
Abstract
To investigate whether D-dimer level could predict pulmonary embolism (PE) severity and in-hospital death, a total of 272 patients with PE were divided into a survival group (n = 249) and a death group (n = 23). Comparisons of patient characteristics between the 2 groups were performed using Mann-Whitney U test. Significant variables in univariate analysis were entered into multivariate logistic regression analysis. Receiver operating characteristic (ROC) curve analysis was performed to determine the predictive value of D-dimer level alone or together with the simplified Pulmonary Embolism Severity Index (sPESI) for in-hospital death. Results showed that patients in the death group were significantly more likely to have hypotension (P = 0.008), tachycardia (P = 0.000), elevated D-dimer level (P = 0.003), and a higher sPESI (P = 0.002) than those in the survival group. Multivariable logistic regression analysis showed that D-dimer level was an independent predictor of in-hospital death (OR = 1.07; 95% CI, 1.003-1.143; P = 0.041). ROC curve analysis showed that when D-dimer level was 3.175 ng/ml, predicted death sensitivity and specificity were 0.913 and 0.357, respectively; and when combined with sPESI, specificity (0.838) and area under the curve (0.740) were increased. Thus, D-dimer level is associated with in-hospital death due to PE; and the combination with sPESI can improve the prediction level.
Introduction
Venous thromboembolism, which clinically presents as either deep vein thrombosis (DVT) or pulmonary embolism (PE), is the third most common acute cardiovascular disease after myocardial infarction and stroke globally. 1 In epidemiological studies, PE has an annual incidence rate between 39 and 115 cases per 100,000 individuals and has high mortality. 2,3 As the clinical signs and symptoms of PE are nonspecific, patients with PE may be asymptomatic or diagnosed incidentally during an examination for another disease. A previous study reported that 34% of patients with PE die suddenly or within a few hours of acute onset before treatment can be initiated or take effect. Of the remaining patients with PE, 59% have PE diagnosed after death, and only 7% are correctly diagnosed with PE before death. 4 For these reasons, it is necessary to find reliable clinical parameters to assess the severity and prognosis of PE. Although the role of D-dimer in both PE diagnosis and the assessment of its severity and prognosis has attracted much attention over the years, the results of previous studies are inconsistent.
Plasma levels of D-dimer, a degradation product of cross-linked fibrin, are elevated in the presence of acute thrombosis due to the simultaneous activation of coagulation and fibrinolysis; it is a valuable diagnostic marker of acute PE. 5,6 Elevated D-dimer levels can also predict PE recurrence after discontinuation of anticoagulant treatment. 7 The extent of D-dimer elevation has been correlated with conditions of hypotension, tachycardia, and oxygen desaturation, as well as a high simplified Pulmonary Embolism Severity Index (sPESI), which can aid both the prognostic assessment and identification of patients with PE predicted to experience an adverse 30-day outcome. 8,9 As these results suggest that D-dimer level is associated with the extent of pulmonary artery obstruction, it could also possibly serve as a prognostic marker. Therefore, we investigated the extent to which plasma D-dimer level alone or together with the sPESI could predict the in-hospital death of patients with PE.
Materials and Methods
This retrospective study included 295 patients who had been admitted to the Second Medical Department of the First Hospital of Jilin University between January 2015 and June 2019, and were identified by a search of the hospital information system database for the diagnostic code of PE (ICD 10: I 26.900 X 001). Qualifying data were obtained for 272 patients (Figure 1). Of these patients, 138 (50.73%) were women, and the median age was 67 years (range, 16–92 years). Patients were assigned to either the survival group (n = 249) or the death group (n = 23).

Participant enrollment procedure to the present study.
The following clinical data were available from the patients’ medical files: general characteristics (age, sex, smoking status, drinking status, blood pressure, and heart rate), comorbidities (histories of hypertension, diabetes mellitus, chronic lung disease, infection, and cancer), laboratory parameters [levels of D-dimer, N-terminal pro-brain natriuretic peptide (NT-pro BNP), cardiac troponin-T (TNT), and arterial oxygen saturation (SaO2)], imaging examination results [transthoracic echocardiography (TTE), lower limb venous compression ultrasonography (CUS), and computed tomography pulmonary angiography], sPESI (based on 6 items, with 1 point for the presence of each item: age > 80 years, history of cancer, history of chronic cardiac or pulmonary disease, pulse rate > 110 beats/min, systolic blood pressure < 100 mm Hg, and SaO2 < 90%), and in-hospital death.
This study was performed according to the Declaration of Helsinki and its subsequent revisions, and the ethics approval was obtained from Ethics Committee of the First hospital of Jilin university.
Statistical Analysis
The statistical analysis was performed using IBM SPSS Statistics version 25.0 software. The Kolmogorov-Smirnov test was used to test for the normality of distribution in continuous variables. Because of a non-normal distribution of the continuous variables, the Mann-Whitney U test was used to assess differences between the 2 groups, and continuous variables were presented as median values and interquartile ranges (the median and 25th and 75th percentiles). Categorical data were expressed in rates, and it was analyzed using the Chi-squared test and Fisher’s exact test for the 2 groups. After performing univariate analysis between 2 groups, significantly obtained variables were used in a backward, stepwise multivariable logistic regression analysis. Spearman’s rank correlation coefficient was used to further exclude the influence of confounding factors. D-dimer level, sPESI and together with D-dimer and sPESI were analyzed with ROC. AUC was calculated in order to assess the predictable ability in-hospital death. For all tests, P < 0.05 were considered statistically significant.
Results
The clinical characteristics of all patients are summarized in Table 1. Among the 272 patients with PE, the median age was 67 years, 50.73% were women, 32.73% were smokers, and 12.50% were drinkers. Hypertension and diabetes mellitus were present in 37.5% and 15.44% of patients, respectively. Hypotension was evident in 2.21% of patients, with 22.69% having tachycardia. An SaO2 less than 90% and left ventricular ejection fraction (LVEF) less than 40% were present in 46.69% and 6.99% of patients, respectively. Chronic lung disease, cancer, and infection were present in 32.35%, 4.78%, and 62.41% of patients, respectively. Laboratory levels of D-dimer and NT-pro BNP were 4.98 ng/mL and 798.40 pg/mL, respectively, and 69.2% of patients exhibited elevated TNT levels. TTE showed right ventricular dysfunction in 62.87% of patients, and CUS showed DVT in 70.22% of patients. The median sPESI was 1. In-hospital mortality occurred in 8.46% of patients.
Clinical Characteristics of the Entire Participants.

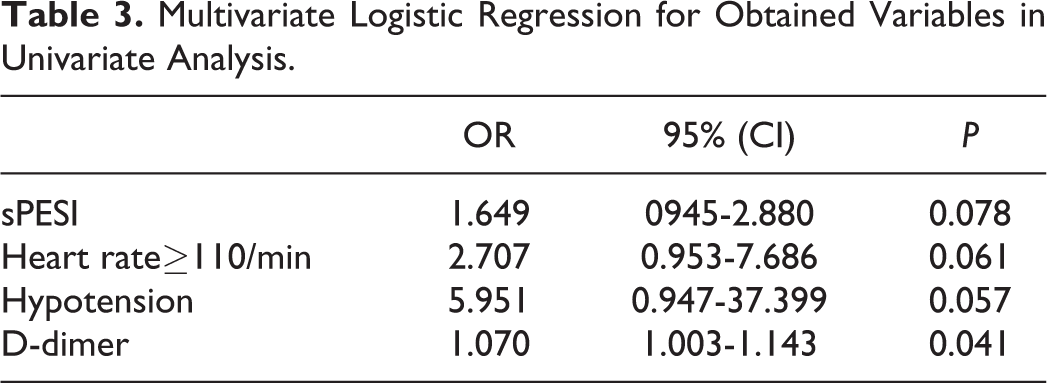
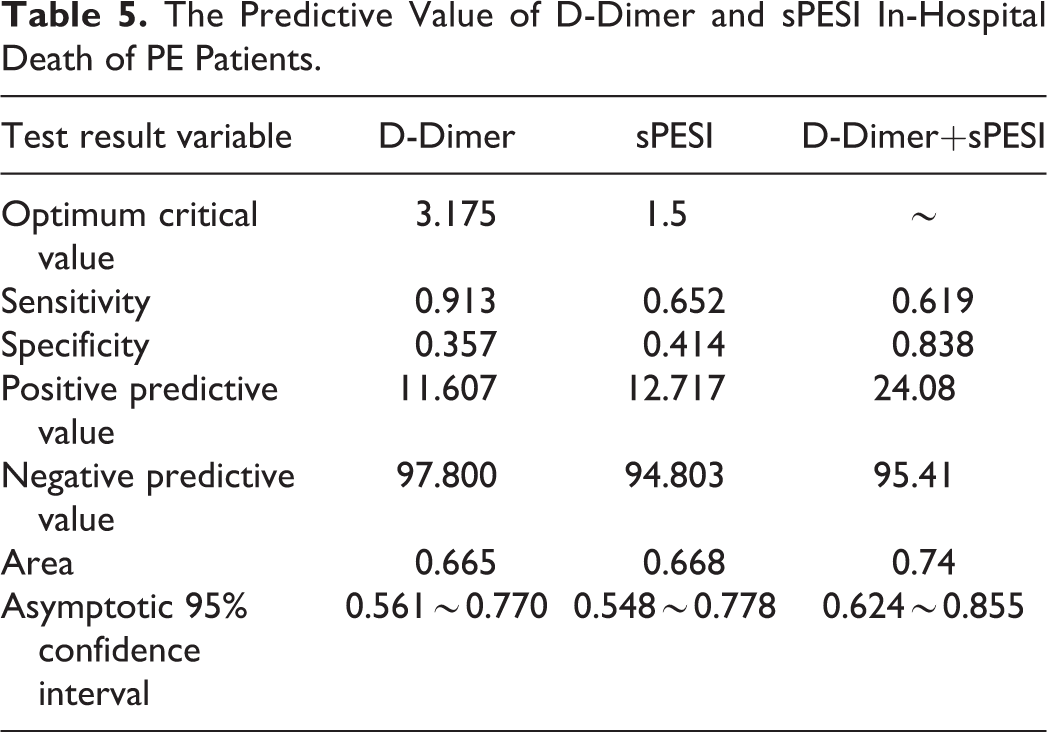
Compared with patients in the survival group, patients in the death group were significantly more likely to have histories of hypotension (2.41% vs. 13.04%, P = 0.008) and tachycardia (19.68% vs. 65.52%, P < 0.01), and have a higher D-dimer level (4.65 vs. 9.51 ng/ml, P = 0.003) (Figure 2) and sPESI (1 vs. 2, P = 0.002); they were also significantly less likely to exhibit a DVT (72.69% vs. 43.49%), according to the results of the univariate analysis (Table 2). The remaining characteristics were not statistically significant. The multivariable logistic regression analysis further revealed a significant association between D-dimer level and in-hospital death [odds ratio (OR) = 1.07, 95% confidence interval (CI) = 1.003–1.143, P = 0.041)] (Table 3). The sPESI (OR = 1.649, 95% CI = 0.945–2.88, P = 0.078), and histories of tachycardia (OR = 2.707, 95% CI = 0.953–7.686, P = 0.061) and hypotension (OR = 5.951, 95% CI = 0.947–37.399, P = 0.057) were not associated with in-hospital death. To further exclude the influence of confounders on the above results, Spearman’s rank correlation coefficient revealed that D-dimer had no correlation with hypotension (r = 0.050, P = 0.417), and had little correlation with a high sPESI (r = 0.125, P = 0.041) and tachycardia (r = 0.166, P = 0.007), because the r values of them were less than 0.4 (Table 4). Receiver operating characteristic (ROC) curve analysis showed that when the D-dimer level was 3.175 ng/mL, the predicted death sensitivity and specificity were 0.913 and 0.357, respectively, and the area under the curve (AUC) was 0.665 (95% CI = 0.561–0.770) (Figure 3, Table 5). When the sPESI was 1.5, the predicted death sensitivity and specificity were 0.652 and 0.414, respectively, and the AUC was 0.668 (95% CI = 0.548–0.778) (Figure 3, Table 5). When the D-dimer level was considered together with the sPESI, the predicted death specificity and AUC were higher than when the D-dimer level was considered alone (0.838 vs. 0.357 and 0.74 vs. 0.665, respectively, 95% CI = 0.624–0.855) (Figure 3, Table 5).

D-dimer level compared in 2 groups.
Clinical Characteristics in 2 Groups.

Multivariate Logistic Regression for Obtained Variables in Univariate Analysis.
The Correlation of D-Dimer With sPESI, Hypotension and Tachycardia by Spearman’s Rank Correlation Coefficient.


ROC curves of D-dimer, sPESI, and D-Dimer + sPESI for predicting in-hospital death of PE patients.
The Predictive Value of D-Dimer and sPESI In-Hospital Death of PE Patients.
Discussion
PE is a thromboembolism that can cause stenosis or even occlusion of the pulmonary artery. The occurrence of a thrombus leads to the activation of the fibrinolytic system as a result of its degradation. D-dimer is a degradation product that consists of cross-linked fibrin and is widely used for the assessment of pulmonary artery thrombus burden and disease severity. D-dimer is also used to determine the effectiveness of treatment and predict short- and long-term prognoses. Although elevated D-dimer levels can also occur in conditions such as cancer, inflammatory disease, surgery, and pregnancy, 10,11 the crucial role of D-dimer cannot be replicated by any other factor.
European Society of Cardiology 2019 guidelines for the diagnosis and management of acute PE, developed in collaboration with the European Respiratory Society, suggest that a suspicion of PE be excluded in patients either without clinical items and a D-dimer level less than 1,000 ng/mL, or with one or more clinical items and a D-dimer level less than 500 ng/mL. This differential diagnosis can rule out PE in patients with a low clinical probability of PE, thus reducing time and costs. 6 Previous studies showed that elevated D-dimer levels are associated with PE severity, 12 disease relapse after the termination of anticoagulant therapy, 13 and increased short- and long-term mortality. 14,15 Based on these observations, D-dimer levels may predict the survival of patients with PE and act as a surrogate marker of disease occurrence, recurrence, and prognosis. 12,16 Although some studies showed an association between D-dimer level and PE prognosis, 17,18 other studies were inconclusive. 19,20 One study showed that D-dimer level predicted PE severity but not long-term prognosis. 21
In the present study, we explored whether D-dimer level could predict in-hospital death among patients with PE. We found that D-dimer level was higher in the death group than in the survival group, according to the results of the univariate analysis (P = 0.003), and the multivariable logistic regression analysis further showed a significant association between high D-dimer level and in-hospital death. Although multivariate logistic regression is a common and reliable method to adjust confounding factors, it is often necessary to use other methods to further confirm the situation of confounders. The results of Spearman’s rank correlation coefficient further revealed D-dimer had no obvious correlation with hypotension, high sPESI and tachycardia, excluding the influence of other factors on the above results. During a further investigation of the sensitivity and specificity of D-dimer predictions of in-hospital death, ROC curves showed a sensitivity and specificity of 0.913 and 0.357, respectively, and the AUC was 0.665 (95% CI = 0.561–0.770) when the D-dimer level was 3.175 ng/mL, consistent with other research findings. 22,23 Our results suggest that elevated D-dimer level is an independent predictor of in-hospital death due to PE.
The sPESI is the most extensively validated parameter to date for estimating PE-related risks of early in-hospital mortality as well as 30-day mortality. 6,9,24 The prognostic performance of the sPESI has been confirmed by observational cohort studies, although it has not yet been prospectively used to guide the therapeutic management of patients with PE. In addition, guidelines recommend the Bova and HFABP scores were used to predict short-term or 30-day mortality in normotensive patients with PE. 25 In our study, the patients with hypotension were included, and the sPESI range was higher in the death group than in the survival group, according to the results of the univariate analysis (P = 0.002). ROC curves revealed that the predicted in-hospital death sensitivity and specificity were 0.652 and 0.414, respectively, and the AUC was 0.668 (95% CI = 0.548–0.778) when the sPESI was 1.5.
We also investigated whether both the D-dimer level and sPESI together improved the sensitivity or specificity of predicted in-hospital death due to PE. ROC curves showed that the 2 parameters together significantly improved the specificity from 0.357 to 0.838 and increased the AUC from 0.665 to 0.74, but reduced the sensitivity from 0.912 to 0.652.
Previous studies have found that other clinical parameters can predict PE severity and prognosis, suggesting that they could also predict in-hospital death due to PE. For instance, hypotension, tachycardia, and oxygen desaturation were all found to be associated with a worse prognosis for patients with PE. 21,25,26 In the present study, we compared age, gender, smoking status, drinking status, history of hypertension, history of diabetes mellitus, history of hypotension, heart rate, SaO2, LVEF, history of chronic lung disease, history of cancer, evidence of infection, D-dimer level, NT-pro BNP level, TNT level, right ventricular dysfunction, and sPESI between the death and survival groups. In addition to D-dimer level and sPESI, a history of hypotension and evidence of tachycardia were significantly more frequently observed in the death group than in the survival group, according to the results of the univariate analysis. These results are similar to those of other studies and demonstrate a relationship between these parameters and in-hospital death due to PE.
This study has some limitations. First, it had a retrospective, observational, single-center design. Second, our small sample size resulted in large 95% CIs and low numbers of events, making it difficult to obtain robust estimates for outcomes. Finally, our measurement of D-dimer levels at a single time point may not reflect the conditions of the patients over time. Thus, prospective, multicenter studies with larger cohorts are needed to confirm our findings and draw definitive conclusions.
Conclusion
Despite the limitations of our retrospective study, we found that D-dimer level was associated with in-hospital death of patients with PE. Considering D-dimer level together with the sPESI could improve the specificity of predicted in-hospital death for patients with PE.
Footnotes
Authors’ Note
Zi-Kai Song and Haidi Wu contributed equally to this work.
Acknowledgments
We thank all participants for their supports and participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.