
Abstract
Background:
Successful trapeziometacarpal (TM) joint arthroplasty depends heavily on bone quality, particularly of the trapezium, where cup loosening remains a leading cause of implant failure. While dual-energy x-ray absorptiometry measures bone mineral density (BMD), it lacks regional specificity. Computed tomography (CT)-derived Hounsfield units (HU) offer quantitative, site-specific bone density estimation and may serve as a surrogate for BMD in preoperative planning. This study investigated the relationship between CT-derived HU values and tactilely perceived bone hardness of the trapezium to evaluate HU as a reliable predictor of bone quality.
Methods:
Ten embalmed Body Donor hands were scanned using a Philips Spectral CT 7500 scanner. Bone segmentation and density analyses were conducted in 3D Slicer software, focusing on trabecular regions of the trapezium (proximal, ridge, and submetacarpal) and the first metacarpal (proximal, medial, and distal). Hounsfield unit values were converted to density (g/cm3) using validated equations. An experienced anatomist assessed trapezium hardness (“soft” or “hard”) using bone forceps. Correlations between HU values, bone volume, and perceived hardness were analyzed using Pearson correlation coefficient.
Results:
The mean trapezium HU was 354 (682.88 g/cm3), with regional trabecular variation: proximal 160.7 HU, ridge 286.5 HU, submetacarpal 241.7 HU. The first metacarpal demonstrated broader density variation (−285.8 to 228.8 HU). Hounsfield unit values correlated significantly with perceived hardness (r = .71, P = .02), whereas bone volume showed no correlation (r = .08, P = .82). Male trapezia displayed higher HU and density (472.7 ± 89.8 HU; 740.9 ± 44.0 g/cm3) than females (436.1 ± 87.2 HU; 723.0 ± 42.7 g/cm3).
Conclusions:
Computed tomography–derived HU values strongly correlate with perceived bone hardness and provide an objective surrogate for assessing bone quality in TM joint arthroplasty. Incorporating preoperative HU assessment may guide implant selection and fixation strategies, reducing trapezium cup loosening and implant failure.
Introduction
The interplay between osteoarthritis (OA) of the trapeziometacarpal (TM) joint, bone quality, and the success of joint replacement surgeries is a complex and multifaceted issue. Aseptic loosening, particularly of the trapezium cup component in total joint replacements, represents a significant challenge, often leading to implant failure.1,2 This phenomenon has been documented extensively, underscoring the multifactorial nature of these failures, which may include variables such as implant design, insertion technique, and patient-specific factors.3,4 Among these, the quality of the trapezium bone emerges as a pivotal concern, especially for cementless implants. 5 However, the relationship between hand OA and osteoporosis remains ambiguous, with studies yielding conflicting results regarding bone mineral density (BMD) in osteoarthritic hands compared with controls.6,7
Given the critical role of bone quality in the success of TM joint replacements, accurate and reliable methods for assessing bone density are essential. Traditional approaches, such as dual-energy x-ray absorptiometry (DXA) scans, offer precision in measuring BMD but face limitations in accessibility and difficulty in identifying bone borders.8,9 As an alternative, Hounsfield units (HU) from computed tomographic (CT) scans present a viable option for estimating bone density, offering the advantage of using existing clinical CT scans to assess regional bone density without incurring additional costs or procedures for the patient.10,11
For this purpose, this study aims to leverage the capabilities of 3D Slicer software in analyzing CT images. By examining the density of the trapezium and first metacarpal bones through CT imaging, this research seeks to provide insights into the potential for preoperative CT scans of the wrist to aid in determining trapezium bone density. This could inform surgical treatment decisions for TM joint OA, potentially guiding the choice toward non-prosthetic treatments or specific implant fixation methods to minimize the risk of implant failure. The endeavor to understand the intricacies of bone composition and its impact on surgical outcomes is crucial for improving patient care and advancing the field of orthopedic surgery and rehabilitation.
Methodology
Ethics
The protocol for this investigation received approval from the University of Melbourne Ethics Committee (Reference #2022-25124-325902-2), ensuring adherence to the ethical guidelines delineated by the Declaration of Helsinki and the International Federation of Associations of Anatomists. This safeguarded the integrity of the research process, emphasizing the dignified treatment and welfare of the donors from whom Body Donor hands were procured.
Body Donor Specimen Preparation and Imaging
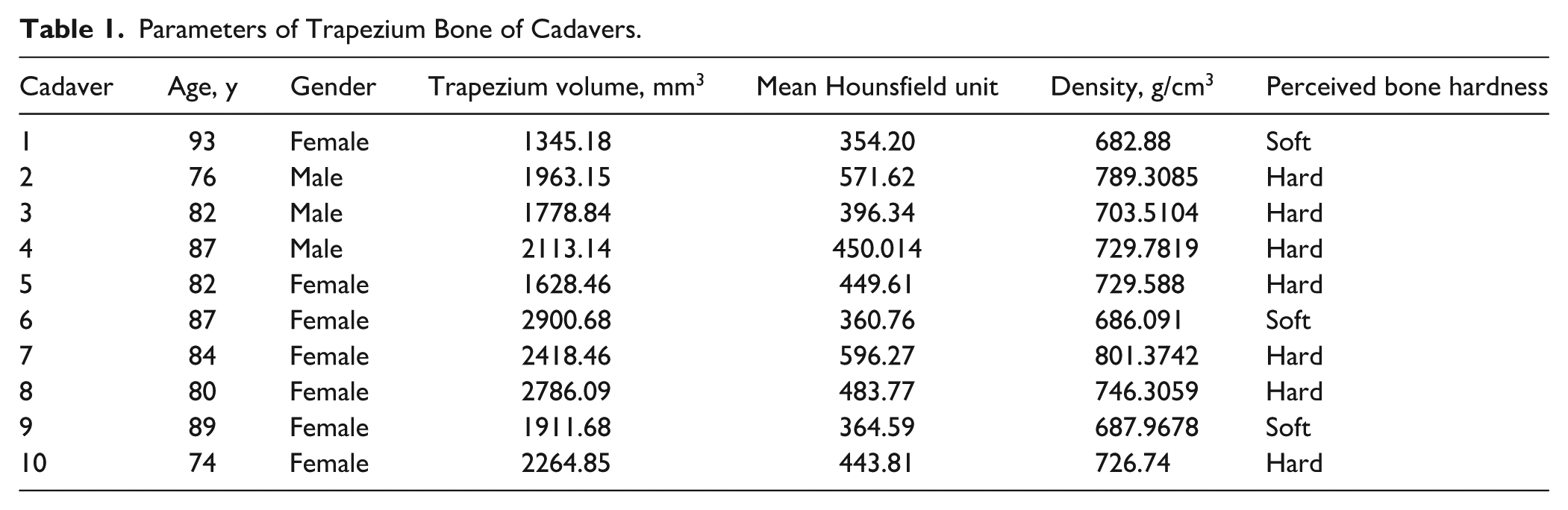
Body Donor specimens (n = 10), selected without regard to age, sex, or history of trapezium injury or surgical interventions, were subjected to comprehensive imaging protocols (Table 1). The mean age of female patients was 84.14 ± 6.26 years, whereas male patients had a mean age of 81.67 ± 5.51 years (Table 2). All Body Donors were sourced from the University of Melbourne Body Donation Program. Detailed visualization of the bone architecture was achieved using a Philips Spectral CT 7500 (16-slice multi-detector CT unit; Philips Medical System, The Netherlands) alongside an Adonis AE 100 Line Frequency X-ray system (Adonis Medical Systems Pvt Ltd, Vestland, Norway). The resultant CT data were then meticulously processed and converted into stereolithography (STL) files, facilitating subsequent 3-dimensional analyses.
Parameters of Trapezium Bone of Cadavers.
Differences in Trapezium Metrics Between Male and Female Patients.

Data Acquisition Through Advanced Imaging Software
The open-source “3D Slicer” software (version 5.2.2 for Windows OS) was employed to quantify and analyze bone density. The software’s “Segment Statistics” module played a pivotal role in deriving density metrics, particularly the mean HU value within defined segmented areas of interest. This module was instrumental in assessing various parameters, including volume, surface area, and mean intensity, among other segmentation-related metrics, for both the trapezium and first metacarpal bones.
Standardized Image Data Collection
The study’s image dataset comprised CT images from 10 anonymized Body Donors, processed in strict compliance with ethical and confidentiality standards. Variables such as gender and laterality were deliberately excluded to maintain a focus on bone density metrics. Imaging parameters were standardized across all specimens, with a 512 × 512 matrix size, 0.6-mm slice thickness, and a pixel size of 0.236328 mm, ensuring consistency in the data collection process.
Measurement Protocol
Targeted measurements were conducted on the trapezium and first metacarpal bones, selecting 3 specific points on each bone to assess volumetric differences effectively. This included:
Trapezium bone measurements: Analysis targeted subregions beneath the first metatarsal surface, between the scaphoid and trapezoid surfaces, and below the surface ridge, prioritizing trabecular bone and excluding cortical bone to elucidate trabecular content (Figures 1-3).
First metacarpal measurements: The focus was placed on the distal, proximal, and medial regions, emphasizing trabecular bone analysis to understand its density variations better.
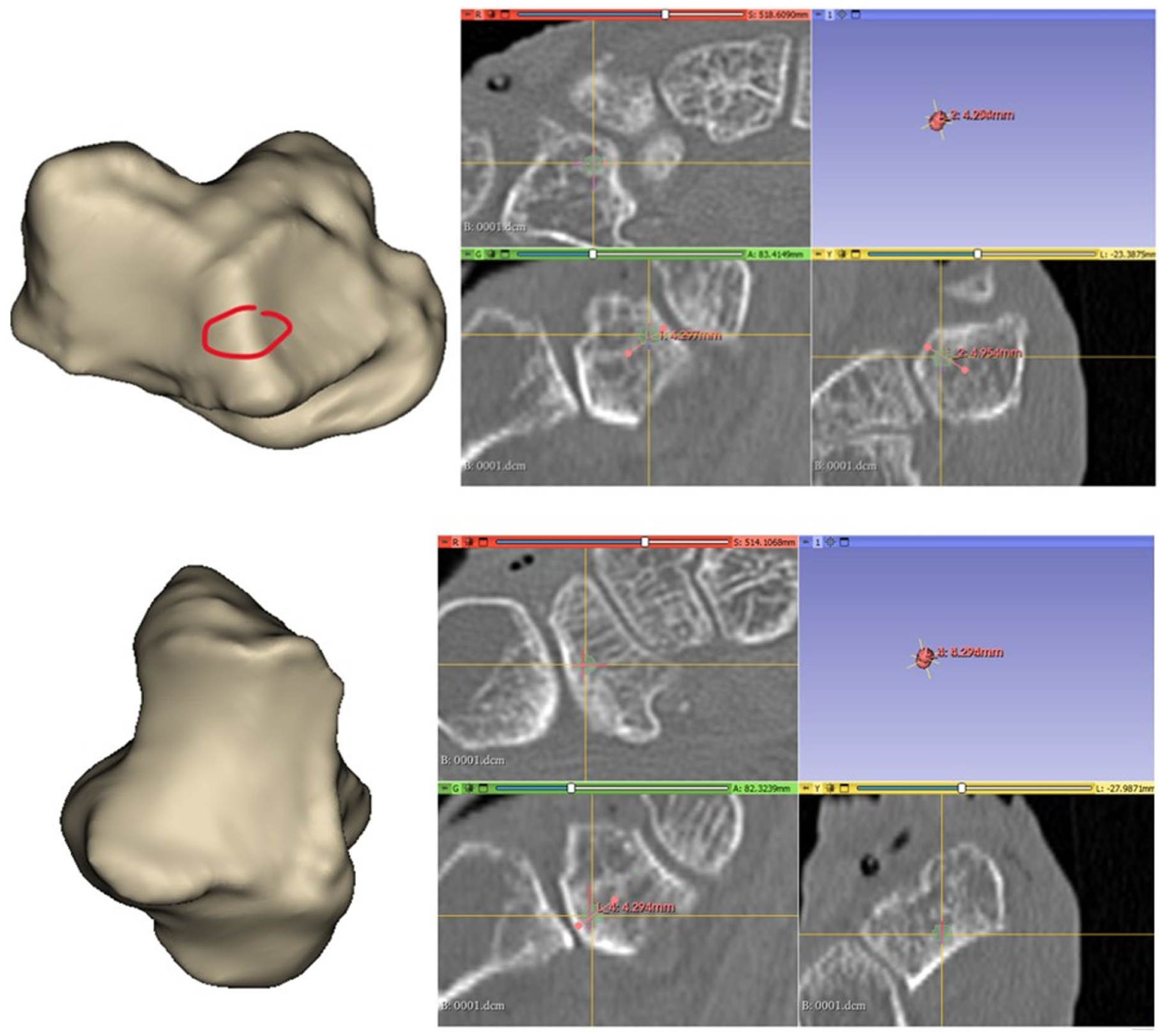
Measurement taken just below the middle of metacarpal at the center of the trapezium cortical bone.
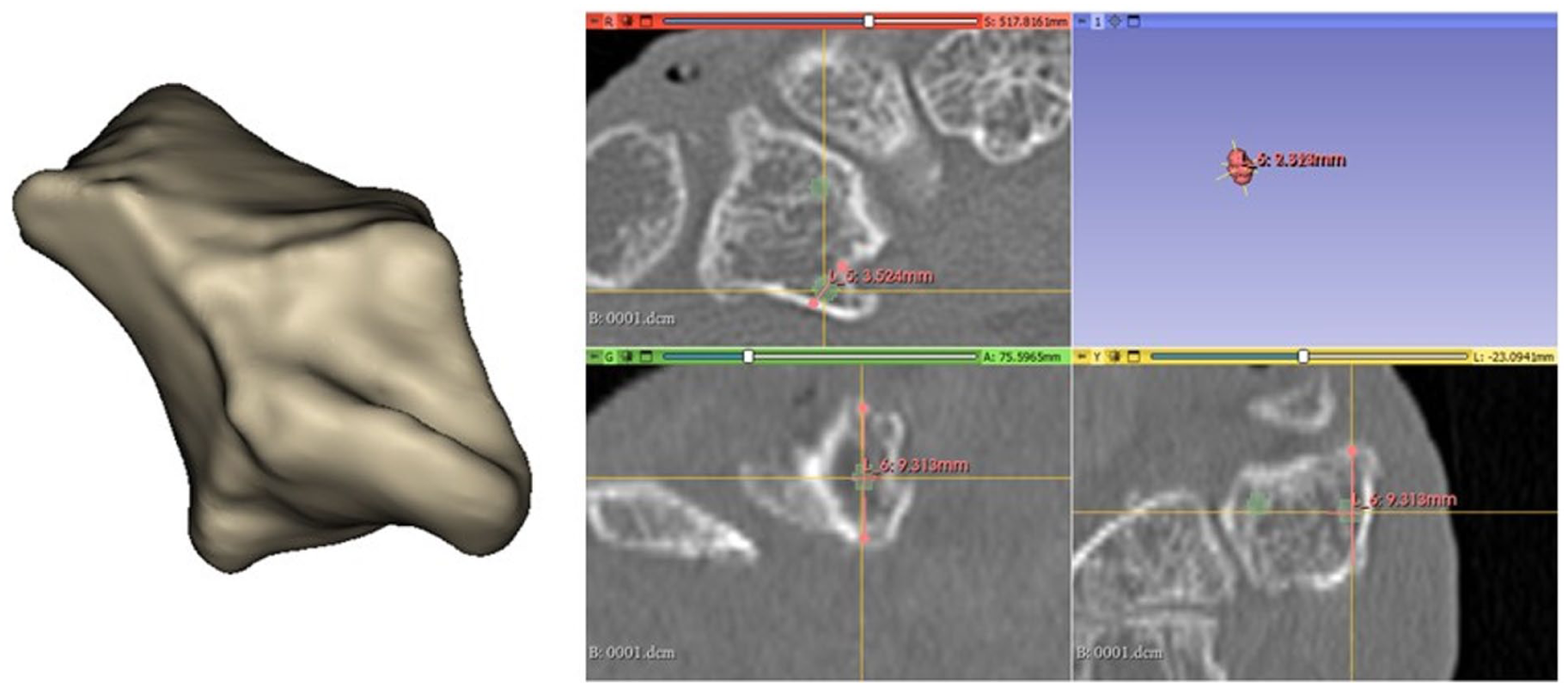
Second measurement taken at the midpoint of the ridge.
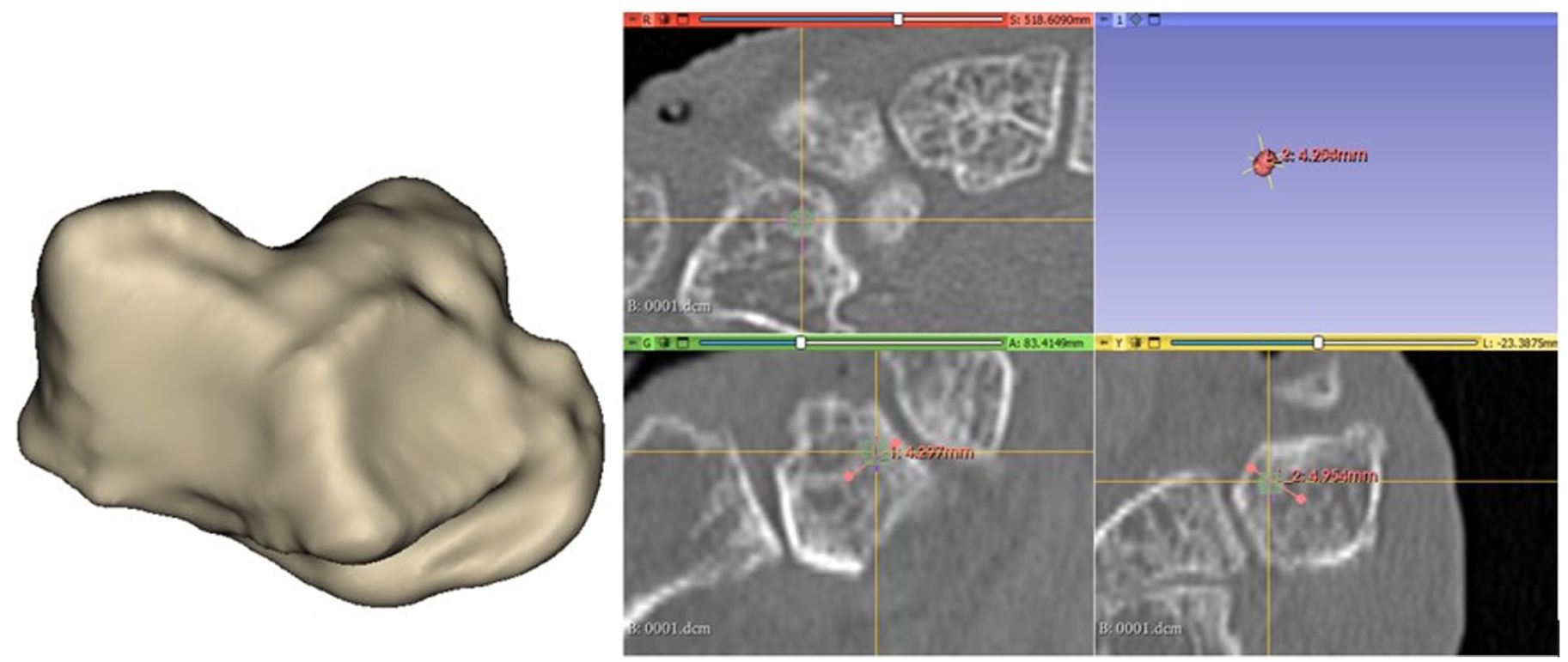
Measurement below the cortical bone of the bulge between the greater* and lesser multangular surfaces.
Analytical Phase and Data Synthesis
A comprehensive data compilation and analysis were undertaken following the data collection phase. Measurement values were tabulated and averaged for each anatomical site. The conversion of HU values into bone density (g/cm3) was performed using a formula proposed by Genisa et al, 12 enabling a standardized approach for density comparison across specimens:

Interpretation of Findings
The analytical process revealed notable disparities in bone density measurements, particularly accentuating the differences between cortical and trabecular bone densities. The variability observed in the trapezium bone density suggests potential implications for surgical outcomes and the success rate of implant integration. Similarly, variability in the density of the first metacarpal bone, influenced by its internal structure, underscores the complexity of bone composition and its significance in clinical decision-making and intervention strategies.
Perceived Bone Hardness Assessment and Correlation Analysis
To further investigate the structural characteristics of the trapezium, qualitative tactile assessments of bone hardness were conducted using standard bone forceps during Body Donor specimen preparation. The hardness of each trapezium was classified as “soft” or “hard” based on the resistance encountered when applying forceps pressure to remove the bone. This perceived bone hardness, evaluated through direct manipulation, provides an essential surrogate measure of bone quality, complementing quantitative imaging-based assessments. Given that quantitative data for each patient is currently unrealistic in a clinical setting, this test of perceived hardness is deemed a valuable and necessary addition.
To determine the relationship between perceived hardness, HU density, and bone volume, statistical analyses were performed to assess correlations between tactile feedback and CT-derived bone density metrics. The study aimed to establish whether higher HU values and greater bone volume corresponded to increased perceived hardness, which could affect implant selection and surgical planning. By integrating quantitative radiological data and qualitative tactile assessments, this study offers a multimodal evaluation of bone quality, improving the understanding of the biomechanical properties of the trapezium in osteoarthritic and surgical contexts.
This approach aligns with prior literature where intraoperative tactile assessments have been used as a surrogate for bone quality in orthopedic and spine surgery. For example, Romme et al 13 demonstrated that perceived vertebral bone hardness correlated with BMD on DXA in spinal surgery patients, whereas Li and Aspden 14 and Gevers et al 15 showed increased stiffness and hardness of osteoarthritic bone based on mechanical testing. In dental surgery, tactile feedback during implant placement has also been linked to radiographic bone density. 12 Moreover, these qualitative assessments are increasingly recognized in OA-related bone studies, often corroborated by quantitative techniques such as nanoindentation and compression testing.16-18
In our study, assessments were performed by a single experienced anatomist with more than 20 years of surgical and anatomical expertise. All bones were assessed in a single sitting to minimize intra-rater variability. Although formal inter-rater reliability was not calculated, a binary classification approach was employed to reflect real-time surgical decision-making. While we acknowledge that mechanical hardness quantification (eg, nanoindentation, microindentation) is valuable, such methods require specialized equipment not available during our cadaveric preparation. Several studies validate these methods as correlating well with biological bone properties, showing that hardness values vary significantly with hydration, embedding, and OA grade.18-20 This remains a key area for future validation studies.
Results
The CT analysis of the trapezium and first metacarpal bones, using embalmed frozen Body Donor hands, yielded volumetric and densitometric data across multiple regions of interest within the bones. The findings are summarized in the following sections.
Trapezium Bone Analysis
The overall density for the full trapezium bone was determined to be 354 HU, correlating to a calculated density of 682.88 g/cm3. Focusing on the trabecular bone, the proximal region exhibited a mean HU of 160.73, the ridge area showed a higher mean HU of 286.53, and the area below the metacarpal exhibited a mean HU of 241.72. Notably, the trabecular bone density varied, with the proximal region presenting a mean per bone HU of 230.00, the ridge did not have a specific value reported, and the area below the metacarpal again lacked a specific mean per bone HU value.
First Metacarpal Bone Analysis
In the first metacarpal, the trabecular bone at the proximal end had a mean HU of 228.80, whereas the medial and distal regions showed a mean HU of −285.81 and 192.08, respectively. The mean per bone HU for the proximal region was reported at 45.0.
Variability and Trends
Significant variability was observed in the density values across different regions of the same bone and between the trapezium and the first metacarpal bones. The trapezium bone consistently exhibited higher mean density values than the first metacarpal, with the full bone measurements yielding mean HU values ranging from 354.00 to 596.00 HU and density values from 682.88 to 801.37 g/cm3. This variability was also evident within the trabecular regions of the trapezium bone, with mean HU values per bone ranging from 230.00 to 393.00 HU. Conversely, the first metacarpal bone displayed a broader range of mean HU values, including negative values in the medial regions, indicating a hollow or less dense internal structure. The mean per bone HU for the first metacarpal varied from −24.00 to 84.00 HU, and the density values ranged from 497.54 to 550.61 g/cm3. The data indicate a trend where the trabecular region of the trapezium bone possesses a higher mean density compared with the trabecular region of the first metacarpal bone.
In addition, within the trapezium bone, the areas below the metacarpal ridge tended to show higher density values than the proximal regions. These results elucidate the complex interplay between bone architecture and density, highlighting the variability that exists not only between different bones but also within different areas of the same bone. The disparities in density measurements underscore the importance of region-specific analysis when evaluating bone quality and may have implications for clinical decision-making regarding surgical interventions and implant design.
Statistical analysis evaluated the relationship between perceived bone hardness, as assessed through tactile feedback with forceps, and quantitative parameters of the trapezium, including volume, density, and mean HU values (Figure 4a
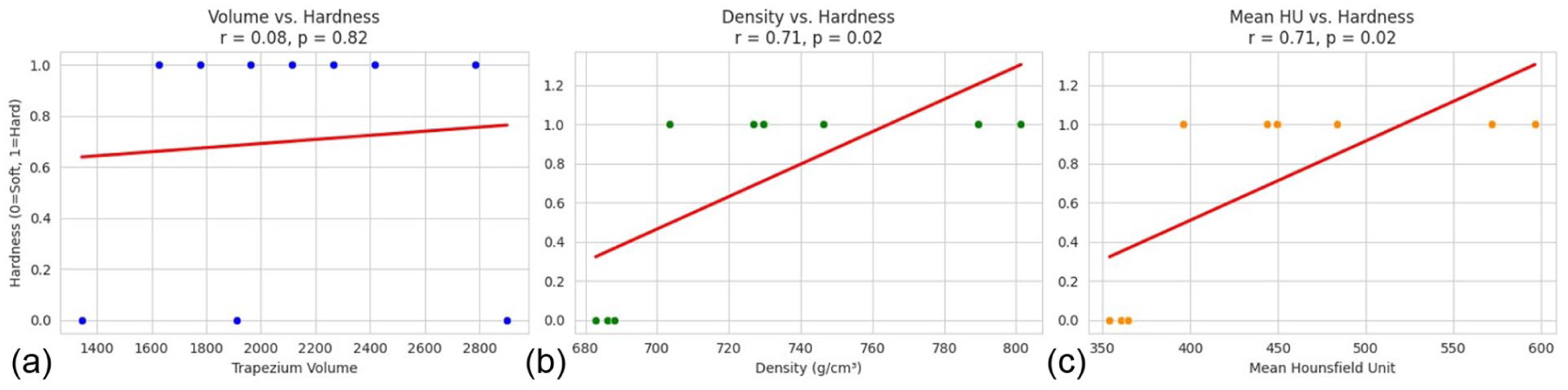
Statistical analysis evaluating the relationship between perceived bone hardness and computed tomography–derived bone parameters of the trapezium.
Differences in Trapezium Properties Between Male and Female Patients
Trapezium volume was higher in female patients (2179.34 ± 580.79 mm3) compared with male patients (1951.71 ± 167.44 mm3). Conversely, male patients exhibited higher trapezium HU (472.66 ± 89.81) and trapezium density (740.87 ± 43.96 g/cm3) compared with female patients, who had values of 436.14 ± 87.24 and 722.99 ± 42.70 g/cm3, respectively.
Discussion
The relationship between OA and BMD in the trapezium has been extensively investigated due to its implications for implant stability in TM joint replacement.12-14,21 Hansen et al 22 used DXA to assess BMD in osteoarthritic trapezium bones and demonstrated high intra-observer and inter-observer reliability. However, their findings indicated only a moderate correlation between trapezium BMD and distal radius BMD, suggesting that systemic bone assessments may not fully represent the localized bone quality of the trapezium. 22 This aligns with the work of Haugen et al, 6 who found no significant association between hand OA and overall total body BMD, reinforcing the need for region-specific bone assessments.
Recent studies have explored the potential of CT-derived HU values as a quantitative measure of bone density. Kim et al found a moderate correlation between CT and DXA measurements, supporting CT as a reliable alternative for assessing bone density in patients with OA. 13 In addition, Schreiber et al demonstrated that HU values were significantly lower in patients with OA (mean 377 HU) compared with asymptomatic individuals (mean 436 HU), highlighting the progressive decline in trapezium bone density with OA severity. Given these findings, this study aimed to evaluate variations in trapezium and first metacarpal bone density using CT imaging and correlate these findings with perceived bone hardness.
This study revealed significant variations in bone density within the trapezium and first metacarpal bones. Specifically, the proximal region of the trapezium exhibited lower mean HU values than the ridge region. At the same time, the first metacarpal displayed a wider range of HU values, including negative values in the medial regions, indicating areas of reduced density or potential bone loss. Hansen et al 22 previously reported increased BMD within the trapezium as OA progresses, suggesting that bone remodeling occurs in response to joint degeneration. The current study supports these findings, reinforcing the importance of region-specific density assessments when evaluating bone quality for surgical planning. Such assessments are critical in optimizing implant design and fixation strategies to reduce the risk of failure.15,16
One of the novel aspects of this study is the integration of tactile feedback assessments using bone forceps to evaluate perceived bone hardness.17,18 This method established a correlation between direct manual assessment and radiological bone quality. Correlation analysis revealed a significant association between HU values and perceived bone hardness (r = .71, P = .02), indicating that CT-derived HU values align well with subjective assessments of bone integrity. These results are consistent with prior studies, which have shown that osteoarthritic bone can be stiffer or harder than normal bone, despite having a lower material density.14,15 In contrast, inflammatory arthritis models such as those used by Vidal et al 17 demonstrated reduced bone hardness and microstructural degradation. Furthermore, this study parallels previously reported methods of tactile assessment, which have been used intraoperatively and correlate well with BMD and mechanical testing. 13 While our method was qualitative, it is representative of how surgeons assess bone quality intraoperatively. The generalizability of our findings could be strengthened by future validation using microindentation and nanoindentation techniques, which have been shown to yield hardness values between 0.47 GPa (wet) and 2.57 GPa (dry embedded), and moduli between 4 and 34 GPa depending on hydration state. 23 These findings support the use of HU as a radiographic surrogate and encourage standardization of future mechanical testing protocols.
In contrast, bone volume alone did not correlate significantly with perceived hardness, suggesting that volume is not the sole determinant of bone quality. These findings are consistent with studies in spinal surgery, where Romme et al reported a strong correlation between intraoperative bone hardness perception and measured BMD in patients undergoing dorsal stabilization with pedicle screws. 12 However, their study also noted that subjective assessments were less reliable in osteoporotic patients, reinforcing the importance of objective imaging modalities.
Furthermore, studies have shown that the mechanical loading history influences bone density changes in the trapezium.20,23 Hwang et al conducted a 3-dimensional analysis of the trapezium subchondral bone. They found that subchondral bone density varied significantly according to OA stage, with lower bone density associated with elevated osteocalcin levels and systemic reductions in BMD. 24 This suggests that osteoarthritic bone degradation may be linked to broader metabolic factors, reinforcing the necessity of preoperative BMD assessments.
Given the impact of bone density on implant longevity, this study underscores the need for routine CT-based assessments of trapezium bone quality in patients undergoing TM joint replacement. Hounsfield unit values provide a reproducible metric that aligns with clinical assessments of bone integrity and may serve as an adjunct to intraoperative tactile evaluations. The findings also have implications for surgical decision-making, particularly regarding the choice between cementless and cemented implants. Patients with lower HU values may benefit from cemented fixation to mitigate the risk of implant loosening, as lower bone density has been associated with poorer outcomes in TM joint arthroplasty.13,15
Despite its strengths, this study has several limitations. The sample size was relatively small, limiting the generalizability of findings. In addition, the Body Donor nature of the study may not fully reflect in vivo bone remodeling processes. Excluding demographic variables such as age and sex may have overlooked key factors influencing bone quality. 25 While CT-derived HU values provide valuable insights into bone architecture, they do not offer direct histological assessments of trabecular structure, which may further influence implant stability. Future research should explore larger clinical cohorts and incorporate direct biomechanical testing to validate these findings.
Conclusion
This study highlights the significant variability in bone density within the trapezium and first metacarpal bones, underscoring the importance of region-specific assessments in preoperative planning for TM joint replacement surgery. The findings suggest that CT-derived HU measurements provide a reliable surrogate for evaluating bone quality, with strong correlations observed between perceived bone hardness, HU values, and BMD. These results support the potential clinical application of preoperative CT scans to guide implant selection, optimize fixation strategies, and reduce implant failure rates. By integrating objective imaging data with qualitative intraoperative assessments, clinicians can make more informed surgical decisions, ultimately enhancing patient outcomes in the management of TM joint OA.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures complied with the Declaration of Helsinki and the International Federation of Associations of Anatomists guidelines. Ethical approval was obtained from the University of Melbourne Human Ethics Committee (Ref. #2022-25124-325902-2).
Statement of Informed Consent
Informed consent for body donation and research use was obtained from all donors through the University of Melbourne Body Donation Program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.