increasing availability and simplicity of CTp, together with its ability in quantification of the abnormal vasculature within tumors led to a growing interest in CTp imaging method for abdominal cancer applications. However, the still present drawbacks, mainly related with the lacking consensus on which CT protocol to use and the fact that published literature is based on small studies with different perfusion algorithms, have resulted in the missing integration of CTp into routine clinical practice protocols for abdominal imaging.14,85 In this scenario, we performed a systematic review on the role of CTp in abdominal cancer with a view to provide important new insights and help to reach a common view on the use of CTp for several clinical purposes in the management of abdominal cancer. After appropriate inclusion and exclusion criteria, we examined 57 studies from 2011 onwards, evaluating the role of CTp in oncologic diseases of abdominal district. Studies were classified according to the abdominal organ investigated and the clinical purpose explored in the study. Most of the included articles (33/57) deal with CTp at the level of the liver, while a low number of studies investigated CTp for oncologic diseases involving UGI tract (8/57), pancreas (8/57), kidneys (3/57), and colon–rectum (5/57). Interestingly, about 60% of included studies and even about 80% of studies on liver cancer aimed at evaluating the response to treatment of the oncologic patients by means of CTp. This could be related with the urgent need of developing individualized approach, in which the treatment strategies are targeted according to the tumor biology. It is well known neoangiogenesis is one of the key elements of tumor physiology that influences the aggressiveness of cancer and its response to treatment and that the presence of high vascularity usually suggests aggressive behavior and is associated with a poor outcome. Perfusion CT displays and permits quantification of the abnormal vasculature within tumors, specifically hypervascularized tumors such as HCC.2,4 This was also highlighted in the study by Goh et al 86 focused on the therapeutic assessment by means of CTp. Promising results were also found in the field of differential diagnosis of liver tumors, even if the number of studies investigating this issue were poor.47,48,53 Even if only 35% of the included studies were performed on other tumors involving abdominal district, our systematic review revealed that CTp parameters could also help in diagnosis, prognosis, grading, and response to treatment in these areas. Notably, included studies involving patients with pancreatic and colon–rectal cancer had diagnostic purpose. Therefore, a larger number of studies are required to deepen grading, prognosis, and response to treatment in the field of these diseases.
Characteristics of the included studies, such as patient treatment, study aim and setting, CTp parameters investigated, segmentation, and analysis, were highly variable across studies, preventing us from performing a meta-analysis.
Moreover, about 30% of the included studies were retrospective, and they are supposed to have more bias and should be validated through prospective studies.87,88 Other important limitations are that the number of patient samples included in the investigated studies was limited and that studies were predominantly single center, thus affecting the generalizability of the results.
To our knowledge, this is the first systematic review aiming at summarizing the role of CTp in abdominal cancer, exploring oncologic diseases of the whole abdominal area. Previous review studies aimed at review clinical applications and technical aspects of CTp.2,89 Kambadakone et al 2 reviewed CTp technical aspects and its oncologic and non-oncologic applications. However, this study was not recent and was not focused on abdominal cancer. Bellomi et al 89 discussed on CTp in solid body-tumors. However, this study was not systematic and was not specific for abdominal cancer. Notably, Ogul et al 4 reviewed the basic principles of CTp discussing both oncologic and non-oncologic applications in abdominal district. Moreover, Hansen et al 10 presented an overview of CTp applications in abdominal cancer. However, any of these studies performed a systematic analysis of CTp applications in abdominal district.
Conclusions
In conclusion, our study revealed that CTp could be a valuable functional imaging tool in the field of abdominal oncology. CTp has the potential to play a crucial role in the management of patients with abdominal cancer, particularly as a biomarker for monitoring the response to anti-tumoral treatment. However, data relating CTp features to clinical outcomes remain limited, mainly due to the limited samples and monocentric setting of the studies, as well as the missing consensus about scan protocols for standardized examination. More collaborative research and robust validation are thus required before this innovative technique can be included in routine clinical practice.
Supplemental Material
sj-pdf-1-dos-10.1177_15593258211056199 – Supplemental Material for A Systematic Review on the Role of the Perfusion Computed Tomography in Abdominal Cancer
Supplemental Material, sj-pdf-1-dos-10.1177_15593258211056199 for A Systematic Review on the Role of the Perfusion Computed Tomography in Abdominal Cancer by Nunzia Garbino, Valentina Brancato, Marco Salvatore and Carlo Cavaliere in Dose-Response
Footnotes
Author’s Note
The opinions expressed in the presented article are our own and not an official position of the institution or funder.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.