
Abstract
Introduction:
Asthma is a serious allergic disorder of the respiratory system. It affects about 300 million people worldwide. This has a great burden on medical treatment. Several medicines are available, but they have many serious side effects. Therefore, there is a need to search for a new therapeutic agent with no or minimal side effects while most economical for patients. In folk medicine, antiasthmatics herbal medicine has been used and showed potential therapeutic antiasthmatic efficacy due to the presence of potential bioactive compounds.
Methods:
Different databases were searched (ie, Embase, PubMed, CBM, AMED, and CINAHL). We have reviewed the published data of the last 20 years. We used MeSH terms “asthma” herbal treatment of asthma, allopathic treatment of asthma, and treatment strategies for asthma. The traditional medicine was compared with modern medicine and the same pharmacotherapies alone or with placebo. The methodology was evaluated by using the GRADE summary of Finding tables and Cochrane Risk of Bias Tool.
Results:
There have been some clear-cut indications toward the recognition of further molecular and cellular mechanisms of asthma. Most of them recommend a further target for treatment. The novel procedures, biologics, and pharmaceuticals are evaluated. Both allopathic and herbal treatments of asthma are effective. Due to none or lesser side effects, herbal medicines are safer than conventional medicine.
Conclusion:
The preliminary documentation of the plants discussed in the review show the presence of several secondary metabolites that are responsible for the management of asthma and its relevant complications. Further research studies are needed to identify the bioactive compounds from these plants that have potential efficacy to cure asthma, and clinically based studies are needed to search for a complete cure for this disease.
Introduction
Bronchial asthma is a paroxysmal attack of breathlessness, chest tightness, and wheezing resulting from paroxysmal narrowing of the bronchial airways. Asthma is characterized by inflammation, obstruction, and hyper-responsiveness of the airway. Patients cough more during sleep and when awake in the morning. Asthma affects 10% of the population. Epidemiology will help us to study prevalence, morbidity, and mortality rate of asthma. About 235 million people worldwide have been affected. Many people die from this deadly disease due to its high prevalence rate in many countries. Number of patients has been increasing day by day. Millions of people have died from asthma. The highest incidence is in New Zealand, Australia, and the United Kingdom, and the lowest incidence rate is in China and Malaysia. About 7% of adults and 15% of children have asthma. 1
Types of Asthma
Allergic Asthma
Allergic asthma is a disorder that it occurs due to airborne substances. It mostly affects children due to environmental factors because children play in a dirty environment and inhale in a dusty environment. 2
Nonallergic Asthma
Nonallergic asthma occurs in adults older than 35 years and in individuals with no previous allergic histories. It mainly sheds an epithelial layer in the lungs, causing thickening of the overlying basement membranes, hypertrophy of bronchial smooth muscle, hyperplasia of lungs muscle due to allergy, and vascularization of neurons. 3
Allergic Bronchopulmonary Mycosis
It is caused by an exaggerated immune response to the fungus Aspergillus. 4
Aspirin-Induced Asthma
It is caused by overuse of nonsteroidal anti-inflammatory drugs such as aspirin. 5
Exercise-Induced Asthma
Strenuous exercise exerts pressure on lungs, and dust deposits on the lungs and causes narrowing of the airways. Bronchial muscles change due to environmental humidity and temperature. 6
Cough-Variant Asthma
It is a type of cough that is not productive, and mucous does not come out from the lungs but deposits in lungs which makes it thicker and causes difficulty in breathing.
Occupational Asthma
It is a disorder that occurs while at work when medical professional dealing with patients inhale allergens; it induces allergic reactions. 7
Nocturnal Asthma
It occurs during sleep; when the person lies down, the nasal secretions start to accumulate in the lungs and cause breathing to be harder. 8
Classification of nocturnal asthma
Intermittent Asthma: Symptoms of intermittent asthma occurs 2 days per week or less. It is rare to wake up at night.
Persistent Mild: It has symptoms more than twice a week but not every day. In this, the patient occasionally wakes up at night.
Persistent Moderate: It has symptoms every day. Kids and adults wake up at least once a week.
Pathology of Allergic Asthma
Asthma is an allergic disease. B cells are important immunological cells in the body which recognize specific antigen cells and produce immunoglobulin E (IgE) in response. It also helps in the production of dependent mast cells, basophils, leukotrienes, and cytokines. B cells in airways act as foreign detectors to detect allergens for endocytosis which comes from airborne substances and present it to the T cells. Respiratory epithelium is activated by the environmental and inflammatory mediators and release lymphopoietin from stromal cells of thymic tissues in airways and inflammatory mediators and attracts leukocytes and recruits more leukocytes to skew dendritic cells toward allergic reaction. These dendritic cells cause differentiation of T cells into T helper cells as well as type II cells. These T cells induce production of IgE antibody from B cells by stimulation of interleukin (IL) mediators. Immunoglobulin binds to receptors on B cells and releases cytokines and basophils from mast cells in the presence of allergens that block the receptors and cause bronchoconstriction and enhance inflammatory response. Production of IL and T cells raise eosinophil levels in the body. Inflammatory mediators release from eosinophils, macrophages, neutrophils, and T cells resulting in damage or destruction of airways and cause bronchoconstriction and stimulate airways epithelium to release more inflammatory mediators. The role is played by cytokines, basophils, eosinophils, T cells, antigen presenting cells (APCs), chemokines, macrophages, neutrophils, stem cells, necrotic factors, epithelial cells, IL-4, IL-5, IL-13, prostaglandin, colony-stimulating factors and ligands, and so on. 9 We have to determine how environmental factors activate Blimp-1 and how Blimp-1 causes T cells to drive allergic asthma.
Defective receptors
B-receptors are found in the lungs and have an agonist effect as a bronchodilator.
Autoimmune receptors
Autoimmune nerve influences airway tone by activating specific receptors on airways smooth muscle. Cholinergic receptor stimulation occurs as a result of acetylcholine release from postganglionic cells.
A considerable number of patients with asthma have a history of additional allergic disorders and elevated level of immunoglobulin. In the earliest part of the 20th century, the allergic theory was considered as the major cause of asthma. 10 Nervous system theory explains that cases with asthma have defective β-receptors, which cause an imbalance between sympathetic and parasympathetic nerves. The imbalance overstimulates the parasympathetic nerves, leading to bronchial constriction. 11 Gene theory explains that patients with asthma get asthma genes from parents. The patient with asthma invariably has asthmatic parents or grandparents. There seems to be a genetic predisposition to asthma. 12 The viral theory explains that respiratory infections especially viral infections often precipitate bronchial asthma. The initial event seems to be the epithelial damage and airway wall inflammation. Viral infection in asthmatic genetic diathesis can be devastating, since viral infections can attack and damage β-receptors and may cause wheezing for a long period. If β-receptors are damaged permanently, then asthma may last for months and years. 13 Mast cell theory explains that millions of mast cells line up on the skin, nose, bronchial tree, and intestines. Mast cells contain leukotrienes and histamines. When any antigen from outside enters the respiratory tract and encounters the IgE antibodies, the mast cells liberate chemicals in the respiratory tract and cause tissue inflammation and swelling. In the nose, mast cells cause sneezing, asthma in the lungs, and itching in skin. 14,15 Inflammation plays an important role in the pathogenesis of asthma.
In an immediate response, usually, allergens are involved. Response occurs within 15 minutes to 1 hour of allergen exposure. Activation of mast cells causes the release of chemical mediators that are involved in inflammatory reactions and manifestations of asthma. Late-phase response occurs after 4 to 6 hours of allergen exposure. In this phase, neutrophils and eosinophils are involved that release chemical mediators resulting in the inflammatory response and symptoms formation.
Various allopathic medicines are available that are used to treat asthma, but they have side effects. 16 Salbutamol and theophylline are effective in the treatment of the early phase inflammation in patients with asthma. Anti-inflammatory drugs and cromolyn sodium are effective in the late phase of inflammation. Early-onset asthma occurs in patients with atopy and in children. Patients with atopy form IgE antibodies against fungal spores, animal dander, feathers, house dust, pollen, and ingested allergen obtained from wheat, yeast, milk, eggs, and fish. Allergic diseases including eczema and allergic rhinitis are usually present. In this type of asthma, certain mediators are released that produces mucus hypersecretion, mucosal swelling, and muscle spasm. Late-onset asthma usually occurs in adults. The autonomic nervous system controls the bronchial secretion and bronchial smooth muscles. Bronchoconstriction occurs due to adrenergic and cholinergic stimulation, while relaxation occurs because of β-adrenergic stimulation. Aspirin, emotion, pollution, and cold stimulate α-adrenergic and cholinergic system causing bronchial constriction and enhancing the mucus secretion. The term atopy is employed to describe people who rapidly develop IgE antibodies against the foreign antigen. The allergen enters the bronchi with the inspired air. The antigen–antibody reaction in the bronchi causes the release of biochemical mediators that are involved in the bronchial constriction. T-lymphocytes, macrophages, neutrophils, and eosinophils are also involved in the inflammatory reactions. Airways hyperactivity to the nonspecific stimuli has been observed in the tracheobronchial tree of people with asthma. The abnormalities may occur in the nerves in such a way that stimulation of parasympathetic system and deficiency of sympathetic system occurred causing hyperactivity to result in constriction of bronchi. Bronchial reactivity can be checked by asking the people to inhale histamine methacholine (bronchial provocation test). It causes a transient episode of narrowing of the airway to susceptible people. The precipitating factors are sudden climatic change, use of medicines such as β-blockers and nonsteroidal anti-inflammatory drugs, atmospheric pollution, tobacco smoke, dust, emotional stress, respiratory viral infection, and exercise. In this inflammatory disorder, several well-known hereditary components and cells such as mast cells, lymphocytes, and eosinophils are involved. Airway inflammation leads to airway edema and hyperactivity resulting in reversible bronchoconstriction. If left untreated, the inflammatory changes may eventually become chronic and irreversible, a process termed airway remodeling. From both laboratory and epidemiological studies, a protective role for infection against the subsequent development of asthma has been established. 17
In comparison to the allopathic treatment of asthma, herbs provide additional effects, and these are used as important regimens in certain areas. Some of the medicines are evidence based and have been prescribed in clinical practice. 18,19 Various researchers are doing experimental studies on herbal medicine and recommending these drugs for clinical practice. In this review, an effort has been made to document the mechanism of action of some medicinal plants (Table 1). Various comparative studies are being conducted all over the world.
Mechanism of Action of Antiasthmatic Plants.
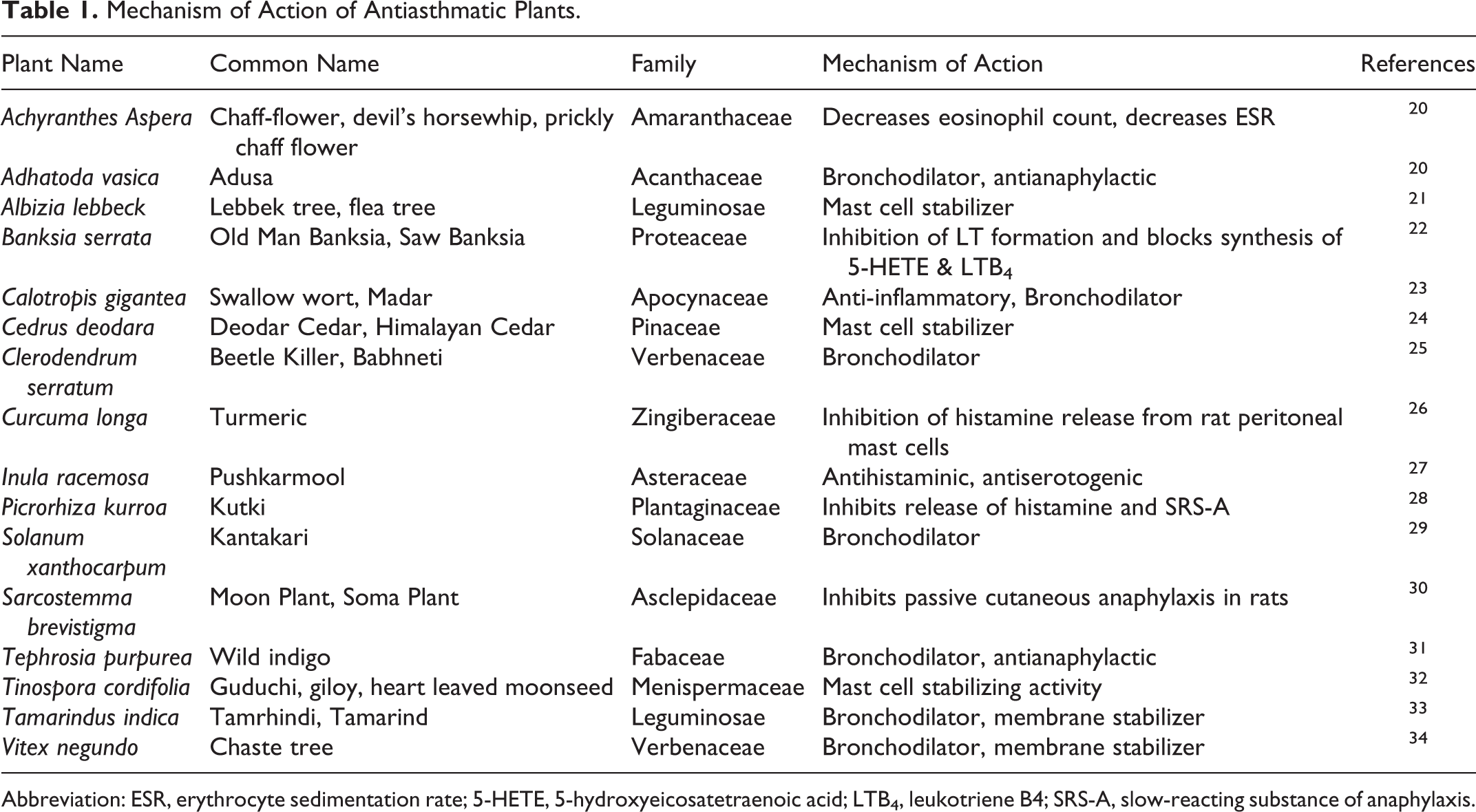
Abbreviation: ESR, erythrocyte sedimentation rate; 5-HETE, 5-hydroxyeicosatetraenoic acid; LTB4, leukotriene B4; SRS-A, slow-reacting substance of anaphylaxis.
This review focuses on novel and promising conventional treatment of asthma. In this review, preliminary documentation of these plants showed the presence of several secondary metabolites that are responsible for the management of asthma and its relevant complication. In this review, we explained the pharmacological properties of plants and demonstrated its importance for the treatment of the asthmatic problems.
Severe Asthma and Its Mechanism
Nowadays, most of the cases with asthma were considered similar but differ only on the basis of disease severity. Therefore, the treatment of patients with asthma requires difference in dose, route of intake or frequency of taking the β2-adrenoceptor agonist, and corticosteroids that are essential to manage asthma disease. 35 However, asthma subphenotypes identification has challenged this view in modern medicinal system. Since past 2 decades, research has identified the fundamental source of asthma is the allergic pathways and a prominent role of T-cells designated as Th2-like producing cytokines and chemokines involved in IgE regulation, maturation, recruitment, priming, and white cells activation including basophils, mast cells, and neutrophils. Allergic pathways contributing the dysfunction of airways in mild-to-moderate asthma are mainly corticosteroid sensitive. Nonetheless, the profile of inflammatory process changes frequently with larger contribution of neutrophils, airway remodeling, and substantial tissue devastation in patients with more severe asthma (Figure 1). 37,38 In patients with severe asthma, the airways show features of chronic wound as an indication of enduring epithelial injury and repair. 39 Necessary stimuli are created in response to any injurious wound to recruit the primary mesenchyme for participation in repair process by releasing certain growth factors such as vascular endothelial growth factors, heparin-binding like growth factor, epidermal growth factor (EGF), amphiregulin, insulin-like growth factors, fibroblast growth factors, keratinocyte growth factor, transforming growth factor (TGF)-β, and TGFα, which in combination promote vasculogenesis and remodeling. 40 Reduced antioxidant defenses and overexpression of EGF receptors are the characteristics of injury and stress displayed by airway epithelium. 41,42 Derangement of epithelial function and mesenchymal response augmentation emphasize the likely responsibility of epithelial–mesenchymal trophic unit which is linked with the lung development and disease remodeling and chronicity (Figure 1). 43,44 This process includes augmented matrix deposition in the subendothelial lamina reticularis of basement membrane, deposition of types 1, 3, 5, and 6 repair collagens, and disruption of elastin filaments and proteoglycans all the way through airway wall resulting in stiffer and thickened airways. 45,46 In severe asthma, the smooth muscle spiral bundles are increased both in size and in number and spread upward affecting the larger airways, alveolar ducts, and respiratory bronchioles. 47 The ability of recruitment, retainment, and activation of selective cells responsible for inflammation such as neutrophils, mast cells, and monocytes changes within this microenvironment. Consequently, regardless of high dose intake of oral corticosteroids, the mast cells may increase in number or persist, particularly those close to or within the smooth muscle bundles of the airway with most of the cells containing increased tumor necrosis factor α (TNFα). 48 The TNFα is raised in airway biopsies at messenger RNA level and in bronchoalveolar lavage fluid. 49 Mast cells are also vital source of cytokines such as IL-13 with driving potential for both the inflammatory and the remodeling processes.

Responses during inflammation and remodeling process in asthma activating the epithelial–mesenchymal trophic unit. Communication set point between bronchial epithelium and underlying mesenchymal cells alters by the epithelial damage, resulting in the activation of myofibroblasts with raised mesenchymal volume and induction of structural changes throughout the airway wall. (Adapted from Holgate and Polosa). 36
Results
Allopathic Treatment
The 2 major features of bronchial asthma include bronchoconstriction and inflammation; thus, the allopathic drugs are used to prevent or reverse the bronchoconstriction and decrease the inflammation via a different mechanism (Figure 2). Smooth muscles of the bronchial tree mainly contain β2 receptors, stimulation of which causes bronchodilation. All those sympathomimetic that cause stimulation of β2 adrenoceptors are useful in the treatment of bronchial asthma, especially those acting mainly on β2 receptors. Sympathomimetic are epinephrine, ephedrine, isoproterenol, albuterol, levalbuterol, bitolterol, metaproterenol, terbutaline, ritodrine, procaterol, isoetarine, formoterol, pirbuterol, and salmeterol. 50 Adrenaline is available as injection and inhaler. The 0.3 to 0.5 mL of 1:1000 solutions can be used subcutaneously for asthma, which can be repeated after 15 to 20 minutes. It is mostly metabolized in the body, and metabolites are excreted in the urine. Adrenaline is metabolized in the body by 2 enzymes, monoamine oxidase and catechol-o-methyl transferase. It produces bronchodilation by stimulating β2 adrenoceptors on the smooth muscles of the bronchial tree. It is avoided in elderly individuals, ischemic heart disease, cardiac arrhythmias, and hypertension. 51 Albuterol can be used orally, by injection, or by inhalation. When given orally, its absorption is good from gastrointestinal tract (GIT). Bronchodilation occurs in about 1 hour and remains for 6 to 8 hours. When used by inhalation it acts in about 15 minutes and remains effective for 3 to 4 hours. By subcutaneous injection, its effects occur in 5 minutes and last for 3 to 4 hours. 52 Tiotropium is a long-acting antimuscarinic drug. It is especially effective in cases of the chronic obstructive pulmonary disease. It also decreases the acute exacerbation in patients with chronic obstructive pulmonary disease. 53 Methyl xanthine drugs are theophylline, aminophylline, theobromine, caffeine, oxtriphylline, dyphylline, pentoxifylline, and acefylline. Aminophylline is prescribed to patients who develop paradoxical abdominal and diaphragmatic fatigue. Aminophylline infusion is effective in improving diaphragmatic contractility. 54 Mast cell stabilizers are cromolyn sodium, nedocromil Na, and ketotifen. These important anti-inflammatory drugs prevent activation of many inflammatory cells, particularly mast cells, eosinophils, and epithelial cells. These agents have no direct bronchodilator activity. Therefore, they are not effective in relieving acute symptoms of asthma. They are effective in mild persistent asthma, particularly when exercise is a precipitating factor. Cromolyn sodium is derived from an Egyptian plant called khellin. It inhibits the release of chemicals from mast cells and therefore prevents all phases of asthmatic attack. It is used 3 to 4 times a day. The drug in powder form can be inhaled and has been developed as 1% Intel solution which is used in the nebulized device and now is available in Intel pocket inhalers. 55 Corticosteroids are triamcinolone, prednisone, mometasone, methylprednisolone, hydrocortisone, fluticasone, flunisolide, dexamethasone, budesonide, and beclomethasone. Corticosteroids are the most effective and constantly successful anti-inflammatory drugs. Corticosteroids reduce inflammation resulting in control of asthma manifestations and prevention of asthma exacerbation. 56 Side effects observed by long use of corticosteroids are an adrenal failure, delay in wound healing, weight gain, osteoporosis, cataract, and growth retardation in children. 57 Cortisone inhalers give local relief in asthma with minimum side effects. Cortisones are effective in asthma and persistent, abnormal breathing. Cortisone inhalers cause hoarseness and oral thrush which can be minimized by mouthwash and use of myostatin locally. 58 The 5-lipoxygenase inhibitor is zileuton, and leukotriene D4 (LTD4)-receptor antagonists are zafirlukast and montelukast. Leukotrienes receptor antagonists are the novel group of medicines for the treatment of asthma. Leukotrienes induce asthma manifestations and airway obstruction by contracting smooth muscle cells, attracting inflammatory cells, and enhancing mucus secretion and vascular permeability. 59
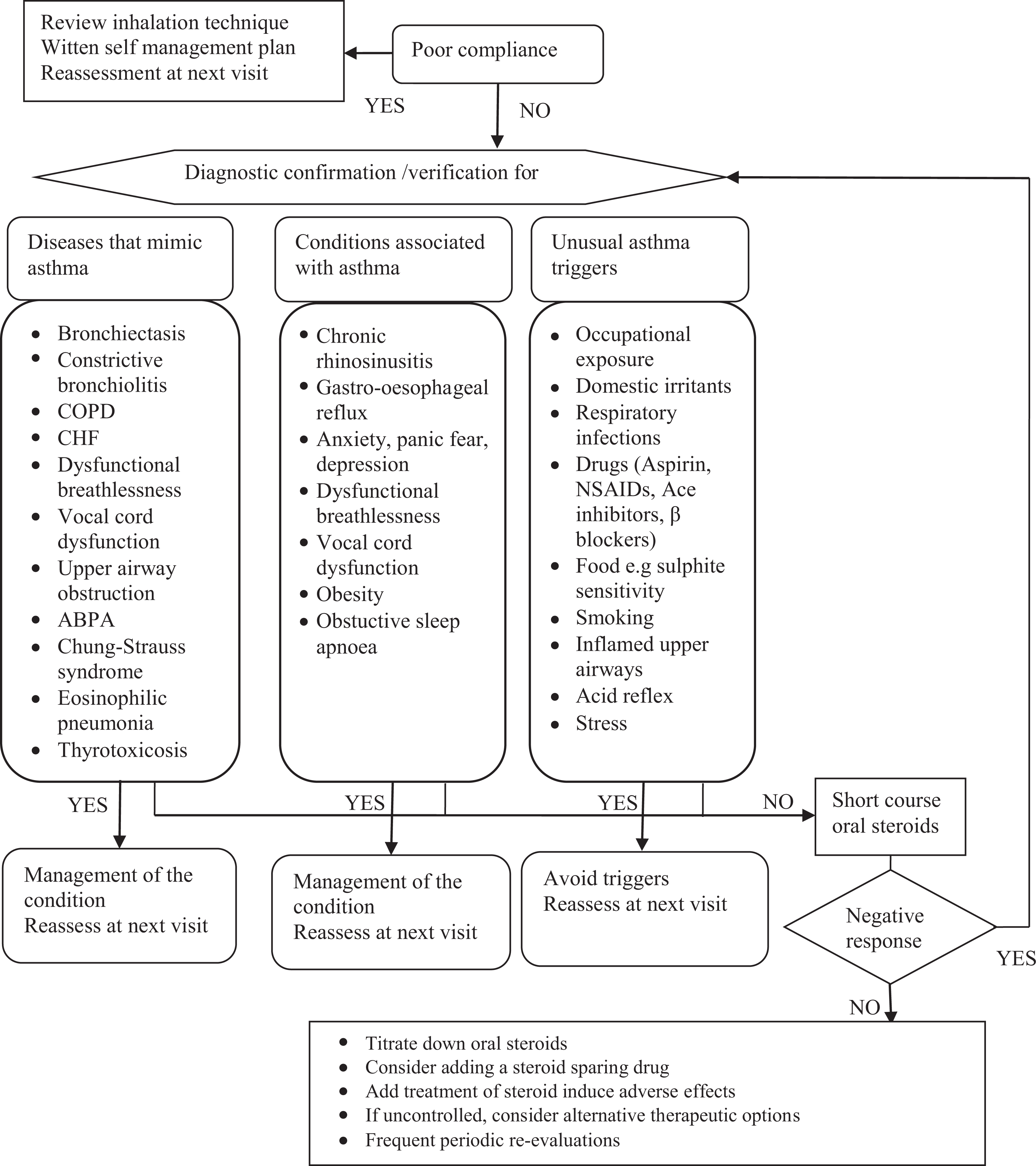
Possible algorithmic strategies and recommendations for managing patients with difficult to control asthma, despite maximum combination treatment. CS indicates cystic fibrosis; COPD, chronic obstructive pulmonary disease; CHF, chronic heart failure, ABPA, allergic bronchopulmonary aspergillosis; NSAIDs, nonsteroidal anti-inflammatory drugs. 36
Herbal Treatment
Adhatoda vasica Linn
Adhatoda vasica Linn belongs to family Acanthaceae. Parts used are roots, leaves, flowers, and barks. Chemical constituents include vasicinol, vaccine, adhatodic acid, salts, alkaloids, essential oil, volatile odorous principle, salts, and pyroquinazoline alkaloids. 60 It is used in tuberculosis, asthma, and sore throat. 61 It is an expectorant, bronchodilator, and antibacterial. 62 Gupta et al reported the antiasthmatic activity of different formulations of Adhatoda vasica. 63
Asystasia gangetica
Asystasia gangetica belongs to family Acanthaceae. Parts used are roots and leaves. It is used in asthma, wound healing, and cardiovascular disorders. 64 It is antiasthmatic and antihypertensive. 65 Akah et al reported the antiasthmatic property of A gangetica leaf extract. This plant is used in the management of asthma in various countries. A study was conducted to investigate its efficacy as an antiasthmatic drug. Methanol, ethyl acetate, and hexane extract of A gangetica were used for the study. The extract was able to inhibit the contraction induced by spasmogens. Histamine-precontracted tracheal strips were relaxed by the use of extract. The most active extract was ethyl acetate. This study indicated that A gangetica is effective in asthma. 66
Clitoria ternatea L
Clitoria ternatea L. belongs to family Fabaceae. Parts used are roots. Its chemical constituents are glycosides, saponins, and flavonoids. 67 It is used to treat constipation, intestinal worm, and diabetes mellitus. 68 It is antiasthmatic, hypoglycemic, antioxidant, antihyperlipidemic, memory enhancer, immunostimulant, and antibacterial. 69 The antiasthmatic activity of C ternatea L. roots has been reported. A study was conducted to investigate the efficacy of C ternatea L. in the treatment of asthma. Ethanolic extract of this plant was used for the study. Rats and mice were selected for the study. Mast cells degranulation was induced by egg albumin in rats. Eosinophilia and leukocytosis were induced by milk. The dose of the extract was 100 to 150 mg/kg administered intraperitoneally. Leukocytosis, eosinophilia, and mast cell degranulation were reduced significantly. This study indicated that this plant has antiasthmatic activity due to the presence of flavonoids or saponins. 70
Curculigo orchioides Gaertn
Curculigo orchioides Gartn belongs to family Hypoxidaceae. Part used is root. Derivatives of this plant are used in asthma and Alzheimer disease. 71 It is antiasthmatic, antiosteoporotic, and immunostimulant. 72 The antiasthmatic activity of C orchioides has been reported. Ethanol extract of this plant was used for the study. Antiasthmatic activity has been investigated in vivo and in vitro. Animal models were used for the study. Mechanism of action of the extract was investigated in isolated goat tracheal chain preparation and isolated guinea pig ileum preparation. This in vitro study indicated that extract has muscle relaxant activity. Furthermore, its antihistamine-induced contraction has been reported. Maximum muscle relaxant effect was observed at a dose of 100 μg/mL in isolated goat tracheal chain preparation. The extract exhibited maximum muscle relaxant activity at a dose of 25 µg/mL in ileum preparation isolated from the guinea pig. Bronchospasm was induced by histamine in guinea pigs. After treatment with the extract of this plant, there was an increase in leukocytes and reduction in eosinophils that indicates its efficacy in asthma. 73 Venkatesh et al. investigated mast cell stabilizing on isolated mice peritoneal mast cells and stated that plant has mast cell stabilizing activity and antihistamine activity. 74
Elephantopus scaber
Elephantopus scaber L. belongs to family Asteraceae. Parts used are roots and whole plant. Chemical constituents include steroids, saponin, flavonoids, and phenolic compounds. It is used to treat cough, malaria, and cancer. 75 It is anti-inflammatory. 76 The antiasthmatic activity of ethanolic extract of E scaber L. leaves has been reported. Ethanol extract of this plant was used for the study. Leaves of this plant were used for study purpose. Different dose levels of the extract were used. Bronchospasm was induced by histamine and acetylcholine. Isolated guinea pig tracheal chain was chosen for study. There was a significant reduction in bronchospasm in the test group when compared to control. This effect was dose dependent. This efficacy of plant is due to flavonoids. 77
Ficus religiosa L
Ficus religiosa L. belongs to the family Moraceae. Parts used are bark and seeds. It is used in gonorrhea, scabies, and herpes infection. 78 It is anticonvulsant, anti-inflammatory, and anti-parkinsonism. 79 Kapoor et al reported the antiasthmatic activity of F religiosa leaves (150 and 300 mg/kg) in guinea pigs. Bronchospasm was produced by administration of acetylcholine and histamine. This study was done in comparison to aminophylline. Aqueous extract of the plant was introduced to guinea pig. Aminophylline was administered at a dose of 25 mg/kg. Furthermore, aqueous extract of the plant was investigated in comparison to ketotifen. Dose of extract was 10, 20, and 30 g/mL. There was a delay in the onset of histamine-induced preconvulsive dyspnea when compared to vehicle control. When an aqueous extract of the plant was administered at the dose of 150 and 300 mg/kg intraperitoneally, there was a significant effect on latency to develop histamine and acetylcholine-induced preconvulsive dyspnea. In in vitro studies, the number of intact cells increased in the mast cell stabilizing model at the dose of 10, 20, and 30 µg/mL. 80
Hyssopus officinalis
Hyssopus officinalis belongs to family Lamiaceae. Parts used are flowers and leaves. Active ingredients include flavonoids, glycosides, tannin, resin, essential oil, fats, sugar, mucilage, isopinocamphone, limonene, and β-pinene. 81 It is an antioxidant, 82 stimulant, and smooth muscle relaxant. 83 Wang et al reported the efficacy of H officinalis in asthma and explored the mechanism of action in asthma. Rats were selected for the study. Water extract of H officinalis was administered. Extract affected differentiation of Th1, Th2, and Th17 on transcription level and played an important role as an antiasthmatic agent.
Hypericum perforatum Linn
Hypericum perforatum Linn belongs to family Hypericaceae. Parts used are leaves, buds, and flowers. Chemical constituents include essential oil, glycoside hyperin, hyperforin, and other florescent chemicals. 84 It decreases LDL cholesterol and reduces oxidative stress. 85 It is an antidepressant, antiasthmatic, and neuroprotective. 69 Khan et al reported the calcium channel blocking activity of H perforatum. 86
Nigella sativa
Nigella sativa belongs to family Ranunculaceae. Parts used are seeds. Melanthin, nigellin, nigellone, carvone,
Picrorhiza kurroa
Picrorhiza kurroa belongs to family Plantaginaceae. Part used is rhizome. Its active compounds are iridoid glucoside, phenolic, flavonoids, and cucurbitacins. 92 It is used in jaundice, asthma, and arthritis. 92 It is hepatoprotective, antiasthmatic, anti-inflammatory, and anticancer in nature. 93 The antiasthmatic effect of P kurroa has been reported. It is prescribed to treat liver and lung diseases. An active compound androsin has been isolated from this plant. Androsin was found effective against bronchial obstruction induced by allergen and platelet-activating factor. 94
Spinacia oleracea Linn
Spinacia oleracea Linn belongs to family Amaranthaceae. Parts used are leaves. Chemical constituents include iodine, lecithin, chlorophyll, carolin, oxalic acid, saponin, and flavonoids. 56 It is used in cardiovascular disorders, obesity, and cancer. 95 It is an antioxidant. 96 Heo et al reported the antiasthmatic activity of S oleracea Linn (SoL). Aqueous extract of SoL was used for study in mice. Asthma was induced by albumin. The extract was administered orally to those mice that were sensitized to ovalbumin. Hematoxylin and eosin staining was used to examine lungs for IL-4/13 cytokine expression. The extract exhibited antiasthmatic activity that is evident from the reduction in the CD4+ cell number and IL-4/13 in the lung. This study indicated that extract has an antiasthmatic activity that is evident in a mouse ovalbumin-challenge model. 97
Discussion
The present approach to treat asthma is mostly based on the use of corticosteroids and inhaled bronchodilators. 98 For a majority of individuals, these therapies are efficient at humanizing function of lung and life quality and decreasing manifestations and disease exacerbations. 99 Apprehension exists concerning the adverse reactions of these therapies in some individuals, particularly when prescribed in high dose. 100 Additionally, there is increasing identification of subgroups of individuals who emerge refractory to existing treatment and who are thought “complex to manage.” At present, new and costly biologic treatments are being emerged to tackle this unmet requirement. Traditional medicines to tackle the concern of adverse reactions and decrease the effectiveness comprises of the application of phytomedicine. 101 However, development in this vicinity is vulnerable by the deficiency of convincing proof. Therefore, there is a necessity for an appropriately carried out controlled study on safe medicine derived from plants. The articles included in this article are mostly comprised of in vitro trials, which indicate that most scientists or researchers consider traditional medicines as effective treatment for different ailments rather than holistic or homeopathic medicines.
Conclusion
The medicinal plants and their extracts possess significant antiasthmatic activities. This article provides up-to-date information regarding patients with asthma and potential medicinal plants having antiasthmatic activity. The medicinal plants have confirmed effectiveness as antiasthmatic agent on a scientific base. The method of action of many medicinal plants has been recognized. This review emphasizes randomized clinical studies using traditional medicines for the management of asthma. Additional research is necessary to determine the bioactivity of additional compounds in simple extracts and to explore their bioactivity as antiasthmatic agents. Thence, novel and effective drugs can be developed by way of detailed investigation of the properties of various constituents.
Footnotes
Authors’ Note
Authors have agreed for publication. Muhammad Daniyal is now affiliated with Faculty of Eastern Medicine, Hamdard University Karachi-Pakistan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.