
Abstract
Objectives
This study aims to investigate a potential association between whole blood and lymphocyte Cyclosporin A (CyA) levels and the occurrence and frequency of infectious complications in kidney transplant patients.
Methods
The study involves 130 kidney transplant recipients who received CyA in addition to Mycophenolate Mofetil and steroids. CyA whole blood trough and maximum level (CyA BL0 and CyA BLm) as well as the corresponding levels in the lymphocytes (CyA L0 and CyA Lm) were measured for 6 months post-transplantation.
Results
Cytomegalovirus (CMV) as well as urinary tract infections (UTIs) were the most commonly diagnosed with an incidence of 24.6% and 26.2%, respectively. Only CyA L0 showed a significant association with CMV infection occurrence (adjusted OR = 1.051, 95% CI .997–1.025, P-value 0.046). A positive linear correlation was found between CyA BL0, CyA BLm and CyA Lm and the number of CMV episodes per patient.
Conclusion
We showed an association between the CMV infections occurrence and the trough lymphocyte level of CyA (CyA L0). Both lymphocyte CyA levels also correlated with the frequency of CMV infections. Further studies are needed to establish the optimal range of both CyA blood and lymphocyte levels and decrease the risk of opportunistic infections in high risk patients.
Keywords
Introduction
It is estimated that 15–21% of deaths in kidney transplant are secondary to infectious complications. Infections can range from mild asymptomatic to life threatening requiring intensive care unit admission or at least reduction in the immunosuppression level.1,2 Infection-related mortality might increase up to 30-fold in transplant recipients compared with the general population. 3
The first 3 months after transplantation, where immunosuppression is at its highest, represent the most critical period regarding the increased risk for infectious episodes. 4 There are many risk factors for infectious complications: donor-related due to the presence of active or latent infections; procedure-related such as the use of catheters; and recipient-related such as diabetes, advanced age and malnutrition. 5
Urinary tract infections (UTIs) are the most common bacterial infections in kidney transplant, followed by pneumonia, postoperative infections, and septicemia. They occur mainly in the first 3 months post-transplantation and hold deleterious effects on the recipient. 5 Overall, the most common causative pathogenic agent identified in several studies was E. coli and the main risk factor was female gender. 6 UTIs are mainly associated with increased graft loss, and may cause prolonged inflammation as well as renal scarring. 7
CMV is an important pathogen in kidney transplantation occurring mainly in the first 3 months post-transplantation in 20–60% of transplants. 8 Clinical manifestation varies among recipients with gastrointestinal symptoms being the most common especially in primary CMV infection. 9
Therapeutic drug monitoring (TDM) improves clinical outcomes, optimizes drug dosing and decreases occurrence of serious adverse events. TDM is crucial for drugs such as Cyclosporin A (CyA) that has a narrow therapeutic index. Routinely, dosage individualization is done by measuring the CyA concentration in blood and adjusting the dosage for each recipient to meet target drug concentrations associated with desirable clinical outcomes.
Few studies investigated the infectious complications in transplant patients and the association with immunosuppressant drug levels.10-14 Our study aims at assessing the association between (i) CyA whole blood and/or lymphocyte levels and the occurrence of infectious complications; and (ii) Between CyA blood and/or lymphocyte levels and the frequency of infectious episodes per patient.
Methods
Study Population
Study was conducted on 130 kidney recipients transplanted at Rizk hospital between 1998 and 2006. The study protocol was approved by the Lebanese University Ethics Committee. All patients received similar induction therapy with an anti-thymocyte globulin (ATG-Fresenius) during the first week post-transplantation to maintain a CD4 count of ≤50 for a total of 3–4 mg/kg body weight. They were maintained on a triple regimen including CyA, MMF, and prednisone. CyA was started at 7 mg/kg and dose was adjusted to maintain a maximum blood level between 1000–1500 and 500–1000 ng/mL during the first 3 months and 3–6 months, respectively.
Therapeutic Drug Monitoring
Blood samples were obtained immediately before and 2 hours following CyA administration for simultaneous whole blood (CyA BL0 and BLm) and lymphocyte (CyA L0 and CyA Lm) drug levels monitoring, respectively. Blood and lymphocyte levels were expressed in ng/mL and picogram per lymphocyte (pg/Lc), respectively.
All relevant clinical events and biological parameters from the first 6 months post-transplantation were recorded. The infectious complications were assessed clinically and confirmed by a series of para-clinical exams.
Statistical Analysis
Data were analyzed using the SPSS software version 23.0. Descriptive statistics were reported using means and standard deviations (SD) for continuous variables, and frequency with percentages for categorical variables. All statistical tests were two-sided, and the significant level was set at 0.05.
Association of CyA Levels With Occurrence of Infections
To investigate the relationship between CyA blood and lymphocyte levels and infections occurrence, multiple logistic regression analyses were performed with the occurrence of infectious complications particularly UTI and CMV as dependent variables. The final logistic regression model was reached after ensuring the adequacy of our data using the Hosmer and Lemeshow test.
CyA Blood and Lymphocyte Levels and Number of Infectious Episodes
Mean scores of the CyA Blood and lymphocyte levels were calculated for the patients divided into three categories according to the number of CMV, UTI, and total infection episodes (0, 1, and 2+). The CyA levels were compared between groups using the analysis of variance test. Bonferroni correction test on post hoc analysis was used for pairwise comparison. Spearman correlation coefficients were used to assess simple correlation between the CyA levels and the number of infectious episodes.
Correlations between the CyA levels and the number of infectious episodes were assessed by means of Spearman’s rank correlation analysis. Results are presented as Spearman’s coefficient (Rs) with appropriate P-value. All statistical tests were two-sided, and the significant level was set at .05.
Results
Demographics and clinical characteristics of renal transplant patients.

Incidence of viral infections and urinary tract infections (UTI) in kidney transplant recipients

N frequency, % percentage.
Association of CyA Levels With the Occurrence of Infections
Factors associated with the UTI occurrence among kidney transplant recipients.

OR unadj, Unadjusted odds ratio; OR adj, adjusted odds ratio; CI, Confidence interval.
P-value <.05 is considered significant.
Factors associated with the CMV occurrence among renal transplant recipients.

OR unadj, unadjusted odds ratio; OR adj, adjusted odds ratio; CI, Confidence interval.
P-value <.05 is considered significant.
CyA Levels and Number of Infectious Episodes
Patient distribution (number and %) by number of infectious episodes (CMV, UTI, and total) in kidney transplant recipients

CyA levels for different patient groups (0: no CMV infections, 1: one CMV infection, 2-4: two to four CMV infections).

Note: Results are expressed as means and standard deviations.
*P < .05 compared with the first group (no infection of CMV).
We then performed a correlation analysis to evaluate the association between CyA levels and infectious episodes. A positive linear correlation was found between CyA BL0, CyA BLm and CyA Lm and the total number of CMV episodes (Table 7 & Figures 1A-C). A. Relationship between total number of CMV episodes and mean CyA whole blood trough level (CyA BL0); B. Relationship between total number of CMV episodes and mean CyA maximum whole blood level (CyA BLm); and C. Relationship between total number of CMV episodes and mean CyA maximum lymphocyte level (CyA Lm). Correlation between CyA levels and CMV episodes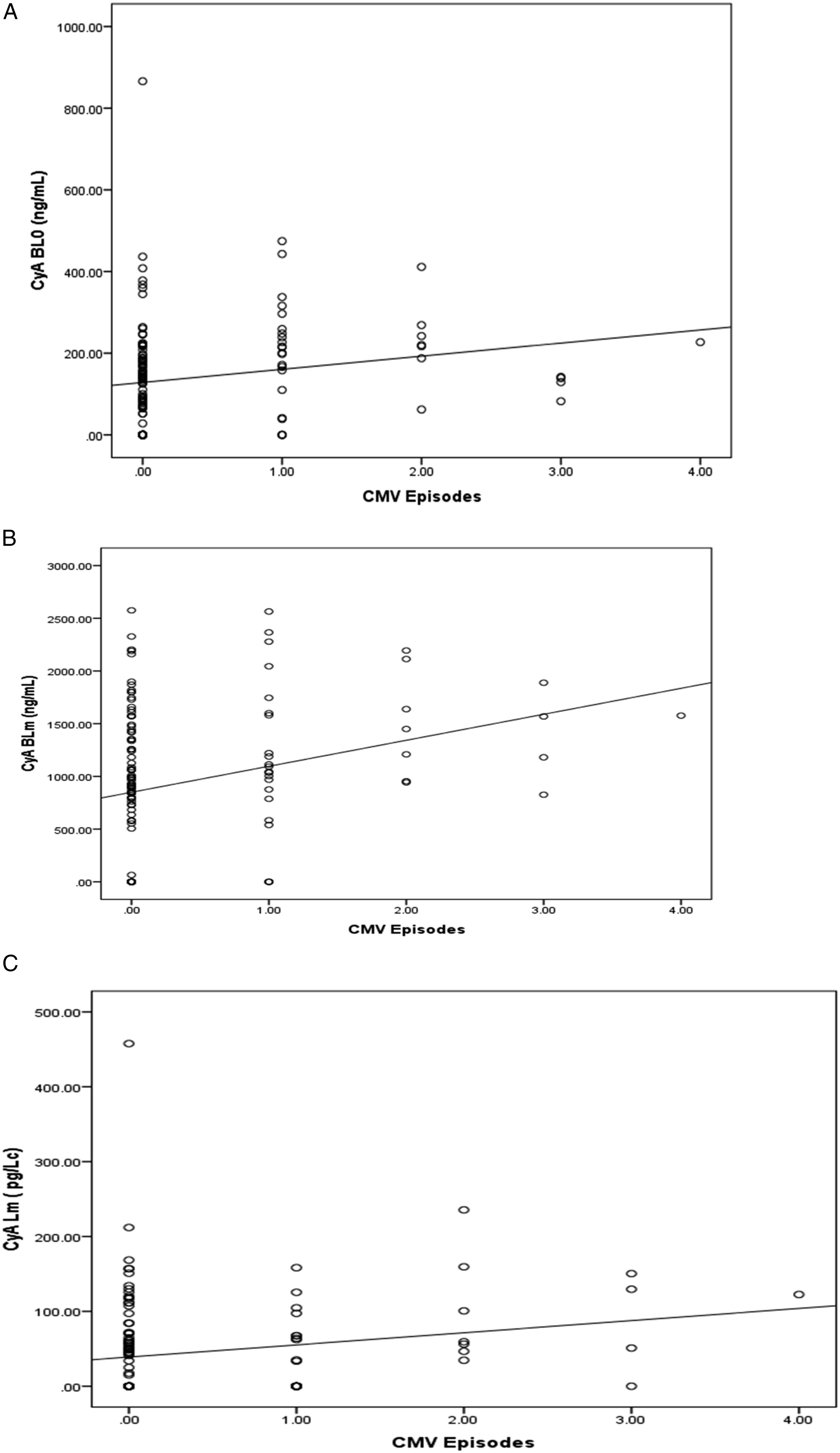

Discussion
Infectious complications are one of the major leading cause of death in kidney transplant patients. The first 6 months post-transplantation hold the greatest risk since immunosuppression would be at its highest level predisposing to infections with microorganisms, most commonly CMV and UTIs.11,15,16
Indeed, in the present study, the most common infections that were diagnosed within the first 6 months following kidney transplant were CMV infections and UTIs. Logistic regression did not show any association between the incidence of UTI and CyA levels. In contrast, a significant association was observed between CMV occurrence and the trough lymphocyte level CyA L0. Furthermore, our analysis showed a positive linear and exponential associations between most CyA blood and lymphocyte levels and the mean number of CMV infectious episodes per patient.
Very little data exists in Lebanon and the region on CyA level monitoring and the association with immunosuppression.17-19 Furthermore, in spite of the well-established genetic impact on the pharmacokinetic and pharmacodynamics effects of immunosuppressive drugs, knowledge of genetic variants affecting CyA bioavailability and bioactivity are also very limited as we have recently shown in the Lebanese population. 20 In spite of the limited resources in such a developing country, the availability of TDM is critical and certainly cost effective given its important role as a tool to monitor immunosuppressive therapy in order to ensure optimal therapeutic efficacy while minimizing serious adverse events such as bacterial and viral infections.
While all our patients received similar induction therapy, the mean CyA concentrations, measured in both blood and lymphocyte, showed wide variability with exceptionally high recorded standard deviation. Therefore, the lack of statistical significance between CyA levels and the occurrence of infections might be due to this considerable inter-individual variability in the context of a relatively small patient cohort.
This well-established inter-individual variability in immunosuppressive drug pharmacokinetics is related to a complex inter-play of a set of ethnic, genetic, and environmental factors. These environmental factors include recipient characteristics such as age, body composition, red blood cell mass, organ function, inflammation, food intake, and co-administration of other medications but also donor-related characteristics such as donor age, graft type, and function, ischemia reperfusion injury, and time since transplantation.21,22
It has always been challenging to conclude on the most relevant parameter for pharmacokinetic monitoring of CyA. 23 The time at which blood should be drawn has also been debated. Both whole blood trough concentration (C0) and concentration 2 hours (C2) post dose have been routinely used for years.24,25 Some studies reported, however, that these two blood levels do not always correlate with graft outcomes.26,27 In previous studies, we assessed those levels and compared them to intracellular levels, we found that maximum lymphocyte level correlates better than whole blood level with rejection-free outcome and lymphocyte count.17,19,28 In the current study, and despite an important inter-individual variability, the only level that was significantly associated with the occurrence of CMV infections was the trough lymphocyte level. The CyA lymphocyte level seem to be consistently associated with either the occurrence (CyA L0) or frequency (CyA Lm) of CMV infections in our sample of renal transplants. Monitoring CyA at the site of the action, the lymphocyte, seems to be accurately reflecting the immunologically relevant drug concentration and hence, providing a good correlate with clinical outcomes and side effects such as opportunistic infections.
Finally, in our patient population, results revealed a significant relationship between UTIs and female gender, the latter being the most important risk factor for UTIs. These findings are in agreement with those reported in other studies.6,29 The lack of association between UTI and blood and lymphocyte pharmacokinetic parameters may be explained by the fact that in addition to the wide variation in pharmacokinetic parameters, several non-immunological predisposing factors may play an important role in predisposing transplant and non-kidney transplant patients to infections of urinary tract. These factors include: the genitourinary anatomical anomalies commonly encountered in kidney transplant patients.
Patients weight was also shown to be associated with CMV occurrence. It is well known that CyA is distributed in adipose tissue due to its lipophilic property. 30 However, many reports showed that the distribution volume of CyA is independent of body weight and composition and suggested that the maintenance dose of CyA should probably be given on the basis of ideal body weight rather than total body weight (TBW). 31 The higher doses given to our patients based on TBW could have modulated the distribution balance between adipose, plasma and intra-lymphocytic compartments, resulting in more immunosuppression.
Conclusion
In conclusion, the present study clearly demonstrates a clear association between CyA lymphocyte levels and both the occurrence (CyA L0) and frequency (CyA Lm) of CMV opportunistic infections in a sample of kidney transplants.
Study Limitations
This is a retrospective analysis comprising a cohort of transplant patients from a single transplant center. Nevertheless, it is the first to investigate the correlation between CyA monitoring parameters and infectious complications in the MENA region.
Author Contributions
Antoine Barbari and Aline Milane designed, initiated the research, analyzed the study results, wrote a part of the manuscript, and reviewed the completed manuscript. Linda Mehanna entered the data into the SPSS, analyzed the study results, and wrote a part of the manuscript. Lara Osmani, Naja Saber and Nadine Mefleh collected data and wrote a part of the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.