
Abstract
Objective:
The aim of this study was to evaluate the levels of caveolin-1 in thyroid follicular epithelial cells of papillary thyroid cancer, follicular thyroid cancer, and nonmalignant thyroid nodule benign follicular adenoma, as well as to explore the relationship between the levels of caveolin-1 and thyroid function.
Methods:
Thirty cases of papillary thyroid cancer, 10 cases of follicular thyroid cancer, 32 cases of nonmalignant thyroid nodule benign follicular adenoma, and 30 controls were enrolled in this study. Caveolin-1 expression in tissue specimens obtained from these cases was evaluated by immunohistochemistry and Western blotting.
Results:
Caveolin-1 expression in thyroid epithelial cells of patients with papillary thyroid cancer, particularly female patients, was significantly higher than that in patients with follicular thyroid cancer and nonmalignant thyroid nodule benign follicular adenoma (P < .005). Serum thyroid-stimulating hormone (TSH) levels in the caveolin-1-positive expression group were lower than that in the caveolin-1-negative expression group, and the lowest expression of caveolin-1 was detected in tissues of patients with Graves’ disease. The serum TSH level was associated with caveolin-1 expression in thyroid epithelial cells.
Conclusion:
Caveolin-1 may participate in regulating thyroid function and is a potential biomarker of follicular thyroid cancer.
Introduction
Thyroid nodules were prevalent in the last decade in the United States and elsewhere. Ultrasonography screening found that the prevalence of thyroid nodules was 19% to 67% in the general population, and only 8% to 16% of these nodules were thyroid cancers. 1 Papillary thyroid carcinoma (PTC) accounts for approximately 85% of thyroid cancers, and most PTCs have a good prognosis. 2 To avoid unnecessary surgery on benign thyroid nodules, fine needle aspiration biopsy is a simple, safe, cost-effective, and efficient technique for identifying malignant thyroid nodules before surgery. However, the remaining 20% to 25% of thyroid nodules have an indeterminate cytologic diagnosis based on the Bethesda classification scheme. 3 When the results of fine needle aspiration biopsy are indeterminate, clinicians often have difficulties in making decisions regarding surgical treatment. In recent years, B-type Raf kinase (BRAF) mutation molecular testing has become the most common method for identifying ambiguous thyroid nodules. However, the sensitivity and predictive value of BRAF testing are questionable. 4,5
Caveolins are a unique family of proteins composed of 3 members, caveolin-1, caveolin-2, and caveolin-3, which oligomerize to generate large macromolecular complexes. Caveolin-1 is a 22-kDa primary structural protein of caveolae located in plasma membranes and expressed in a variety of cells such as adipocytes, pneumocytes, fibroblasts, and endothelial cells. 6,7 Caveolin-1 acts through its scaffolding domain as a modulator of several intercellular signal transduction proteins (eg, G proteins, 8 Src-like tyrosine kinases, 9 tyrosine kinase receptors, cyclic Adenosine monophosphate (cAMP)-dependent protein kinase, 10 and endothelial nitric oxide synthase 11 ) to activate cell proliferation. The caveolin-1 protein is also expressed on human thyroid cell membranes. It is associated with apical membranous localization of the thyroperoxidase (TPO)-dual oxidase protein complex to form thyroxisomes in human epithelial thyroid cells; thyroxisomes must be located at the apical membrane to be active in terms of efficient hormone synthesis. A lack of caveolin-1 expression on the apical membranes of thyroid epithelial follicular cells is associated with localization of thyroxisomes in the thyrocyte cytoplasm. 12,13
Prolonged stimulation of isolated human thyrocytes by thyroid-stimulating hormone (TSH)/cAMP/cAMP-dependent protein kinase inhibits caveolin expression. 14 Downregulation of caveolin-1 protein is observed in human follicular thyroid carcinoma (FTC) and human thyroid autonomous adenomas. 15,16 The link between thyroid function and caveolin-1 expression has never been investigated. Furthermore, caveolin-1 is downregulated in ovarian, lung, and mammary carcinomas, whereas it is overexpressed in bladder, esophageal, thyroid, and prostate carcinomas. 17 However, the expression status of caveolin-1 in PTC remains unclear. 16,18 -20
To determine whether caveolin-1 protein expression is useful as a potential clinical biomarker of PTC and its relationship with thyroid function, we evaluated its expression in different types of thyroid nodules and tissues of patients with Graves’ disease (GD) by both immunohistochemistry staining and Western blotting analyses. To better understand the factors affecting caveolin-1 expression in thyroid tissues, we investigated the relationship between its expression and clinical parameters in patients who had undergone thyroid surgery. In this study, we confirmed that caveolin-1 expression is characteristically upregulated in PTC and that the positive expression prevalence of caveolin-1 in human thyroids was negatively related to human serum TSH levels.
Materials and Methods
Tissue Specimens
Thyroid tissue specimens were obtained from 102 patients (80 females and 22 males) who underwent surgery in the Department of Surgery, Ma’anshan People’s Hospital. Patients were categorized according to their histopathological results. This classification resulted in 4 groups: PTC, FTC, benign adenoma (BA), and control. The control group was defined as patients with paranodular thyroid tissue located 1 cm away from a benign follicular adenoma. All clinical-pathological data were obtained from the patients’ medical records. This project (MR20160226) was approved by the ethics committee of the hospital, and informed consent was obtained from participating patients. For immunohistochemical studies, tissues were fixed in 10% formalin and paraffin embedded.
Antibodies
The rabbit antihuman polyclonal antibody against caveolin-1 was purchased from Abcam (Ab2910; Cambridge, United Kingdom). The antibody was applied at a dilution of 1:500. The dilution of the second antibody was 1:2000.
Immunohistochemistry
For immunostaining, sections (5-µm thickness) were dewaxed and rehydrated. The sections were then heated in a pressure cooker at 121°C for 3 minutes in citrate buffer to retrieve antigenic activity and then cooled to approximately 25°C. H2O2 of 0.3% was incubated in pure water for 20 minutes to inhibit endogenous peroxidase activity. The sections were then incubated with a primary polyclonal antibody for caveolin-1 at 4°C overnight. After rinsing in phosphate-buffered saline (PBS), the specimens were treated with peroxidase-labeled goat antirabbit immunoglobulin IgG H&L (A0208; Beyotime Biotechnology, Shanghai, China) for 30 minutes. After rinsing 3 times in PBS, the peroxidase reaction was visualized by incubating the sections with 0.02% 3,3′-diaminobenzidine tetrahydrochloride in 0.05 M Tris buffer with 0.01% H2O2. The sections were counterstained with hematoxylin. Negative control sections omitted the primary antibody.
Immunohistochemical Evaluation
Evaluation included the proportion of reactive cells within the lesion (the percentage) as well as staining intensity. We selected the 3 high-magnification fields of the most abundant expression of cav-1 protein. The intensity of caveolin-1 immunostaining was evaluated by light microscopy. We estimated the fraction of positive cells presenting caveolin-1 positivity by defining immunoreactivity as clearly observed in the cytoplasm of thyroid follicular cells or in the thyrocyte membranes. The results of 3 counts from the 3 most highly expressed fields of vision were averaged. We classified each case based on the positive cell rate: negative expression was defined when the number of immunoreactive cells was less than 10%, while staining equal to or more than 10% of the immunoreactive cells was regarded as positive expression of caveolin-1 protein.
Clinical Biochemistry
Venous blood samples were obtained from individual participants and subjected to routine laboratory tests for full blood counts and serum chemistry using a DPP-800 biochemical automatic analyzer (Roche, Indianapolis, Indiana). Serum concentrations of TSH, total T3 (TT3), free triiodothyronine (FT3), total T4 (TT4), and free thyroxine (FT4) in individual participants were determined using a Modular Analytics E-170 Immunology Analyzer (Roche). Anti-TPO and antithyroglobulin antibodies (TG-Ab) were measured by an electrochemical luminescent immunoassay according to the manufacturer’s instructions (Roche).
Reference normal ranges: TSH: 0.27 to 4.20 mIU/L; TT3: 1.18 to 3.40 nmol/L; TT4: 57.9 to 162 nmol/L; FT3: 3.40 to 6.50 pmol/L; FT4: 10.3 to 22.0 pmol/L; anti-TPO antibody (TPO-Ab): 0 to 60 IU/L; and anti-TG-Ab: 0 to 60 IU/L.
Preparation of Tissue Protein Samples
Tissues (approximately 100-300 mg) were cut into small pieces (1-2 mm2) and placed into 2-mL centrifuge tubes. Three steel balls were then added to each tube. Lysates were prepared as follows: a certain amount of radio Immunoprecipitation assay (RIPA) protein lysates was prepared (the actual amount was determined according to the amount of protein), and the lysates contained protease inhibitors at a final concentration of 1 mM. Five microliters of protein lysates were mixed with 50 µL phenylmethylsulfonyl fluoride, and the lysates were placed on ice. Samples were then moved to an ice-grinding box, balancing, and ground and homogenized at 4°C, 60 Hz, for 2 minutes. The homogenate was centrifuged at 4°C at 13 800g for 10 minutes. The supernatant was added to the sample buffer (4:1), heated at 100°C for 10 minutes, and then frozen at −20°C.
Western Blot
Samples containing equal amounts of protein were separated by 12% sodium dodecyl sulfate polyacrylamide gradient gel electrophoresis, then electroblotted onto polyvinylidene difluoride membranes. The membranes were blocked with 5% skim milk at room temperature for 2 hours and incubated with the primary antibody (anti-caveolin-1, ab2910; anti-glyceraldehyde 3-phosphatedehydrogenase, the dilution is 1:2000, ab181602, Abcam, the dilution is 1:5000) overnight at 4°C. The molecular weight of cav-1 protein is 21 kDa. The membranes were then washed in PBS containing 0.05% Tween-20 3 times and incubated with the horseradish peroxidase–conjugated secondary antibody at room temperature for 2 hours. Protein bands were visualized by enhanced chemiluminescence (PerkinElmer, Waltham, Massachusetts).
Statistical Analyses
SPSS 19.0 (SPSS, Inc, Chicago, Illinois) was used in this study. The data are expressed as the mean ± standard deviation. Statistical analyses were performed using Student t test or, for non-normally distributed data, Mann–Whitney test and Wilcoxon rank sum test with 2-tailed distribution. All experiments were carried out at least 3 times independently. Chi-square test and Fisher exact probability test was used to examine the relationship between variables. A multiple stepwise regression method was used to analyze the independent risk factors for caveolin-1 expression. A P value <.05 was considered as statistically significant.
Results
Patient Clinical Characteristics
We collected 102 nodule specimens from 80 female and 22 male patients. There was a much higher incidence of thyroid nodules in females than in males. The age of males was greater than that of females (P = .006). Furthermore, females showed significantly increased TG-Ab levels compared to males (P = .028, Table 1). Although TPO-Ab was elevated in females, there was no significant difference between the level of TPO-Ab in different genders. In contrast, the female group showed higher TSH and lower FT3 levels compared to the male group, but the difference was not significant.
Comparison of Clinical Parameters Between Female and Male Patients.

Abbreviations: FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyroid-stimulating hormone; TG-Ab, thyroglobulin antibody; TPO-Ab, thyroid peroxidase antibody; TT3, total T3; TT4, total T4.
Clinicopathological Characteristics of Caveolin-1 Protein in Thyroid Carcinoma Specimens
Positive immunohistochemical staining for caveolin-1 protein was observed at the cell membrane and/or in the cytoplasm of thyroid follicular epithelial cells (Figure 1). Caveolin-1 expression was frequently detected in vascular endothelial cells, which were used as an internal positive control. Moreover, caveolin-1 expression was strongest in PTC, while much lower levels were observed in FTC compared to the control specimens (Figure 1).

Expression patterns of caveolin-1 in thyroid follicular tissue of PTC, FTC, BA, and control tissues by immunohistochemistry. Caveolin-1 is expressed at a much higher level in PTC (A, E) compared to in FTC (B, F), BA (C, G), and control tissues (D, H), which did not significantly differ from each other. The caveolin-1 protein is most strongly expressed in vascular endothelial cells of thyroid tissue. (A-D) Scale bar: 100 µm; (E-H) scale bar: 25 µm. BA indicates benign adenoma, FTC, follicular thyroid cancer; PTC, papillary thyroid carcinoma.
Relationship Between Expression of Caveolin-1 Protein and Clinical Outcomes in Patients With Different Thyroid Lesions
We further analyzed the prevalence of caveolin-1-positive expression in PTC compared to the FTC, BA, and control groups (Table 2). Thirty cases of PTCs, 10 of FTCs, 32 of BAs, and 30 control patients were included in the study. Caveolin-1-positive expression was found in 18 (60%) PTCs, 1 (10%) FTCs, 8 (25%) BAs, and 6 (20%) controls. Positive rates were significantly higher in patients with PTC compared to those with FTC, BA, and control patients (χ2 = 15.643, P = .001). Caveolin-1 expression levels were not significantly different among the FTC, BA, and control groups.
Expression of Caveolin-1 Protein in PTC, FTC, BA, and Control Groups.a

Abbreviations: BA, benign adenoma; Cav-1, caveolin-1; FTC, follicular thyroid cancer; PTC, papillary thyroid carcinoma.
a χ2 = 15.643, P = .001.
Furthermore, in female PTC patients, the prevalence of positive caveolin-1 protein expression was 69.2%, while no males expressed this protein; this difference was significant (P = .01). However, this phenomenon was not found in other thyroid lesions or in the control group (Table 3).
Expression of the Caveolin-1 Protein in Female and Male PTC Patients.a
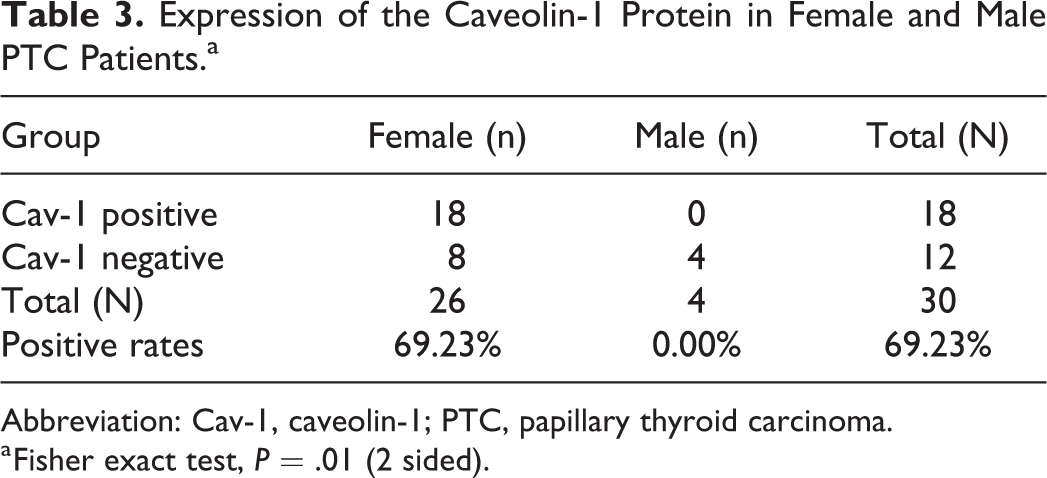
Abbreviation: Cav-1, caveolin-1; PTC, papillary thyroid carcinoma.
a Fisher exact test, P = .01 (2 sided).
Demographics, Thyroid Function, and Thyroid Autoantibodies Features in Patients With Thyroid Carcinomas
Patients were categorized according to their histopathological results. This classification resulted in 4 groups: PTC, FTC, BA, and control. The control group was defined as patients with paranodular thyroid tissue located 1 cm away from a BA. We compared the age, thyroid function, thyroid autoantibodies, and caveolin-1 expression status among these 4 groups and found that FT3, TG-Ab, and caveolin-1-positive expression were significantly different between the PTC and control groups. The FT3 level was significantly lower, while TG-Ab and positive caveolin-1 expression status were markedly higher in PTC than in the control group (P = .002, .049, and .002, respectively; Mann-Whitney U test). Compared to the FTC group, FT4 was significantly higher in patients with PTC (P < .05). However, the levels of TT4 were lower in FTC than in controls (P < .05; Tables 4 and 5).
Comparison of Thyroid Hormone and Thyroid Autoantibody Levels Among PTC, FTC, BA, and Control Groups by Students t Test.
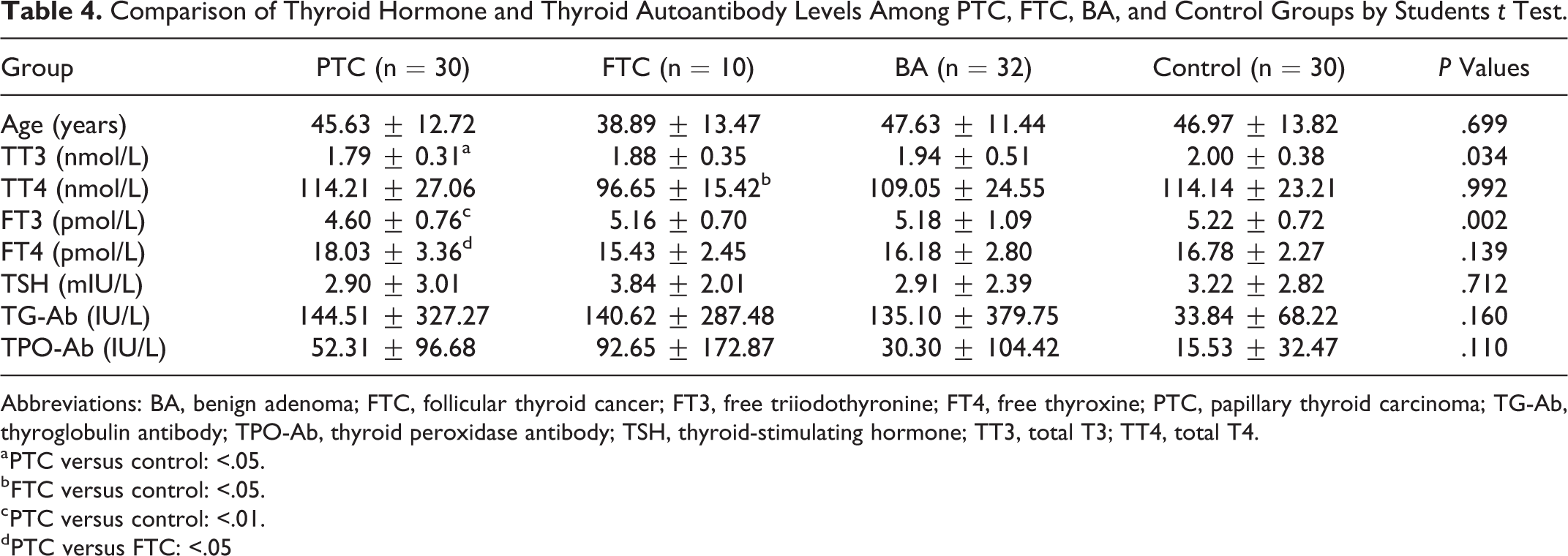
Abbreviations: BA, benign adenoma; FTC, follicular thyroid cancer; FT3, free triiodothyronine; FT4, free thyroxine; PTC, papillary thyroid carcinoma; TG-Ab, thyroglobulin antibody; TPO-Ab, thyroid peroxidase antibody; TSH, thyroid-stimulating hormone; TT3, total T3; TT4, total T4.
a PTC versus control: <.05.
b FTC versus control: <.05.
c PTC versus control: <.01.
d PTC versus FTC: <.05
Comparison of Thyroid Hormone and Autoantibody Levels Between PTC and Control Patients by Mann-Whitney U Test.a

Abbreviations: Cav-1, caveolin-1; FT3, free triiodothyronine; FT4, free thyroxine; PTC, papillary thyroid carcinoma; TG-Ab, thyroglobulin antibody; TPO-Ab, thyroid peroxidase antibody; TSH, thyroid-stimulating hormone; TT3, total T3; TT4, total T4.
a Grouping variable: group PTC and control.
Comparison of Clinical Parameters Between Caveolin-1-Positive and Caveolin-1-Negative Patients
When the demographics, thyroid function, and levels of thyroid autoantibodies were compared between the caveolin-1-positive and caveolin-1-negative groups, the serum TSH level was found to be significantly lower in the caveolin-1-positive expression group (P = .043; Mann–Whitney U test). Although somewhat higher TG-Ab and higher TPO-Ab values were observed in the caveolin-1-negative group, the change was not significant (Tables 6 and 7).
Comparison of Demographics, Thyroid Function, and Thyroid Autoantibodies Between Caveolin-1-Positive and Caveolin-1-Negative Groups.a

Abbreviations: Cav-1, caveolin-1; FT3, free triiodothyronine; FT4, free thyroxine; TG-Ab, thyroglobulin antibody; TPO-Ab, thyroid peroxidase antibody; TSH, thyroid-stimulating hormone; TT3, total T3; TT4, total T4.
Comparison of Demographics, Thyroid Function, and Thyroid Autoantibodies Between Caveolin-1-Positive and Caveolin-1-Negative Groups by Mann-Whitney Test.

a Grouping variable: Cav-1.
Abbreviations: Cav-1, caveolin-1; FT3, free triiodothyronine; FT4, free thyroxine; PTC, papillary thyroid carcinoma; TG-Ab, thyroglobulin antibody; TPO-Ab, thyroid peroxidase antibody; TSH, thyroid-stimulating hormone; TT3, total T3; TT4, total T4.
Relationship Between Caveolin-1-Positive Expression and Clinical Features
We considered the incidence of caveolin-1-positive expression as a dependent variable in stepwise logistical regression model analysis. Adjusted for the effect of age, TT4, TT3, FT4, FT3, TG-Ab, TPO-Ab, and serum TSH levels were negatively related to caveolin-1 protein expression. The serum TSH level was an independent predictive factor for caveolin-1-positive expression (adjusted R 2 = 4.8%; P = .033).
Caveolin-1 Protein Expression Levels in Different Thyroid Tissues
We also evaluated caveolin-1 protein expression levels in PTC, para-PTC tumor tissues (less than 1 cm away from tumor parenchyma tissues), BA, para-BA tissues (less than 1 cm away from solid adenoma tissues), and hyperthyroid tissues from patients with GD. Compared to control thyroid tissue (more than 1 cm away from solid adenoma tissues in the BA group), caveolin-1 expression was significantly increased in BA solid tumors and markedly decreased in PTC thyroid and GD samples as demonstrated by Western blotting. Caveolin-1 protein was more abundant in the tumor parenchyma than in its paired para-tumor tissues. Hyperthyroidism states in GD showed the lowest caveolin-1 expression compared to that in any other thyroid tissues. The caveolin-1 protein levels ranged from high to low expression in thyroid tissues as follows: BA > control > PTC > BA-para > PTC-para > GD (Figure 2).

Caveolin-1 expression in tumor parenchyma of PTC, PTC-para, BA, BA-para, GD, and control tissues by Western blot (samples of PTC and para-PTC, BA, and para-BA were paired from the same patients, respectively) (A). The caveolin-1 expression level ranged from high to low in thyroid tissues: BA > control > para-BA, PTC > para-PTC > GD (B). BA indicates benign adenoma; FTC, follicular thyroid cancer; GD, Graves’ disease; PTC, papillary thyroid carcinoma.
Discussion
In the present study, we explored the potential of caveolin-1 protein as a new biomarker of PTC. We demonstrated that caveolin-1 protein is highly expressed in PTC specimens. Furthermore, we provided the first evidence that caveolin-1 expression is related to thyroid function in humans. Serum TSH levels and caveolin-1-positive expression rates were negatively related, and caveolin-1 protein was found to be dramatically reduced in hyperthyroidism thyroid tissues in GD. We speculated that caveolin-1 expression is regulated by TSH according to the degree of oxidative status in thyroid cells.
We focused on PTC in this study because it is the most common type of thyroid carcinoma, accounting for more than 50% of all thyroid cancer-related deaths. This is nearly 3-fold the number of thyroid cancer deaths compared to FTC and nearly 4-fold that from undifferentiated anaplastic thyroid carcinoma. 21 A previous study revealed BRAF mutations in approximately 45% of clinically evident PTC cases and in 18% of microcarcinomas. 22 Tumors with BRAF mutations are associated with more aggressive biological behavior. 23,24 We noticed that most PTCs (particularly in thyroid microcarcinomas in which the diameters of nodules were less than 1 cm) did not have the BRAF mutation. The caveolin-1 protein has been increasingly reported as a biomarker related to malignant tumors, particularly in breast and prostate cancer in recent years. Caveolin-1 is also a novel biomarker for radiation therapy resistance and has the potential to improve the clinical outcome of patients with cancer undergoing this type of treatment. 25 Altogether, these findings suggest that caveolin-1 has an important role in diagnosis, prognosis, follow-up, and therapeutic effects, among others, in cancer.
We explored caveolin-1 protein expression in PTC and assessed the possibility of using this protein as a biomarker in differentiated thyroid carcinomas. We also found that caveolin-1 was expressed in human thyroid follicular cells previously identified by Costa et al in human and animal thyrocytes. 26 We examined caveolin-1 in PTC, FTC, and BA and found that the caveolin-1-positive expression rate was markedly and significantly increased in PTC specimens compared to that in FTC, BA, and control specimens (60%, 10%, 25%, and 20%, respectively). However, no significant difference among FTC, BA, and control tissue samples was observed. Although the lowest positive expression rate of caveolin-1 in FTC did not show a significant difference in our study, the trend was still consistent with those observed in previous studies showing that FTC exhibits downregulated caveolin-1 protein levels. 16,27
The protein expression of caveolin-1 was upregulated in PTC but downregulated in anaplastic carcinomas. 22 Furthermore, caveolin-1 has been suggested as a negative regulator of carcinoma progression in PTC, and a lack of caveolin-1 expression was linked to the increase in biological aggressiveness. Caveolin-1 expression is higher in epithelial thyroid cells of classical PTC and much more abundant in the tumor stroma. 28 In our study, caveolin-1-positive expression was significantly increased in PTC tissues as revealed by immunohistochemistry staining (χ2 = 15.643, P = .001), in agreement with previous studies. 18,19 Unexpectedly, we found that the solid tissue of BA had higher caveolin-1 expression, whereas solid tumor tissue of PTC had lower caveolin-1 expression, accompanied by downregulation of caveolin-1 expression in para-tumor tissue compared to in normal thyroid tissue as evidenced by Western blot analysis (Figure 2). Therefore, the change in caveolin-1 expression in different thyroid tissues may be like the changes in insulin levels in different phases during the development of type 2 diabetes mellitus. In the early stage of developing thyroid masses, caveolin-1 protects against malignant transformation. We detected a disparity in caveolin-1 expression by immunohistochemistry and Western blotting. This phenomenon has been reported by Paskas et al, 28 but the reason is unclear; the thyroid tissues in the control group were relatively normal, possibly because of the difficulty in acquiring actual normal thyroid tissues from healthy people due to ethical principles in human research. Furthermore, in Western blot analysis, thyroid tissues of the control group consist of thyroid follicular epithelial cells and tissue stroma cells. Thus, the caveolin-1 protein levels detected were not exclusively extracted from thyroid follicular epithelial cells but also from the thyroid stroma.
The caveolin-1 gene is located on human chromosome 7q31.1, and the D7S522 locus on it is commonly deleted in various human cancers, including breast, kidney, prostate, neck, ovary, and colon cancers. The P132L mutant of caveolin-1 can induce cellular transformation and cause upregulation of several signaling pathways, such as those involving endothelial growth factor, hepatocyte growth factor, and mitogen-activated protein kinase, 29 suggesting that caveolin-1 is a tumor suppressor. 20,30,31 In our study, females comprised 75% of all patients. These patients were significantly younger (P = .006) and had higher levels of thyroid autoantibodies, specifically TG-Ab. In 30 patients with PTC, including 26 females and 4 males, nearly 70% of female patients showed positive caveolin-1 expression, while all males were negative. Epidemiological data showed that males were at a higher risk of developing malignant thyroid carcinoma. We found that women had higher thyroid autoimmune antibodies, which can be regarded as a risk factor for developing thyroid tumors, 32 suggesting that women who have thyroid autoimmune antibody positivity were prone to suffer from PTC; however, high thyroid autoimmune antibody titers in PTC were associated with a better prognosis. 33 -35 We propose that some factors related to the female gender may suppress PTC. Although women are more likely to have thyroid problems because of their higher thyroid autoantibody levels, they also have higher caveolin-1 protein expression in PTC, indicating a better prognosis than in men with PTC. Additional long-term observations of these patients are needed to verify this prediction. Moreover, the gender distinction in expression was previously not clear, and further studies are needed.
The thyroid is an endocrine gland. Follicular epithelial cells comprise the thyroid and are the functional and structural units of this gland. Thyrocytes have a polar characteristic. The caveolin-1 protein is found in the apical membrane of normal thyroid follicular cells where it may have an important functional role. For example, caveolin-1 participates in regulating the synthesis of thyroid hormones in human thyroid follicular cells and in the oxidation status of thyrocytes. 36 Loss of caveolin-1 leads to the mislocalization of TPO and dual oxidase and increases intracellular H2O2 production causing oxidative stress, apoptosis, and finally hypothyroidism. The association between the loss of caveolin-1 and development of hypothyroidism has also been demonstrated in Pendred syndrome 37 and Hashimoto thyroiditis. 38 In our study, caveolin-1 protein expression was markedly decreased in hyperactive thyroid function tissue from patients with GD. Furthermore, the prevalence of caveolin-1-positive expression in thyroid follicular epithelial cells was negatively and independently related to the serum TSH level according to multiple stepwise logistic regression, adjusted for gender, age, and other factors (P = .033). Thus, stimulation of isolated human thyrocytes by TSH/cAMP/cAMP-dependent protein kinase inhibits caveolin-1 expression, and TSH may affect caveolin-1 protein expression in thyrocytes by modulating the synthesis of thyroid hormones. 14
Misallocated thyroxisomes lead to the production of thyrocytes displaying intracellular iodination and deficient transport of the thyroid hormone synthesis machinery to the apical membrane in caveolin-1−/− mice. 12 Caveolin-1 protein expression on the apical membrane of thyroid follicular cells may contribute to maintaining cell homeostasis. 39 Decreased caveolin-1 expression may result in thyroid hormone synthesizes in the cytoplasm of thyroid follicular cells rather than classical synthesis sites on the apical membranes. This may induce an aberrant oxidative stress status in thyrocytes. 40 Overproduction of reactive species can promote carcinogenesis via inducing genetic mutations and activating oncogenic pathways. Hallmarks of thyroid physiology, including thyroid hormone synthesis and H2O2 production, are very likely the ultimate cause of frequent mutagenesis in the thyroid gland. In fact, the oxidative burden appears to be a potential starting point for DNA damage and the formation of somatic mutations, particularly in iodine-deficient regions. 41
Patients with GD, Hashimoto thyroiditis, and PTC exhibit increased levels of oxidative stress. Particularly, patients with PTC have higher oxidative profiles compared to those with autoimmune disorders. 36 Oxidative stress can induce caveolin-1 degradation and impair caveolae function in skeletal muscle cells, 42 and upregulation of caveolin-1 can inhibit oxidative stress. 43 Emerging evidence has indicated that caveolin-1-targeted treatments can scavenge reactive species. Thus, caveolin-1 may be a promising oxidative stress-related target for cancer prevention. 44 Multiple clinical studies have verified the critical role of caveolin-1 in cancer prevention. For example, Bertino et al observed that higher caveolin-1 levels in tumor-associated stroma were significantly correlated with improved partial response rates and overall survival in patients with advanced non-small cell lung cancer. 45 Sotgia et al found that a loss of stromal caveolin-1 is a marker of oxidative stress, hypoxia, and autophagy in the tumor microenvironment, 46 explaining the downregulated caveolin-1 expression in hyperthyroidism and thyroid carcinoma in the solid or para-tumor tissues examined in the study.
With the development of research on caveolin-1, this protein has been detected not only in tissues but also in plasma to actively screen for early-stage prostate cancer. 47 Finally, an important finding in our study was increased caveolin-1 expression in thyroid tissue as a protective factor for an injured thyroid, independently of the type of thyroid lesions. Solid tumors of differential thyroid carcinoma downregulated caveolin-1 expression to varying degrees. However, the caveolin-1-positive expression rate was significantly increased in PTC, particularly in female patients, indicating its better prognosis in PTC. Caveolin-1 may play a critical role in affecting cell transformation and regulating thyroid cell function by oxidative stress-related signal pathways. Caveolin-1 is a promising biomarker of PTC, which should be verified in further in-depth studies of its underlying molecular mechanism in the thyroid.
Conclusions
Collectively, the results of our study show that caveolin-1-positive expression in PTC may be a promising biomarker for differentiating PTC from other thyroid nodules. In addition, we found that caveolin-1 is regulated by TSH levels and degraded in GD with hyperthyroidism. Upregulated expression of the caveolin-1 protein may be a protective factor from malignant thyroid tumors. Thus, the increased caveolin-1 protein expression found in female PTC patients may be a good prognostic characteristic.
Footnotes
Acknowledgments
The authors would like to thank all the participants of the studies. The authors are grateful to Longjun Li for her excellent technical assistance. The authors acknowledge support from Dr Hui Lu and Ying Wang in the First Affiliated Hospital of Nanjing Medical University who provided human thyroid tissues used for Western blot analysis.
Author Contributions
J.Y.Z., H.Z., and Y.D.P. contributed to the conception and design of the study. D.X.Y. and Q.Z. performed immunohistochemistry staining on all the specimens and analyzed the pathological results. J.Y.Z and S.W. performed all the other experiments including Western blot. J.Y.Z. and L.P.H. analyzed the data, and J.Y.Z. drafted the manuscript. J.Y.Z. and H.Z. critically revised the article and approved the final version for publishing and the accuracy of the data analysis. Y.D.P. and H.Z. are the guarantor of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.