
Abstract
Introduction. Intracranial epidermoid cysts are the most frequent congenital intracranial lesion. They rare and benign tumors that can present in different clinical situations depending on location and extension of the disease. Diagnosis is obtained with radiological imaging with RM and non-enhanced TC as elective investigating methods. Elective treatment is surgery, based on total/subtotal excision sparring healthy neurovascular structures, considering the benign nature of this lesion. Case Report. In this study we present the case of a 79-year-old woman affected by recidivist epidermal cyst of the posterior fossa. Clinical presentation was characterized by positional subjective vertigo, intense headache localized in the right part of the head increased by Valsalva maneuver and retroarticular subcutaneous swelling. Radiological investigation found a giant epidemoid cyst of the posterior fossa (8,4 x 4,8 x 5,8 cm), treated with surgery. In the postoperative, the patient was fine and no neurological deficit has been encounterd. REVIEW. In this study, we present a review of the literature regarding giant epidermoid cysts of posterior fossa. Only 11 cases were reported before ours, which actually is one of the largest ever described.
Introduction
[INTRO] Intracranial epidermoid cysts are the most frequent congenital intracranial lesion. It is estimated they represent 0.2–1.8% of all intracranial tumors and up to 7% of cerebellopontine angle tumors. 1 These rare and benign tumors are considered originating from the aberrant migration of ectodermal elements during embryogenesis. As a result, cutaneous epithelial tissue is trapped within neural tissue forming ectodermal inclusion cyst. 2
Epidermoid cysts are externally covered by a thin capsule of keratinized stratified squamous epithelium, which grows as a result of desquamation of epithelium, later breaking down into keratin and cholesterol. They are named “pearly tumors” for their white and glittering aspect. Inside the capsule they are filled with a soft, waxy, white material formed by the desquamation and deterioration of keratin from epithelial internal layer of the cysts. 3
Their growth rate is very slow and linear, so they tend to be diagnosed very lately when symptoms occur for compression or irritation of vascular or neurological structures. 4
[LOCATION] Although the vast majority of epidermoid cysts are intradural, they can rarely be extradural as well. They are commonly localized in the basal cisterns and spread along cisternal spaces, becoming adherent to adjacent neurovascular structures. They usually develop eccentrically in the cerebellopontine angle and para-sellar area. Other common locations are posterior cranial fossa, diploe, spinal canal. The following location are instead considered unusual: nasal dermal sinus, intracerebral, pineal gland, above and below tentorium, anterior fontanelle. 5,6,7
[SYMPTOMS] Giant epidermoid cysts are usually discovered in adults, commonly during the 5th decade (mean age of 55 years). Very few occur in childhood, because of their very linear and slow growth. 4 Epidermoid tumors’ symptomatology reflect the location of the tumor (Table 1): the most frequently involved cranial nerves are the V, VII, VIII and IX. Clinical neurological features can be caused by cranial nerves irritation (resulting in trigeminal or glossopharyngeal neuralgia or hemifacial spasm) or compression (with functional deficit). Permanent cranial nerve paralysis usually occurs only after the adhesion of the tumor to the nerve, causing ischemia. Other symptoms are usually attributed by compression of anatomical structures close to the neoformation. Patients often report headache and seizures at clinical presentation.
Mechanisms of rapid onset include complications as tension pneumocephalus, hydrocephalus, intracranial hemorrhage, trauma, bacterial and chemical (aseptic) meningitis and cerebral edema. 2,6 Another possible cause of sudden presentation of this tumor is due to vascular involvements, as a rare case of basilar artery dissection described by Pikis et al. 8
Symptoms Related to Involved Anatomical Structures.

Intracranial epidermoid cysts can rarely degenerate to Squamous Cell Carcinoma (SCC). Their malign degeneration is very little described in literature, but a few case reports show how a development of carcinomatous cells can set in the context of this benign, slow-growing region. In accordance with Solanki at al., the range time of malignant degeneration in the 31 since-then reported cases was from 6 to 33 months. In two-thirds of these cases, malignant change occurred after initial diagnosis and resection of benign epidermal cyst. Sudden cognitive deterioration after surgery and an initial remission was a common feature. 2,7, 16
[IMAGING] CT and MRI are fundamental diagnostic tools to gain useful information for surgical programming.
Nonenhanced CT scans show a well-defined, lobulated, low density mass insinuating around the cisterns, sometimes with deep invagination into the adjacent brain parenchyma. Most epidermoid cysts are non-enhancing, but may show calcification or hemorrhage. Moreover, CT scan allows to study diploe erosion: it’s unusual to observe both diploic tables involved (usually just the inner table is) but in giant epidermoid cysts a massive diploic erosion can be observed.
MRI allows to better characterize the lesion, showing low-intensity signal on T1-weighted images, high-intensity on T2-weighted images, FLAIR heterogeneous signal (due to cholesterol and cellular debris) with moderate peripheric enhancement and diffuse hypersignal. Epidermoid cysts show restricted diffusion with higher signal intensity than that of cerebrospinal fluid (CSF) on diffusion-weighted imaging.
Differential diagnosis is mainly with arachnoid cyst. It is possible to distinguish them through diffusion-weighted MRI sequences: epidermoid cysts are generally isointense with brain parenchyma. Moreover, MRI distinctive features of this kind of tumor include lobulated appearance of the margins, irregular bone infiltration and inhomogeneous signal intensity in all sequences. Other possible differential diagnosis include dermoid cysts, hemangiomas, eosinophilic granulomas. 3,5,17,18
[TREATMENT AND ITS COMPLICTIONS] Epidermoid cysts are benign, slow-growing tumors and for these characteristics medical therapy has not lead to significant results: surgery remains the mainstay of management.
Treatment of epidermoid cysts consists in simple aspiration and total or subtotal excision, depending on the adherence of the tumor capsule to the surrounding neurological and vascular structures. When the capsule is adherent to those structures, radical resection it’s not recommended because of its important complications. Although it would prevent recurrence, in these cases radical resection is not recommended considering the benign histological nature of this tumor. The suggested approach is conservative, sparing nervous and vascular structures whose damage would deteriorate patient’s life quality considerably. 1,4
Epidermoid tumors have a significant risk of perioperative complications (Table 2). The most frequent is recurrence, with a rate between 1% and 54%. 4 Other possible complications include permanent cranial nerve deficits, hydrocephalus and aseptic meningitis. This last complication is caused by breakdown products (keratin and cholesterol) produced during the desquamation of epithelial or as a result. It seems to occur in 40% of patients undergoing subtotal resection and it’s related to the amount of residual cyst. Perioperative administration of corticosteroid and intraoperative irrigation of hydrocortisone is effective in minimizing that risk. 1,6,19,20
Most Frequent Perioperative and Postoperative Complications of Giant Epidermoid Cysts of Posterior Fossa.

Personal Experience
We propose a singular case of a 79-year-old woman affected by epidermal cyst of the posterior fossa, treated with surgical asportation for the first time in 2001 and for the second time in 2007 for a recurrence. She presented in our Outpatient Department for positional subjective vertigo and intense headache localized in the right part of the head increased by Valsalva maneuver, without neurovegetative symptomatology. Spontaneous nystagmus was absent. Neurological physical examination was negative. The audiometric exam evidenced moderate bilateral pantonal presbycusis. Retroauricolar subcutaneous swelling was objectivly noticed.
Encephalic CT scan and MRI revealed a massive extradural lesion with important mass effect in posterior cranial fossa. CT scan (Figure 1) evidenced a capsuled round lesion, 8,4 x 4,8 x 5,8 cm with fluid-like density, reducing the amplitude of lateral recess of IV ventricle and shifting it to the left, stamping midline structures and eroding temporal bone. This lesion had all radiological characteristics of epidermal cysts previously cited: a well-defined, lobulated, low-density mass insinuating around the cisterns, with deep invagination into the adjacent brain parenchyma.

Preoperative coronal, sagittal and axial TC scan.
MRI (Figures 2 and 3) evidenced low signal intensity on T1-weighted images, high signal intensity on T2-weighted images and heterogeneous signal in FLAIR with moderate peripheric enhancement and diffuse hypersignal. MRI allowed a deeper preoperative study, identifying critical surgical areas and surgical planning with anatomical awareness, especially thanks to FLAIR sequences because of signal differences between the tumor and the brain.
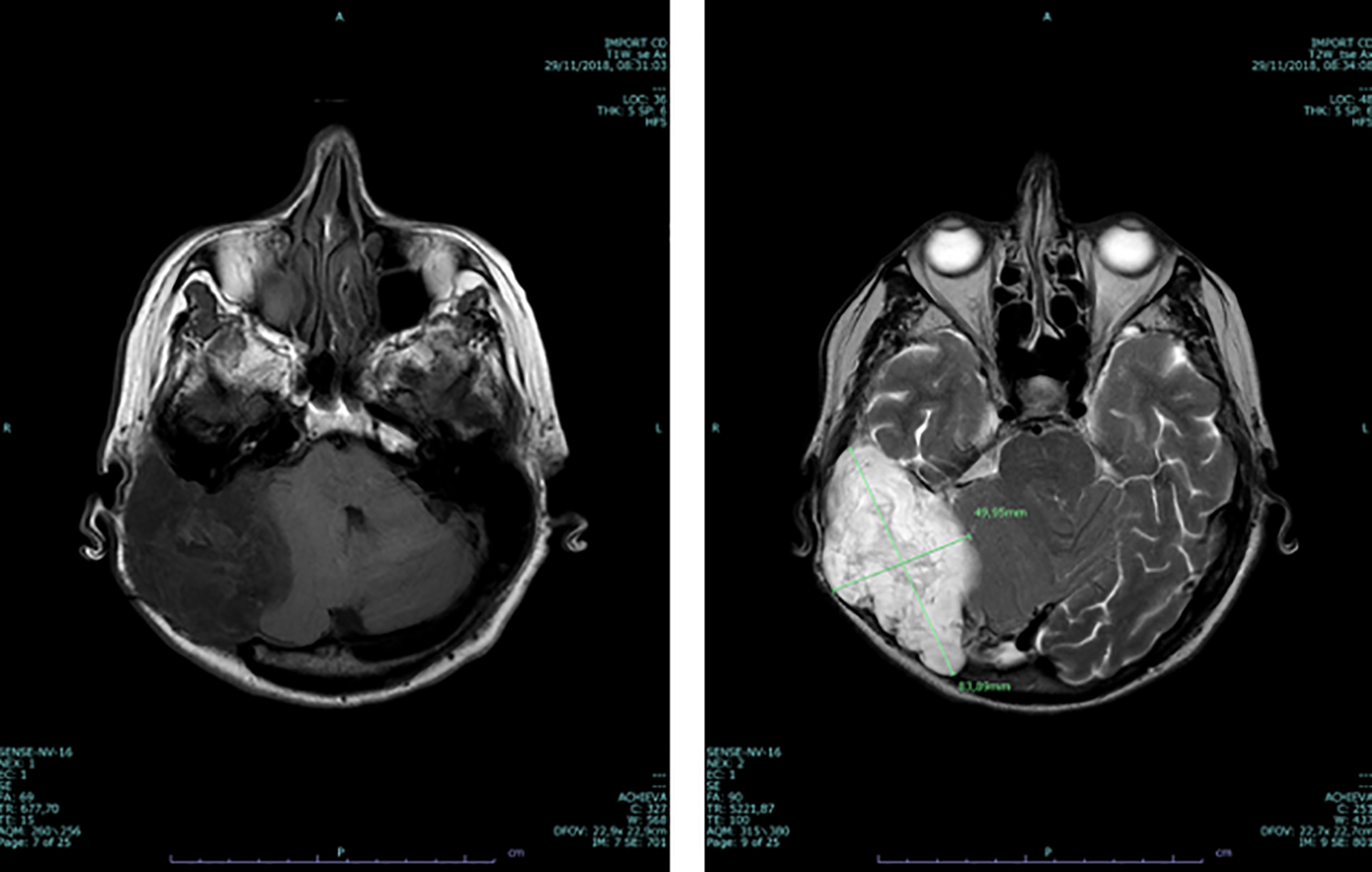
Preoperative axial MRI, T1 and T2-weighted images.

Preoperative axial, sagittal and coronal MRI, FLAIR sequences.
After accurate multidisciplinary evaluation, a surgical plan was made by otolaryngologists and neurosurgeons with intracranial access through temporo-parietal craniotomy (Figure 4).

Intraoperative surgical passages: craniotomy and mass display after craniotomy.
After removing the lesion, the pseudocapsule was partially detached from the matrix. The remaining matrix was coagulated in order to avoid entering in subaracnoideal space.
Despite a severe temporal bone erosion, cochleo-vestibular and facial nerve preservation was possible, monitoring their functionality during procedure.
The cavity has been filled with abdominal fat.
Postoperative course has been regular, with no access to Intensive Care Unit. Neurological functionality has been monitored with no deficit encountered. In the second post-operative day the patient completely recovered her autonomy and none of pre-operative symptoms remained.
She was discharged in the fifth post-operative day.
Post-operative CT scan (Figure 5) confirmed that the lesion was completely removed. The histological exam confirmed the epidermoid cyst diagnosis.
After two months otoscopy and audiometric exam were negative, the surgical wound was regular and no neurological deficit were encountered (Figure 6). Pre-operative headache and vertigo were solved with complete recovery.

Postoperative coronal, axial and sagittal TC scans.

A, Post-operative outcome. B, Post-operative check-up: negative cranial nerves examination.
Discussion and Literature Review
This case report illustrates our clinical and surgical management of a rare giant epidermoid cyst. It’s very infrequent to find a such dimension epidermoid cyst. The Group of Valencia evidenced epidermoid cyst superior than 5 cm are considered atypical and present peculiar heterogenous radiological features. In their study only 8 cases on 37 exceeded those dimensions. 21
At the best of our knowledge, 12 giant epidermoid cysts of the posterior fossa have been described, including our one, as reported in Table 3. 18,22,23
Giant Epidermoid Cysts of Posterior Fossa Reported in Literature.

In 2004 Maiuri F. et al reviewed the literature state-of-art. In their research 24 it was evidenced the presence of 30 large epidermoid cysts of posterior fossa described but just 4 of them (including their own) could be considered giant.
In 2011 the Sofia Group 13 reported the only known giant epidermoid cyst developed in posterior fossa with traumatic etiology and they reviewed literature published until that time. They updated the count of giant epidermoid cysts of the posterior fossa, adding 4 more cases.
Our review includes 4 more cases (including our one). It evidences an average age of presentation of 55 years, with a range from 27 to 79 years. Clinical presentation is frequently characterized just by headache and occipital subcutaneous swelling, usually without any other sign or symptom. This reflects the slow and benign growth of this kind of tumor. Cerebellar signs and symptoms appeared in 4 cases. Vertigo was present in just 2 cases, the one of Zhi-xin Duan et al 18 and our.
Cranial hypertension isn’t a common feature. The posterior fossa epidermoid cysts described by the Kensas City 25 and the Verona Groups 26 compressed posterior sinus and torcular Herophili and were the only associated with cranial hypertension. This confirms Maiuri F. et al hypothesis 24 in epidermoid cysts intracranial hypertension seems to be due to posterior sinus and torcular Herophili compression and obstruction more than to the mass effect of the tumor.
CT scan is considered an efficient preoperative exam, useful for investigation of bone erosion (common pattern in these kind of tumors). However the most complete imaging exam to study giant epidermoid cysts of posterior fossa is MRI. The most common pattern is an homogeneous hypointense lesion in T1-weighted, hyperintense in T2-weighted and heterogeneous signal in FLAIR images. Post-gadolinium peripheric enhancement was frequent but not always present. Moreover, MRI-angiography allowed an investigation of posterior sinus and torcular Herophili compression, defining the entity of venous obstruction.
Surgery is worldwide considered the election treatment. Complete tumor removal was performed with success in all reported cases. Anyway, radical excision was considered not worthy when the tumor was too much adherent to vascular and nervous structures, considering the benign histological nature of epidermoid cyst.
In literature lateral basal subtemporal and occipital approach were both practiced, depending on tumor position, development inside posterior fossa and surgeon confidence.
Conclusion
Giant epidermoid cysts of posterior fossa are extremely rare lesions and their management should be based on multidisciplinary approach, early diagnosis and accurate surgical plan mainly based on MRI, taking advantage of CT scan additional information.
Surgery is the most recommended treatment, with radical and multidisciplinary approach when possible. However considering epidermoid cysts’ benign histological nature, sparing nervous and vascular structure is suitable when they are too intimately involved by tumor’s expansion.
An imaging-guided surgical planning and the most appropriate multidisciplinary surgical approach are necessary to ensure neoplasia excision, low relapse rate and the best quality of life for the patient.
Footnotes
Authors’ Note
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.