
Abstract
Background:
Complications of thumb basal joint arthritis surgery include surgical wound pain and cheiralgia paresthetica through involvement of the radial nerve superficial branch (RNSB). The aim of this study is to compare the risk of nerve injury between anterolateral and dorsal approaches to the first carpometacarpal joint (1CMCJ) by measuring the distance between the incisions and RNSB, recording crosses between them, and evaluating the density of skin nerve endings at incision sites.
Methods:
In this descriptive study of 20 cryopreserved cadaver specimens, the anatomical distribution of the RNSB and its relationship with 1CMCJ anterolateral and dorsal approaches were determined by macro-dissection, and histomorphological analysis and digital imaging were used to measure cutaneous nerve ending density at the 1CMCJ and incision sites.
Results:
In comparison to dorsal approach, the minimum distance from the RNSB was significantly shorter (1.30 ± 1.94 mm vs 3.70 ± 2.71 mm), and the total number (16.60 ± 8.50 vs 9.97 ± 7.51) and density (2.00 ± 0.83 vs 1.29 ± 0.77 mm2) of nerve endings were significantly higher with anterolateral approach. With the anterolateral approach, more nerve structures were observed in the distal versus proximal section of the incision, although the difference was only close-to-significant.
Conclusion:
The incision is closer to the RNSB pathway with Wagner’s anterolateral approach than with Gervis’ dorsal approach, crossing with nerve branches in 50% of cases. The density of nerves is higher in the skin overlying the anterolateral versus dorsal aspect of the carpometacarpal joint. The risk of neuropathic wound pain after 1CMCJ surgery could be higher with the anterolateral approach, which should therefore be avoided.
Keywords
Introduction
Complications of open or arthroscopic surgery of the first carpometacarpal joint (1CMCJ) include wound pain and complex regional pain due to involvement of the radial nerve superficial branch (RNSB).1-5 However, their prevalence among patients undergoing thumb basal joint arthritis surgery is not always reported in published case series. We hypothesized that the site of the surgical wound might influence the risk of these complications.
Open surgery of the 1CMCJ is usually performed via a dorsal or anterolateral approach. 6 In the dorsal approach, described for trapeziectomy by Gervis in 1949, 7 the incision extends from the proximal two-thirds of the first metacarpal to the distal third of the trapezium, posing a potential risk to the integrity of the radial artery and/or RNSB. 8 In the anterolateral approach, proposed for Bennett’s fracture-dislocation by Wagner in 1950, 9 the incision is performed at the junction between palmar and dorsal skin overlying the 1CMCJ, and it also involves a potential risk of RNSB injury and postoperative dysesthesias. 6 To our best knowledge, no published study has compared the risk of RNSB injury between dorsal and anteroposterior approaches to the 1CMCJ.
The objective of the present descriptive study in cadaver specimens was to compare the risk of iatrogenic nerve injury and surgical wound pain between dorsal and anterolateral approaches to the 1CMCJ, examining the proximity of incisions to the RNSB pathway and using histomorphometry and digital imaging analysis to compare the density of skin nerve endings at incision sites.
Materials and Methods
This anatomical and histomorphometric descriptive research study was approved by the Biomedical Research Ethics Committee of Andalusia in April 2023 (Annex I; supplementary material). All studied individuals had given their informed consent to the utilization of their remains for scientific purposes.10,11
The study used 20 forearm-and-hand specimens (11 left-side, 9 right-side) from 15 cryopreserved cadavers (7 men) aged between 52 and 78 years at death. No specimen had any history of wrist surgery or injury. All specimens were defrosted at room temperature and dissected in the Department of Human Anatomy of the University of Medicine of Granada (Spain) between October and December 2023.
Anatomical Study
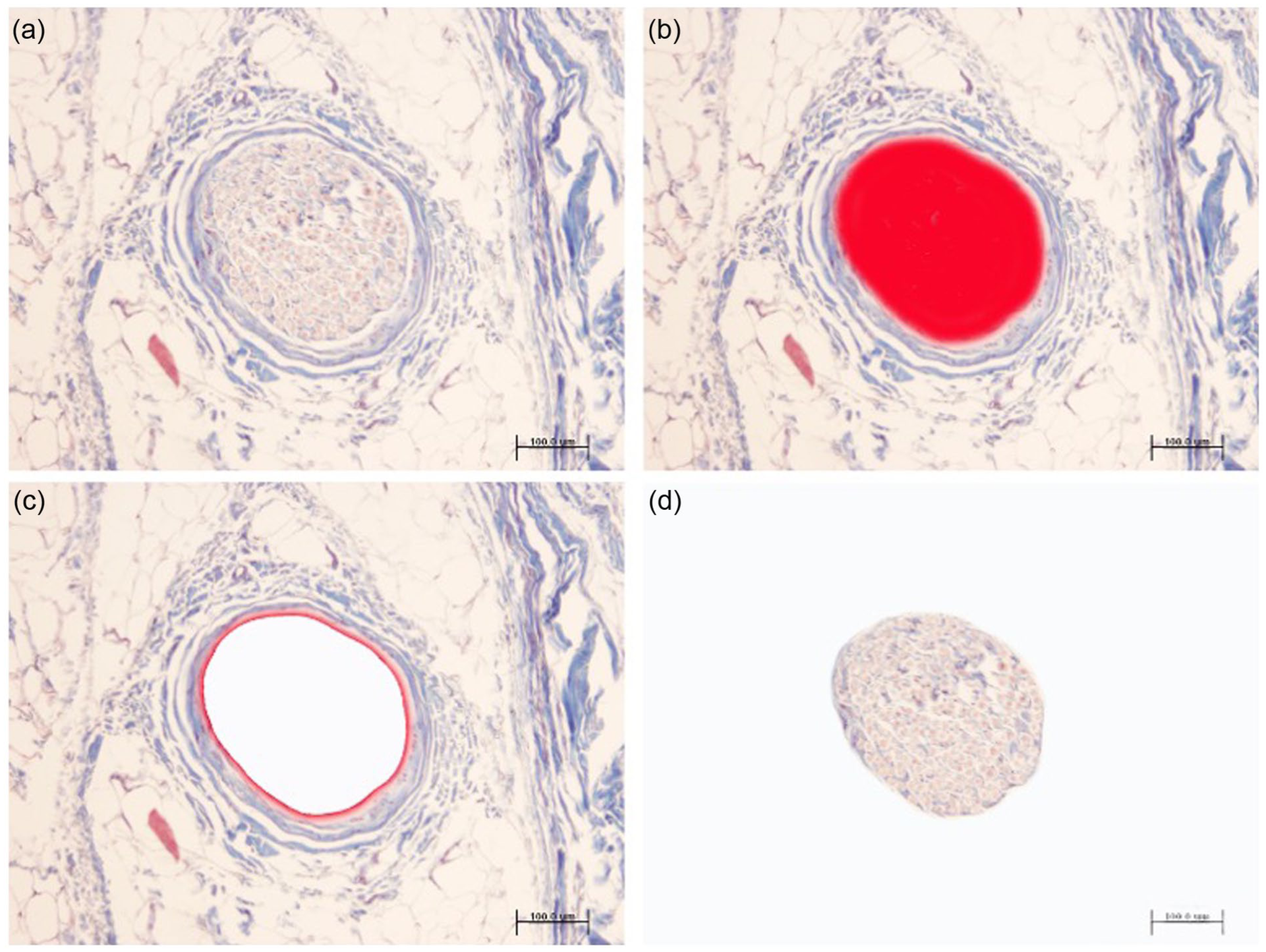
On 10 specimens, indelible ink was used to mark the styloid radial process, trapezium, first metacarpal bone, and the theoretical incisions for anterolateral and dorsal approaches to the 1CMCJ. An incision was performed in the lateral aspect of the forearm to identify the RNSB (Figure 1a).

Cadaver specimen dissection.
A scalpel was used to elevate the skin of the radial aspect of wrist and hand en bloc with the subcutaneous cell tissue (Figure 1c). The RNSB was dissected with the subcutaneous cell tissue facing upward under ×3.5 magnification loupes, individualizing and labeling each branch with black Indian ink.
Superimposed images of the 1CMCJ, RNSB, and incisions were drawn on paper for each specimen (Figure 2). Two independent examiners (IPGV and NMM) used a millimeter ruler to measure the minimal distance from the incisions to the RNSB.
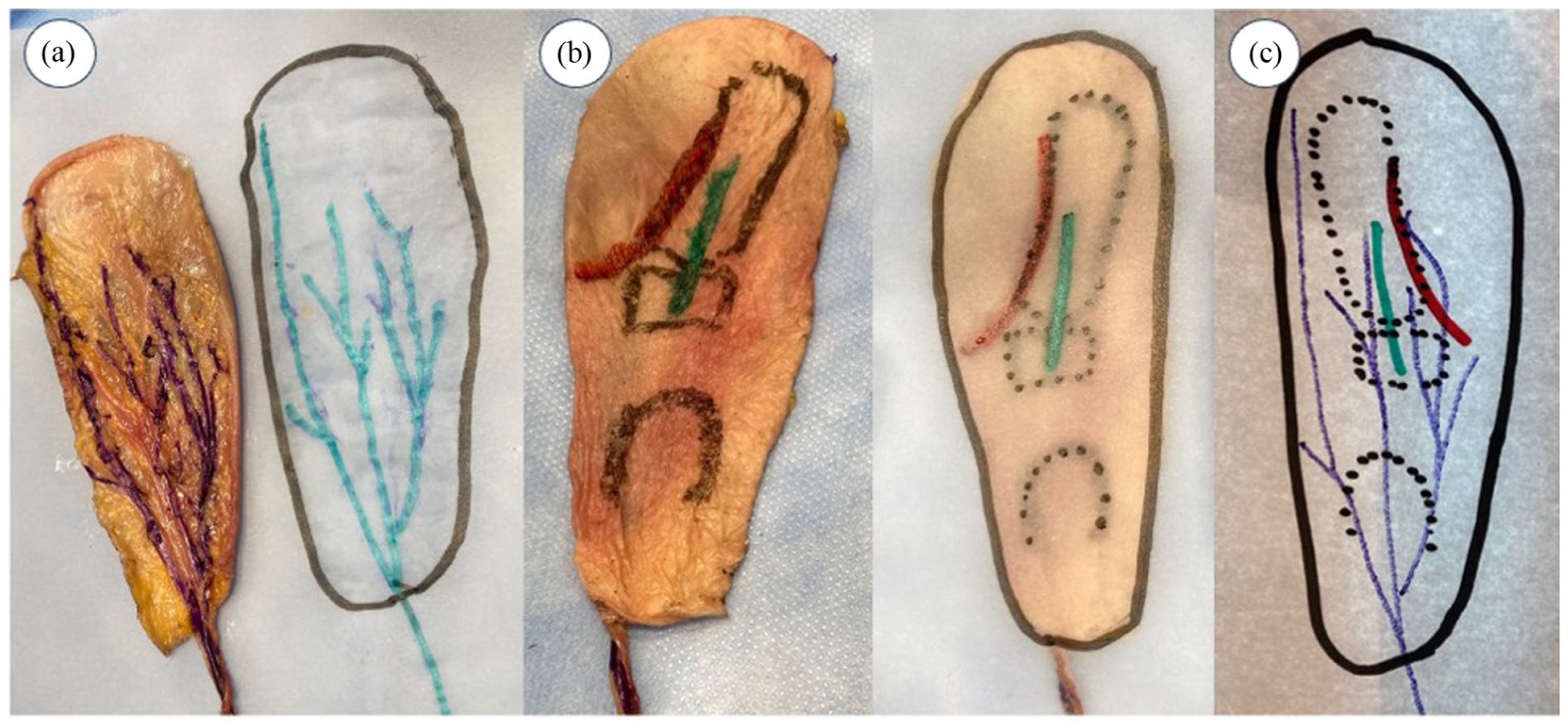
Procedure for studying the topographic relationship between the radial nerve superficial branch (RNSB) and the anterolateral and posterior incisions.
Histomorphological Study
A skin sample from each incision (anterolateral and dorsal) was taken from 10 forearms for histologic study. After fixing each sample in 10% buffered formalin for 48 hours at room temperature, it was divided into 2 proximal sections (P1 and P2) and 2 distal sections (D1 and D2) (Figure 1c). These were paraffin-embedded using an automatic tissue processor (model TP1020, Leica Biosystems, Danvers, Massachusetts) and then cut into 4-μm longitudinal sections with a manual microtome (Minot HistoCore-BICOUT, 149BIO000 C1, Leica Biosystems). Tissue sections were deparaffined and rehydrated in successive baths of xylol, 100% ethanol, 95% ethanol, 75% ethanol, 50% ethanol, and distilled water. They were then stained with hematoxylin-eosin and Masson’s trichrome.
The total number of nerve endings was counted in each skin sample, calculating the density (per mm2). A millimetric scale in the ×40 objective lens of an Olympus BH 2 microscope (Olympus Optical Company, Tokyo, Japan) was used to count the nerve structures in each sample (Figure 3). Counts were performed by 2 independent researchers (IPGV and JTU), using the mean values obtained. Results were expressed as nerve endings/mm2 according to the following formula:
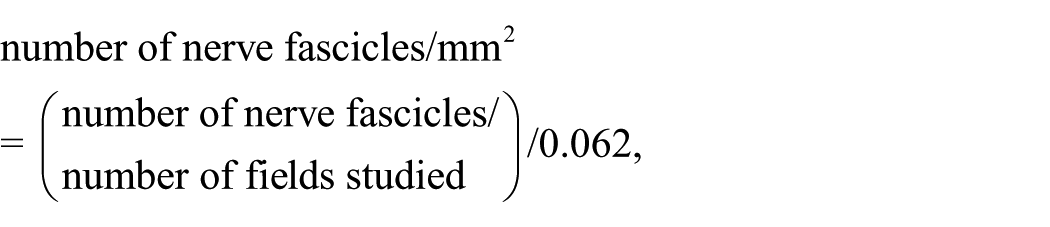
Count of nerve elements on a millimetric scale in the ×40 objective lens of the microscope.
Digital Imaging Analysis
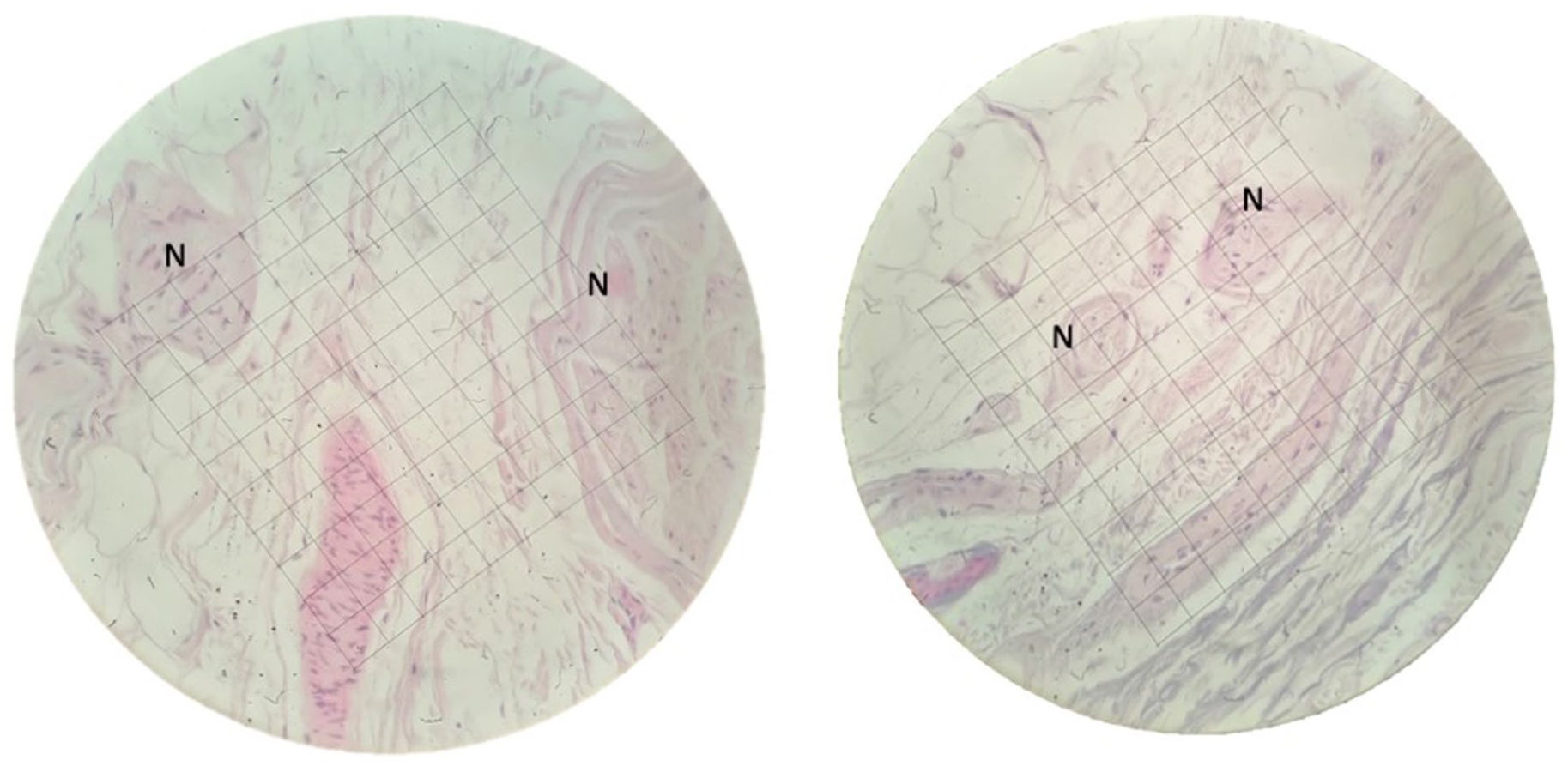
The percentage area occupied by nerve structures was studied under an Olympus BX43 microscope (×20 objective) equipped with an Olympus DP70 digital camera connected to a computer, using ImageJv. 1.48 software (http://rsb.info.nih.gov/ij/). The total sample area was measured with a Nikon camera coupled to a Zeiss Axiophot microscope (×1.5 objective), using the ImageJv program. The percentage area corresponding to nerve structures was calculated in each sample (Figure 4).
The area occupied by nerve structures was studied under an Olympus BX43 microscope (×20 objective) equipped with an Olympus DP70 digital camera connected to a computer, using ImageJv.1.48.
Statistical Analysis
SPSS for Windows version 23.0 (IBM SPSS Inc.) was used for statistical analyses. The number and density of nerve endings and the percentage surface area occupied by the nerve were expressed as means with standard deviations. Application of the Kolmogorov-Smirnov test confirmed the normal distribution of quantitative variables. The Student t test was used to compare between the 2 sections, and the χ2 test was used for qualitative variables. P value less than .05 was considered significant in all tests.
Results
Anatomical study. Table 1 exhibits the results of the anatomical study. The RNSB was defined as Pattern A if it had 2 branches and Pattern B if it had 3 or more branches. The RNSB branch pattern type had no influence on the frequency of intersections with either anterolateral or dorsal approaches (Student t test; P = .527). There was no statistically significant difference between approaches in the number of intersections with the RNSB (Student t test; P = .325). However, the minimum distance to the RNSB was significantly lower (Student t test; P = .035) with the anterolateral versus dorsal approach (Table 1).
Histomorphometry. Nerve quantification and total density of nerve endings. Table 2 displays the results obtained. The total number of nerves and the density of nerve endings were significantly higher with the anterolateral versus dorsal approach (Student t test; P < .001 for both) (Table 3). The number of nerves, density of nerve endings, and percentage area occupied by nerve structures did not differ between the distal and proximal sections with the dorsal approach (Student t test; P = .954, P = .892, P = .776, respectively) or with the anterolateral approach, although the differences in density and percentage area were close-to-significantly higher in distal versus proximal sections with the latter (Student t test; P = .101, P = .541, P = .068, respectively) (Table 3).
Results of the Anatomical Study.
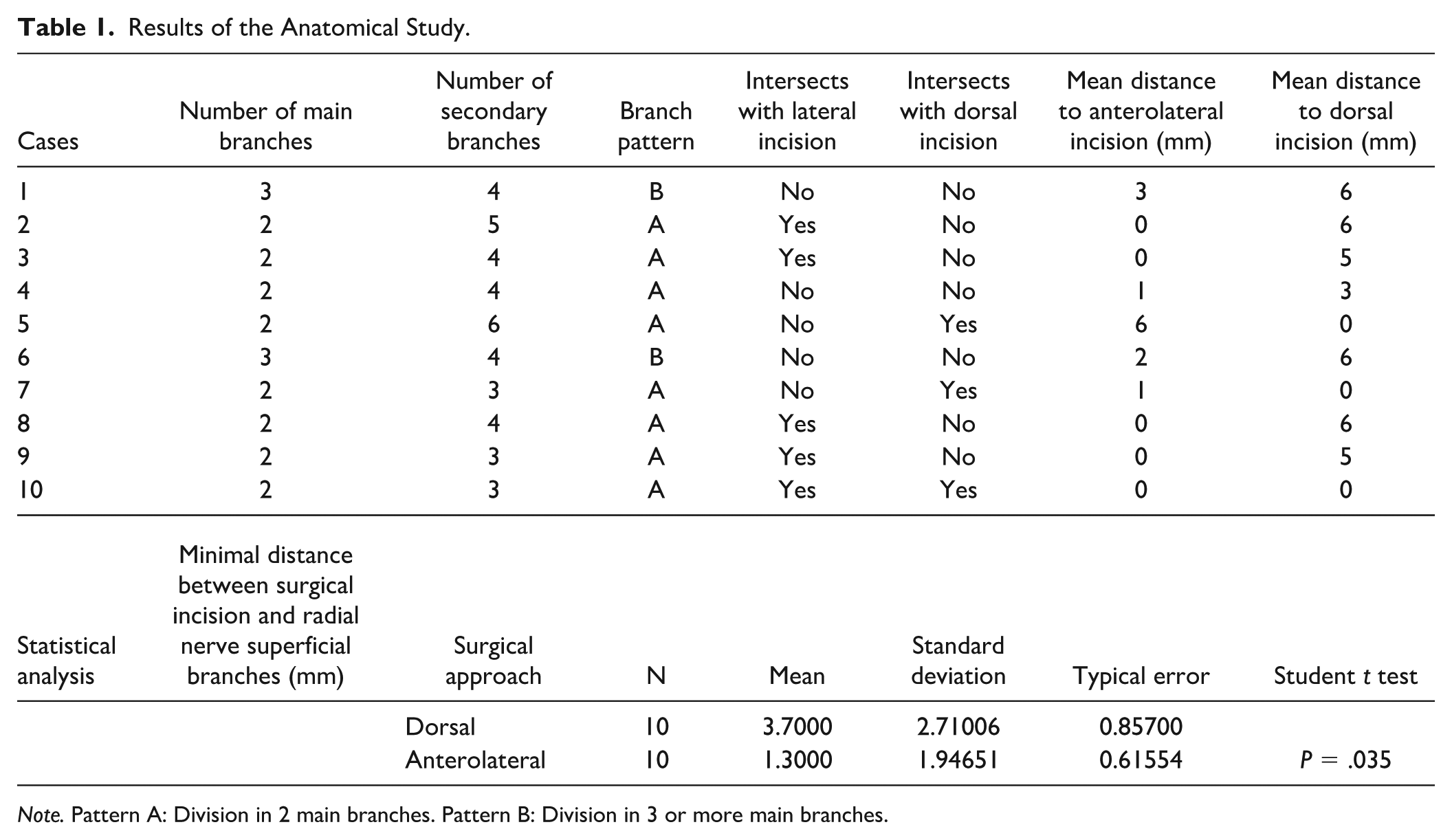
Note. Pattern A: Division in 2 main branches. Pattern B: Division in 3 or more main branches.
Results of the Histomorphometric and Digital Imaging Analyses.
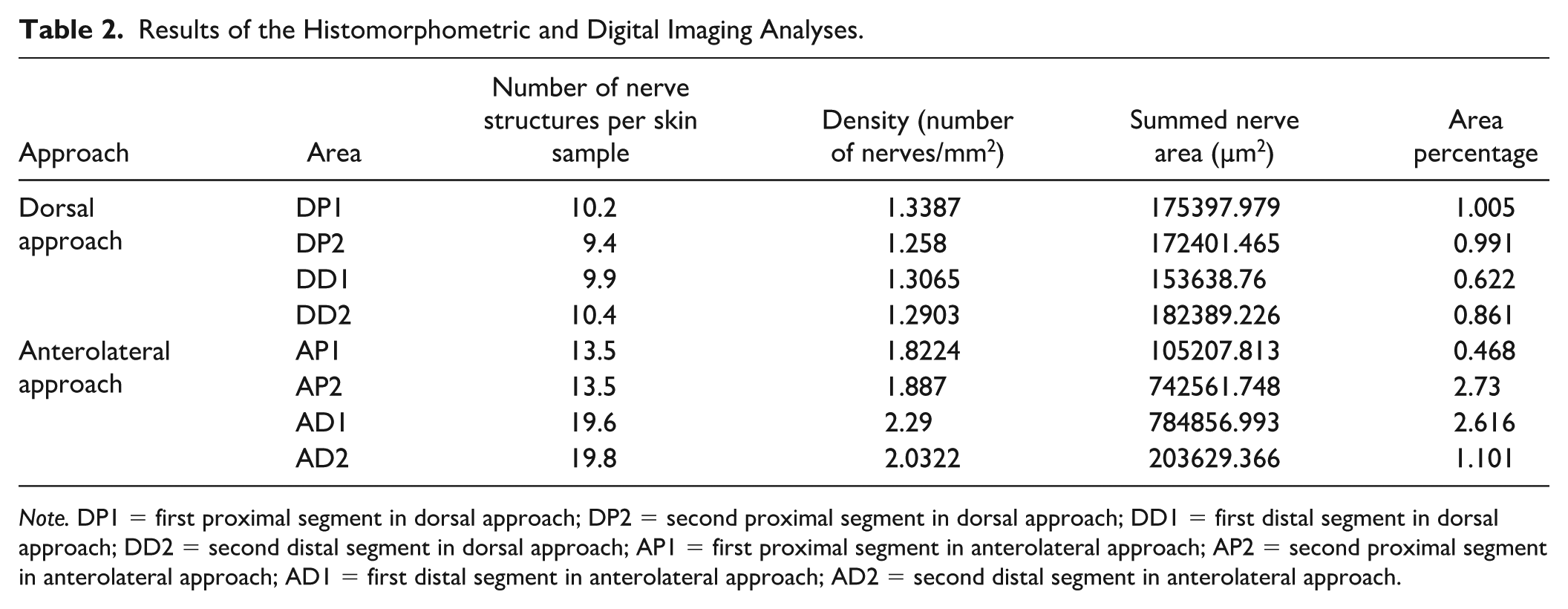
Note. DP1 = first proximal segment in dorsal approach; DP2 = second proximal segment in dorsal approach; DD1 = first distal segment in dorsal approach; DD2 = second distal segment in dorsal approach; AP1 = first proximal segment in anterolateral approach; AP2 = second proximal segment in anterolateral approach; AD1 = first distal segment in anterolateral approach; AD2 = second distal segment in anterolateral approach.
Comparison of the Total Number of Nerves, Nerve Ending Density (Number of Nerve Structures Per mm2), and Percentage Area Occupied by Nerve Structures Between Anterolateral and Dorsal Incisions.
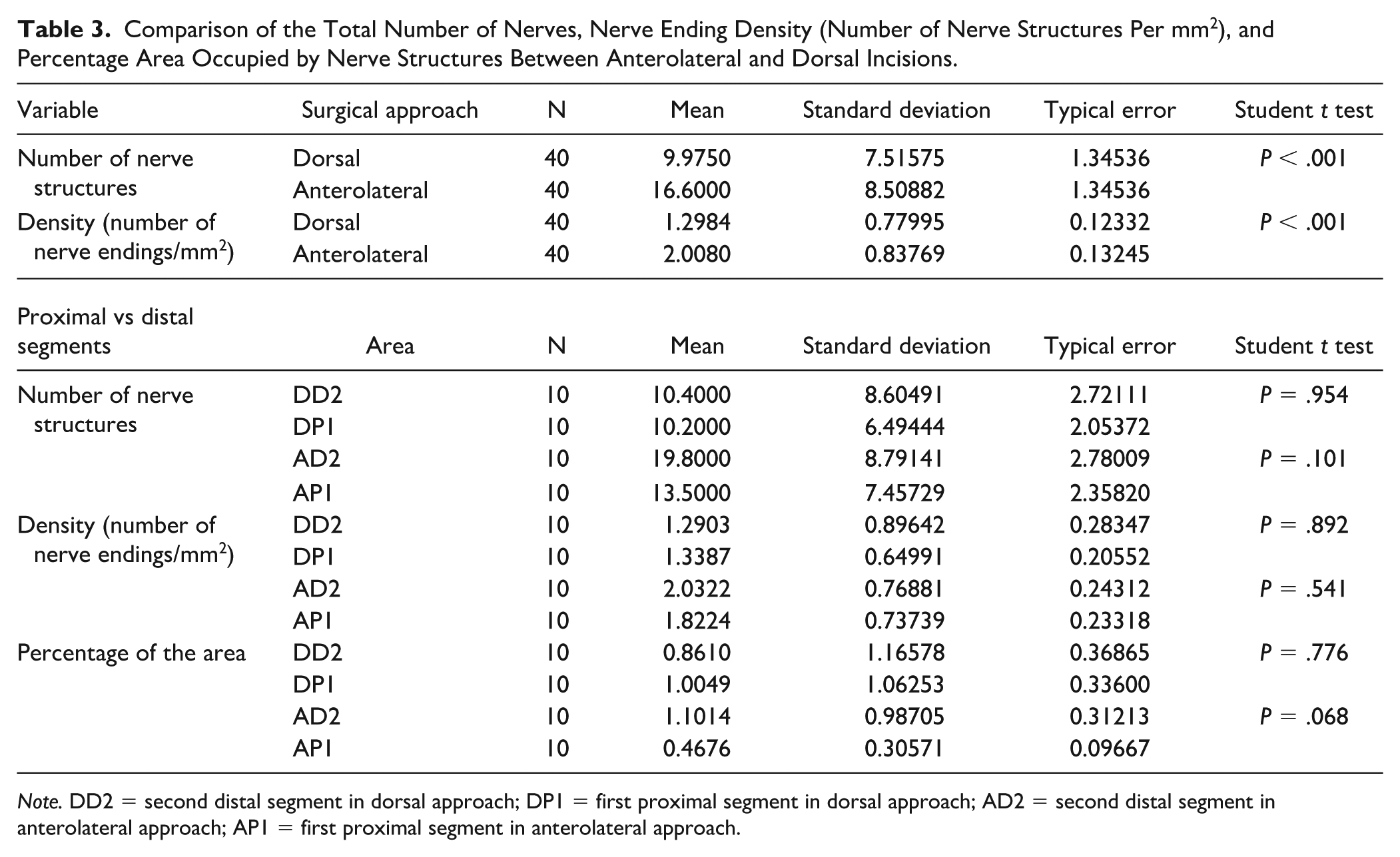
Note. DD2 = second distal segment in dorsal approach; DP1 = first proximal segment in dorsal approach; AD2 = second distal segment in anterolateral approach; AP1 = first proximal segment in anterolateral approach.
Discussion
The optimal surgical approach offers the best view and exposure of the structures to be treated while posing the lowest risk of injury to adjacent tissues. To our best knowledge, this study provides the first comparison of this risk between the dorsal and anteroposterior approach to the 1CMCJ, based on anatomical examination of the RNSB and histomorphometric study of the nerve density at incision sites. The main finding was that the minimum distance between incision and RNSB was significantly lower with the anterolateral versus dorsal approach and the number of nerves and density of endings were significantly higher. In addition, the density of nerve endings and the percentage area corresponding to nerve structures appeared to be higher in distal versus proximal sections with the anterolateral approach, although the differences were only close to significant, possibly due to the limited sample size. With the dorsal approach, distal and proximal sections did not differ in number of nerves, nerve ending density, or percentage area occupied by nerve structures, which may suggest that the dorsal incision could be distally extended without increasing the risk of RNSB damage. These findings differ from the observations by Belcher and Nicholl 12 and Ritchie and Belcher 13 of a higher frequency of complications with dorsal versus lateral incisions.
Most anatomical studies designed to identify the surgical incision trajectory with the lowest risk of nerve injury have been based on macro- and microscopic dissection of peripheral nerves in the areas of interest.14-22 The main strength of the present investigation was the incorporation of histomorphometric and digital imaging analyses to evaluate not only the number and distribution of nerves but also their density and size.
First carpometacarpal joint innervation is known to be based on the RNSB, 23 and a study of 10 cadavers by Lorea et al 24 found that it also involves thenar and palmar cutaneous branches of the median nerve and the external cutaneous antebrachial nerve (ECAN). Connections between the RNSB and ECAN were also described by Abrams et al, 25 Ikiz and Üçerler, 26 and Mackinnon and Dellon 27 (reporting a high frequency [70%] of communicating branches). Although Robson et al 28 highlighted the relationship between the RNSB and the cephalic vein, we do not believe that this negatively impacts on 1CMCJ surgery outcomes.
The present findings are in line with previous reports of the entry of the RNSB into the subcutaneous layer at a mean of 9.0 cm proximal to the radial styloid between the tendons of the brachioradialis and the extensor carpi radialis longus 25 and of its bifurcation into 2 major branches at approximately 5 cm proximal to the radial styloid.25,26,28-30
In the present study, 8 out of 10 specimens had 2 main RNSB branches and the other 2 had 3 or more branches. Likewise, a study of 48 arms by Ikiz and Üçerler 26 found that the RNSB had 2 main branches in 44 arms (91.67%) and 3 main branches in only 4 (8.33%), while Abrams et al 25 observed 3 main branches in only 15% of cases. At any rate, the risk of intersection did not appear to be influenced by the RNSB distribution pattern in either surgical approach under study.
Widely varied reports have been published on the incidence of neuropathic wound pain after 1CMCJ surgery, and no definitive criteria have been established. Kleinman and Eckenrode 31 studied 40 patients who underwent trapeziectomy via an anterolateral approach and described persistent wound pain in 2 of these, including one with iatrogenic RNSB injury. In a follow-up study by Dhar et al, 32 pain was reported in 11 out of 39 hands treated 6 years earlier with a simple trapeziectomy. Belcher and Nicholl 12 observed neuroma and reduced sensitivity in 4 out of 43 patients at 13 months after trapeziectomy via a dorsal approach. Davis et al 33 studied 62 patients who also underwent trapeziectomy via a dorsal approach and described wound pain in 5 and symptoms of RNSB dysfunction in 12 at 3 months, although these complications persisted in only 6 patients at 1-year postsurgery. In a retrospective study of 100 thumbs, Weilby 34 reported 3 permanent and 5 transient cases of RNSB injury after trapeziectomy using a modification of Wagner’s anterior approach with an oblique incision over the thenar eminence. There is a need for prospective studies with strict diagnostic criteria to establish the frequency of RNSB injury in these cases.
Durand et al 35 explored the relationship between neurovascular structures and incisions in arthroscopic trapeziectomy with tenosuspension. They examined 3 approaches in 15 cadavers with thumb basal joint arthritis: an ulnar portal at the ulnar border of extensor pollicis brevis tendon, a radial portal at the midline between flexor carpi radialis tendon and the abductor pollicis longus, and a novel transosseous portal at the base of the first metacarpal (“trans-M1” approach). Neurovascular structures at risk were found to be the radial artery with the ulnar portal, branches of the superficial branch of the radial nerve with all portals, and the ending of the lateral cutaneous nerve of the forearm with the radial and “trans-M1” approaches. Other authors have reported a high risk of nerve injury with approaches at the radial border of the abductor pollicis longus36,37 or radial margin of the carpal radial flexor tendon. 38 The present results are in line with these findings, observing a larger number of nerve endings with the anterolateral approach, corresponding to the most radial area of the 1CMCJ, than with the dorsal approach.
Knowledge of the course of the RNSB helps to prevent injury in 1CMCJ surgery. The dorsal approach appears to be safer than the anterolateral approach because the incision is located between the 2 branches of the “V” formed by the division of the RNSB, and it can be extended distally if necessary, without increasing the risk of nerve injury. However, the dorsal approach does not guarantee avoiding injury to the RNSB, and careful dissection is still necessary even if the incision location seems more favorable.
The main study limitations are the small sample size and the utilization of cryopreserved specimens, given that postmortem loss of tissue tone can alter anatomical relationships and there is no clinical outcome. In addition, analog methods were used for macroscopic measurements, and the digital imaging analyses were semi-automatized, although the examiner selected the area for evaluation.
Conclusions
The incision is closer to the RNSB pathway with Wagner’s anterolateral approach than with Gervis’ dorsal approach, crossing with nerve branches in 50% of cases. The density of nerves is higher in the skin overlying the anterolateral versus dorsal aspect of the carpometacarpal joint. The risk of neuropathic wound pain after carpometacarpal joint surgery could be higher with the anterolateral approach, which should therefore be avoided.
Supplemental Material
sj-docx-1-han-10.1177_15589447251392940 – Supplemental material for Risk of Injury to the Superficial Branch of the Radial Nerve in Dorsal and Anterolateral Approaches to the First Carpometacarpal Joint
Supplemental material, sj-docx-1-han-10.1177_15589447251392940 for Risk of Injury to the Superficial Branch of the Radial Nerve in Dorsal and Anterolateral Approaches to the First Carpometacarpal Joint by Irene Pérez de Gracia-Velázquez, Javier De Torres-Urrea, Olga Roda, Clarisa Simón-Pérez, Natividad Martín-Morales, Francisco O’Valle and Pedro Hernández-Cortés in HAND
Footnotes
Acknowledgements
The authors thank Richard Davies, MA, for language review of the manuscript.
Ethical Approval
This study was approved by the Biomedical Research Ethics Committee of Andalusia.
Statement of Human and Animal Rights
Not required for this study.
Statement of Informed Consent
No informed consent was obtained or required for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.