
Abstract
Objectives:
Asthma and chronic obstructive pulmonary disease (COPD) are chronic illnesses of the airways affecting a good number of people in Lebanon and the Middle East. Pressurized metered-dose inhalers (pMDIs) are important drug delivery systems used to treat such pulmonary diseases. Drugs proven to be valuable and effective may fail to act effectively if such inhalers are used incorrectly. The purpose of this study was to assess the technical use of pMDIs by patients with pulmonary diseases presenting to the community pharmacies in Lebanon.
Methods:
A structured questionnaire was developed to collect data. A total of 601 patients using drugs delivered through pMDIs and presenting to 12 Lebanese community pharmacies were recruited to participate in the research project. The questionnaire items were divided into 3 subscales: subscale 1—assessing the device preparation; subscale 2—investigating the device use; and subscale 3—examining the knowledge and use of spacers. After confirming the reliability and validity of the survey tool, patients’ responses were analyzed and compared according to many variables.
Results:
Many patients answered inaccurately to questions assessing both the device preparation and use. Around 40% of patients said they do not coordinate the inhalation with pressing the canister down. The mean scores were 1.72 (± 0.73) over 6 and 5.67 (± 1.44) over 7 for subscales 1 and 2, respectively. The mean total score on all questions was 7.39 over 13, with a standard deviation of 1.75. While patients’ age did not impact the results, asthmatic, well-educated, male patients had fewer wrong answers when it comes to preparing and using the device (P < .01).
Conclusions:
Our study showed that many patients with asthma and COPD might not be properly using their pMDIs. Appropriate inhaler use is crucial for successful pulmonary disease management. As pMDIs are one of the most difficult devices to use, proper and tailored instructions should be given to patients.
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are both chronic inflammatory disorders of the airways that cause significant morbidity and mortality. 1 -3 Chronic obstructive pulmonary disease is expected to become the third cause of mortality by 2030 according to the World Health Organization with a gradually increasing burden. 4 Similarly, asthma is another major public health concern, affecting 300 million people worldwide. 5
Direct drug delivery and deposition in the airways and lungs is the optimal way to control inflammation in asthma and COPD while minimizing side effects. 6 Pressurized metered-dose inhalers (pMDIs) are commonly used and require critical coordination. 7 They are more difficult to use than dry powder inhalers. 6,8 -12
Despite the progress achieved in inhalation therapy and the continuous evolution of guidelines, many patients still fail to achieve disease control. 13 Efficient pharmacological management not only relies on the physician’s prescription but also on the patient’s adherence and proper inhalation technique. In fact, less than 50% of prescribed asthma medications are administered as indicated. 14 Moreover, up to 90% of patients prescribed an inhaler, use it improperly. 15 This leads to increased morbidity and mortality, as well as increased hospitalization, death, and global cost on the health-care system. 15 -17 Improper techniques include not shaking the inhaler before use, not priming it, not breathing out before actuation of the inhaler, not breathing in while pushing down the canister, failure to hold the breath after inhalation, holding the inhaler with its canister down, not inhaling slowly and deeply and exhaling quickly. 7 Furthermore, old age, 18,19 gender, 20 low education level, 21 disease-specific knowledge, 22 and limited access to primary care 23 were all linked to poor inhaler technique.
It is estimated that 9.7% of the adult Lebanese population have COPD. 24 Similarly, asthma constitutes a major health issue with a national prevalence of 8.3%. 25 However, only few studies have evaluated patient compliance and the proper use of inhaler among the Lebanese patients. Little is known about the medical and sociodemographic factors that impact the outcomes related to treatment adherence and inhaler technique in Middle Eastern population. It is crucial to analyze and understand the issues regarding the use of such devices in order to reveal the difficulties that prevent patients from adhering to medication.
The purpose of this study was to assess, at a selected community pharmacy in Lebanon, using a validated tool, the asthma and COPD patients’ perception of their pMDIs technical use. The effect of patient age, gender, education level, and the perceived disease severity on patient responses was also investigated.
Methods
Setting and Design
A concurrent type of drug use evaluation study was conducted at 12 Lebanese community pharmacies in Beirut and Byblos area over a 3-year period (between 2015 and 2018). Patients, presenting to the community pharmacies, using pMDIs were approached to participate in the research project. A structured questionnaire was used to collect data. The study was approved by the institutional review board of Lebanese American University (LAU), and a waiver of consent was obtained from patients before filling out the questionnaire.
Sources of Data
The questionnaire (Appendix A) comprised 20 questions grouped into 4 categories (patient characteristics; subscale 1; subscale 2; subscale 3): subscale 1 included questions assessing patients perception of the device preparation steps (6 items); subscale 2 included questions assessing patients perception of the device use (5 items); and subscale 3 included questions assessing patients knowledge of the spacer use and its role (3 items).
A score of “1” was allocated if the answer to the question item was correct and “0” if the answer was not correct. Total scores, mean, and standard deviation (SD) were subsequently calculated by item and by subscale.
Statistical Analysis
Patients’ responses were tabulated and cross-tabulated. Data were analyzed using the Statistical Package for Social Sciences (SPSS, version 21, Chicago, Illinois). Cronbach α and factor analysis were performed to examine the reliability and validity of the survey tool. Analysis of variance test was used to assess the effect of age, educational level, and study severity on the subscale scores. T test was used to assess the effect of gender on the scores.
Results
Patient Characteristics
In total, 601 patients across 12 community pharmacies were included in this study. As shown in Table 1, most of the patients in this study were 19 to 30 years old, males, and diagnosed with asthma or COPD 1 to 5 years ago. The most common pulmonary disease was asthma, with a moderate perceived severity of the disease.
Baseline Patient Characteristics.

Abbreviation: COPD, chronic obstructive pulmonary disease.
Survey Tool
The reliability of the survey tool in our population, assessed with Cronbach α, was 0.86 for the total survey score, and 0.94, 0.82, and 0.75 for subscales 1, 2, and 3, respectively.
Table 2 illustrates the patients’ responses to the various items of the questionnaire. Around 24% of patients said they do not prime or shake their inhaler. More than 70% of the patients stated they do not breathe right before the inhalation and do not tilt their head back. Around 8% of patients answered that they do not hold the pMDI right nor close the mouth well around it. Around 40% of patients said they do not coordinate the inhalation with pressing the canister down, and more than 20% inhale quickly and exhale immediately and quickly when done.
Questionnaire Items by Subscale and Patient Answers.

Patients’ answers were also coded, and scores were analyzed by question item and by subscale. The mean scores were 1.72 (± 0.73) over 6 and 5.67 (± 1.44) over 7 for subscales 1 and 2, respectively. The mean total score on all questions was 7.39 over 13 with an SD of 1.75.
As shown in Table 3, age did not impact subscale 1 scores nor subscale 2 significantly (P = .09 and P = .07, respectively). Moreover, patients perceiving the severity of the disease was not correlated with the subscale 1 and 2 scores (P = .304 and P = .266). Males had significantly higher subscale 1 and subscale 2 scores (P < .01). The level of education was significantly associated with higher scores for both subscales (P < .01). Asthma patients scored significantly better on both subscale 1 and subscale 2 when compared to other pulmonary diseases (P < .01).
Mean and SD Scores for Subscales 1 and 2 by Patient Characteristics.
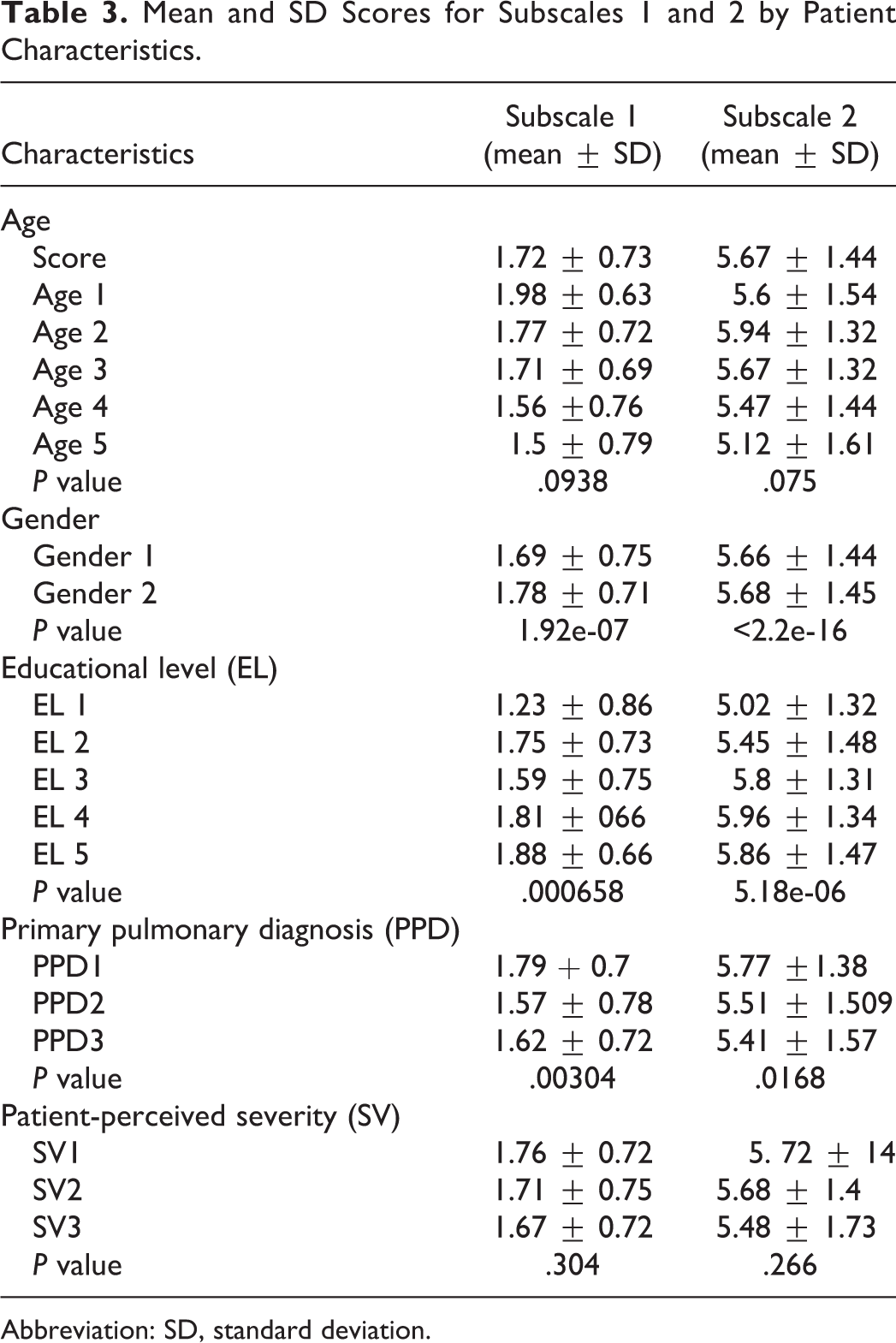
Abbreviation: SD, standard deviation.
Discussion
In this study, many errors were observed concerning the preparation and use of pMDIs. Patients do not all understand how to activate the device well by priming and shaking it. Furthermore, numerous patients say they miss the steps related to the coordination and the slow inhalation.
Individual scores of subscale 1 were low, which shows that most patients might have answered correctly on 1 or 2 questions out of 6 but missed all the other steps. An incomplete preparation of the device might affect the following inhalation steps and thus the dosing and drug exposure.
As for the subscale 2, a significant number of patients’ answers show that they do not correctly perform the crucial steps of coordination, slow inhalation and exhalation, which can dramatically decrease the number of drug particles that would reach the respiratory tract.
In a previous study conducted in Lebanon, patients using pMDIs performed lowest in coordinating between pressing the canister and inhaling. 25
A systematic review of 144 articles from 1975 till 2014 showed that in patients using pMDIs, the most common technical errors were in coordination (45%), inspiration (44%), and holding the breathe before exhaling (46%). 26 The review also found that there was no statistically significant reduction in the incorrect use of inhalers over the past 40 years. 26 This finding is alarming and urgently requires more impactful approaches for patient education.
Age
Our results showed more errors and lower subscale scores in the older age groups. Even though the difference was not statistically significant, the literature does show that older age is associated with higher misuse of inhalers. 10,19,27 -31 Thus, this age group requires special attention during counseling. For example, instructions should be printed in a large font size, oral counseling should be made simple and clear, and the health-care professional (HCP) should confirm and reconfirm steps of the counseling.
Gender
Males answered significantly better than females when it came to both preparing and using the device. One study found that the male gender was a predictor for several correct steps in inhalation technique but not critical ones. 32 This could be explained by the fact that, in general, men have a better hand-to-eye coordination 33 and spatial abilities than women. 34
Educational Level
Similar to most of the published studies, 10,28,30,35 patients with lower educational levels tend to commit more errors while using inhalers. When counseling, patients’ educational level should be assessed, and accordingly, their approach and communication should be customized.
Primary Pulmonary Diagnosis
Patients with asthma seem to perform better when it comes to preparing and using the device. Several studies showed that the inhaler technique does not differ between asthma and COPD patients. 28,36,37 However, a possible explanation could be that COPD patients are usually older, have more comorbidities, and therefore tend to do more errors. 9,12,37
Patient-Perceived Severity
We did not find a statistically significant association between patient-perceived disease severity and the preparation nor the use of the device. Similarly, Amin et al did not find an association between confidence in the correct use of inhaler and COPD severity. 38 Another study found that the severity of dyspnea and lung function impairment, low CAT score, history of frequent exacerbation, being treated by a pulmonologist in the previous 2 years, were not associated with incorrect technique. 35
Spacer-Related Questions
Most of the patients in our study were not aware of the use and the role of the spacer. Spacers or valved holding chambers were developed in the 1950s. 39,40 Their design was improved to address several problems in the use of pMDI, including the poor coordination between actuation, inhalation, and the deposition of large particles in the oropharynx. 41 The latest recommendations for asthma emphasize that spacer devices improve drug delivery, increase lung deposition, and reduce the potential for side effects. 42 There are reports about patients negatively perceiving their use. 43,44 However, HCPs should first introduce them to patients and afterward highlight their role in improving the therapy.
Conclusion
Our study investigated the frequency of errors in pMDIs use. Attributes that were found to influence patient understanding, which HCPs should be aware of include gender, education level, and primary pulmonary diagnosis. As inhalers are integral in the effective management of several pulmonary diseases, it is crucial that patients learn how to use them properly including the addition of spacer devices as required. Health-care professionals should tailor, individualize, and allocate enough time for their counseling. Special attention should be given to particular patient groups such as the elderly. There are several effective tools that can make instructions more impactful such as printed material, videos, and patient support programs. 45 –47 Future studies should focus on individualizing counseling and assessing which interventions are the most impactful by the patient group.
Limitations of the Study
A major limitation of the study is that it assessed patients’ understanding of correct pMDI use and technique, rather than their actual use and technique. As such, the results do not directly relate to clinical use. Future studies could include observational assessments of the pMDI technique to evaluate whether understanding translates to actual use. In our study, we did not assess whether proper education was provided to the patients or not; this should be taken into consideration in future studies. Finally, asthma or COPD diagnosis was solely based on patients’ answers.
Footnotes
Appendix A

| MDI Questionnaire | ||
|---|---|---|
| Baseline Patient Characteristics | ||
| Age | Gender | Time of Diagnosis |
| 1. 10-18 years | 1. Female | 1. <1 month |
| 2. 19-30 years | 2. Male | 2. 1 month to 1 year |
| 3. 31-40 years | 3. 1-5 years | |
| 4. 41-60 years | 4. 6-10 years | |
| 5. >60 years | 5. >10 years | |
| Educational level | Primary pulmonary diagnosis | Patient-perceived severity of pulmonary disease |
| 1. No school | 1.Asthma | 1.Mild |
| 2. High school graduate or less | 2. COPD | 2. Moderate |
| 3. Some college | 3. Other pulmonary disease | 3. Severe |
| 4. College graduate | ||
| 5. Postgraduate studies | ||
| Subscale 1: preparation of the device | ||
| If you are using a new inhaler, do you prime it? | Before using your inhaler, do you shake it? | How do you breathe just before using your inhaler? |
| 0. No | 0. No | 1. Inhale |
| 1. Yes | 1. Yes | 2. Exhale |
| 3. Breathe in and out | ||
| How do you tilt your head while using your inhaler? | How do you hold your inhaler while using it? | How do you position the mouthpiece? |
| 1. Tilt head forward | 1. Upright (canister up) | 1. In your mouth (lips around it) |
| 2. Keep head level | 2. Down (canister down) | 2. 1-2 inches from your lips with mouth open |
| 3. Tilt head backward | ||
| Subscale 2: use of the device | ||
| When pushing down the canister for a dose, when do you take a breath? | How do you inhale while taking the dose? | How do you breathe after taking the dose? |
| 1. Begin to breathe in a while pushing down the canister and continue breathing in | 1. Inhale slowly and deeply | 1. Breath out immediately |
| 2. Push down the canister then take a breath | 2. Inhale quickly | 2. Hold your breath for about 5 to 10 seconds before exhaling |
| 3. Take a breath then push down the canister | ||
| How do you exhale after inhaling the medicine? | If your directions are to take “2 puffs” for your dose, how do you manage? | |
| 1. Exhale slowly | 1. Push down the canister twice while taking a breath | |
| 2. Exhale quickly | 2. Push down the canister once then wait about a minute before doing it again | |
| 3. Push down the canister once then push it down again for the very next breath | ||
| Spacer-related questions | ||
| Do you use a spacer with your metered dose inhaler? | Do you know about the role of a spacer? | Do you prefer (or think you need) using a spacer? |
| 0. No | 0. No | 0. No |
| 1. Yes | 1. Yes | 1. Yes |
Abbreviation: COPD, chronic obstructive pulmonary disease.
Authors’ Note
Wijdan Ramadan and Aline Milane designed, initiated the research, collected data, wrote a part of the manuscript, analyzed the study results, and reviewed the completed manuscript. Aline Sarkis and Sandrine Sarine entered the data into the SPSS, analyzed the study results, and wrote a part of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.