
Abstract
The US Environmental Protection Agency (USEPA) is the primary federal agency responsible for promulgating regulations and policies to protect people and the environment from ionizing radiation. Currently, the USEPA uses the linear no-threshold (LNT) model to estimate cancer risks and determine cleanup levels in radiologically contaminated environments. The LNT model implies that there is no safe dose of ionizing radiation; however, adverse effects from low dose, low-dose rate (LDDR) exposures are not detectable. This article (1) provides the scientific basis for discontinuing use of the LNT model in LDDR radiation environments, (2) shows that there is no scientific consensus for using the LNT model, (3) identifies USEPA reliance on outdated scientific information, and (4) identifies regulatory reliance on incomplete evaluations of recent data contradicting the LNT. It is the time to reconsider the use of the LNT model in LDDR radiation environments. Incorporating the latest science into the regulatory process for risk assessment will (1) ensure science remains the foundation for decision making, (2) reduce unnecessary burdens of costly cleanups, (3) educate the public on the real effects of LDDR radiation exposures, and (4) harmonize government policies with the rest of the radiation scientific community.
Introduction
The US Environmental Protection Agency (USEPA) was established in 1970 and gained authority to promulgate environmental standards to limit man-made radioactive materials in the environment and develop national radiation protection guidance for Federal and State agencies. 1 Congress enacted several statutes providing USEPA the authority to regulate hazardous materials (eg, Clean Air Act, Safe Drinking Water Act, and the Comprehensive Environmental Response Compensation and Liability Act), including both chemical and radiological hazards. 2 Among many federal programs whose regulatory authorities were transferred to the USEPA, the Public Health Service Act (PHSA) authorities are of particular interest in this article. The PHSA authorities give the USEPA the ability to conduct monitoring of environmental radiation, perform research on the environmental and human health effects of exposure to radiation, and provide technical assistance to states and other federal agencies. These authorities are consistent with the mission of the USEPA to protect human health and the environment.
This article examines the radiation protection framework and policies of the USEPA as they are applied to low-dose, low-dose rate (LDDR) radiation exposures. It focuses on current scientific literature, policy implications, public health impacts, and future directions for developing a radiation protection framework based on sound scientific principles.
In this article, we refer to dose in Gy (or mGy), unless citing a direct quote that uses other units. Low-dose throughout this report is arbitrarily defined as a dose of 100 mGy (10 rad) above natural background. Low-dose rate is defined as <0.01 mGy/min (1 mrad/min) above natural background. The definitions for LDDRs have varied over time but generally fall below 200 mGy for low-dose and <0.05 mGy/min for low-dose rate. 3
The USEPA relies on the linear no-threshold (LNT) dose–response model developed in the US National Academy of Sciences (NAS) biological effects of ionizing radiation VII report 4 to (1) set regulatory standards to protect human health, 5 (2) project risks of LDDR radiation exposure among the US population, and (3) develop tools to help establish cleanup levels. 6 We critically review the latest scientific literature and present alternative risk assessment models (eg, threshold or hormesis) for determining radiological cleanup levels in environments containing low-level residual radioactivity. Throughout this article, we note USEPA’s public policy positions for radiation protection and suggest alternative risk assessment approaches that are consistent with the latest science, protective of human health and the environment, and reduce unnecessary public health and financial burdens to society affected by low-level residual contamination from man-made or natural radioactive materials.
Two recent petitions to US regulators have drawn increased attention to this issue. In 2015, several members of the group, Scientists for Accurate Information (SARI), submitted petitions 7,8 to the US Nuclear Regulatory Commission (NRC), requesting “…that the NRC greatly simplify and change Part 20 to eliminate the use of the LNT paradigm and take radiation hormesis into account.” This petition cited 36 references in support of the petitioners’ request. The bases of the petition were also presented in a peer-reviewed scientific article. 9 The USEPA submitted comments opposing the petition 10 ; however, the USEPA’s comments declined to address all but 2 references cited by the petitioners. The SARI also recently submitted a letter to the current administrator of the USEPA, 11 requesting that USEPA cease the application of the LNT for LDDR environments. The USEPA’s response 12 cited its comments on the NRC petition.
Another recent event relevant to this topic is the issuance of Executive Order 13777
13
by the President of the United States. This Executive Order established a policy to eliminate unnecessary regulatory burdens. As a result, the USEPA formed a Regulatory Reform Task Force to evaluate existing regulations and identify regulations that should be repealed, replaced, or modified. The USEPA administrator advised the Office of Air and Radiation (OAR) to provide recommendations regarding specific rules that could be repealed, replaced, or modified to make them less burdensome by May 15, 2017. The OAR hosted a public meeting on April 24, 2017, to solicit proposals. The Health Physics Society (HPS) gave verbal comments during the meeting urging USEPA to reconsider their adherence to LNT and to improve several documents (eg,
6,14
–17
) by better addressing uncertainties in LDDR environments. The HPS also stated that reliance on the LNT model “…tends to foment the public’s fear of all types of radiation.” The HPS followed up with written comments, which stated, As a scientific organization of professionals who specialize in radiation safety, the HPS believes the EPA’s reliance on the LNT model, especially at very low doses and dose rates, is inappropriate and can exaggerate the risk. Of most concern to the HPS is the EPA’s extrapolation of the LNT model to calculate collective dose and the use of collective dose as a metric for risk.
18,19
This article is divided into sections addressing several questions regarding the continued use of the LNT model for LDDR radiation environments:
Introduction
What is the scientific basis for using the LNT in LDDR radiation environments?
Is the USEPA using the concept of collective dose appropriately?
Is there scientific consensus for using the LNT model to estimate risk in LDDR environments?
Should the BEIR VII report continue to be used to justify the use of the LNT model for LDDR radiation environments?
What other information is available in the scientific literature and does it support the continued use of the LNT model for LDDR environments?
Is it appropriate to regulate ionizing radiation in the same manner as toxic chemicals?
Should the current USEPA regulatory radiation policies be reconsidered and harmonized with the radiation protection philosophy given the lessons learned from Fukushima?
Discussion
Conclusion
What is the Scientific Basis for Using the LNT in LDDR Radiation Environments?
Studies to understand health effects on people exposed to LDDR are especially important, since they most closely reflect the environment following a radiological cleanup effort. They also serve to help regulatory agencies determine whether the cleanup policies are adequate to protect the people and environment while accounting for social and economic factors (ie, do they do more good than harm to society?). Does the LNT model withstand scientific scrutiny to link cancer with causation from LDDR exposures to ionizing radiation? Over 50 years ago, Sir Austin Bradford Hill established a set of objective criteria that help determine when causation can be legitimately concluded from an observed correlation. 20 These criteria are (1) temporal relationship (eg, exposure must occur before the disease), (2) strength (eg, size of the association between exposure and disease), (3) dose–response relationship, (4) consistency, (5) plausibility, (6) consideration of alternate explanation (eg, confounding effects), (7) experiment (eg, the condition can be altered by an appropriate experimental regimen), (8) specificity, and (9) coherence (eg, associated compatible with existing theory and knowledge?). Hill’s criteria have been specifically applied to LDDR, 21 and the case for LDDR increasing carcinogenic risk has been found lacking. In the current article, we point out when any of Hill’s criteria can be applied to particular arguments or evidence.
In its comments on SARI’s petition to the NRC, the USEPA stated, The U.S. Environmental Protection Agency strongly disagrees with the petition to the Nuclear Regulatory Commission (NRC) to cease using the linear no-threshold (LNT) model as a basis for regulating exposures to ionizing radiation. The USEPA’s Carcinogen Assessment Guidelines specify that LNT should be used as a default assumption unless there is compelling evidence that the biological mechanism for carcinogenesis is inconsistent with LNT.
10
This argument was also published by a senior official within the USEPA in a scientific article using a disclaimer that the article represented his own personal opinion. However, his article continues to be used by the agency to justify reliance on the LNT model. Puskin wrote: Radiation protection, like the regulation of other carcinogenic agents, is—in the absence of compelling evidence to the contrary—predicated on the linear, no-threshold (LNT) hypothesis…
5
These explanations are not consistent with basic scientific study designs that accept a null hypothesis (eg, no effect at low doses 22 ), unless there is strong evidence (eg, statistical significance P < .05) to suggest otherwise (eg, LNT is valid at low doses). The burden of proof lies with those asserting the LNT model is correct, not on those asserting the null hypothesis of no effect at low doses. These arguments inappropriately shift the burden of proof to proving that LNT is not valid, which is an impossible task. 23 It can always be argued that an LNT-predicted risk might exist but is too small to be detected, rendering the LNT hypothesis unfalsifiable. To be scientifically sound, compelling evidence must be provided that the valid null (no effect at low doses) should be rejected in favor of an alternative hypothesis (eg, there are detrimental health effects at low doses, as predicted by the LNT model; or there are no detrimental health effects at low doses but there are effects at higher doses, as predicted by the threshold model; or there are beneficial health effects at low doses, as predicted by the hormesis model). The current USEPA policy takes the position that the LNT model is accurate unless “compelling evidence to the contrary” is presented. This approach is included in the agency’s guidelines that direct the use of the LNT even if the scientific evidence cannot substantiate that conclusion. This is a circular argument that excludes the option of other alternative models from being considered.
USEPA goes on to comment, Biophysical calculations and experiments demonstrate that a single track of ionizing radiation passing through a cell produces complex damage sites in DNA, unique to radiation, the repair of which is error-prone. Thus, no threshold for radiation-induced mutations is expected, and, indeed, none has been observed.
10
This statement relies on a biological plausibility argument to support the use of the LNT dose–response model in LDDR environments. However, a biologically plausible argument based on more recent scientific evidence suggests that extensive protective biological processes are initiated upon initial DNA damage to prevent potential development of cancer (eg, cellular- and tissue-level defense mechanisms including not only DNA damage repair but also apoptosis, premature terminal differentiation, and immunosurveillance
9,24,25
). As explicitly acknowledged by the National Council on Radiation Protection and Measurements (NCRP) over 15 years ago,
26
Application of this [microdosimetric] argument to complex endpoints such as radiation-induced carcinogenesis is, however, more uncertain. Based on these biophysical considerations about the shape of the dose-response relation for low-dose radiation-induced carcinogenesis, conclusions can be drawn if: (1) radiogenic cancer induction is causally related to radiation induced damage in a single cell and (2) the ways in which other cells or cell systems subsequently modify the probability that any given initially radiation-damaged cell becomes the clonal origin of a cancer do not vary with dose in a nonlinear fashion. (emphasis added)
More and more scientific evidence has accumulated in recent years that neither of these underlying assumptions are valid.
24,27
In fact, even references cited by USEPA as supporting this position actually contradict it. For example, Trott and Rosemann stated, Since the cell is able to repair a very high level of endogenous DNA damage without frequent mutagenic consequences, a further small increment of such DNA damage from low dose rate irradiation should, equally efficiently, be repaired. Mutation rates will only increase if due to higher dose and dose rate, the capacity for high fidelity DNA repair is exceeded.
28
And also, The mechanism which induces ‘radiation-induced genomic instability’ appears to involve a non-nuclear target and upregulation of oxidative stress, which also is the main mechanism of metabolic DNA damage. These experimental observations are not compatible with a single hit mechanism which is the basis for the microdosimetric justification of the linear-non threshold dose response hypothesis.
28
Current evidence demonstrates that biological responses to LDDR radiation are distinct from those occurring at high doses. 21,24,29 –33 Similarity of mechanisms is one of the fundamental assumptions underpinning the LNT extrapolation from high-dose and high-dose rate (HDDR) to LDDR, and there is growing evidence that this assumption is inaccurate.
The USEPA’s assertion that no threshold in radiation-induced mutations has been observed is inaccurate. Early data on mutations in fruit flies were very influential in adoption of the LNT model. These data actually indicated a threshold but was misrepresented as supporting the LNT model. 34 –36 In similar experiments, more recent studies examining mutations in fruit flies confirm that the dose–response is characterized by a threshold or even hormesis. 37 –41 These studies relate to another of Hill’s criteria—Experiment which can greatly strengthen the case for causation. 20 However, these studies do not support the LNT model but rather a threshold or hormesis model.
A threshold for radiation-induced mutations has also been observed in mice, 42 –46 human-hamster hybrid cells, 47 and human cells. 48 These findings also relate to another of Hill’s criteria—Consistency, defined by Hill as generality or repeatability 20 —but here again, they do not support the LNT model; instead, they demonstrate thresholds.
The USEPA’s own Scientific Advisory Board (SAB)
49
has cautioned the Agency on taking this position on LNT, stating, Radiation-induced genomic instability seems to be one of the early stages in the carcinogenesis process and has been seen both in vitro and in vivo. These observations challenge the relative importance that initial mutations play in radiation-induced cancer,
50
Genomic instability and the ability to modify responses after the radiation exposure both challenge the linear relationship between initial DNA damage and cancer frequency. (emphasis added)
The USEPA response suggests that unless cells repair DNA damage with 100% fidelity, the risk of cancer is increased. 5,10 This is not supported by current evidence. 24 DNA repair mechanisms act on both radiation-induced damage and on preexisting spontaneous background DNA damage resulting from oxygen metabolism and other endogenous sources. If the resulting sum of radiation plus spontaneous DNA damage after radiation exposure is less than the level of damage that existed prior to radiation exposure, it is entirely reasonable and biologically plausible that radiation risks are not increased (consistent with a threshold) or may even be decreased (consistent with hormesis).
Nonetheless, USEPA continued, Of all the agents demonstrated to be carcinogenic, the evidence for LNT is particularly strong for ionizing radiation. Within limitations imposed by statistical power, the available (and extensive) epidemiological data are broadly consistent with a linear dose-response for radiation cancer risk at moderate and low doses.
10
Strength of association is another of Hill’s criteria.
20
The USEPA states the evidence is strong and consistent with the LNT response at moderate and low doses. However, radiation in general is a weak carcinogen,
51,52
and the evidence that LDDR radiation exposure in particular increases cancer risk is lacking.
21
In fact, many professional organizations have explicitly warned against estimating risks from low-dose radiation environments due to large uncertainties associated with the epidemiologic data.
53
–55
The USEPA’s position on this point appears to contradict their own guidance document,
6
which states, Generally speaking, epidemiology cannot be used to detect and quantify the carcinogenic effects of radiation at doses below about 100 mGy of low-LET [linear energy transfer] radiation because of limitations on statistical power.
56,57
Is the USEPA Using the Concept of Collective Dose Appropriately?
International expert advisory bodies have repeatedly cautioned against application of the LNT model to calculate hypothetical risks from LDDR exposures.
53,55
For example, United Nations Scientific Committee on the Effects of ionizing Radiation (UNSCEAR) has stated, In general, increases in the incidence of health effects in populations cannot be attributed reliably to chronic exposure to radiation at levels that are typical of the global average background levels of radiation.…the Scientific Committee does not recommend multiplying very low doses by large numbers of individuals to estimate numbers of radiation-induced health effects within a population exposed to incremental doses at levels equivalent to or lower than natural background levels.
53
Similarly, the ICRP has stated, Collective effective dose is an instrument for optimisation, for comparing radiological technologies and protection procedures. Collective effective dose is not intended as a tool for epidemiological studies, and it is inappropriate to use it in risk projections. This is because the assumptions implicit in the calculation of collective effective dose (e.g., when applying the LNT model) conceal large biological and statistical uncertainties. Specifically, the computation of cancer deaths based on collective effective doses involving trivial exposures to large populations is not reasonable and should be avoided. Such computations based on collective effective dose were never intended, are biologically and statistically very uncertain, presuppose a number of caveats that tend not to be repeated when estimates are quoted out of context, and are an incorrect use of this protection quantity.
55
Despite this guidance, the USEPA develops risk estimation tools based on the LNT model to determine cleanup policies and guidelines for its Comprehensive Environmental Response, Compensation, and Liability Act (CERCLA) superfund sites. Because they multiply very small doses by large populations to predict excess cancer incidence or mortality, these tools conflict with the scientific guidance provided by other governmental or scientific organizations and professional societies. The impact to the United States is real, resulting in enormous cleanup costs that show no demonstrable benefit to society, creates a social stigma on affected communities, and foments fear among the public, causing unnecessary harm by promoting ill-advised decision-making. The USEPA’s estimates of cancer incidence and mortality risks due to low doses of ionizing radiation for US population as well as their advice to the public and tools used to establish cleanup levels are at odds with UNSCEAR’s and ICRP’s guidance. For example, USEPA states, …overall, if each person in a group of 10,000 people exposed to 1 rem of ionizing radiation, in small doses over a life time, we would expect 5 or 6 more people to die of cancer than would otherwise. In this group of 10,000 people, we can expect about 2,000 to die of cancer from all non-radiation causes. The accumulated exposure to 1 rem of radiation, would increase that number to about 2005 or 2006.
58
This advice to the public is inconsistent with the intended purpose of effective dose (prospective dose estimation for the purpose of optimization), which is inappropriate for predicting future cancer risk. 59
Is There Scientific Consensus for Using the LNT Model to Estimate Risk in LDDR Environments?
USEPA’s comments on the public petitions to the NRC
7,8
stated,
Given the continuing wide consensus on the use of LNT for regulatory purposes as well as the increasing scientific confirmation of the LNT model, it would be unacceptable to the USEPA to ignore the recommendations of the NAS [US National Academy of Sciences] and other authoritative sources on this issue. The USEPA cannot endorse basing radiation protection on poorly supported and highly speculative proposals for dose thresholds or doubtful notions concerning protective effects from low-level ionizing radiation. Accordingly, we would urge the NRC to deny the petition.
And similarly, Over the last half century, numerous authoritative national and international bodies have convened committees of experts to examine the issue of LNT as a tool for radiation regulation and risk assessment. These include the U.S. National Academy of Sciences (NAS), the National Council on Radiation Protection and Measurements (NCRP), the International Commission on Radiological Protection (ICRP), and the United Nations Scientific Committee on the Effects of ionizing Radiation (UNSCEAR). Again and again, these bodies have endorsed LNT as a reasonable approach to regulating exposures to low dose radiation. One exception was a French National Academy Report, which found low-dose radio biological effects in vitro indicative of nonlinearity in the dose response.
10
This argument was also repeated in
5
: To assist the Agency in its assessment of the health risks from ionizing radiation, EPA has often helped sponsor reports from these organizations, particularly from the NAS ‘BEIR Committees’. The risk models and supporting evidence is then reviewed by EPA’s Scientific Advisory Board of outside distinguished scientists before becoming final and being implemented. Thus, EPA’s estimates of risk to low dose radiation reflect a broad scientific consensus.
In these arguments, the USEPA “appeals to authority,” 23 where the LNT model is asserted to be valid because some authority putatively endorses it. This is an academic point because there is in fact no consensus in favor of the LNT model among individual scientists, professional societies, expert advisory bodies, US regulators, nor even within USEPA itself. As acknowledged earlier, contradictory recommendations were issued by the French National Academies of Science and Medicine, 60 and evidence supporting the French conclusions has grown in the recent years. The French report contradicts the claim of consensus among expert advisory bodies in support of the LNT model. 5,10
The USEPA’s own SAB has expressed caution about applying the LNT at low doses as well. The USEPA has claimed that unfettered application of the LNT, …is the position adopted by the USEPA after review by the Agency’s Scientific Advisory Board, an independent group of distinguished outside scientists.
However, the SAB’s Radiation Advisory Committee cautioned
49
: …a major issue with the choice of the LNT model is whether it is appropriately applied at low doses. …while the RAC endorses USEPA’s use of the LNT model, the Agency is advised to continue to monitor the science of the biological mechanisms underlying cancer induction at low doses of ionizing radiation and of their influence on the biophysical models used to estimate the cancer risk in this dose range. At radiation exposures in the range of natural background, it is difficult to distinguish radiation-induced changes in risk from the baseline. Thus, as a cautionary note, the RAC recommends that the USEPA discuss potential problems associated with the use of LNT dose response model risk estimates in very low dose settings. Currently at these low doses, statistically significant differences between the cancer rates among ‘exposed’ (defined study populations) and ‘non-exposed’ (defined comparison populations) are not observed. As BEIR VII acknowledges, the epidemiological data below 100 mSv (0.1 Sv) are not sufficient by themselves for risk estimation, and considerable cellular and animal data suggest complexities beyond the application of a simplified DNA damage model which historically has been used as support for an LNT dose-response model.
It is important to note that since the SAB last took up this issue and advised USEPA to explicitly monitor developments on these topics, the NCRP has issued comprehensive reports on uncertainties in the measurement and dosimetry of external radiation, 61 internal radiation dose, 62 and in the estimation of radiation risks. 63
There is also no consensus among US regulators. The US General Accounting Office (GAO) has on multiple occasions investigated whether or not there is a consensus among USEPA, the NRC, and the Department of Energy (DOE) on approaches to regulating LDDR radiation exposures to the public.
2,64
–66
Over 20 years ago, the GAO found, the radiation standards that have been developed reflect a lack of overall interagency consensus on how much radiation risk to the public is acceptable Differences in radiation limits and risks, calculation methods, and protective strategies reflect the historical lack of a unified federal framework for protecting the public from radiation exposure.
65
The situation had not been resolved by 2000, with GAO finding,
2
U.S. regulatory standards to protect the public from the potential health risks of nuclear radiation lack a conclusively verified scientific basis, according to a consensus of recognized scientists. In the absence of more conclusive data, scientists have assumed that even the smallest radiation exposure carries a risk. This assumption (called the ‘linear, no-threshold hypothesis’ or model) extrapolates better-verified high-level radiation effects to lower, less well-verified levels and is the preferred theoretical basis for the current U.S. radiation standards. However, this assumption is controversial among many scientists …USEPA and NRC have disagreed on exposure limits. Although we recommended as far back as 1994 that the two agencies take the lead in pursuing an interagency consensus on acceptable radiation risks to the public, they continue to disagree on two major regulatory applications: (1) the proposed disposal of high-level nuclear waste in a repository at Yucca Mountain and (2) the cleanup and decommissioning of nuclear facilities.
As recently as 2017, the GAO again recommended the DOE take the lead on reestablishing and coordinating federal research on the topic of low-dose radiation effects. 66
There is also no consensus in support of the LNT model among relevant professional societies.
54,67
–69
Extrapolation of LDDR risks via the LNT model is at odds with the advice of professional societies around the world. For example, the Australasian Radiation Protection Society has stated, There is insufficient epidemiological evidence to establish a dose-effect relationship for effective doses of less than a few tens of millisieverts in a year above the background level of exposure and further,…no inference may be drawn concerning the risk to health or risk of fatality of an individual from an effective dose below 10 mSv in a year. For individual doses less than some tens of millisieverts in a year, risk inferences are unreliable and carry a large uncertainty that includes the possibility of zero risk.
68
In the United States, the HPS has concluded, The Health Physics Society advises against estimating health risks to people from exposures to ionizing radiation that are near or less than natural background levels because statistical uncertainties at these low levels are great…Substantial and convincing scientific data show evidence of health effects following high-dose exposures (many multiples of natural background). However, below levels of about 100 mSv above background from all sources combined, the observed radiation effects in people are not statistically different from zero. Scientists evaluate and estimate radiation risk using several assumptions that, taken together, may lead to a range of hypothetical health risk estimates for any given exposure scenario. For radiation protection purposes and for setting radiation exposure limits, current standards and practices are based on the questionable premise that any radiation dose, no matter how small, could result in detrimental health effects such as cancer or heritable genetic damage. Implicit in this linear no-threshold (LNT) hypothesis is the core assumption that detrimental effects occur proportionately with radiation dose received (NAS/NRC 2006). However, because of statistical uncertainties in biological response at or near background levels, the LNT hypothesis cannot provide reliable projections of future cancer incidence from low-level radiation exposures (NCRP 2001).
54
Additional examples from medical physics and radiology professional societies are provided in “What Other Information Is Available in the Scientific Literature and Does It Support the Continued Use of the LNT Model for LDDR Environments?” section.
In addition to expert advisory bodies and professional societies, numerous individual scientists have argued against application of the LNT at low doses. 24,70 –72 Studies have also been conducted of individual scientists’ views regarding the accuracy of the LNT dose–response model for radiation effects 73,74 (Table 1). A survey of scientists employed at US national laboratories revealed that 70% believed that a threshold model accurately reflected radiation effects, compared to only 12% who believed an LNT model is accurate. 74 Even among members of the Union of Concerned Scientists, a group that has expressed concerns about the US nuclear power industry, 48% believed a threshold model accurately describes LDDR effects while only 21% favored an LNT model. The results were similar when scientists from the United States and Europe who subscribe to the journal Science were surveyed 73 : (1) 75% of US scientists believed a sublinear threshold model accurately described radiation effects, compared to only 19% who favored an LNT model; (2) for British scientists, the breakdown was 71% for sublinear threshold and 21% for LNT models; (3) for French scientists, 70% and 18%, respectively; (4) for German scientists, 64% and 22%, respectively, and (5) for other European scientists, 69% and 23%, respectively. These studies indicate that a majority of individual scientists are skeptical of the accuracy of the LNT model—exactly the opposite of a pro-LNT consensus claimed by USEPA. 5,10
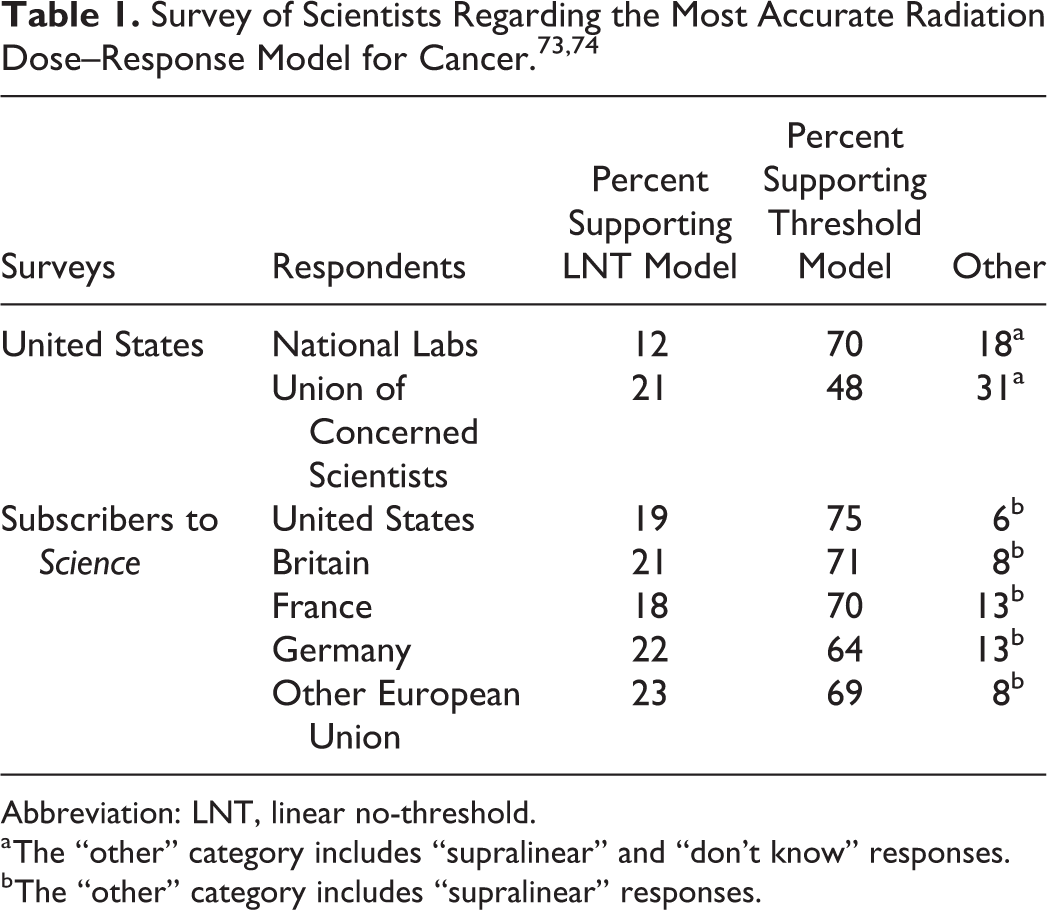
Abbreviation: LNT, linear no-threshold.
a The “other” category includes “supralinear” and “don’t know” responses.
b The “other” category includes “supralinear” responses.
Should the BEIR VII Report Continue to be Used to Justify the Use of the LNT Model for LDDR Radiation Environments?
In short, the answer is “no.” The USEPA places great weight on a few scientific references to support its application of the LNT model, most notably, the BEIR VII report from the US NAS.
6
For example, USEPA states, The BEIR VII study, which was sponsored by several federal agencies including the USEPA and the NRC, determined that ‘the balance of evidence from epidemiologic, animal and mechanistic studies tend to favor a simple proportionate relationship at low doses between radiation dose and cancer risk.’
The NAS originally adopted the LNT model as the basis for its philosophy to protect against radiation-induced genetic mutations in the human population at the recommendation of its Biological Effects of Atomic Radiation Committee Genetics Panel in 1956.
75
This recommendation was made in spite of the fact that radiation-induced genetic effects in the offspring of irradiated parents have never been observed in humans. Recent historical research has revealed that this recommendation was made under questionable circumstances (
76
–80
but see also
81
–83
). Even so, the LNT model was later expanded and applied to radiation-induced cancer risks. Controversial from the beginning, this recommendation nevertheless initiated decades of institutional inertia, with multiple iterations of NAS Committees repeatedly reaffirming the suitability of the LNT model as the basis of radiation protection philosophy, most recently in the BIER VII report over a decade ago.
4
The BEIR VII Committee concluded, …current scientific evidence is consistent with the hypothesis that there is a linear, no-threshold dose-response relationship between exposure to ionizing radiation and the development of cancer in humans.
Although they acknowledged that a linear-quadratic model fit the data better than the LNT model at low doses, they reported the improvement was not statistically significant. In large part, because the NAS inappropriately treated the LNT model as if it were the null hypothesis rather than appropriately treating it as an alternative hypothesis to be tested against the null of no effect, the LNT model became the Committee’s preferred recommendation. In turn, the USEPA incorporated BEIR VII risk models into their policy and guidance. 84
However, two major pieces of evidence the BEIR VII Committee relied upon to support their endorsement of the use of the LNT model to estimate risks from low doses, the Lifespan Study (LSS) of the Japanese atomic bomb survivors and the 15-country study of nuclear workers, no longer support the LNT model. 85 We summarize the problems with continuing to cite these two pieces of evidence to justify risk estimates using the LNT model in LDDR environments below.
It is widely acknowledged (in the BEIR VII report and elsewhere) that the LSS was the most influential study in setting radiation protection guidelines around the world. It is also evident that even these data set do not provide definitive evidence of increased cancer risk after exposure to low radiation doses.
86
In fact, the most recent epidemiological study on cancer mortality in the Japanese survivors of the atomic bombings states, the estimated lowest dose range with a significant ERR [excess relative risk] for all solid cancer was 0 to 0.20 Gy.
87
Another way of saying this is that no significant ERR was observed for doses below 0.20 Gy. The authors also concluded that, …statistically significant upward curvature was observed when the dose range was limited to 0–2 Gy…The curvature over the 0–2 Gy range has become stronger over time.
This means the argument for an LNT relationship has weakened over time. This is an example of epidemiological data possibly reflecting dissimilarity of biological responses to LDDR and HDDR; however, it is not discussed by the authors in spite of explicit calls to integrate biology and epidemiology.
88,89
Despite that evidence, these authors concluded,
…a formal dose-threshold analysis indicated no threshold; i.e. zero dose was the best estimate of the threshold.
87,90
Reviewing their threshold analysis, others found that they excluded the possibility of negative risk values despite eight of the 10 lowest data points having confidence intervals, including negative values. Alternative analyses that did not exclude negative values revealed the possibility of a nonzero threshold. 35,91 –94
Similarly, for cancer incidence in the LSS cohort, The lowest dose range that showed a statistically significant dose response using the sex averaged, linear ERR model was 0–100 mGy.
95
In other words, there are no detectable health effects below 100 mGy. It is evident that statistical power limitations preclude the selection of one alternative hypothesis over another (eg, LNT vs linear with threshold); therefore, the assertion that the LSS data provide definitive evidence in support of the LNT is not accurate. A threshold model is also consistent with both the latest solid cancer incidence and the mortality data.
The second piece of evidence the BEIR VII Committee relied heavily upon was the so-called “15-country study.”
96
This study initially concluded that, Significantly increased risks were found for mortality from all cancers excluding leukemia and from lung cancers.
However, further analysis revealed that this conclusion is also no longer valid. The Canadian Nuclear Safety Commission concluded that Atomic Energy of Canada, Ltd nuclear energy workers cohort included in the original 15-country study did, …not have an increased risk of solid cancer mortality. Incomplete dose records are likely the cause for the apparent increased risk of solid cancer mortality in AECL NEWs first employed before 1965 (1956-1964).
97
Furthermore, Zablotska et al
98
concluded: Significantly increased risks for early AECL workers are most likely due to incomplete transfer of AECL dose records to the National Dose Registry. Analyses of the remainder of the Canadian nuclear workers (93.2%) provided no evidence of increased risk Study findings suggest that the revised Canadian cohort, with the exclusion of early AECL workers, would likely have an important effect on the 15-country pooled risk estimate of radiation-related risks of all cancer excluding leukaemia by substantially reducing the size of the point estimate and its significance.
These findings should serve as a warning against relying on BEIR VII to justify the use of the LNT model for LDDR risk estimation purposes.
In summary, two influential pieces of evidence relied upon by the BEIR VII Committee (the LSS cohort and the 15-country study) no longer support the LNT model based on the latest scientific literature. However, the USEPA relies heavily upon the recommendations of the BEIR VII report on this issue and continues to use it to support is current policies and risk assessment strategies. This evidence alone is enough to warrant a new look at the science for risk assessment decision-making and determining radiation cleanup levels in LDDR environments.
What Other Information is Available in the Scientific Literature and Does it Support the Continued Use of the LNT Model for LDDR Environments?
The USEPA has cited studies published after BEIR VII, which they assert provides support for the LNT model in LDDR environments
99
: Since publication of BEIR VII, additional evidence has accumulated supporting the use of LNT to extrapolate risk estimates from high acute doses to lower doses and dose rates. In this connection, we would note, inter alia, results of epidemiological studies on: nuclear workers in the United States, France and the United Kingdom
100
; residents along the Techa River in Russia who were exposed to radionuclides from the Mayak Plutonium Production Plant
101,102
; and children who had received CT scans.
103
These studies have shown increased risks of leukemia and other cancers at doses and dose rates below those which LNT skeptics have maintained are harmless - or even beneficial.
10
Follow-up studies of a selected part of the cohort included in the 15-country study has recently been published to examine leukemia
100
and solid cancer
104
risks. These studies, also known as the International Nuclear Workers Study (INWORKS)] studies, examined risk in worker cohorts from the United States, France, and the United Kingdom (a subset of the larger cohort included in the 15-country study). The leukemia study
100
concluded, This study provides strong evidence of positive associations between protracted low-dose radiation exposure and leukaemia.
Similarly, the solid cancer study
104
concluded, The study provides a direct estimate of the association between protracted low dose exposure to ionising radiation and solid cancer mortality.
Several methodological questions have been raised about these studies,
105,106
and the authors have replied.
107
In addition, numerous methodological objections have been raised in Sacks et al.
108
These include: failure to account for natural background radiation exposure, the differences in which potentially dwarf the occupational exposures of the study cohort; failure to account for medical exposures experienced by the public; failure to account for dose–rate effects; the a priori assumption of an LNT dose response; mischaracterization of the y-intercept as 0 total dose when in fact it was 0 occupational dose; arbitrary exclusion of all dose responses except LNT and linear-quadratic (which actually provided a better fit to their observed data, but the authors claimed the improvement was not statistically significant); dismissing 6 of 7 disease outcomes as being highly imprecise rather than stating that they are not statistically significantly different from no-effect; creating an artificial disease category by arbitrarily combining 3 forms of leukemia and excluding a fourth, then characterizing this artificial grouping as an additional statistically significant association; providing misleading characterizations of the data above 200 mGy as statistically significant when in fact, only the 200 to 300 mGy dose category was significantly elevated, whereas the highest dose category was not (nor was any other dose category); insufficient consideration of age as a possible confounder; a priori and arbitrary consideration only of the possibility of increased risks and excluding the possibility of decreased risks; and the arbitrary choice of a 90% confidence limit rather than the more conventional 95%, thus increasing the possibility of significance, then mischaracterizing the results as strong evidence of risk from LDDR radiation exposure.
To this list of methodological shortcomings, we add the omission of occupationally required medical imaging examinations (which are distinct from medical doses received by the public at large—raised as #2 above), resulting in potential significant underestimation of external radiation dose. With regard to potential confounding by diagnostic medical dose, the INWORKS authors state, …for confounding to occur, medical radiation exposures would need to be associated with occupational doses…which is unlikely to be the case.
107
The basis for the authors’ conclusion that such confounding is unlikely is not provided. The omission of dose from medical imaging received by workers as a condition of employment presents one of the most serious questions about the methodology of these studies, as it likely resulted in potentially significant underestimation of external radiation dose. At several of the US sites included in the study, workers were required to undergo a medical examination at least yearly, which included medical imaging examinations. Of particular concern is the use of photofluorography in the early years (eg, 1940s to 1950s). Photofluorography delivered high-dose rate radiation exposures to workers at the Savannah River Site (1951-1960, 0.46 mGy per examination to male red bone marrow),
109
Hanford (1943-1962, 1.41 mGy),
109
and the 3 Oak Ridge Sites: Y-12 (at least 1943-1947, 2.76 mGy),
110
X-10 (at least prior to 1947, 2.58 mGy),
For the Techa River cohort, it is unclear why USEPA chose to cite an outdated reference
101
when there is a more recent update
115
; however, risk estimates in the most recent update are less than half of the estimates in the earlier reference USEPA cited. Furthermore, Krestinina et al
115
states, For the basic dose–response model, the ERR was assumed to be linear in dose but we also considered models where the dose response was taken as a linear-quadratic, a pure quadratic function of dose, or threshold models in which the ERR was assumed to be 0 up to some threshold dose and taken as linear for higher doses.
No further details are provided on their analysis of thresholds. It is not clear whether the authors allowed ERR to assume negative values, which would certainly be indicated given that the total leukemia rates reported for the 5 lowest dose groups were lower than the control group (those who received <0.01 Gy). Only the 2 highest dose groups (those receiving 0.5-1 Gy and 1+ Gy) exceeded controls. For leukemia excluding chronic lymphocytic leukemia, the rates for 2 of the 3 lowest dose groups were below that for the control group, suggesting a threshold or even potential hormetic effect which is often dismissed as a potential healthy worker effect. The authors reported that their data, “…are consistent with a linear dose response…”; however, they do not report whether or not their data are also consistent with a threshold or hormetic dose response, which would seem to be the case given these results. If multiple models adequately describe the observed dose response, then USEPA should not cite these results as supporting the LNT model and excluding the threshold model as petitioned by SARI.
For solid cancers in the Techa River Cohort, the situation is similar. The USEPA cited,
102
and again, the authors claimed, There is a statistically significant (P = 0.02) linear trend in the smoking-adjusted all-solid cancer incidence risks.
However, a closer look at the data in this study reveals that the two lowest dose categories have ERR estimates lower than the zero dose controls, consistent with a hormetic dose response or at least a threshold (Figure 1). This is another example of epidemiological data possibly reflecting the dissimilarity of biological responses to LDDR and HDDR, but again it is not discussed by the authors.

Solid cancer excess relative risk (ERR) estimates for the Techa River cohort plotted against stomach dose. Reproduced from figure 1 of Davis et al 102 , used with permission, circle added for emphasis.
Within the past few years, new studies of pediatric patients receiving computed tomography (CT) medical imaging examinations claimed to observe increases in risks from relatively low doses (though delivered at a high-dose rate).
103,116
These studies received extensive press coverage, and almost immediately, claims were made that, …the new data confirm that the cancer risk associated with the radiation from a CT scan is very small, but not zero.
117
In presentations to the Interagency Steering Committee on Radiation Standards, USEPA has referenced these studies to suggest potential adverse health effects from LDDR radiation.
99
However, these early enthusiastic pronouncements have not held up to scientific scrutiny. A number of significant methodological issues have been identified in these studies,
118,119
including (1) individual doses were not directly assessed, but rather “typical” doses were assumed; (2) doses applied were for adults and assumed no decrease for pediatric patients, even though this is the standard of care; and (3) the reason for the CT was not considered, and it is possible that the underlying condition indicating the CT has associated cancer susceptibility (this point was acknowledged in one of the USEPA presentations
99,120
). On the latter point, as explained by Ulsh,
91
One of the strongest associations
103
observed was for gliomas, but they did not control for prior head injury. Head injuries are a common reason for head CT in children, and head injury may be associated with brain tumors.
This assessment agrees with UNSCEAR,
121
which concluded …There are concerns about the risk estimates because of lack of information about indications for the CT scans and the consequent potential for ‘reverse causation’ (i.e., cancers may have been caused by the medical conditions prompting the CT scans rather than by the CT dose).
The NCRP came to similar conclusions, stating: Children who receive frequent examinations may have some underlying disability related to the outcome of interest. That is, a child who receives multiple CT examinations of the head may have a central nervous system disorder that is prompting such examinations and it is these underlying disorders that are related to the cancer diagnosis and not the CT radiation dose.
63
Furthermore, two recent studies from France 122 and Germany 123 have demonstrated that failing to account for the underlying reason requiring the examination can inflate risk estimates in studies of populations exposed to CT scans.
In spite of the UNSCEAR and NCRP conclusions, and multiple papers pointing out the limitations of these studies (eg, 91,119 ), they continue to be cited by USEPA and others as providing strong or definitive evidence of risks of very low radiation doses and supportive of the LNT model. 99 However, the application of the LNT model and the As Low As Reasonably Achievable (ALARA) principle to medical imaging has come under heavy criticism. 72,124 –126 Professional societies with expertise in medical imaging continue to unanimously maintain that the carcinogenicity of low radiation doses has not been demonstrated, and estimates of risks from low doses like those associated with medical imaging examinations remain speculative and unproven. For example:
American Association of Physicists in Medicine
At the present time, there is no convincing epidemiological evidence of increased cancer incidence or mortality from low radiation doses (<100 mSv). Because medical imaging exposures are typically much lower than 100 mSv, when such exposures are medically appropriate, the anticipated benefits to the patient are highly likely to outweigh any small potential risks. Therefore, when discussions of risk occur, it is essential that the benefit of the clinical task also be discussed. Additionally, the AAPM discourages describing potential risks associated with medical imaging using predictions of hypothetical cancer incidence and deaths. These predictions are contrary to directives of radiation protection organizations, are highly speculative and can lead to sensationalistic coverage in the public media, leading some patients to fear or refuse appropriate medical imaging.
69
International Organization for Medical Physics
Prospective estimates of cancers and cancer deaths induced by medical radiation should include a statement that the estimates are highly speculative because of various random and systematic uncertainties embedded in them. These uncertainties include dosimetric uncertainties; epidemiological and methodological uncertainties; uncertainties from low statistical power and precision in epidemiology studies of radiation risk; uncertainties in modeling radiation risk data; generalization of risk estimates across different populations; and reliance of epidemiological studies on observational rather than experimental data. Such uncertainties cause predictions of radiation-induced cancers and cancer deaths to be susceptible to biases and confounding influences that are unidentifiable.
127
The Society for Pediatric Radiology
To prevent misconceptions and public alarm, it is important to realize that the radiation used in CT scans has not been proven to cause cancer during a child’s lifetime. The very small risk of cancer from radiation exposure is an estimate and is based on information and statistics that are debatable.
67
USEPA has also cited studies of natural background and other environmental LDDR radiation exposures. Studies to understand health effects on people exposed to LDDR radiation are especially important, since they more closely reflect the environment following a radiological cleanup effort. They also serve to help the agency determine whether the cleanup policies are adequate to protect human health and environment while accounting for social and economic factors (ie, do they do more good than harm to society?). USEPA cited a study of leukemia risk due to natural background radiation exposure 128 and noted that this study claimed to have observed significant excess risk associated with dose rates as low as 1 mGy/yr. 99 We reviewed 128 and have identified several methodological issues.
The authors conclude, The possibility of confounding by some unidentified factor can never be entirely disproved, and is of particular concern when dealing, as here, with small RRs. However, we were unable to identify any mechanism whereby such confounding might plausibly account for the observed magnitude and specificity of effect in this study.
Socioeconomic status was the only confounder considered. There is evidence that paternal smoking is also associated with increased risk of childhood leukemia, 129 yet the authors did not consider this. The USEPA presented 128 as evidence of an LNT relationship for LDDR exposures despite the fact that it ignored potential confounding due to exposure to tobacco smoke. It is also worth noting that USEPA explicitly criticized other ecological LDDR studies that contradicted the LNT model 130,131 for not accounting for smoking ( 132,133 but see also 134,135 ). In the same presentation citing, 128 USEPA acknowledged the potential role of confounding factors, stating “variations in cancer rates due to other causes tend to swamp out those due to [ionizing radiation] exposure,” but apparently did not consider the potential for smoking to confound this study by noting this limitation.
This study
128
estimated background gamma and radon doses based on the residence location of the mother, using county measurements. This information was available for cases both at birth and at time of diagnosis. It was discovered that about half of the cases had moved between birth and diagnosis. For controls, only the residence location at time of birth was available, so the number of the controls who moved after birth is unknown. The UNSCEAR warned that, The study should be interpreted with caution because of the large uncertainties associated with using an ecological measure of dose.
121
The study considers only radiation exposure from natural background gamma radiation and radon. It ignores other, potentially larger sources of radiation exposure, for example, medical exposure. This is in spite of the fact that one of the coauthors of this study (MPL) was a coauthor of a separate study which claimed that exposure of British children to CT scans has increased their leukemia risk. 103 If it is true that exposure to CT scans is an important risk factor for childhood leukemia in this population, then omitting it from Kendall et al 128 cannot be justified. This is not consistent with the author’s stated inability to identify other possible sources of bias or confounding.
The number of cases with a γ-ray dose rate different from their control(s) was 14 308 (52% of all cases). This means that for 48% of the cases, the γ-ray dose rate was not different from their controls. This is not a result that strongly demonstrates a causal relationship between background γ-ray dose rate and leukemia. This observation does not satisfy Hill’s criteria of strength of association. 20
The authors used a log-linear logistic model for data analysis. But the use of such a model to analyze dose–risk relationships contains the intrinsic assumption that dose is linearly related to leukemia risk without threshold. They did not report testing other possible dose–response relationships. The authors assumed the validity of the LNT model, and citing this study in support of the LNT model is therefore a circular argument. 23
We also note that the USEPA presentations do not discuss the numerous studies of high natural radiation background areas that have observed no excess risks of cancer, even in populations exposed to dose rates well in excess of 100 mGy/yr (eg, 136 –141 ), except to categorically characterize them as “specious.” An objective evaluation of these studies is warranted to better understand any health effects from LDDR exposure to ionizing radiation, especially following the large-scale accidents in Chernobyl and Fukushima.
A similar LDDR situation, but involving a man-made elevated radiation background, occurred in Taipei, Taiwan, where construction materials contaminated with 60 Cobalt were used to build hundreds of structures throughout the city. 142 These buildings included schools and nearly 1000 apartments. More than 4000 people were chronically exposed to elevated radiation levels in this incident, some estimated as high as 1.2 Gy of cumulative dose. 143 It has also been the basis of legal action against the Taiwanese government. 144 The USEPA cited a study of this population as supporting the LNT model.
Doses to the apartment dwellers were estimated by survey instrument measurements in the affected apartments and compared to doses measured by personal dosimeters. 145 This study found agreement to within 10% to 15% for adults but only to within 60% for children. Large uncertainties were also noted in other dose reconstruction efforts, 146 which found that children received the smallest radiation doses compared to other family members. Reconstructed doses were found to agree with measured doses to within a factor of 3. 147 Radiation doses have also been measured using thermoluminescent dosimeters (TLDs), 148 and studies have been conducted to determine how to convert TLD measurements to doses received by residents using phantoms. 149
Epidemiological studies of this population reveal evidence that low doses of radiation not only failed to increase cancer risk but actually are consistent with a protective effect.
150
A study of cancer mortality in this population observed, The experience of these 10,000 persons suggests that long term exposure to radiation, at a dose rate of the order of 50 mSv (5 rem) per year, greatly reduces cancer mortality….
151
A separate study of cancer incidence was also conducted. 152 The abstract of this article highlighted the few specific cancer subtypes that yielded increased standardized incidence ratios (SIRs) based on very low numbers of cases (eg, leukemia, 7 cases vs 3.3 expected). No mention was made in the abstract of the lack of increase for the other 19 types of cancer which showed no statistically increased risks, nor more importantly, the observation of statistically significantly lower SIRs for all cancers (95 observed vs 114.9 expected), all cancers except leukemia (88 observed vs 111.6 expected) and all solid cancers (82 observed vs 109.5 expected). The USEPA’s presentation highlighted only the result for leukemia and breast cancer from a follow-up study that arbitrarily excluded the possibility of lower risks in the exposed population and forced a linear fit to the data on selected cancers to estimate hazard ratios at 100 mGy. 153 The hazard ratio at 100 mGy for leukemia excluding chronic lymphocytic leukemia was just barely significant at the 90% α level (confidence interval [CI], 1.01-1.31) but not at the more conventional 95% level. The USEPA presentations did not discuss that no statistically significant increases were observed in all cancers, all cancers excluding leukemia, all solid cancers, or cancers of the cervix, lung, thyroid, liver, stomach, or rectum, even when the data were forced to follow an LNT model. Further, the USEPA presentation did not mention two other studies, including a larger study of cancer incidence by the same authors, which found statistically significantly reduced mortality 151 and incidence 152 of all cancers combined and all solid cancers, suggesting not only a lack of cancer risk from low radiation doses but possibly also a protective effect. This creates the misleading impression that the Taiwan studies support the LNT model when in fact they directly contradict it.
Another update on this cohort was recently published,
154
which claimed, Dose-dependent risks were statistically significantly increased for leukaemia excluding chronic lymphocytic leukaemia (HR [hazard ratio] 100 mSv 1.18; 90% CI 1.04-1.28), breast cancers (HR100 mSv 1.11; 90% CI 1.05-1.20), and all cancers (HR 100 mSv 1.05; 90% CI 1.0-1.08, P = 0.04).
However, as observed by Doss,
155
The Hsieh et al publication reports that 249 cancer cases were observed in the cohort up to the end of 2012. To calculate the SIR, we need to know the expected number of cancer cases for the same period. In the 2006 report, Hwang et al reported that the expected number of all cancers was 114.9, and the average age of the irradiated cohort was 33.3 at the end of 2002 (The average age of the population was 17.1 at the time of irradiation and the cohort was followed-up for an average of 16.2 years).
152
Hence, for the Hsieh et al publication, the average age at the end of the study period (end of 2012) would be 43.3. The cancer incidence rates for the ages of 33.3 and 43.3, obtained by interpolation of the average of male and female cancer incidence rates during 1998–2002 from Taiwan Cancer Registry (TCR, 2008), are 86.3 and 222.4, respectively, indicating there would be an increase in cancer incidence between these two ages by a factor of ∼2.58. Therefore, considering the 114.9 expected cases to the end of 2002 (Hwang et al, 2006), the expected cancer cases up to the end of 2012 would be 296.4, resulting in a SIR of 249/296.4.0.84 (95% CI: 0.74–0.95).
Is it Appropriate to Regulate Ionizing Radiation in the Same Manner as Toxic Chemicals?
In 1992, the USEPA SAB provided guidance on ways to harmonize risk assessment and risk-reduction strategies for radiation and chemicals.
156
They noted that the regulations for radiation and chemical risks developed under different paradigms and stated: USEPA’s priorities should be directed towards reducing the greatest risks first, especially when that can be accomplished economically. The corollary to that principle is that similar risks should be treated similarly, which calls for harmonization, in so far as is possible, of risk reduction strategies between chemical and radiation. Harmonization does not necessarily imply identical treatment, but it does imply that any differences in treatment are clearly explained and justified. (emphasis added)
The options noted in the SAB Commentary were: bring risk-reduction strategies for excess radiation exposures consistently in line with the chemical paradigm, a direction that it noted that some parts of the agency were already headed; bring chemical risk-reduction strategies more in line with the radiation paradigm; or achieve harmony between the 2 systems by modifying both in appropriate ways, explaining residual differences, and placing more emphasis on what can reasonably be achieved. In this case, background risk could be incorporated, and the balancing of benefits and costs of risk-reduction measures could be strengthened while maintaining much of the Agency’s current approach to chemicals.
The radiation paradigm approach to control radiation exposures is based on principles developed over many decades by the ICRP and the NCRP.
75
These principles are: JUSTIFICATION: the need to justify any radiation exposure on the basis that the benefits to society exceed the overall societal cost; ALARA (Optimization): maintain any exposures as low as reasonably achievable, economic and social factors being taken into account; and LIMITATION: radiation exposures are kept to levels of acceptable risk.
As described by the ICRP, For any situation where intervention is considered, some protective actions might be justified while others are not justified. Of those protective actions which are justified, it is necessary to establish the level at which the best protection will be provided. In other words the radiation detriment averted by each protective action should be balanced against the cost and other detriments of the action in such a way that the net benefit achieved by the protective action is maximized (i.e. optimization of protection).
157
The principles of ALARA (Optimization) and LIMITATION can be viewed as a “top-down” approach to limit radiation exposure and health risk (Figure 2). Therefore, radiation exposures are considered acceptable if they are less than a specific limit and they are as low as reasonably achievable. Compliance with a dose limit alone does not define acceptable exposures or risk.

Cancer risk management paradigms. Reprinted with permission from the National Council on Radiation Protection and Measurements, http://NCRPonline.org.
The chemical paradigm approach can be viewed as a “bottom-up” approach. The historical use of this paradigm by the USEPA is based on the Delaney Clause of the Federal Food, Drug and Cosmetic Act Food Additives Amendment of 1958. This clause set a standard of zero risk to the public from carcinogenic food additives (eg, pesticides) that concentrate in processed foods. This was interpreted in terms of a “negligible” but nonzero lifetime cancer risk of 10−8, which was later increased to 10−6 due to pesticide measurement difficulties at levels corresponding to the lower risk. This lifetime cancer risk criterion and the concept of risk goals were later incorporated into various USEPA regulations (eg, CERCLA, Safe Drinking Water Act, Clean Air Act, and Resource Conservation and Recovery Act). This paradigm has two basic elements: a goal for acceptable risk and allowance for an increase (relaxation) in risks above the goal, based primarily on considerations of technical feasibility and cost.
The USEPA made the decision to regulate radiation the same way it regulates toxic chemicals for consistency purposes,
158
despite advice from the SAB describing problems with such an approach
159
: To many radiation scientists, reducing excess exposures much below 100 mrem/yr seems unnecessary and in any case exceedingly difficult to monitor for compliance because it is within the natural variability of background. The application of standard chemical risk-reduction criteria to radionuclides in these situations leads to limitations on excess radiation dose that are small in comparison to natural background radiation. “In calculating excess risk from human sources of a chemical, background levels, if any, are therefore frequently seen as irrelevant….” This is in marked contrast to radiation, which is universally distributed in the natural environment.
The USEPA treats inorganic metals differently than other chemicals. In the assessment of human risks from exposures to inorganic metals,
160
USEPA takes into account metals that are naturally occurring and vary in concentrations across geographic regions. According to USEPA, the implications of these properties include: Humans, other animals, and plants have evolved in the presence of metals and are adapted to various levels of metals. Many animals and plants exhibit geographic distributions that reflect variable requirements for and/or tolerance to certain metals. These regional differences in requirements and tolerances should be kept in mind when conducting toxicity tests, evaluating risks, and extrapolating across regions that differ naturally in metals levels.
The USEPA also acknowledges that some metals are essential for maintaining proper health of humans, animals, plants, and microorganisms. As a result, USEPA considers the following implications for risk assessment
160
: Adverse nutritional effects can occur if essential metals are not available in sufficient amounts. Nutritional deficits can be inherently adverse and can increase the vulnerability of humans and other organisms to other stressors, including those associated with other metals. Excess amounts of essential metals can result in adverse effects if they overwhelm an organism’s homeostatic mechanisms. Such homeostatic controls do not apply at the point of contact between the organism and the environmental exposure. Essentiality thus should be viewed as part of the overall dose-response relationship for those metals shown to be essential, and the shape of this relationship can vary among organisms. For a given population, ‘reference doses’ designed to protect from toxicity of excess should not be set below doses identified as essential. Essential doses are typically life-stage and gender specific.
These properties are analogous to those ascribed to radiation by the threshold and hormesis response models. An exception has been made to treat risk assessment for inorganic metals differently because of their essential characteristics or natural existence in background. Radiation has not been afforded the same consideration despite the similarities with inorganic metals. Instead, USEPA has stated, …as the purpose of a risk assessment is to identify risk (harm, adverse effect, etc.), effects that appear to be adaptive, non-adverse, or beneficial may not be mentioned.
161
(emphasis added) As a general principle, our practice is not to base risk assessments on adaptive, non-adverse, or beneficial events.
161
Applying this guidance to radiation risk assessment excludes any scientific evidence on potential benefits from radiation exposures simply by policy mandate. That introduces bias by allowing only information claiming support for the LNT model while prohibiting evidence that contradicts it. Excluding evidence of adaption or benefits, and only considering evidence of harm, is contrary to radiation protection philosophy as described by the ICRP. 162 National and international expert advisory bodies acknowledge adaptive and hormetic effects, and their consideration has even been formally included in new European standards for protection of the environment against radiation. 163
Regulating radiation the same way as toxic chemicals also does not take into account that risks from radiation exposure have been established based largely on observations in humans exposed to well-known individual doses, whereas chemical risks are more often based on projections from experiments on animals or human epidemiology that suffer from poorly characterized individual exposures. Since background radiation is an underlying factor that isn’t present for most toxic chemicals, the USEPA SAB acknowledged the existence of threshold models for radiation carcinogenesis (eg, the radium dial painters) or at least “practical thresholds” (eg, the idea that cancer latency was inversely related to dose such that manifestation of risks at low doses could be delayed so long that no cancers would occur during a normal lifetime). 156
Radiation protection philosophy is distinct from toxic chemical protection philosophy: The precautionary principle is an alternative risk management strategy that gives disproportionate weighting to technological risks. It is often summarized by the phrase ‘better safe than sorry’ and requires forgoing, postponing or otherwise limiting a product or activity until uncertainty about potential risks has been resolved in favor of safety. ALARA, on the other hand, treats risks and benefits on a level playing field. Accordingly there is no prescribed dose goal. The end result of an ALARA practice is a residual dose and risk that is considered acceptable.
164
The distinguishing hallmark of the ALARA philosophy is that interventions and radiation protection policies must be low, reasonable, and achievable. The USEPA application of the LNT model for determining risk and developing cleanup levels often result in very low numbers that are nearly three orders of magnitude below, where adverse effects are reliably observed and significantly lower than those recommended by national and international expert advisory bodies. For example, the USEPA suggests that radiation exposures above 3 × 10−4 risk (about 0.12 mSv/yr based on the LNT) is not protective of human health or the environment. 165
Soil radiological cleanup criteria required by USEPA’s preliminary remediation goals (PRGs), for example, as related to legacy uranium mining sites, are frequently within the statistical uncertainty of background and, in fact in some cases, less than natural background values. This often results in extensive remedial action costs with no demonstrable health benefits. In fact, cleanup standards as low as USEPA’s PRGs often cannot be satisfied with current analytical capabilities. This is an example of where the toxic chemical approach is not appropriate for naturally occurring radionuclides, since the background contains naturally occurring radioactive material, in some cases at levels that exceed the PRG values. Additionally, there are large variations in natural background depending on altitude and geographic location. 166 This is in stark contrast to the background of most chemicals of concern. 156 As mentioned earlier, even BEIR VII acknowledges that epidemiological data below 100 mSv (0.1 Sv) are not sufficient by themselves for risk estimation, yet the USEPA maintains policies that require cleanup to levels where no net benefit to human health or the environment can be detected.
The USEPA SAB recognized in 1992 156 that the USEPA Superfund policy documents, like the risk assessment guidance for Superfund, 167 were being developed to be more consistent with the chemical risk paradigm. In contrast, it also noted that the USEPA radon policy was applying a rule of practicality based on the difficulty of reducing radon levels below 150 Bq/m (4 picocuries/L) within a reasonable budget. The associated risk for its radon policy translates to a lifetime risk of over 1 in 100 for an average person 168 based on the LNT model. More recently, USEPA’s approach to radon regulation has been challenged. 169
Should the Current USEPA Regulatory Radiation Policies Be Reconsidered and Harmonized With the Radiation Protection Philosophy Given the Lessons Learned From Fukushima?
The NCRP issued reports providing guidance on responding to a radiological or nuclear terrorism incident
170,171
and decision-making for late-phase recovery from nuclear and radiological incidents.
172
These recommendations from the NCRP endorse the strategy laid out by the ICRP
173
and apply them to the situation in the United States. This new strategy presents a: marked contrast to the current clean-up approach carried out under statutory regulatory provisions that focuses on radiological risk, precautionary decision making, and clean-up goals close to background.
170
The ICRP suggests that the reference level should be selected in the lower part of the 1 to 20 mSv/yr range (100-2000 mrem/yr 173 ). This is much more realistic and achievable than the LNT 10−6 risk-based PRGs developed by USEPA, which are approximately 2 to 3 orders of magnitude lower than other guidance provided by NCRP and ICRP.
Although the simplicity of the LNT model used for risk assessment has traditionally been thought to be reasonably conservative, its application has led many to believe that any amount of radiation brings unwarranted risk. This contributes to society’s response to make personal decisions to avoid any radiation exposures at all costs, thus potentially resulting in more societal harm than good. It also drives down cleanup levels, resulting in extraordinary cleanup costs. Furthermore, USEPA has provided guidance stating “approaches that do not follow the remedial program’s policies and guidance should not be used at CERCLA remedial sites.” 158 It specifically targets any guidance developed by other federal, state, or tribal agencies or by international or national organizations (eg, ICRP, NCRP, and other scientific or professional organizations) and leaves only USEPA guidance available for consultation.
A recent example of where LNT-based guidance may have caused more harm than good is the evacuation in Fukushima, Japan. 174 The Fukushima accident involved no deaths directly related to radiation exposure 175 ; however, the evacuation itself caused increased mortality primarily among the elderly individuals. 176 –178 Well over a thousand people died from causes related to the evacuation, 179 and the continued exclusion of residents from their homes for extended periods of time. This occurred in spite of the fact that “no significant contamination was found in the patients evacuated from the 20 km zone despite the fact that 48 h had passed between the first explosion and their evacuation.” 180 During the Fukushima incident, the public exhibited distrust of radiation experts and confusion regarding what risks radiation from the accident actually presented. 181 The population that evacuated from the area around the Fukushima plant is now at increased risk for mental health problems and other social and psychological problems because of their continued exclusion from their homes, and they are subject to social stigma. 181,182
The application of the LNT to estimate cancer risks associated with residual contamination, without appropriately considering the uncertainties involved (ie, LNT predictions represent an upper bound estimate of risks, and real risks might in fact be 0), has contributed to continued exclusion of the evacuated Fukushima population from their homes. The same situation occurred at Chernobyl. 183 In addition, recent research has indicated that even when hypothetical radiation risks from residual radioactive contamination are calculated via the LNT model, mass evacuations and relocations like those following Chernobyl and Fukushima have been unjustifiably extensive 184,185 and are almost never part of the optimal response strategy. 174,186,187 Therefore, it is reasonable to question the perceived protectiveness of the LNT model for setting protective standards in LDDR radiation environments. 72 The long-term response to the Fukushima accident will undoubtedly involve, and in fact emphasize, providing accurate information about radiation risks to returning residents and dealing with their fears. 188,189 These fears are exacerbated by strident statements that “there is no safe dose” and “doses outside the USEPA risk range are not protective” and by inaccurate and incomplete information about the uncertainties involved in estimating risks from very low residual radiation doses. 190
While some of the remedial strategies in response to the Fukushima accident have been retrospectively analyzed and determined to be justified based on an LNT calculation of risk from residual contamination, 191 others response measures have been found to be unjustified. 192 Unrealistic cleanup standards, which fail to properly account for the real possibility that risks from such low doses, may very well be zero, exacerbate public fears, fail to optimize response strategies by ignoring the economic and public health consequences of these actions, 193 and can distort the allocation of resources in the recovery effort. The mission of the USEPA is to protect human health and the environment. The mission of the US Public Health Service is to protect, promote, and advance the health and safety of our nation. Both the USEPA and the USPHS develop policies to accomplish these missions. Although it is acknowledged that the determination of acceptable risk values is a matter of judgment and risk management policy, 194 the USEPA Scientific Integrity Policy explicitly states that science forms the backbone of its decision-making. 195 The science behind low-dose risk estimation and determining cleanup levels is showing that the LNT has the real potential to cause more economic, environmental, and public health harm than good to society.
A comprehensive review of the application of ICRP guidelines and the problems encountered at Fukushima has been documented
196
and offers many lessons. Among the highlights are the following: It has been noted that the uncertainties surrounding the crisis itself, in addition to the absence of demonstrated risk at the tiny exposures to the population and the uncertain validity of the linear extrapolation of risk down to such tiny doses, raise serious questions about whether these calculations could provide even an order-of-magnitude guess as to possible health consequences. Further, given the wide range of uncertainties in the risk models used, it is likely that zero effects should be included as a lower bound to the estimates, or even as a central estimate of the likely future effects. These hypothetical computations of effects are based on assumptions that cannot be validated because the estimated doses are substantially below the level where epidemiology has the ability to detect increases above the natural occurrence. The large number of deaths reported following these theoretical predictions, especially when not contrasted with the normal high occurrence of death, is alarmist and unfounded and has caused severe anxiety and emotional distress in the Japanese population. It should be recognized, however, that ‘balancing’ good and harm is not confined to issues associated with radiation exposure. Other non-radiation-related benefits and detriments arising from the protective action must also be considered, thus going far beyond the scope of radiological protection. (emphasis added)
Fukushima and Chernobyl offer very rare opportunities to learn from the application of radiation protection guidance and strategies in challenging, real-world situations. A frank assessment of the successes and shortcomings of these strategies and how they may impact the agency’s cleanup policies is necessary.
The USEPA has taken the position that any residual contamination concentration exceeding the upper risk range of 3 × 10−4 (a dose of about 0.12 mS/yr [12 mrem/yr]) is “not protective.”
165
Is this a valid interpretation, given the very different advice given by the ICRP? Gonzalez
196
state: Thus, the public has doubts about what type of exposure the inhabitants of the rehabilitated area will be subject to when the rehabilitation starts. If these people are regarded as members of the public and if the exposure situation is regarded as a planned one, the dose limit of 1 mSv year-1 and the corresponding dose constraint could in principle be considered as applicable, therefore requiring annual doses to the residents to be kept below a few tenths of a millisievert, a restriction that might be considered unrealistic and furthermore rather strange and unreasonable.
196
(emphasis added) There was a particular misunderstanding about the appropriate use and application of the dose value of 1 mSv year-1. The public tended to regard a dose above this value as dangerous, which created challenges in coping with the aftermath of the accident. The fact that there is little convincing evidence for human health effects below 100 mSv year-1 (or 100 times the dose limit) appeared to hold little sway over the level of concern.
The USEPA’s interpretation is clearly at odds with the views of the ICRP, which stated, The Commission’s recommended limits are set at a level which is thought to be associated with a low degree of risk; thus, unless a limit were to be exceeded by a considerable amount, the risk would still be sufficiently low as not to warrant such countermeasures as would themselves involve significant risks or undue cost. It is therefore clear that it is not obligatory to take remedial action if a dose-equivalent limit has been or might be exceeded.
197
(emphasis added)
In answer to the question, “Is any Amount of Radiation Safe?,” USEPA has explained, In setting limits, USEPA makes the conservative (cautious) assumption that any increase in radiation exposure is accompanied by an increased risk of stochastic effects.
58
Similarly, USEPA has explained, LNT also has the great advantage of simplicity, risks from multiple exposures being proportional to the total dose. Given these features of protectiveness and convenience, there is very wide support for LNT in the context of radiation protection, even among scientists and regulators who harbor serious doubts about its scientific validity.
5
Note that these explanations are based on the assumption that LNT is “conservative” and “cautious.” In light of the Fukushima experience, these assumptions are no longer tenable. Others have argued that radiation protection guidelines are confusing and overly stringent, based on the application of LNT at doses far below where risks can actually be observed, and that this had directly observable negative public health consequences. 9,72
Discussion
In the event of a large-scale domestic radiological dispersal device (RDD) attack, nuclear power plant (NPP) release, or an improvised nuclear detonation (IND), the long-term cleanup challenges will likely have a larger impact on the surrounding communities, cities, and regions, where factors other than potential radiation exposure may become the driving force behind the final cleanup levels. For example, psychosocial, economic, and speed-of-recovery issues all affect the long-term viability and survivability of the affected area. Risks associated with moving an entire population on a temporary or permanent basis may be higher than allowing some low-level exposures from residual contamination. Nondestructive cleanup technologies may prove to be too costly or applicable to only small portions of the recovery effort. Overall costs could become so expensive as to reduce the ability to protect human health and the environment if there are limited resources. Given the potential scope and urgency of the situation following an RDD/NPP/IND scenario, the preference to work toward an acceptable cleanup level (radiation risk paradigm) rather than having to raise a preliminary cleanup goal (chemical risk paradigm) has many political, economic, and societal benefits.
Both radiological and chemical risk paradigms warrant equal consideration when making cleanup decisions. The radiation risk paradigm was included in the Department of Homeland Security guidance with USEPA and other federal agencies’ concurrence. The chemical risk paradigm is routinely used at USEPA superfund sites. Both employ risk-based methods and can lead to similar cleanup levels. However, risk is a metric that cannot be measured; only radiation exposure or radioactive surface contamination can be directly measured. Using the USEPA PRG calculators to meet the CERCLA, risk range suggests that the agency knows the risk with a much greater certainty than is scientifically possible. These are based on the LNT model and are inconsistent with the guidance from UNSCEAR, HPS, World Health Organization, and many others. They are tools that foment fear and uncertainty in the affected communities. Instead, a dose-based cleanup approach is more scientific and practical.
There is precedent for the USEPA to quickly change policy based on SAB recommendations. In 1992, the USEPA SAB changed its earlier 1988 recommendation from averaging the radon risk estimates from BEIR IV and ICRP 50 to just using those published in BEIR IV. 198 Recent findings from the ongoing Life Span Study and other peer-reviewed articles as late as 1990 were used to justify this change. This change to the USEPA’s radon risk assessment policies is consistent with the goal and objectives of the existing USEPA Scientific Integrity Policy, which requires science to be the backbone of agency decision making. 195 Perhaps, findings or recommendations from a new USEPA SAB review will serve to justify changes to the agency’s existing policies on the use of the LNT model in LDDR radiation environments.
Conclusions
The USEPA is the lead federal agency responsible for protecting human health and the environment from hazardous agents. It carries out this mandate by applying scientific information to promulgate regulations and policies that other federal agencies (eg, NRC and DOE) and states incorporate into their regulations or policies where appropriate or applicable. Thus, the USEPA has a tremendous responsibility to ensure its radiation regulations, policies, and guidance are scientifically sound while providing adequate protection without placing an unnecessary burden on the affected population or organizations subject to them. An objective and unbiased reliance on scientific information to inform decision-making is an integral part of the agency’s scientific integrity policy. It sets the foundation for objective discussions among all the affected stakeholders (eg, public, industry, professional organizations, international communities) for determining (1) what are acceptable radiation regulations and policies associated with determining cleanup levels following a large-scale radiological or nuclear incident and (2) what risk assessment model should be used to best represent the risks from LDDR radiation environments when a residual low-level contaminated environment becomes reality.
The scientific understanding of the effects of radiation exposures has evolved since its discovery in the late 19th century. The scientific information supporting the use of the LNT model for LDDR radiation environments developed over that past 70 years but is mainly extrapolated from HDDR environments. The application of the LNT model to determine health risks has created a culture where a few clicks on a radiation dose rate meter equate to cancer in the minds of the public. Society has become so fearful of radiation that unnecessary steps are taken, and other risks are accepted, to avoid even trivial radiation exposures at all costs. This includes potentially life-saving medical examinations, which is recognized as a problem by the many scientific and professional organizations specializing in radiation.
Since the Three Mile Island Nuclear Power Plant accident in 1979, the world has experienced several large-scale nuclear or radiological accidents (eg, Chernobyl, 1986; Goiania, 1987; Fukushima, 2011), affecting millions of people and contaminating millions of hectares of land. The 2011 Fukushima NPP accident is the most recent radiological accident. The accident itself caused no radiation-related deaths 175 ; however, the evacuation in response to the accident, combined with the extended exclusion of area residents from their homes, has increased mortality from various stress-related causes. The elderly individuals are especially vulnerable to these effects, 176 –178 and over 1600 people died as a result 179 of the response to the Fukushima accident. A retrospective evaluation has concluded that the risk from the evacuation outweighed any hypothetical risk of radiation exposure calculated using the LNT model, 184,185 particularly among the elderly individuals, 199 the evacuation did not protect human health, and was therefore unethical. 200
Scientists and society continue to learn from these events by questioning how we can strengthen our resilience, reduce the time it takes to resume normal lifestyles, maintain economic viability, and minimize adverse psychological effects. The scientific literature is showing, and scientific organizations acknowledge, that adverse health effects from LDDR radiation exposures are not detectable and that there may be a threshold or even a beneficial effect. These findings contradict the use of LNT model-based predictions.
It is time for the USEPA to reconsider the use of the LNT model in LDDR radiation environments in the regulatory process, especially in the tools it has developed to determine cleanup levels. Change does not occur quickly or easily within government frameworks. It took decades of institutional inertia to arrive at the current regulatory framework. The USEPA SAB recommended “change in the agency culture, change in how the agency works, and increased support for scientists and managers in programs and regional offices responsible for science integration” 201 to occur and thereby improve its regulations and policies. Despite these recommendations by the EPA SAB, there’s been no change in the agency’s posture or policy associated with using the LNT model for risk assessment and determining cleanup levels in LDDR environments, nor a desire to have it reevaluated by the SAB for more than 20 years.
Objectively evaluating and incorporating the latest scientific evidence on LDDR dose–response relationships for application to the regulatory and policy-making process for risk assessment purposes will (1) ensure science remains the foundation for its decision making, (2) reduce the unnecessary burden of costly cleanups, (3) provide a much needed platform to educate the public on the risks or benefits from LDDR radiation exposures, and (4) harmonize the agency’s policies with those recognized by the rest of the radiation scientific community. A continued resistance to conducting a comprehensive review of the latest science regarding LNT-based policies will only diminish the agency’s credibility and influence to protect human health and the environment.
Footnotes
Authors’ Note
The views expressed in this article are those of the author(s) and do not necessarily reflect the views or policies of the US Public Health Service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.